
Gary Smith, Cille Kennedy, Sarah Knipper, John O'Brien and Janet O'Keeffe
Research Triangle Institute
"This report was prepared under contract #HHS-100-97-0014 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and Research Triangle Institute. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Cille Kennedy, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. Her e-mail address is: Cille.Kennedy@hhs.gov.
The views expressed in this report do not necessarily reflect the views of the Department of Health and Human Services or the Research Triangle Institute.
MEMORANDUM
Dear Reader:
Medicaid is the major public payer of community services and supports for working age adults with serious mental illnesses. Working in partnership, Federal and State governments, along with advocates, have developed an evolving array of mental health services and supports configured in systems that reflect the uniqueness of each state and locality. Medicaid has been, and continues to be, the linchpin in all these designs. States have creatively used existing Medicaid options, and the Federal program has developed Medicaid waivers that reflect advances in the philosophy and treatment of adults with serious mental illnesses.
As the philosophy and treatment of mental health disorders has evolved, programs and systems have been refined, documented and evaluated. With the identification of evidence-based and emerging practices, States have sought either to adapt or initiate these practices. Fundamental to this development has been financing. Medicaid is one of many sources of funding for mental health and related services and supports. In addition to Medicaid, there are at least 39 other Federal programs across nine Departments that provide support to people with mental illnesses. It is within this context that Using Medicaid in Support of Working Age Adults with Serious Mental Illnesses in the Community: A Handbook is developed to describe the Medicaid program in the delivery of services to adults with serious mental illnesses. We are pleased to offer this Handbook to serve as a reference guide. Its purposes are:
- To explain how existing Medicaid options and waivers are used by states to finance a broad range of community services and supports for adults with serious mental illnesses; and,
- To demonstrate what aspects of state-of-the art community services and supports for this population are funded by Medicaid.
This Handbook would not have been possible without the commitment and hard work of many people. However, a few individuals deserve special recognition for their outstanding efforts and dedication, which has made this Handbook a reality: Janet O'Keeffe, of Research Triangle Institute; Gary Smith, of Human Services Research Institute; Ruth Katz and Cille Kennedy of the Office of the Assistant Secretary for Planning and Evaluation; and Gail Arden, Mary Jean Duckett, Mary Clarkson, and Peggy Clark of the Centers for Medicare and Medicaid Services.
As the Medicaid program continues to evolve to meet the needs of its multiple beneficiaries, new policy and clarification of existing policy will be made subsequent to the publication of this Handbook. These will be disseminated through State Medicaid Directors' Letters and the State Medicaid Manual, both of which are available on the Centers for Medicare and Medicaid Services website.
/ Signed /
Michael J. O'Grady, Ph.D.
Assistant Secretary for Planning and Evaluation
ACKNOWLEDGMENTS
This Handbook could not have been completed without the contributions of many individuals who are acknowledged below.
At the Centers for Medicare and Medicaid Services, Glenn Stanton, Carey O’Connor, Peggy Clark, Mary Clarkson and Jackie Wilder.
At the Center for Mental Health Services/Substance Abuse and Mental Health Services Administration, Crystal Blyler, Neal Brown, Jeffrey Buck, Eileen Elias, and Betsy McDonel Herr.
We would like to convey special thanks to Letty Carpenter. Chapter 3 of this handbook is based in large part on the especially clear description of Medicaid eligibility she authored Chapter 2 (“Financial Eligibility Rules and Options”) in Gary Smith, Janet O’Keeffe, Letty Carpenter, Pamela Doty, Gavin Kennedy, Brian Burwell, Roberta Mollica, and Loretta Williams (2000). Understanding Medicaid Home and Community Services: A Primer. George Washington University, Center for Healthy Policy Research. Available at http://aspe.hhs.gov/daltcp/reports/primer.htm (accessed February 22, 2005).
Thanks are also due to advisory group members, expert consultants, and reviewers, including the following people:
Joyce Allen, Wisconsin Department of Health and Family Services
Sharon Autio, Minnesota Department of Human Services
Michael Cheek, The Lewin Group (formerly of American Public Human Services Association)
Michael Deily, Utah Department of Health
Michael Fitzpatrick, National Alliance for the Mentally Ill
Larry Fricks, Georgia Office of Consumer Relations, Department of Human Resources
Andrew Hyman, National Association of State Mental Health Directors
Mary Kennedy, Minnesota Department of Human Services
Chris Koyanagi, Bazelon Center for Mental Health Law
Meredith Lee, American Public Human Services Association
H. Stephen Leff, Human Services Research Institute
Virginia Mulkern, Human Services Research Institute
John O’Brien, Technical Assistance Collaborative
Lee Partridge, National Association of State Medicaid Directors
Celeste Putnam, Florida Department of Children and Families
Amy Sander, The Lewin Group (formerly of American Public Human Services Association)
Robert Seiffert, Nebraska Department of Health and Human Services
Don Shumway, New Hampshire Department of Health & Human Services
Elizabeth Tanzman, Vermont Department of Developmental and Mental Health Services
Wendy White Tiegreen, Georgia Department of Human Resources
Jennifer Urff, National Association of State Mental Health Directors
INTRODUCTION
| Our country must make a commitment: Americans with mental illness deserve our understanding and they deserve excellent care. They deserve a health system that treats their illnesses with the same urgency as a physical illness. President George W. Bush1 |
Mental illness is the leading cause of disability in the United States.2 It can strike at any stage in life. Serious mental illnesses (including schizophrenia, manic-depressive illness, and severe depressive disorders) can be especially disabling if undiagnosed and untreated.3 Individuals with serious mental illnesses experience substantial limitations in major life activities, at home, at work, and in the community. Each year, approximately five to seven percent of adults experience a serious mental illness.4
If unaddressed, serious mental illnesses can trap individuals in a lifetime of poverty, dependency and homelessness. They also can lead to costly and frequent hospitalization, institutionalization, and recurrent involvement in the criminal justice system. Many individuals with serious mental illnesses also experience co-occurring substance abuse disorders. Serious mental illness has major fiscal consequences for state and local governments and exacts a high toll on the nation’s economy.5 Most importantly, serious mental illness has severe human costs and, too often, tragic outcomes.
| We envision a future when everyone with a mental illness will recover, a future when mental illnesses can be prevented or cured, a future when mental illnesses are detected early, and a future when everyone with a mental illness at any stage of life has access to effective treatment and supports -- essentials for living, working, learning, and participating fully in the community. President’s New Freedom Commission on Mental Health6 |
There has been enormous progress in treating and supporting individuals with serious mental illnesses. There are now effective medications, evidence-based and other promising practices that can aid many individuals with serious mental illnesses to live fulfilling, productive lives in the community. Recovery has emerged as the essential goal of mental health service provision. Recovery envisions that individuals actively self-manage their illnesses “while reclaiming, gaining and maintaining a positive sense of self, roles, and life beyond the mental health system in spite of the challenge of the psychiatric disability.”7 There also is increased emphasis on consumer-centered and consumer-driven service planning and provision. It is clear that effective treatment and support can enable individuals with serious mental illnesses to live, learn, work, participate in, and contribute to their communities.
Medicaid and Publicly-Funded Mental Health Services
Publicly-funded mental health services play a linchpin role in supporting individuals with serious mental illnesses. In the United States, public funds account for almost $3 of every $5 spent on mental health services.8 The organization and management of public mental health systems is a state responsibility. States and localities underwrite a substantial share of national mental health expenditures. At one time, public mental health systems revolved around the operation of large public institutions. Today, these systems principally focus on assisting individuals in the community. State/local mental health systems are often described as the safety net because they are called upon to support individuals who experience especially challenging psychiatric disabilities.
The federal role in supporting individuals with serious mental illnesses includes making grants-in-aid to states, underwriting basic mental health research, and promoting the development and implementation of effective support strategies that can be applied in both the public and private sectors. These federal efforts are vital in improving the quality and effectiveness of mental health services for persons of all ages with serious mental illnesses.
Medicaid is a multi-faceted, complex federal-state program that underwrites the costs of health care, primarily for low-income persons and individuals with disabilities, including adults with severe mental illnesses in community settings.
The joint federal-state Medicaid program is the single largest source of funding for public mental health services.9 In the future, Medicaid is expected to account for a growing proportion of the resources that underwrite state-administered mental health services.10 No single source of public funding -- including Medicaid -- is sufficient in its amount or purpose to fully support effective community mental health services. Many funding sources must be tapped to support individuals. However, Medicaid can play a pivotal role in underwriting vital services and supports for low-income individuals with serious mental illnesses.
| In some states, Medicaid underwrites services for more than 60 percent of the individuals served in the public mental health system.11 |
States have considerable latitude in shaping their Medicaid programs. While each states Medicaid program must meet mandatory federal requirements, including covering essential health services (e.g., inpatient hospital) and serving core eligibility groups, federal law and regulations give states many options. These options include extending Medicaid eligibility to additional low-income groups beyond those mandated, offering additional optional services, and configuring services and their delivery in innovative ways by obtaining waivers of federal law.
State mental health systems face financial and other pressures. There is broad agreement that the mental health services system does not adequately serve millions of people who need care.12 Against this backdrop, the effective use of Medicaid can aid states in strengthening services for individuals with serious mental illnesses.
| More individuals could recover from even the most serious mental illnesses if they had access in their communities to treatment and supports that are tailored to their needs. The Presidents New Freedom Commission on Mental Health13 |
Through Medicaid, states can obtain federal financial participation (FFP) in the costs of a variety of community mental health services. Individuals who experience major disability as a result of their mental illness frequently qualify for Medicaid services. While there are limitations in using Medicaid to serve people with serious mental illnesses, the program offers significant, critical opportunities for states in advancing their mental health policy goals.
All states offer some mental health services in their Medicaid programs. Federal Medicaid law does not contain explicit provisions concerning the exact types of mental health services and supports that a state must offer. Community mental health services may be furnished under certain optional service coverage categories, principally as rehabilitative services or under the clinic option. Over the years there has been relatively little formal federal guidance to states concerning Medicaid-funded community mental health services. Because of the great flexibility afforded states in program design, there are essentially 51 unique state Medicaid programs.
The many changes in federal law and regulations since Medicaid was created in 1965 have enhanced the program, but have also added to its complexity. In the arena of community mental health services, Medicaids potential role in supporting individuals with serious mental illnesses can be confusing for policymakers, state officials, service providers, advocates, and consumers alike.
Purpose and Organization of the Handbook
This Handbook is designed to improve understanding and provide greater clarity concerning Medicaids contribution in supporting working-age adults with serious mental illnesses in the community. The Handbook focuses on working-age adults between the ages of 21 and 64 with serious mental illnesses, whose need for support extends beyond mental health services that can be effectively provided by primary care physicians or periodic visits to outpatient settings.
The mental illnesses these individuals experience result in significant functional impairment and have serious repercussions when left untreated. They may need intensive services over an extended period of time, either continuously or episodically, as well as ongoing access to appropriate services and interventions while in recovery. Sometimes, these individuals are labeled as having severe mental disorders or severe and persistent mental illnesses.
The decision to focus the Handbook on services for working-age adults stemmed from practical considerations and in no way discounts the importance of the needs of children and older persons who are affected by mental illnesses.
The Handbook assembles considerable information about pertinent federal policies into a single publication. It also contains information about how individual states have supported individuals with serious mental illnesses under Medicaid.
The Handbook seeks to provide useful, practical, reliable and comprehensive information to state policymakers and state officials -- in both state mental health authorities and state Medicaid agencies. The Handbook focuses on Medicaid but recognizes that other federal, state and local funding streams are also essential contributors to fashioning a comprehensive array of critical supports. The Handbook also is intended to serve as a resource to others who want to understand how Medicaid supports individuals with serious mental illnesses.
The Handbook complements Understanding Medicaid Home and Community Services: A Primer, released by the Department of Health and Human Services Office of the Assistant Secretary for Planning and Evaluation in October 2000.14 The Primer concentrated on Medicaid home and community services for individuals with disabilities other than serious mental illnesses. The Handbook is intended to complement and round out the information contained in the Primer about supporting people with disabilities in the community. It also reflects the commitment in President Bushs New Freedom Initiative to actively support and assist states to promote community living for all individuals with disabilities.
The information contained in the Handbook is current as of January 2005. However, federal Medicaid policy continues to evolve, both legislatively and in the form of updated federal guidance to states about how Medicaid can be used to support people with serious mental illnesses. States also modify their policies and coverages to improve and strengthen services. Chapter 2 provides information about resources for tracking federal policy developments.
Preparation of the Handbook
The preparation of the Handbook benefited substantially from the active participation of many individuals on a Technical Advisory Group (TAG) that was formed to guide its preparation. The TAG was composed of federal and state officials, along with subject matter experts and consumer representatives. The TAG assisted in framing the content of the Handbook, offered many valuable suggestions and insights during its preparation and reviewed drafts of each chapter. The Disabled and Elderly Health Programs Group (DEHPG) at the Center for Medicaid and State Operations (CMSO), Centers for Medicare and Medicaid Services (CMS) also reviewed and provided extensive input into the Handbooks preparation.
Organization of the Handbook
The Handbook recognizes that readers have different interests and knowledge concerning (a) the Medicaid program and (b) services and supports for working-age adults with serious mental illnesses. The Handbook is designed to serve as a reference guide that includes sufficient annotation of reference material to fulfill its technical support role.
The first part of the Handbook provides basic information about supporting working-age adults with serious mental illnesses in the community and about the Medicaid program.
Chapter One provides a broad overview of community support services for working-age adults with serious mental illnesses. It traces the evolution of these services, including the emergence of recovery as the central goal of mental health services. The chapter emphasizes that successfully supporting individuals in the community must address many types of needs and draw upon multiple resources (including but not limited to Medicaid).
Chapter Two provides information about the fundamental purpose and features of the Medicaid program. It is intended to provide a basic grounding for readers who are unfamiliar with Medicaid.
The next two chapters address two fundamental aspects of the provision of Medicaid-funded mental health services to working-age adults with serious mental illnesses: eligibility and benefits.
Chapter Three addresses the topic of eligibility. It provides an explanation of Medicaid financial eligibility criteria, one of the most complicated dimensions of Medicaid law. It describes federal mandates and options in extending Medicaid eligibility to adults with disabilities, along with special issues and problems that arise in securing eligibility for adults with serious mental illnesses.
Chapter Four provides detailed information concerning the principal Medicaid options (e.g., targeted case management, clinic, and rehabilitative services). The discussion of each option includes information concerning relevant statutory provisions, statutory history, regulations, and federal guidance to states in employing each option. The chapter also describes other Medicaid benefits (e.g., prescribed drugs) that play an important role in supporting individuals. The objective of this chapter is to describe federal policy regarding Medicaid benefits.
The final three chapters of the Handbook address several important topics in employing Medicaid to support working-age adults with serious mental illnesses.
Chapter Fives theme is finding the fit. It links mental health practices and service approaches to Medicaid coverage options. In particular, the chapter identifies key mental health services (e.g., Assertive Community Treatment and peer support), discusses the feasibility of offering them through the Medicaid program, and illustrates how various states have successfully incorporated these services into their programs. The information in this chapter can serve as a starting point for states interested in exploring new directions in employing Medicaid to underwrite community mental health services.
Chapter Six describes the Medicaid waiver and demonstration authorities that provide an avenue for states to employ alternative approaches to the provision of Medicaid-funded mental health services. These waiver authorities have been used by several states to deliver mental health services under alternative configurations. The chapter also discusses the potential pros and cons of employing these alternatives to the standard Medicaid coverage options.
Chapter Seven explores several topics in crafting effective strategies for using Medicaid to support working-age adults in the community. These topics include consumer-directed services, facilitating the transition of persons from institutional settings to the community, and the management of Medicaid services.
Throughout the Handbook, examples illustrate how individual states have shaped Medicaid services to effectively support people with serious mental illnesses in the community.
The Handbook includes appendices with important federal primary source documents and other information. Each chapter of the Handbook also has an annotated bibliography of additional resource materials that readers might find useful, along with information about how to obtain them. There also are descriptions of other resources available on the Internet.
Conclusion
The provision of effective services and supports to working-age adults with serious mental illnesses is a critical concern at both the state and federal levels. The Handbook is intended to assist states in assessing how Medicaid can be most effectively used to address the needs of these individuals. It is up to state policymakers working with the mental health community to identify their states unique needs and goals, and then to use the Handbooks information (a) to choose the alternatives best suited to their state, and (b) to decide how these alternatives might be best used.
Endnotes
-
Remarks by President Bush on April 29, 2002 in Albuquerque New Mexico announcing the formation of the New Freedom Commission on Mental Health.
-
World Health Organization (2001). The World Health Report 2001 -- Mental Health: New Understanding, New Hope. Geneva: World Health Organization.
-
As defined by Section 1912(c) of the Public Health Services Act (as amended by P.L. 102-321), an adult with a serious mental illness is:
a person age 18 and over, who currently has, or at any time during the past year has had a diagnosable mental, behavioral, or emotional disorder of sufficient duration to meet diagnostic criteria specified within the DSM III-R (Diagnostic and Statistical Manual for Mental Disorders), and that has resulted in functional\ impairment that substantially interferes with or limits one or more major life activities.
Functional impairment is defined as difficulties that substantially interfere with or limit role functioning in one or more major life activities including basic daily living skills (e.g., eating, bathing, dressing); instrumental living skills (e.g., maintaining a household, managing money, getting around the community, taking prescribed medication); and functioning in social, family, and vocational/educational contexts. Adults who would have met functional impairment criteria during the referenced year without benefit of treatment or other support services are considered to have serious mental illnesses.
-
United States Public Health Service, Office of the Surgeon General (1999). Mental health: A Report of the Surgeon General. Rockville, MD: Department of Health and Human Services, U.S. Public Health Service.
-
The estimated annual economic cost of mental illness is $79 billion, including loss of productivity. Presidents New Freedom Commission on Mental Health (2003). Achieving the Promise: Transforming Mental Health Care in America. Final Report. Rockville, MD: Department of Health and Human Services Publication No. SMA-03-3832. [Hereafter, PNFCMH (2003)]
-
Steven J. Onken, Ph. D. and Jeanne M. Dumont, Ph.D. (2002). Mental Health Recovery: What Helps and What Hinders? Alexandria VA: National Association of State Mental Health Program Directors and the National Technical Assistance Center for State Mental Health Planning.
-
Coffey, R.M., Mark, T., E., Harwood, H., McKusick, D., Genuardi, J. et al. (2000). National Expenditure Estimates of Expenditures for Mental Health and Substance Abuse Treatment, 1997. Rockville, MD: Substance Abuse and Mental Health Services Administration. (SAMSHA Publication SMA-00-3499)
-
Jeffrey A. Buck (2003). Medicaid, Health Care Financing Trends, and the Future of State-Based Public Mental Health Services. Psychiatric Services, Vol. 54, No. 7. In 1997, Medicaid accounted for about one-half of state and locally administered mental health spending. This share is forecast to increase to about two-thirds of spending by 2017.
-
For example, in Florida it is estimated that Medicaid accounts for 62 percent of spending (Celeste Putnam, Florida Director of Mental Health: personal communication, June 2003.) In California, the figure is even higher -- 68 percent. California Mental Health Planning Council (2003). California Mental Health Master Plan: A Vision for California. Sacramento: MHPC. Available on the Internet at: www.dmh.cahwnet.gov/MHPC/masterplan.asp
-
President's New Freedom Commission on Mental Health. (2002) Interim Report of the New Freedom Commission on Mental Health. Rockville MD.
-
PNFCMH (2003).
CHAPTER 1: COMMUNITY SUPPORT AND FUNDING
| Working age adults with serious mental illnesses can live, work, and participate successfully in the community when they have services and supports tailored to meet their individual needs and contribute to their recovery. Effectively supporting individuals requires drawing on multiple types of federal, state and local resources. No single funding stream – including Medicaid – is sufficient to meet the varied needs of individuals with serious mental illnesses. This chapter describes public funding for services and supports, how supporting individuals in the community has evolved, and the role that Medicaid can play in addressing the needs of these individuals. |
Services for persons with serious mental illnesses have changed markedly over the past fifty years. They continue to evolve, benefiting from both solid research and a fuller appreciation of the importance of addressing more than just a person’s mental illness in order to promote successful community living. This chapter briefly describes the evolution of mental health services and the contemporary consensus regarding the constellation of services and supports that are needed to effectively support individuals in the community. Next, it identifies the funding streams that are used in supporting working-age adults with serious mental illnesses and discusses Medicaid’s important role in underwriting community services.
Evolution of Community Support
Fifty years ago, government-funded mental health services principally consisted of large state-run mental institutions, funded solely with state funds. Community-based services -- especially for low-income individuals -- were scant and not well-organized.2 First-generation antipsychotic medications that effectively relieved the psychotic symptoms of many individuals -- most notably chlorpromazine (Thorazine) -- were discovered during the mid-1950s. These medications -- coupled with litigation to end the confinement and segregation of individuals in mental institutions -- catalyzed the deinstitutionalization of thousands of individuals from state mental institutions. However, it was soon evident that communities were ill-prepared to provide the mental health care and basic life supports that many individuals needed. As a result, many people lived isolated lives in poverty, were often homeless and experienced high rates of crisis and rehospitalization.
At the urging of President Kennedy, Congress enacted the Community Mental Health Centers Act of 1963. Federal funding was provided directly to localities for the development of community mental health centers to furnish essential services, notably for the uninsured poor. This landmark legislation sparked the creation of centers around the nation that became the foundation of publicly-funded community mental health systems. The Act also was the federal governments first step in providing federal financial assistance for community mental health services. The centers were given the broad charge of furnishing mental health care -- principally in outpatient clinic settings -- to all individuals with mental illnesses, regardless of their type or severity, within their designated geographic catchment areas. Community Mental Health Centers (CMHCs) were not directed to focus exclusively on individuals with serious mental illnesses.
During the 1970s, a consensus emerged that successfully supporting community life for individuals with serious mental illnesses required the adoption of a more comprehensive approach to meeting their needs than tying services exclusively to treatment in office-based settings and outpatient clinics. While outpatient services could address the needs of many people, they had their limitations, especially with respect to individuals with serious mental illnesses. A different approach was needed to address the multiple challenges these individuals face.
In the 1970s, as a result of studies conducted by the National Institute of Mental Health and dialogue within the mental health community, the community support system (CSS) was formulated to serve as a conceptual framework for supporting individuals with serious mental illnesses who are especially reliant on mental health and other com-munity support systems to live successfully in the community. The federal Community Support Program (CSP) was launched and is now located at the Center for Mental Health Services (CMHS) in the U.S. Department of Health and Human Services Substance Abuse and Mental Health Services Administration (SAMHSA). Starting in 1977, CSP made grants to states specifically to aid development of service systems for people with serious mental illnesses. CSP also underwrote technical assistance, federally sponsored research and demonstration programs, and active networking.3
The CSS framework encompasses a core set of principles concerning the provision of services for individuals with serious mental illnesses. In particular, services should be:4
- Person-centered
- Empowering of individuals
- Ethnically and culturally appropriate
- Flexible
- Focused on a persons strengths
- Normalized and incorporate natural supports
- Tailored to meet special needs
- Coordinated
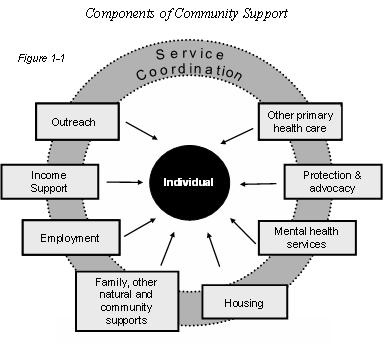
The CSS concept also identified the essential service and support components that are necessary to successfully support individuals with serious mental illnesses in the community, as illustrated in Figure 1-1.
In CSS, specialized mental health services are a critical component. However, CSS strongly emphasizes the importance of supporting individuals in the everyday world rather than confining services to fixed-site clinics and offices. CSS also points to the importance of crisis response capabilities and recognizes that individuals with serious mental illnesses frequently need supports beyond treatment and clinical services. These supports include income support and services (e.g., vocational rehabilitation) that help them obtain employment and, thereby, achieve greater independence and self-esteem. Assistance in securing community housing also is vital. CSS also underscores the critical role that peers, families, friends, and other sources of community support outside the formal service delivery system can play in helping individuals to live successfully in the community. Because CSS spans multiple types of supports, case management/service coordination is an essential feature of CSS, both to assist individuals to obtain other supports and to coordinate services.
 |
The CSS framework has had a significant influence in shaping public community mental health programs. During the late 1970s and throughout the 1980s, community support programs were started around the country. Indeed, today in some states (e.g., New York) services for individuals with serious mental illnesses who need intensive, ongoing supports are known as community support services. Early community support programs had promising results in aiding individuals to experience positive outcomes in the community.5
The past two decades have been marked by state efforts to amplify and mainstream the essential components and features of CSS in their public mental health systems. State-operated mental health facilities now typically provide short-term treatment.6 States have shifted their resources to community support, concentrating more intently on supporting individuals with serious mental illnesses.
As a result of the CSS framework, consensus exists that a comprehensive consumer-centered system of specialized mental health services for persons with serious mental illnesses should span multiple components, as Table 1-1 on the following page illustrates.7 Especially important has been the coupling of rehabilitation with treatment to assist individuals to overcome the functional limitations that stem from serious mental illnesses. Rehabilitation assists individuals to regain the essential skills that they need in order to live more independently, reduce their dependency on the service system, and build self-esteem.
| TABLE 1-1: Consumer-Centered System Components | |
|---|---|
|
|
In subsequent chapters, more information will be provided concerning the nature and scope of many of these services and supports. Not every individual with a serious mental illness requires or will use every one of these services. Rather, these components describe a constellation of services and capacities that a community system should have available in order to respond to the unique needs of each individual. An effective community support system is individually centered, capable of tailoring services to each persons needs and changing circumstances, and respectful of each persons right to make decisions concerning their services and how they are provided.
| The greatest potential for improvement does not lie in mental health systems, it lies within the individual who has faith that she or he can recover, does recover, and then shares that good news with others. Larry Fricks8 |
Recovery has emerged as an especially compelling and powerful paradigm for supporting individuals with serious mental illnesses. Recovery has its roots in the fundamental principles of the CSS concept and stresses how critical it is for people with mental illnesses to take responsibility for their lives, make decisions about their services, and achieve independence. Recovery engages and empowers individuals with serious mental illnesses to take control of their lives. Recovery shares many of the same philosophical underpinnings as the broader self-direction movement among people with disabilities of all types who are asserting greater authority over service provision and assuming personal responsibility for improving the quality of their lives.
Successfully transforming the mental health service delivery system rests on two principles:
The President's New Freedom Commission on Mental Health9 |
Also in recent years, effectively supporting individuals with serious mental illnesses has benefited from development of new pharmaceutical products for treatment of certain disorders, including the development of atypical antipsychotics for schizophrenia. Today, there is a wider array of effective medications to treat many disorders. There also have been significant strides in medication management.
Evidence-based practices (briefly described on the following page) are being identified that have demonstrated efficacy and cost-effectiveness in securing positive outcomes for individuals with serious mental illnesses.
| Evidence-Based Mental Health Practices | |
An evidence-based practice (EBP) is a method to address a condition, which meets scientific and stakeholder criteria for safety, effectiveness, and cost-effectiveness. EBPs translate research findings into practice. The deployment of EBPs is widely regarded as central to improving health care quality. EBPs have been developed and are being researched across a broad spectrum of health services.10 There are now six recognized11 adult mental health EBPs12:
|
The principles of recovery and the emergence of evidence-based practices are exerting strong influence on the provision of public community mental health services. For example, the New York State Office of Mental Health has launched a major initiative, entitled Winds of Change, to incorporate evidence-based practices into its system.16 Many other states also have launched initiatives to introduce and amplify the use of evidence-based practices in their community mental health systems. SAMHSA and the Robert Wood Johnson Foundation are co-leading a nationwide effort to promote the application of evidence-based practices. Georgia has revamped its coverage of Medicaid mental health services to embrace the essential principles of recovery by redefining its array of services and including more peer oriented approaches.17 Ohio has strongly emphasized recovery as well. Other states are engaged in similar efforts.
In summary, the CSS framework had a major influence on public mental health systems. In the case of working-age adults with serious mental illnesses, public systems are frequently designed to: (a) address multiple dimensions in supporting individuals with serious mental illnesses in the community, stressing not only treatment but rehabilitation and other community living dimensions; (b) organize around meeting each persons unique needs; and, (c) focus on recovery. The translation of science to service is leading to the adoption of evidence-based practices that promise to improve the value of community mental health services. A robust community mental health system promotes both positive outcomes for people with serious mental illnesses and pays substantial dividends in the form of reduced state, local and private costs due to hospitalization and incarceration.
 |
States are at different stages in their capabilities to support individuals in the community. Many face major challenges in marshaling the resources necessary to meet the needs of working-age adults with serious mental illnesses in the community. This is why the funding of mental health services is a major issue nationwide and why the Medicaid program is increasingly important.
Funding the Constellation of Community Services
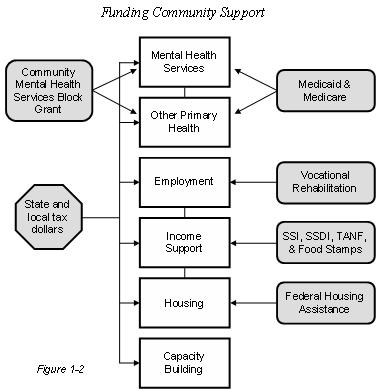
Supporting low-income working-age adults with serious mental illnesses in the community involves not only furnishing them with effective mental health services but also addressing other important needs, including housing, jobs, other primary health care, and income assistance. Funding the constellation of services that comprise a comprehensive array of community support is challenging because it requires tapping a variety of federal, state, and frequently, local resources, as illustrated in Figure 1-2.
Resources for community support flow through many federal and federal-state programs and funding streams.18 State and, often, local tax dollars also underwrite the full spectrum of services and supports. States and localities (in some states) match federal Medicaid and other federal funds (e.g., for vocational rehabilitation). There are a wide variety of federal housing assistance programs; here too, states and localities often provide significant funding. With respect to income support, working-age adults with serious mental illnesses frequently receive federal benefits such as Supplemental Security Income (SSI) and Social Security Disability Insurance (SSDI). Some states supplement these benefits.
The federal Medicare program pays for some mental health services (discussed in Chapter 4) and, in the case of individuals who are eligible for both Medicare and Medicaid (discussed in Chapter 3), also underwrites other primary care. The joint federal-state Medicaid program is a critical source of funding for both basic primary health services and for mental health services for low-income working-age adults with serious mental illnesses. Through the federal Community Mental Health Services Block Grant program, states receive flexible formula-based grants to fund community mental health services. The Mental Health Block Grant program is the single largest federal contribution dedicated toward improving mental health service systems across the country.19 Block grants have played an important role in capacity building by enabling states to target dollars to special populations and underwrite the development of new services. Annual block grant funding accounts for less than two percent of total public mental health services outlays nationwide.
Numerous challenges inhibit the development of effective strategies for combining federal, state, and local funding for community mental health services to support individuals. As observed in a report to the Presidents New Freedom Commission on Mental Health:
A coordinated system that addresses the needs of people with mental illnesses must include a comprehensive range of mental health services including ancillary supports such as housing, vocational rehabilitation, education, substance abuse treatment, income support, and other basic services. While federal funds are potentially available to individuals, states, localities, or public and private providers, most of the federal programs that contribute funding to the current mental health system are designed to address broadly defined human needs rather than serving the specific needs of adults with serious mental illnesses or children with serious emotional disturbances.20
A major challenge in marshaling resources to meet the varied needs of working-age adults with serious mental illnesses is that federal and state programs are often structured as funding silos with their own unique rules and requirements, which makes coordination difficult at both the system and service delivery levels.21 The Presidents New Freedom Commission on Mental Health identified funding fragmentation as a major barrier to effectively supporting individuals with mental illnesses. To address this barrier, the Commission recommended that states develop and implement comprehensive mental health plans to promote a unified approach to system planning and management at the state level.22
Medicaid and Community Services: Opportunities and Boundaries
The federal-state Medicaid program is an especially important source of funding for community mental health services. The program offers states the opportunity to secure federal dollars to strengthen and expand community services. The Medicaid rehabilitative services option is particularly important in underwriting services that contribute to the recovery and independence of working-age adults with serious mental illnesses. At the same time, there are boundaries that circumscribe the use of Medicaid to underwrite some types of services.
Opportunities
Medicaids role in paying for mental health services has grown considerably over the years. In 1997, it accounted for about 20 percent of all behavioral health spending23 and 35 percent of all public mental health expenditures.24 Medicaid is the single largest payer of public mental health services and is expected to play an even larger role in underwriting these services in the future.25
Medicaid plays a critical role in supporting working-age adults with serious mental illnesses. About 1.2 million working-age adults with mental disorders (excluding mental retardation) receive SSI benefits.26 These individuals are nearly universally eligible for Medicaid and include those who rely heavily on mental health services.
Federal Medicaid law does not spell out a defined set of mental health services or benefits. However, the Medicaid program includes certain basic coverage options (e.g., targeted case management, clinic and rehabilitative services) through which a state may elect to offer community mental health services as part of its Medicaid program. Medicaid permits states to provide a wide-range of critical community mental health services, including evidence-based practices such as ACT, and important recovery-oriented services such as peer support. While some Medicaid benefits include psychiatric services (e.g., short-term hospitalization), none are specifically defined as mental health services.
| All available evidence shows that Medicaid has made enormous contributions to expanding access to mental health care for low-income populations. It also has expanded consumer choice for low-income people with mental disorders and has promoted community-based treatment for people with mental and addictive illnesses. Mental health care in the United States is unquestionably better because of the Medicaid program than it was thirty-five or even fifteen years ago.27 |
As will be described in greater detail in Chapter 4 and Chapter 5, many states have successfully incorporated a wide variety of community mental health services into their Medicaid programs. As states have concentrated more and more on supporting individuals with serious mental illnesses in the community and have adopted the CSS framework in their public systems, they have shifted away from employing the more circumscribed, outpatient treatment-oriented clinic option coverage in favor of using the more robust and flexible rehabilitative services option. Moreover, the scope of services that states are furnishing under the rehabilitative services option has broadened, thereby improving system capabilities to better respond to individual needs.
For example, from 1971 through 1993, California relied on the clinic option to underwrite public mental health services. But, under the clinic option, services had to be directed by a physician, provided mainly in a clinic, and focused primarily on the treatment of the mental disorder. In 1993, the state adopted the rehab option because services can be directed by licensed mental health practitioners (not just physicians) and may be provided almost anywhere in the community, and may be focused both on the treatment of the mental disorder and the associated functional limitations that may jeopardize community living.28
Federal law gives states the flexibility to align their Medicaid mental health coverages to their broader system goals and objectives. Medicaid is very much a state-shaped program. In the case of community mental health services, this is especially the case because federal policy gives states considerable latitude within broad guidelines in selecting the services that they offer. For example, states have extensively shaped the rehabilitation option, broadening its scope and securing coverage of important services such as peer supports and ACT. In addition, as will be discussed in Chapter 6, states also have the flexibility to adopt alternative service delivery models under Medicaid, including managed care models.
In many respects, the Medicaid program is best understood as a financing tool that enables states to obtain federal financial participation in the costs of services they elect to furnish and which comport with federal statutory and regulatory parameters. Federal Medicaid policy does not dictate a states service system goals and objectives. It sets parameters that determine whether the costs of services will qualify for federal funding. Medicaids contribution to underwriting community services for individuals is heightened when a states Medicaid coverages and core services are in close alignment.
Boundaries
Even though Medicaid helps fund mental health services -- especially on behalf of low-income individuals who have the most intensive need for services -- the Medicaid program cannot provide all the services and supports that beneficiaries with serious mental illnesses require in order to live successfully in the community. Medicaid is principally a purchaser of mental health and other primary health services, and with respect to mental health services, there are fundamental boundaries concerning the types of services that Medicaid may purchase. These boundaries have their roots in basic provisions of federal Medicaid law. While these boundaries often are less constraining than sometimes believed, it is nonetheless the case that not every service or support can -- or should -- be covered under Medicaid. Employing Medicaid to underwrite mental health services involves finding the fit between the services and supports that a state has identified as critical to meeting the needs of individuals with serious mental illnesses and Medicaid program requirements (as discussed in Chapter 5).
Medicaid-funded community mental health services have evolved along different lines than home and community services for individuals with other disabilities.29 Because federal Medicaid law prohibits the coverage of services in Institutions for Mental Disease (IMDs) that have more than 16 beds (the IMD exclusion is discussed in detail in Chapter 4), most states have not used the Medicaid home and community-based services waiver program to support working-age adults with serious mental illnesses. Instead, states employ Medicaid state plan services and other federal waiver authorities to support individuals in the community.
The principal boundaries that circumscribe the extent to which Medicaid can be employed to underwrite community mental health services include:
- Eligibility. Medicaid services can be provided only to individuals who meet a states Medicaid eligibility criteria. States have latitude in establishing these criteria (as discussed in Chapter 3). Medicaid is a means tested program; in addition to meeting financial eligibility criteria, individuals with disabilities must also meet service eligibility criteria, which typically are based on functional limitations. The proportion of working-age adults with serious mental illnesses who qualify for Medicaid in a state depends on each states eligibility policies for adults with disabilities of all types. Medicaid eligibility rules can mean that some individuals with relatively low incomes may not qualify for Medicaid even though they have a serious illness. Individuals who do not qualify for Medicaid must be supported through other state and local resources.
- Housing. Medicaid does not pay for housing. Except for certain institutional settings, Medicaid dollars generally cannot be used to pay for room and board or the routine living expenses of individuals. Medicaid, however, can finance services that are furnished in community residences or in a persons own living arrangement, including the family home.
- Vocational Services. Medicaid law does not permit states to obtain federal financial participation in the costs of job-specific vocational training, except under a waiver program (see Chapter 6), since the costs of such training may be underwritten with federal-state vocational rehabilitation dollars and/or state and other dollars. Medicaid dollars can be used to underwrite the costs of job-related rehabilitative, pre-vocational and personal assistance services (see Chapter 5). In addition, states may craft eligibility policies that enable people with disabilities to maintain Medicaid coverage when they obtain employment (see Chapter 3).
- Capacity Building. Medicaid is designed to pay for services provided to eligible individuals. Medicaid funding is not available to underwrite the costs of starting up services. For example, in Michigan there is an especially robust network of ACT teams in place around the state. Michigan officials regarded the creation of this network as vital in order to minimize costly hospitalizations. The state used community mental health services block grant dollars to start up these teams. Once the teams were operational, they qualified for and began receiving Medicaid funding to sustain their ongoing operation.30 Capacity building frequently requires the investment of state, local and private resources. The Community Mental Health Block Grant also has been an important resource for states to launch services that later could qualify for Medicaid funding.
Just as the provision of treatment services alone are not sufficient to promote community living for individuals with serious mental illnesses, Medicaid funding by itself is insufficient to meet many fundamental and diverse needs. Medicaid is a powerful, important contributor to the provision of mental health services and other primary health care for individuals. But, Medicaid funding must be employed in tandem with other federal, state, and local funding sources in order to comprehensively address the full range of supports that working-age adults with serious mental illnesses require to live successfully in the community. As recommended by the Presidents New Freedom Commission on Mental Health, it is important that states develop comprehensive mental health plans that take a broad view of how Medicaid along with other federal and state programs can work together to support individuals with mental illnesses.
Conclusion
CSS has proven to be an important framework for successfully supporting working-age adults with serious mental illnesses in the community. The principles of recovery build on the CSS framework while also emphasizing empowerment and individuals taking control of their lives. State public mental health systems have focused on enhancing their community service systems and capabilities to support individuals with serious mental illnesses.
Medicaid plays an important role in underwriting community mental health services. Medicaid also provides a means for states to leverage their own dollars to enhance and expand community services in order to advance their goals and objectives for supporting working-age adults with serious mental illnesses in the community. To be successful, Medicaid must be used in tandem with other federal, state and local funds to address the full range of individual needs across the many dimensions of community life.
Since Medicaid can play a vital role in supporting individuals, it is important to have a clear understanding of the program. Chapter 2 provides a description of the essential features of the Medicaid program.
Annotated Bibliography
The following are especially useful resources for obtaining more information about many of the topics addressed in this chapter. Resources about Medicaid are identified in the following chapters.
U.S. Department of Health and Human Services. (1999). Mental Health: A Report of the Surgeon General. U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services, National Institutes of Health, National Institute of Mental Health, Rockville, MD: Author. (458 pages)
In 1999, the Surgeon General of the United States, in collaboration with SAMHSA and NIMH, released this groundbreaking, comprehensive report. The report covers a wide range of topics, including state-of-the-art information on serving individuals of all ages. Particularly relevant chapters include Adults and Mental Health and Organizing and Financing Mental Health Services. In 2001, the Surgeon General issued a follow-up report entitled Mental Health: Culture, Race and Ethnicity, A Supplement to Mental Health: A Report of the Surgeon General. The 1999 report may be obtained at www.surgeongeneral.gov/library/mentalhealth/home.html. The 2001 report may be accessed at www.surgeongeneral.gov/library/mentalhealth/cre/.
Presidents New Freedom Commission on Mental Health. Achieving the Promise: Transforming Mental Health Care in America. DHHS Pub. No. SMA-03-3832. Rockville, MD: 2003
Established in April 2002, the Presidents New Freedom Commission on Mental Health was charged with assessing the status of mental health services and developing policy recommendations at the federal, state, and local levels regarding effective implementation of community-based mental health care, resource development, and general treatment of adults with a serious mental illness and children with a serious emotional disturbance. The Commissions final report was released in August 2003 and contains a series of findings that identify major problems in mental health policy, especially system fragmentation. The report contains numerous recommendations for improving the provision of community services and supporting community living for children and adults. The report may be obtained at www.mentalhealthcommission.gov/reports/reports.htm.
Frank, R., Goldman, H., & Hogan, M. (2003). Medicaid and Mental Health: Be Careful What You Ask For. Health Affairs 22(1): pp. 101-113.
This article traces the historical relationship between Medicaid and mental health services, highlighting the increasing role that Medicaid has taken as a funder of public mental health services and supports. The authors discuss the major factors leading to this rising Medicaid role, such as the deinstitutionalization movement and cost-shifting efforts by states. The article cautions about the effects of over reliance on Medicaid funding.
Carol Bianco and Susan Milstrey Wells (eds.) (2001). Overcoming Barriers to Community Integration for People with Mental Illnesses. Rockville MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Administration, Center for Mental Health Services. (68 pages).
This report describes many of the barriers that people with mental illnesses face in the community. It discusses funding streams that cross several dimensions of community living. The report may be obtained at www.olmsteadcommunity.org/OvercomingBarriers.pdf.
Web Resources
Substance Abuse and Mental Health Services Administration/Center for Mental Health Services
www.samhsa.gov/centers/cmhs/cmhs.html
The Center for Mental Health Services at SAMHSA web site contains extensive information on all elements of the Community Support Program as well as a wide variety of other information about mental health services. The site also has Resource Kits for the implementation of evidence-based practices, containing resources specifically geared to consumers, family and friends, mental health program leaders, public mental health authorities, and clinical practitioners.
National Association of State Mental Health Program Directors (NASMHPD)
www.nasmhpd.org/
- NASMHPD Research Institute (NRI)
nri.rdmc.org/ - National Technical Assistance Center for State Mental Health Planning (NTAC)
www.nasmhpd.org/ntac.cfm
NASMHPD identifies public mental health policy issues, apprises its members of research findings and best practices in mental health service delivery, fosters collaboration, provides consultation and technical assistance, and promotes effective management practices and financing mechanisms. The NASMHPD site contains information about each of its six divisions (adults, attorneys, children, consumers, forensics, medical directors, older persons and state hospitals), explanations of its position on various mental health issues (i.e., the IMD exclusion), and updates on new mental health policies. NRI compiles extensive information about individual state mental health systems (including system capabilities and the use of Medicaid funding by states). NTAC has developed numerous policy resources, tool kits, and other materials.
National Association for Mental Illness (NAMI)
www.nami.org/
NAMI is a leading advocacy and public policy organization for individuals with mental illness. There are approximately 1,000 state and local NAMI affiliates nationwide. The web site offers information on mental illness and its history, recommended treatment, policy alternatives in support of individuals and families coping with mental illness, and statistics.
National Mental Health Association (NMHA)
www.nmha.org/
NMHA is a nonprofit organization that addresses all aspects of mental health and mental illness. It has more than 340 affiliates nationwide. NMHA works to improve the mental health of all Americans, especially the 54 million people with mental disorders, through advocacy, education, research and service. Its web site contains a wide variety of information concerning mental health services.
Bazelon Center for Mental Health Law
www.bazelon.org/
The Bazelon Center advocates for the rights of people with mental disabilities. Its web site contains a host of materials concerning mental health services and related topics such as housing. The Center also has prepared numerous publications concerning Medicaid and public mental health systems.
Endnotes
-
Cille Kennedy contributed to the preparation of this section.
-
The 1954 New York State Community Care Act was the first venture by a state to furnish services to individuals with serious mental illnesses in the community. The Act provided that state mental hospital psychiatrists could continue to provide services to individuals who had been discharged from hospitals to the community.
-
Virginia Mulkern (1995). The Community Support Program: A Model for Federal-State Partnership. Washington DC: Mental Health Policy Resource Center. Early Community Support Program (CSP) efforts included funding for statewide planning and system building in eight states along with funding to establish demonstration programs. In 1980, CSP funding was modified to give states more flexibility in employing funds for infrastructure and system development. By 1984, all 50 states and the District of Columbia had received strategy development grants. Funds also were earmarked to conduct studies of homelessness and demonstration programs to provide services to homeless individuals. Later on, funding was earmarked for demonstrations involving services for older persons, young adults with co-occurring conditions, consumer-operated services, and supportive housing. Funds also supported statewide system improvement, consumer and family support activities, and research demonstrations.
-
Ibid.
-
Ibid.
-
A notable exception is their responsibility to serve individuals committed by the courts.
-
Adapted from: Bazelon Center for Mental Health Law (2002). An Act Providing for a Right to Mental Health Services and Supports: A Model Law. Washington, DC.
-
Remarks by Larry Fricks, Director, Office of Consumer Relations, Georgia Department of Human Resources, December 13, 1999 at the White House for the Unveiling of the Surgeon General 's Report on Mental Health.
-
Presidents New Freedom Commission on Mental Health (PNFCMH). Achieving the Promise: Transforming Mental Health Care in America. DHHS Pub. No. SMA-03-3832. Rockville, MD: 2003.
-
In health, the fundamental precepts of EBP emerged roughly a decade ago. In the United States, the Institute of Medicine has been a central force in promoting the development and implementation of EBPs (see especially, Committee on Quality of Health Care in America (2002). Crossing the Quality Chasm. Institute of Medicine). The Agency for Health Care Policy and Research at the U.S. Department of Health and Human Services has lead responsibility for promoting evidence-based practice in everyday care.
-
These practices were identified by a consensus panel sponsored by the Robert Wood Johnson Foundation (RWJF). This panel was composed of researchers, families, individuals with mental illnesses and mental health administrators. Funding from RWJF, SAMHSA and other sources is underwriting the preparation of materials by the New Hampshire-Dartmouth Psychiatric Research Center in collaboration with several other organizations in order to facilitate and accelerate the implementation of EBPs by agencies and mental health systems. Implementation Resource Kits have been prepared for each practice for use by administrators, program directors, practitioners, individuals with mental illnesses, and families. These toolkits are designed to promote interest in the use of these practices, facilitate their adoption, and provide tools (fidelity measures) to assess if the practice is being used consistently. These kits are located at www.mentalhealth.org/cmhs/communitysupport/toolkits
-
Unless otherwise specified, all the descriptions of evidence-based practices summarize materials included in: the 2002 draft toolkits, materials disseminated by the New York State Office of Mental Health via its web site, and the 1999 Surgeon Generals Report on Mental Health.
-
There are extensive materials concerning ACT that are available from the National Alliance for the Mentally Ill (NAMI), which has been a leading advocate for the expanded availability of ACT nationwide. NAMI employs the acronym PACT (Program for Assertive Community Treatment). NAMI also has exercised leadership in the development of standards for ACT. For more information, go to: www.nami.org/about/pact.htm
-
NAMI Issue Spotlight: Employment and Income www.nami.org/Template.cfm?Section=Issue_Spotlights&template=/ContentManagement/ContentDisplay.cfm&ContentID=13158
-
PNFCMH (2003), op cit
-
New York State Office of Mental Health (2002). OMH Introduces Winds of Change. Available at www.omh.state.ny.us/omhweb/omhq/q0302/Wind.htm
-
Personal communication: Larry Fricks and Wendy White-Tiegreen, Georgia Department of Human Resources.
-
The federal and state-federal programs identified in the graphic are not exhaustive. For example, there are additional federal programs that furnish targeted dollars to support homeless individuals and families, including individuals with serious mental illnesses. A complete listing and discussion of federal and state-federal programs that play a role in meeting the needs of individuals (children and adults) with mental illnesses is contained in Major Federal Programs Supporting and Financing Mental Health Care (January 2003), prepared on behalf of the Presidents New Freedom Commission on Mental Health, available at www.mentalhealthcommission.gov/reports/Fedprograms_031003.doc.
-
Ibid.
-
Ibid.
-
Ibid. See also: Carol Bianco and Susan Milstrey Wells (eds.) (2001). Op. cit.
-
PNFCMH (2003). Op. cit.
-
Behavioral health includes mental health and substance abuse services.
-
Coffey, Mark, King, et al. (2000). National Estimates of Expenditures for Mental Health and Substance Abuse Treatment 1997. Rockville MD: Substance Abuse and Mental Health Services Administration, U.S. Department of Health and Human Services. (SAMSHA Publication SMA-00-3499).
-
Jeffrey A. Buck (2003). Medicaid, Health Care Financing Trends, and the Future of State-Based Public Mental Health Services. Psychiatric Services, Vol. 54. No.7.
-
Social Security Administration. 2002 Annual Statistical Supplement, Social Security Bulletin.
-
Frank, R., Goldman, H., & Hogan, M. (2003). Medicaid and Mental Health: Be Careful What You Ask For. Health Affairs 22(1): pp. 101-113.
-
California Department of Mental Health (1999). Frequently Asked Questions About Systems of Care, Medicare and Medi-Cal.
-
In particular, states have used the Medicaid home and community-based services (HCBS) waiver program extensively to underwrite home and community services for individuals of all ages with all types of disabilities, except individuals with disabilities due to mental illnesses. For individuals with developmental and other disabilities, states may offer HCBS as an alternative to services in a Medicaid-reimbursable institutional setting (nursing facilities or ICFs/MR).
-
Glenn Stanton, CMS, personal communication.
CHAPTER 2: ESSENTIAL FEATURES OF THE MEDICAID PROGRAM
| Medicaid is a very large, complex, multi-faceted federal-state program. Through the program, states and the federal government each year underwrite health and long-term services for about 51 million low-income children and adults. This chapter describes the essential features of the Medicaid program. It is principally intended for readers who may not be familiar with the programs basic features. |
Medicaid is a joint federal-state program that provides health and long-term services to low income adults and children, including people with disabilities. About one out of every seven of our nations citizens obtains health care that is funded through Medicaid.1 In 2003, state-federal Medicaid expenditures totaled $259.6 billion, an increase of more than 50 percent since 1997.2 Federal funds account for more than one-half of total expenditures. Medicaid ranks second only to Medicare in federal health care outlays; it also is the single largest source of federal financial aid to states. At the state level, only spending for elementary and secondary education exceeds state tax dollar expenditures for Medicaid.
Medicaid is multi-faceted. It not only provides access for low-income individuals to essential health care but also pays for more than one-half of all long-term services for older persons and people with disabilities. As noted in Chapter 1, Medicaid is playing an increasingly important role in underwriting critical services and supports for working-age adults with serious mental illnesses.
This chapter provides basic background information concerning the nuts and bolts of Medicaid, including its history, the nature of the programs federal-state relationship, eligibility, benefits, and other topics. The annotated bibliography lists additional resources that contain more in-depth information concerning Medicaid. Later chapters delve more deeply into facets of Medicaid that are most directly related to supporting working age adults with serious mental illnesses in the community.
A Brief History of Medicaid
Medicaid (Title XIX of the Social Security Act) was created in 1965 in tandem with the Medicare program (Title XVIII).3 The Medicare program is a federally funded and administered health insurance program for retirees, disabled workers, and their spouses and dependents. In contrast, Medicaid is a joint federal-state program through which states, the District of Columbia and the territories receive federal financial participation in their costs of furnishing health and long-term services to federally recognized groups of low-income families and individuals.
Before Medicaid was enacted, limited federal payments were made to states for health care services they purchased on behalf of public assistance recipients. In 1960, Congress authorized open-ended federal matching payments to states for health care provided to indigent older persons.4 Still, in the early 1960s, states varied widely in the scope of the health care services they funded for low-income individuals and families.
Medicaid was designed to expand access to mainstream health care for low-income individuals and families. The federal government would make payments to states to pay for half or more of their costs in furnishing services to beneficiaries. At the same time, the program was framed to give states considerable latitude in fashioning their medical assistance programs. States that elected to participate in the program were required to furnish a core set of basic health services to public assistance recipients. They were also allowed to offer additional services at their option and could elect to serve medically needy individuals who did not receive public assistance. Then, as now, the Medicaid program combined federal mandates and state-selected options with respect to who receives services and what services are offered.
The past four decades have seen many changes in federal Medicaid law, including significant modifications in eligibility, benefits, payment arrangements, and other administrative details. The cumulative effect of these changes -- combined with state decisions regarding the scope of their programs -- has been to expand Medicaid well beyond its original focus on furnishing principally acute care services to public assistance recipients. In addition, Medicaid has become the dominant funder of long-term services for people with disabilities. Despite the myriad changes in federal law, the fundamental nature of the programs federal-state relationship has not changed appreciably.
From 1965 to 1980, federal Medicaid law changed in a variety of ways. In 1972, the Supplemental Security Income (SSI) program was created. This federally-funded income assistance program for people with disabilities replaced the preceding federal-state aged, blind and disabled cash assistance programs. Medicaid eligibility was linked to SSI eligibility.5 Other changes during this period included adding the 1967 requirement6 that states operate Early and Periodic Screening, Diagnosis and Treatment (EPSDT) programs for children and giving states the option to cover Intermediate Care Facilities for the Mentally Retarded (ICFs/MR).7
The 1980s saw many expansions in both mandatory and optional eligibility groups, especially focused on extending Medicaid benefits to low-income pregnant women and children who do not receive public assistance payments.8 The Omnibus Budget Reconciliation Act of 1981 (OBRA-81)9 required that states make additional Disproportionate Share Hospital (DSH) payments to hospitals that serve especially large numbers of Medicaid and other low-income individuals. OBRA-81 also added two new important waiver authorities. In particular, Section 1915(b) of the Social Security Act gave states greater latitude to employ managed care and other care management approaches in their programs. The addition of §1915(c) allowed states to launch home and community-based services (HCBS) waiver programs to provide a wide range of services -- including those not covered under the Medicaid state plan -- to assist individuals with disabilities who otherwise require institutionalization to remain in the community.
The Omnibus Budget Reconciliation Act of 198710 included nursing home reform provisions to bolster protections for nursing facility residents, including requirements for additional screening and treatment of individuals with mental illnesses. In 1989, Congress revised and strengthened the EPSDT program to mandate that states furnish all medically necessary services to eligible children.11
The 1990s saw more changes in the program. The Personal Responsibility and Work Opportunities Act (PRWOA) of 199612 (otherwise known as welfare reform) severed the historical link between Medicaid eligibility and the Aid to Families with Dependent Children (AFDC) cash assistance program. The AFDC program was replaced by the Temporary Assistance to Needy Families (TANF) block grant program. A new mandatory Medicaid eligibility group was established for low-income households; eligibility for Medicaid was no longer automatically tied to receipt of public assistance cash payments.13 The passage of PRWORA also included major changes in eligibility for legal immigrants.14
In 1997, the State Childrens Health Insurance Program (SCHIP) was created to offer states additional funding to extend Medicaid services to children in low-income households or provide them an alternative package of benefits.15 The 1990s also saw limits imposed on DSH payments as well as states use of provider taxes and donations to capture additional federal dollars.16 Also in 1997 and 1999, Congress changed Medicaid law to permit states to continue Medicaid benefits for workers with disabilities who are no longer eligible for SSI (these provisions are discussed in more detail in Chapter 3).17
An especially noteworthy development during the 1990s was the expanded use of managed care arrangements in Medicaid. In 1996, about 40 percent of Medicaid beneficiaries nationwide were enrolled in managed care; by 2003, the figure had climbed to more than 59 percent.18 This shift to managed care delivery systems also significantly affected Medicaid mental health services in many states. Chapter 6 discusses Medicaid managed care service delivery arrangements in more depth.
In the Balanced Budget Act of 1997, Congress gave states new options to implement managed care approaches without having to seek special waivers. The 1990s also saw expanded state use of the Social Security Acts Section 1115 Research and Demonstration waiver authority in conjunction with state initiatives to extend health care to uninsured individuals previously ineligible for Medicaid.
Most recently, states have been allowed to employ the Section 1115 waiver authority to extend services on a targeted basis to low-income uninsured individuals and families who would otherwise not qualify for Medicaid. Also, states are encouraged to employ the waiver authority to test alternative service delivery approaches. Finally, through the Presidents New Freedom Initiative, federal policies are being clarified to encourage states to promote community living for people with disabilities of all ages, including the expanded use of consumer-directed approaches in long-term services and supports (discussed in Chapter 7).
Since its enactment, federal Medicaid law has been modified many times. Federal mandates have increased, especially in the area of services for low-income children. However, the effect of most changes has been to expand the options available to states in designing and administering their Medicaid program. Today, states may offer a wider range of Medicaid services to a broader range of low-income children and adults. States retain considerable flexibility in crafting their Medicaid programs, a principle inherent in Medicaid from its beginning.
The combination of Medicaid mandates and options has resulted in the emergence of 51 highly distinctive Medicaid programs that operate under broad national guidelines but have been shaped by state decisions about who is eligible and what they are eligible to receive.
Changes in federal Medicaid law and policy have been beneficial for people with disabilities, including working-age adults with serious mental illnesses. They have permitted states to employ Medicaid to support people with disabilities in the community. However, as emphasized in Chapter 1, Medicaid cannot meet all the needs of people with serious mental illnesses across all dimensions of community living.
Medicaid and Working-Age Adults with Disabilities
Medicaid plays an especially important role in supporting low-income people with disabilities, including working-age adults with serious mental illnesses. There are about seven to eight million Medicaid beneficiaries with disabilities (about 19 percent of all beneficiaries). An estimated 30 percent of children with chronic conditions and 15 percent of adults with chronic disabilities are Medicaid beneficiaries.20 In 2002, Medicaid beneficiaries with disabilities accounted for an estimated 43 percent of all Medicaid outlays. As a group, people with disabilities account for the largest proportion of Medicaid expenditures; in contrast, children comprise about 50 percent of beneficiaries but account for only 18 percent of total outlays.
Essential Features of Medicaid
Medicaid has several essential, fundamental features. These features are described here briefly in the context of the basic Medicaid program. Some of these features may be altered by waivers of federal Medicaid law that states may obtain. The final section of this chapter briefly describes the three waiver authorities that are included in federal law and their effect on the features described here.
Federal-State Relationship
Medicaid was originally structured as and remains a cooperative federal-state venture through which the federal government financially assists states in providing medical assistance, rehabilitative and other services to eligible low-income individuals and families. Within broad national guidelines contained in federal law, regulations and other policies, states obtain federal financial participation in their costs of furnishing services to low-income individuals and families. This federal-state relationship is a cornerstone of Medicaid. Federal policy dictates that states observe fundamental guidelines but in large part allows them to determine the scope of their programs.
Medicaid is very much a state-shaped program. Therefore, each Medicaid program looks and operates very differently. The design of a Medicaid program is based on each states demographics, health policy goals, objectives, needs, and financial capabilities. States are responsible for: (1) establishing eligibility standards within federal parameters; (2) setting the type, amount, duration, and scope of services; (3) determining payments for Medicaid services; and (4) administering the program.
Each state spells out its Medicaid program in a Medicaid state plan.21 The state plan specifies the eligibility groups that the state serves, the benefits provided, and other aspects of how the state operates its program. Each states plan (and amendments to the plan) must be approved by the federal Centers for Medicare and Medicaid Services (CMS; formerly, HCFA -- Health Care Financing Administration) at the U.S. Department of Health and Human Services. The CMS Center for Medicaid and State Operations (CMSO) has lead federal responsibility for Medicaid. There are ten CMS Regional Offices located around the country, which are responsible for reviewing and approving most proposed changes in each states Medicaid program, and assuring that they operate in compliance with the approved state plan, applicable federal regulations, and other CMS program guidance.22
Federal law dictates that each state designate a single state Medicaid agency (SSMA) that is responsible for the administration of its program. The SSMA has responsibility for the implementation of the state plan. The SSMA may not delegate its responsibilities to another state agency, although it may enter into cooperative agreements with other state agencies to administer certain aspects of the program under the supervision of the SSMA. This topic is discussed in Chapter 7.
Federal law concerning the Medicaid program is in Title XIX of the Social Security Act.23 Federal regulations governing the program are located in Parts 430 et seq. of Title 42 of the Code of Federal Regulations (CFR).24 Additional federal guidance concerning the operation of Medicaid programs is contained in the State Medicaid Manual25 as well as letters, memoranda and technical assistance guides issued by CMS from time-to-time.26
Federal Payments to States
The amount of money that each state receives for Medicaid services is determined by the Federal Medical Assistance Percentage (FMAP). This percentage is applied to state expenditures for services that are furnished to eligible individuals. The resulting federal payment to a state is termed federal financial participation. The FMAP is calculated each year by comparing a states average per capita income level with the national average. The higher a states per capita income, the lower its FMAP. However, the minimum FMAP is 50 percent and the maximum is 83 percent.27 The average FMAP across all states is about 57 percent, meaning that for every dollar spent on Medicaid services, the states provide 43 cents.
Because Medicaid is an entitlement program, federal financial participation in the cost of Medicaid services is contributed on an open-ended basis -- i.e., there is no cap on federal payments to states for Medicaid.28 States manage their Medicaid expenditures by selecting covered benefits, eligibility parameters, payments, and other methods.
States must provide matching dollars from their own public funds or a combination of their own funds and local tax dollars.29 In some states (e.g., New York), counties are required to provide a portion of the states matching fund obligation.
Under federal law, Medicaid is termed a payor of last resort. With a few exceptions, Medicaid payment is only available if no other funding sources are able to pay for a service provided to a beneficiary. If, for example, a beneficiary also has employer health insurance, Medicaid payment is only available to the extent that the service is not covered by that health insurance. States are required to seek third-party payments whenever feasible.
States can also claim matching federal dollars for the costs associated with the administration of the Medicaid program. Functions that are eligible for such funding include day-to-day program administration and the costs of processing and paying claims submitted by providers for services furnished to beneficiaries. The base rate of federal financial participation in state Medicaid administrative costs is 50 percent. However, higher rates are available for certain activities, including the development and operation of automated Medicaid claims processing systems. Chapter 7 discusses how federal financial participation in administrative costs can be used to strengthen the provision of Medicaid services to working-age adults with serious mental illnesses.
Eligibility Groups
Federal Medicaid law includes more than fifty distinct eligibility groups to which states may offer Medicaid services -- some mandatory and most optional. These groups are defined by income and resource tests and, in some cases, disability or other tests. Eligibility groups are also classified as categorically needy or medically needy. The latter comprises persons whose income is too high to qualify for Medicaid but, at state option, can spend down their excess income to become eligible.
An individual qualifies for Medicaid by being a member of a federally-recognized eligibility group that a state includes in its plan and by meeting the income and resource tests associated with the group, as spelled out by the state. Being a low-income person does not automatically translate into Medicaid eligibility. For example, low-income childless adults without disabilities cannot qualify for Medicaid unless the state operates a waiver program covering this population. As seen in Figure 2-1 on the following page,30 children comprised about one-half of all Medicaid beneficiaries in 2003, with older adults and people with disabilities together making up only about 30 percent of beneficiaries.31 Chapter 3 discusses Medicaid eligibility in greater detail and how it relates to adults with serious mental illnesses.
Beneficiary Cost Sharing
Depending on how they are eligible for Medicaid and the particular state in which they live, categorically eligible beneficiaries may be required to pay nominal deductibles, coinsurance or co-payments in order to receive services. States have some discretion to decide who will pay for services and how much they must pay. However, some groups are exempt from cost sharing requirements. These include: pregnant women and children under 18 at or below 100 percent of the Federal Poverty Level (FPL). Nursing home residents must make contributions toward the cost of their institutional care if they have income in excess of their personal needs allowance. In addition, states are prohibited from imposing cost sharing for family planning or emergency services. Medically needy beneficiaries also must make out-of-pocket payments for health services in order to qualify for Medicaid. Workers with disabilities who qualify under buy-in options also may be required to pay premiums if their income exceeds certain levels. Individuals and families who receive Medicaid services through a waiver, but would not otherwise qualify for Medicaid, also may be required to make premium payments.
Benefits
Just as states are required to cover certain mandatory populations in their Medicaid programs, the same is true about the scope of benefits that states offer. Under federal law, every state must offer fourteen basic mandatory services to all categorically needy eligibility groups. Above and beyond the mandatory services, a state may elect to include other optional benefits in its program. If a state elects to include an optional benefit, it is subject to the same standards regarding amount, duration and scope (discussed later) as mandatory benefits when provided to categorically needy individuals. Table 2-1 and Table 2-2 on the following page list the mandatory and optional Medicaid benefits.
With respect to many of these optional benefits, it is important to point out that states have considerable latitude in defining the specific services they offer within an optional coverage category. For example, states that employ the rehabilitative services option to support individuals with serious mental illnesses include different mixes of services under their coverages.
Except for institutional services for children and youth under age 22 and older persons age 65 and above, federal law does not delineate a distinct set of mental health benefits. Such benefits are furnished under the broader mandatory and optional coverage categories. For example, medications fall under the prescribed drugs category. States provide mental health services to working age adults with serious mental illnesses under the clinic or rehabilitative services categories; but neither category is reserved exclusively to mental health services. Medicaid coverages that are especially pertinent in supporting working age adults with serious mental illnesses are discussed in greater detail in Chapter 4 and further illustrated in Chapter 5.
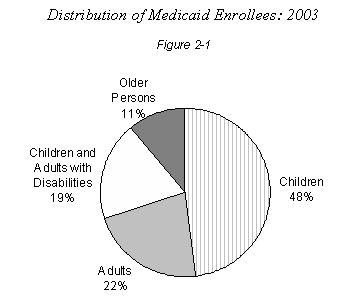 |
In the case of medically needy individuals, federal requirements regarding benefits are less prescriptive than those for the categorically needy. Just as states are required to cover certain populations to get federal matching payments for services provided under the medically needy option, they also must cover certain benefits such as prenatal and delivery care for pregnant women and ambulatory care for children. However, they are not required to provide mandatory and optional benefits to medically needy individuals at the same level as for categorically eligible individuals.
The statutory distinction between mandatory and optional services is long-standing. However, it is worth noting that about two-thirds of Medicaid spending nationwide goes toward the purchase of optional services. Some optional services (e.g., prescribed drugs) are offered by every state. About 83 percent of spending on optional services is for services for people with disabilities and older persons.32
| TABLE 2-1: Mandatory Medicaid Benefits | |
|---|---|
|
|
| TABLE 2-2: Optional Medicaid Services | |
|---|---|
|
|
Medical Necessity
In the Medicaid program, states are responsible for developing their own medical necessity criteria. Often these criteria are embedded in states' limitations on the amount, duration, and scope of services. Medicaid beneficiaries are entitled to covered services that are medically necessary to meet the person's needs. A state may deny payment for a service that is not considered medically necessary even if it arguably falls under a state benefit. Depending on a state's definition, this could occur if an individual's diagnosis does not warrant such an intense level of treatment (even if the treatment is generally covered by the state). For example, states often limit the provision of Medicaid mental health rehabilitative services to individuals whose mental illness has resulted in substantial life limitations. States may also require prior authorization before a service is furnished to a beneficiary in order to determine its necessity. States also engage in utilization review and management to ensure that services furnished to beneficiaries are medically necessary.
Amount, Duration, and Scope of Services
Within broad federal guidelines and certain limitations, states may establish limits on the amount, duration, and scope of the services offered in their Medicaid plan. For example, states may limit the number of outpatient mental health visits covered in a year or limit the number of hours of community support furnished each month. However, the limitations must be crafted so that each covered benefit is "sufficient in amount, duration, and scope to reasonably achieve its purpose."33 To illustrate, a state that has chosen to offer intensive day treatment under the rehabilitation option cannot limit that to two sessions per year, as that would obviously be insufficient to achieve the intended effect of the treatment.
Also, a state may not arbitrarily deny or reduce the amount, duration, or scope of a service based on a beneficiary's diagnosis, type of illness, or condition.34 This restriction is relevant for all categorically needy individuals, even those whose eligibility depends upon a specific diagnosis, such as women in need of treatment for breast or cervical cancer.
The amount, duration, and scope limitation must uniformly apply to all categorically needy beneficiaries in a state's plan, regardless of whether they are mandatory or optional beneficiaries. However, it does not apply to groups of medically needy beneficiaries. States have more flexibility in restricting benefits to this group of beneficiaries. There is one benefit on which states are not permitted to place limitations of amount, duration, and scope: EPSDT services for children under 21.
Comparability
Any Medicaid benefit offered to a categorically eligible individual must be offered to all categorically eligible individuals,35 except when federal law itself creates an exception (e.g., as in the case of ICF/MR services which may only be furnished to persons with mental retardation and other related conditions). A state cannot alter the benefit package so that, for example, dental services are available to SSI recipients but not other categorically eligible adults. Contingent on any amount, duration, and scope limitations, dental services must also be available in the same quantity to all categorically needy beneficiaries. An exception to the comparability requirement is "targeted case management." Under the provisions of Section 1915(g) of the Social Security Act, states may "target" case management services to specific subpopulations of Medicaid beneficiaries, such as persons with serious mental illness or pregnant women under age 21.
Statewideness
States are required to offer the services in their Medicaid benefit package to all eligible recipients without regard to geographic location.36 For example, a state cannot offer services under the clinic option to persons in urban areas but exclude access to these same services to people living in rural areas. Again, the exception to this rule is targeted case management. Not only can a state target its case management option to a specific population, it can also limit its availability to one or more specific areas of the state.
Free Choice of Provider
Medicaid law (Section 1902(a)(23) of the Social Security Act) provides that beneficiaries must be free to choose a provider from among all qualified participating providers, except as specifically provided by law.37 The principal exception to this fundamental and longstanding requirement is when a state has secured federal approval to employ a managed care service delivery model or employ a physician case management model.
Provider Requirements
States have latitude in establishing the requirements that Medicaid providers must meet. Providers, of course, must possess any licenses or meet other requirements specified in state law that pertain to the provision of a service. In the case of a few services (e.g., nursing facility or ICF/MR), providers are required to meet very detailed standards that are spelled out in federal law and/or regulations. Once a state has established its requirements, then the state must offer a provider agreement to any willing provider that meets the state's requirements, agrees to accept Medicaid payment, and abide by other fundamental requirements. The main exception to the open enrollment of qualified providers again arises in managed care service delivery models.
Beneficiary Protections
Federal Medicaid law provides certain basic protections for all beneficiaries.38 Specifically, each state must make the Medicaid Fair Hearing appeal process available to any individual who has been denied eligibility, who has been denied a service, whose services would be reduced or terminated, or who faces loss of eligibility. The state must notify beneficiaries in advance before an "adverse action" affecting Medicaid coverage takes effect and include an explanation of their rights regarding the Fair Hearing process, including the right to an evidentiary hearing conducted by an impartial, uninvolved official (e.g., an administrative law judge). As long as an individual requests a hearing on a timely basis, services must be continued through the duration of the hearing process. In pursuing an appeal, beneficiaries have the right to enlist other individuals to assist them in pursuing the appeal (e.g., peers, friends, families, advocates, attorneys).
Payments for Services
Except in the case of capitated managed care arrangements, Medicaid operates in a "fee-for-service" framework. Providers are paid for each distinct service they furnish to a specific Medicaid beneficiary. Payments are "unit" based -- e.g., a provider is paid for a "visit," an hour or partial hour of service or, in the case of institutional services, a "day." Medicaid payments are made after the provider submits a "claim" for services that specifies the service rendered, the date of service and the beneficiary to whom the service was provided. In the fee-for-service framework, advance payments for services may not be made. Provider claims for services are processed through claims processing systems. These systems verify the beneficiary's eligibility and check other elements of the claim. With some exceptions, federal Medicaid law requires that payments to providers be made directly by the state to the provider. In short, Medicaid does not operate as a "grant" program but instead is structured to pay for discrete services furnished to beneficiaries. Payments are discussed in more depth in Chapter 7.
States have latitude in establishing payment amounts for services and units of reimbursement. Federal law (Section 1902(a)(30) of the Social Security Act) directs states to assure that "payments are consistent with efficiency, economy, and quality of care, and are sufficient to enlist enough providers so that care and services are available under the plan." In general, providers cannot charge Medicaid more than they charge other payers for the same service. In addition, providers may not charge beneficiaries an additional amount over and above the amount that they receive from Medicaid because the Medicaid payment is considered "payment in full."
Under a managed care arrangement, a state may make capitated prepayments to managed care organizations to furnish the full range of contracted services to enrolled beneficiaries. The amount of such payments must be based on data concerning the costs of serving beneficiaries under a fee-for-service arrangement.
Waiver Authorities
Federal Medicaid law allows the Secretary of Health and Human Services (HHS) to grant waivers of various statutory provisions that normally govern the operation of a state's Medicaid program. Since the early 1990s, the use of these waiver authorities has increased, including their use to provide services for individuals with serious mental illnesses. Waivers allow states to receive federal financial participation for covering individuals and/or services in ways that would not ordinarily be permitted. Depending on the type of waiver, a state can "waive" requirements such as comparability and statewideness to provide a targeted benefit package to individuals with a specific medical condition or who live in a certain geographic area. Chapter 6 has an indepth discussion of the use of waiver authorities in serving individuals with serious mental illnesses. Here, the three main types of waivers -- Section 1115, Section 1915(b) and Section 1915(c) -- are outlined.39
1115 Demonstration Waivers
Under Section 1115 of the Social Security Act, states may gain permission from the Secretary of HHS to use federal Medicaid dollars to cover groups of individuals and/or services not otherwise matchable, or to demonstrate alternative approaches to furnishing services to beneficiaries. The 1115 demonstration authority is relatively broad, allowing the waiver of a wide range of statutory requirements. In order to obtain federal approval of an 1115 demonstration, a state must demonstrate "budget neutrality," meaning that federal spending will not be more than what it would have been in the absence of the demonstration.
The 1115 waiver authority requires a research and demonstration component. States must arrange for an independent evaluation of the waiver to determine how successful they were at achieving their goal(s). States have employed 1115 demonstrations to expand Medicaid services to include uninsured individuals and families who could not otherwise be covered. The authority also has been used on a more targeted basis to test different ways of serving Medicaid beneficiaries. Once an 1115 demonstration is approved, it usually expires after five years. As discussed in Chapter 6, some 1115 waiver programs include mental health services.
1915(b) Waivers
A 1915(b) waiver is commonly referred to as a "freedom of choice" waiver (because it permits a state to waive the free choice of provider requirement). It also provides for waivers of comparability of services and statewideness requirements. Originally, 1915(b) waivers were most commonly used by states to implement managed care programs by restricting beneficiaries' choice of providers. However, the 1997 Balanced Budget Act allowed states to employ managed care for certain Medicaid beneficiaries through a state plan amendment rather than a waiver. Still, the 1915(b) waiver authority can be used to create a "carve out" system of managed care delivery for specialized services such as mental health services, as well as target certain services to a particular region or segment of the population.
Unlike the 1115 demonstration waiver authority, a state cannot use a 1915(b) waiver to expand eligibility. By law, 1915(b) waivers are approved for an initial two-year period and may be renewed for additional two-year periods. By statute, a 1915(b) waiver program must be "cost effective" -- i.e., the per-beneficiary costs must be no greater than the costs of serving individuals in the absence of a waiver program. As discussed in Chapter 6, several states furnish mental health services through Section 1915(b) waiver programs.
1915(c) Home and Community-Based Services Waivers
The 1915(c) waiver authority permits states to provide services (e.g., personal care, respite, habilitation, case management) to individuals who would otherwise require and be eligible for institutional services in a hospital, nursing home facility or ICF/MR. States must demonstrate that the average per person costs of furnishing home and community services does not exceed the average per person cost of institutional services to persons in the target group. Section 1915(c) permits states to obtain a waiver of Medicaid's comparability and statewideness requirements as well as extend institutional financial eligibility rules to people in the community. The waiver of comparability permits a state to target services to specific groups of beneficiaries (e.g., individuals with developmental disabilities). In addition, a state may limit the number of individuals who participate in a program. Many of the benefits that a state may offer through an HCBS waiver cannot ordinarily be offered under the Medicaid state plan. As discussed in Chapter 6, this waiver authority has not been used frequently to support working age adults with serious mental illnesses.
Conclusion
Medicaid is a linchpin in meeting the health needs of low-income individuals and families in the United States. It has grown enormously in scope and depth over the past four decades. During that time, federal policy has evolved considerably. Within federal parameters, states have substantial flexibility in crafting their Medicaid programs with regard to who will be served and which services will be offered. To incorporate Medicaid financing into systems that support working-age adults with serious mental illnesses, states must examine how they can employ Medicaid's flexibility to advance their goals and objectives.
The next chapter discusses in detail how federal rules affect Medicaid eligibility for adults with serious mental illnesses. A state's eligibility policies play a critical role in determining the extent to which people with serious mental illnesses can receive Medicaid services.
Annotated Bibliography
Understanding Medicaid Home and Community-Based Services: A Primer (2000). Washington, DC: US Department of Health and Human Services; Office of the Assistant Secretary for Planning and Evaluation.
The Primer is a comprehensive publication that describes how Medicaid can be used to support individuals with disabilities in the community. It provides detailed explanations of Medicaid policy, including financial and service eligibility, as well as information regarding coverage design, community transition, and cost-effectiveness issues. It also contains many state examples to assist states in designing their own community-based Medicaid coverages for people with disabilities.
King, M. & Christian, S. (1999). Medicaid Survival Kit. Washington DC: National Conference of State Legislatures
Originally published in 1996 and updated in 1999, the NCSL Medicaid Survival Kit is a comprehensive resource designed to help policymakers understand Medicaid's rules, regulatory structure, and options. It provides: (1) a clear, detailed presentation of the Medicaid program and its eligibility groups, (2) complete information about programmatic choices available to states within the current federal structure, and (3) examples of how states combat cost increases and implement efficient health care delivery. Available for purchase at www.ncsl.org/public/catalog/pubs.cfm?topic=Health&topiccode=xhlt
Rowland, D. & Garfield, R. (2000). Health Care for the Poor: Medicaid at 35. Health Care Financing Review, 22(1): pp. 23-34.
This article describes the history of Medicaid from its inception in 1965 to the present. This historical perspective examines relevant legislation as well as the evolution of the program. The article discusses current challenges concerning Medicaid at the state and federal levels and potential ways of addressing them. Available at cms.hhs.gov/review/00fall/00fallpg23.pdf
Schneider, A., Elisa, R., Garfield, R., et al. (2002). The Medicaid Resource Book. Menlo Park CA: The Kaiser Commission on Medicaid and the Uninsured. (215 pages).
This publication provides comprehensive information concerning Medicaid policy, focusing on four topics: eligibility, benefits, financing, and administration. It provides extensive information on the demographics of Medicaid beneficiaries, expenditure and financing data and trends, federal and state obligations and options, different types of waivers, and examples of specific state policies. It also contains a useful reference guide with the entire Medicaid legislative history, statutory index, and regulatory index. Available at www.kff.org/medicaid/2236-index.cfm
Web Resources
Because the Medicaid program is complex and multi-faceted, it can be difficult to keep abreast of new developments and their implications for specific groups of beneficiaries. In the case of mental health services, CMS, the Bazelon Center on Mental Health Law and the National Alliance for the Mentally Ill (see Chapter 1) regularly make information available on their web sites concerning Medicaid developments of interest in the arena of mental health services. Other sites include:
Centers for Medicare and Medicaid Services
cms.hhs.gov/medicaid/
The CMS web site has extensive resources concerning the Medicaid program, including program descriptions, state specific information, and descriptions of major CMS initiatives, including those related to the President's New Freedom Initiative.
Kaiser Commission on Medicaid and the Uninsured
http://www.kff.org/about/kcmu.cfm
The Kaiser Commission provides information and analysis on health care coverage and access for the low-income population, with a special focus on Medicaid's role and coverage of the uninsured. It publishes a wealth of information on numerous Medicaid topics. It is an especially well-respected information source.
State Medicaid Agency Web Sites
www.cms.gov/medicaid/allStateContacts.asp
Since Medicaid programs vary appreciably from state-to-state, it is important to keep abreast of developments at the state level. State Medicaid agency contact information and web sites are located at this URL.
Endnotes
-
Kaiser Commission on Medicaid and the Uninsured (1999). Medicaid 101: A Primer. Washington DC
-
Brian Burwell, Kate Sredl, and Steve Eiken (May 2004). Medicaid Long-Term Care Expenditures in FY 2003. The MEDSTAT Group (Cambridge MA).
-
P.L. 89-97 (Social Security Amendments of 1965).
-
The Social Security Act Amendments of 1950 provided for federal financial participation in state vendor payments for health care services furnished to Aid to Families with Dependent Children (AFDC) and aged, blind and disabled cash assistance recipients. However, the amount of such payments was limited by formula. This state-managed vendor payment approach shaped the structure of the Medicaid program. The Kerr-Mills Program was created in the Social Security Bill of 1960. This program provided open-ended federal matching payments for state expenditures for health and other services provided to indigent older persons and, subsequently, people with disabilities. States had wide latitude in deciding what services they would furnish to individuals. Prior to the enactment of Medicaid, there were wide variations in state programs and ten states did not purchase health care services of any type for cash assistance recipients. The history of the enactment of Medicaid and its early implementation period is found in: Robert Stevens and Rosemary Stevens (1974). Welfare Medicine in America: A Case Study of Medicaid. New York: The Free Press. See also Rowland, D. & Garfield, R. (2000). Health Care for the Poor: Medicaid at 35. Health Care Financing Review, 22(1): pp. 23-34.
-
P.L. 92-603 (Social Security Amendments of 1972).
-
P.L. 90-248 (Social Security Act Amendments of 1967).
-
P.L. 92-223 (Act of December 14, 1971).
-
The expansion of Medicaid eligibility mandates and options began in 1988 when Congress mandated that states provide Medicaid coverage for pregnant women and infants with incomes up to 100 percent of the Federal Poverty Level (FPL). In 1989, mandatory Medicaid coverage of children under age 6 in households with incomes up to 133 percent of FPL was mandated. In 1990, Congress mandated the coverage of children ages 6 through 18 in households with incomes of up to 100 percent of FPL; this mandate was phased in and fully took effect in 2002. These mandates also were accompanied by options for states to expand coverage to children and pregnant women in households with incomes in excess of the FPL minimums.
-
P.L. 97-35 (Omnibus Budget Reconciliation Act of 1981)
-
P.L. 100-203 (Omnibus Budget Reconciliation Act of 1987)
-
P.L. 101-239 (Omnibus Budget Reconciliation Act of 1989)
-
P.L. 104-193
-
The §1931 family coverage was established. States were required to continue to cover families who met July 1996 AFDC-related eligibility criteria but also could provide for higher eligibility thresholds.
-
The legislation stipulated that individuals with legal resident status who entered the United States on or after August 22, 1996 are ineligible for SSI, Medicaid and other public benefits until they have been in the country at least five years. Immigrants who entered before that date -- as well as those who have remained through the five year window -- are coverable at state option. Most states have exercised this option.
-
P.L. 105-33 (Balanced Budget Act of 1997).
-
The ceiling on DSH payment adjustments and restrictions on the use of provider taxes and donations were contained in P.L. 101-234 (Medicaid Voluntary Contribution and Provider-Specific Tax Amendments of 1991.) DSH ceilings also were lowered in the Balanced Budget Act of 1997 but modified in the Medicare, Medicaid, and SCHIP Improvement and Protection Act (P.L. 106-554).
-
P.L. 105-33 (Balanced Budget Act of 1997) and P.L. 106-170 (Ticket to Work and Work Incentives Improvement Act of 1999)
-
This section draws from The Kaiser Commission on Medicaid and the Uninsured (May 2003). Medicaid: Fiscal Challenges to Coverage. Washington, D.C.
-
The Kaiser Commission on Medicaid and the Uninsured (April 2001). Medicaids Role for the Disabled Population Under Age 65. Washington, D.C.
-
Federal statutory provisions concerning the state Medicaid plan are contained in §1902 of the Social Security Act.
-
A list of CMS Regional Offices is at cms.hhs.gov/about/regions/professionals.asp
-
Located at www.access.gpo.gov/nara/cfr/waisidx_02/42cfrv3_02.html
-
Some of this guidance takes the form of state Medicaid director letters. These letters are located on the web at www.cms.gov/states/letters/default.asp. More guidance also is found at cms.hhs.gov/states/
-
There are a few services (e.g., family planning) for which there is a uniform rate of federal financial participation set in statute. In the Jobs and Growth Tax Reconciliation Act of 2003 (P.L. 108-27), Congress temporarily increased each states FMAP (including states at the FMAP minimum) by 2.95 percent for the period April 2003 through June 2004 to provide states additional federal assistance.
-
However, in the case of the territories, federal financial participation is limited to a specific amount set by Congress.
-
See 42 CFR 457.220.
-
The Kaiser Commission on Medicaid and the Uninsured (May 2003), op. cit.
-
Based on the number of Medicaid enrollees at any given time during the year. The categories of children and adults do not include beneficiaries with disabilities; the category of people with disabilities does not include adults 65 and over (they are in the Older Adults category).
-
The Kaiser Commission on Medicaid and the Uninsured (May 2003), op. cit.
-
42 CFR 440.230(b).
-
42 CFR 440.230(c).
-
42 CFR 440.240.
-
§1902(a)(1) of the Social Security Act; 42 CFR 431.50.
-
Also, 42 CFR 431.51.
-
§1902(a)(23) of the Social Security Act; also 42 C.F.R. 431.200-.250.
-
These waivers are "named" after the respective sections of the Social Security Act that authorize their use. From here on, they are referred to simply as 1115, 1915(b), and 1915(c) waivers.
CHAPTER 3: MEDICAID ELIGIBILITY
| Federal policy establishes the fundamental parameters concerning the groups of individuals that a state may serve in its Medicaid program. This chapter explains Federal requirements and options that determine Medicaid eligibility for working-age adults with serious mental illnesses. |
In order to receive the mental health and other benefits that a state covers in its Medicaid program, working-age adults with serious mental illnesses must meet state eligibility criteria. Medicaid is a means-tested program; that is, eligibility depends on whether individuals income and resources are at or below specified threshold levels. Medicaid eligibility also hinges on whether the person meets other categorical requirements, such as disability criteria. Federal law gives states latitude to expand Medicaid eligibility for people with disabilities beyond fundamental federal mandates.
This chapter describes federal policies that affect Medicaid eligibility for working-age adults with serious mental illnesses, including the eligibility expansion options available to states. There are many intricacies to Medicaid eligibility, both in federal policy and within each states policies. While Medicaid eligibility criteria are described in some detail, the chapters main purpose is to provide an overview rather than explore every intricacy. When assessing the role that Medicaid might play in supporting working-age adults with serious mental illnesses in the community, it is important to become familiar with the states eligibility policies, including whether such policies might be changed to improve access.
The chapter devotes considerable attention to the interplay between Medicaid eligibility and employment. Recent changes in federal law and policy permit states to continue Medicaid eligibility for people with disabilities who work. Because employment is important for working-age adults with serious mental illnesses, these policy changes -- if adopted in a state -- can allow individuals to continue receiving Medicaid benefits when their recovery leads to employment.
At the outset, it is important to stress that the extent to which working-age adults with serious mental illnesses qualify for Medicaid is directly dependent on a states generic eligibility policies concerning non-elderly adults with disabilities. There are no special Medicaid eligibility groups reserved exclusively for people with serious mental illnesses. A states Medicaid eligibility policies may not exclude individuals with serious mental illnesses based on their diagnosis. Similarly, a state may not establish more liberal eligibility policies for individuals with serious mental illnesses than for people with other disabilities. Eligibility policy changes that might benefit individuals with serious mental illnesses must encompass all people with disabilities. The description of Medicaid eligibility that follows applies to working-age adults with serious mental illnesses insofar as they qualify for Medicaid by meeting generic disability, income and asset tests.
Some aspects of Medicaid eligibility pose special challenges for working-age adults with serious mental illnesses. Ways to identify and address these challenges are also discussed in this chapter.
Overview
The Basic Features of Medicaid Eligibility are summarized on the next page. Medicaid eligibility is rooted in two federally financed programs of cash assistance to help support low-income individuals and families: the former Aid to Families with Dependent Children (AFDC) program, which provided income support for low-income families with children, and the Supplemental Security Income (SSI) program for older persons, blind persons, and persons with disabilities. In 1996, welfare reform legislation replaced AFDC with a new program, Temporary Assistance for Needy Families (TANF), but maintained existing Medicaid eligibility criteria based on AFDC eligibility stand-ards for dependent children and parent(s).
Like AFDC/TANF and SSI, Medicaid is a means-tested entitlement program. That is, a person qualifies for Medicaid if: (a) their income and resources do not exceed the state threshold specific to their eligibility group and (b) they satisfy all other relevant eligibility criteria.
Medicaid eligibility rules fall into two basic sets: categorical and financial. The categorical set of rules defines specific categories of persons for whom federal law permits coverage. In the case of people with serious mental illnesses, the disability categorical group usually is the most pertinent. Medicaid criteria for determining who has disabilities are generally the same as SSI criteria, as established by the Social Security Administration. To qualify in a disability category, a person must have a long lasting, severe, medically determinable physical or mental impairment. Medicaids eligibility rules for persons with disabilities are also built on a foundation of Social Security Administration disability determination rules. But many exceptions and variations have been enacted over the years so that low-income persons who need health care but do not qualify for cash assistance may become eligible for Medicaid. With respect to the disability categorical group, the discussion of Medicaid eligibility includes: (a) persons who qualify for Medicaid by virtue of the receipt of SSI cash assistance or under more restrictive rules in some states (see explanation of 209(b) below) and (b) options that permit eligibility expansions to other individuals.
| Basic Features of Medicaid Eligibility2 | |
There are five generic, broadly applicable parameters that govern Medicaid eligibility:
|
Working-age adults with serious mental illnesses also may qualify for Medicaid by being a member of a low-income family with children or under special provisions that apply to low-income pregnant women. A persons disability is not a criterion for eligibility in these groups; instead, the applicable criteria revolve around the composition of the household (which must include one or more children in the case of adults applying for family coverage) and income. While there is no direct tie between disability and Medicaid eligibility for adults in these households, there is considerable evidence that many adults in qualifying low-income households also have serious mental illnesses.4
Medicaid for SSI Cash Assistance Beneficiaries
Medicaid eligibility for people with disabilities is tied very closely to eligibility for SSI cash assistance, the federally administered program that ensures a nationally uniform income floor for persons who are elderly, who are blind, or who have disabilities.5 In many states, SSI beneficiaries are automatically eligible for Medicaid. However, there are some states (called 209(b) states) where Medicaid eligibility for people with disabilities is more restrictive than SSI requirements or where SSI beneficiaries are required to apply separately for Medicaid (SSI-criteria states). In 209(b) states, SSI beneficiaries still must be granted Medicaid eligibility once they satisfy certain requirements (described below).
In order to be eligible for SSI, a non-elderly adult (age 18 to 64) must have a severe, medically determinable physical or mental impairment or impairments. The impairments that are the basis for SSI eligibility (and SSDI eligibility) are contained in the Listings of Impairment that are promulgated by and periodically revised by the Social Security Administration.6 The impairments in the Listings are similar to diagnoses. (The box, SSI and SSDI, (below) describes the similarities and differences between the two programs.)
For example, the Listings of Mental Impairments were drafted to parallel the Diagnostic and Statistical Manual, which is used to diagnose mental disorders, including mental illnesses such as schizophrenic, affective, and anxiety disorders.7 Not all impairments qualify a person for SSI. For example, individuals for whom drug addiction or alcoholism is the contributing factor material to their disability are not eligible for SSI and, therefore, ineligible for Medicaid on the basis of their disability.
Having a severe impairment (including a serious mental illness) is not sufficient to make a person eligible for SSI. In the case of adults,8 the impairment must be judged to be so severe that a person not only is unable to perform his or her previous work but cannot, considering his [her] age, education and work experience, engage in any other kind of substantial gainful work.
In 2005, a persons inability to work is defined in part as having earnings less than $830 per month net of income-related work expenses. Earnings above this level are considered by regulation as evidence of a persons ability to engage in substantial gainful activity (SGA).9 SSI eligibility is based on an individuals having a listed severe impairment that causes the person to be unable to engage in regular work where the individual earns more than the SGA standard.
| SSI and SSDI | |
| The SSI program sometimes is confused with the Social Security Disability Insurance (SSDI) program.10 SSI and SSDI both provide assistance to individuals with severe impairments who are unable to work. The SSDI program makes payments to medically disabled individuals who have worked and paid Social Security taxes for a minimum number of years. SSI eligibility does not hinge on a person's previously paid Social Security taxes; children also can qualify for SSI. An individual's SSDI entitlement is based on work history. SSDI payments also are made to the "adult disabled children" of deceased or retired workers. Some individuals receive both SSI and SSDI payments, when the amount of their SSDI entitlement is less than the standard SSI payment. Adults with disabilities who apply for Social Security benefits are evaluated to determine whether they qualify for either program; individuals who are determined eligible are assigned to the SSDI program if they qualify and SSI if not. Because SSI and SSDI disability criteria are the same, SSDI-only beneficiaries may also qualify for Medicaid based on disability but usually in the "optional" eligibility groups. SSDI-only beneficiaries have income that is higher than the income standard associated with SSI eligibility. In 2001, there were 5.2 million "disabled worker" SSDI beneficiaries, 28 percent of whom had mental disorders other than mental retardation. In comparison, there were 3.8 million SSI beneficiaries between the ages of 18 and 64, including 35 percent who had mental disorders other than mental retardation.11 There were approximately 1.2 million individuals between the ages of 18 and 64 who received both SSI and SSDI public assistance benefits.12 |
The SSI program was created and structured to provide support to persons who have especially severe disabilities. Consequently, not all persons who have serious mental illnesses qualify for SSI. Anyone who does not meet SSI disability criteria cannot receive Medicaid in a disability category of eligibility, even if they have extensive medical needs or high medical bills. There are special exceptions that allow Medicaid eligibility for certain former child beneficiaries of SSI disability benefits as well as for persons who do not meet one or more of the usual SSI disability criteria because they earn more than $830 per month. These exceptions are discussed later in the chapter.
Thirty-nine states and the District of Columbia grant Medicaid to all individuals in any month in which they receive an SSI payment.13 Of these, thirty-three do so automatically, based on a list of SSI beneficiaries compiled by the federal Social Security Administration and transmitted to the states.14 The other seven states15 (known as SSI-criteria states) require that SSI beneficiaries file a separate application with the state for Medicaid benefits. The remaining 11 states16 follow what is known as the 209(b) exception option (described below) which allows them to provide Medicaid to SSI beneficiaries only if they meet the states criteria, which may be more restrictive than SSI.
General Rule: SSI Income and Resource Eligibility
In states where Medicaid eligibility is directly tied to receipt of SSI, SSI income and resource eligibility rules are followed. The general income eligibility rule for SSI specifies the level of countable income at or below which a person is financially eligible for benefits. Countable income includes cash income plus certain in-kind goods or services a person receives in a given month, minus certain amounts that are exempt from the SSI benefit calculation (discussed more fully below).
In 2005, the maximum monthly federal SSI benefit for persons with no more than $20 in other income is $579 for an individual and $869 for a couple.17 These maximum payment amounts are also known as the Federal Benefit Rate (FBR). Persons with income from other sources (e.g., Social Security or a pension) receive a lesser amount -- equal to the difference between the full SSI benefit rate and the amount of their countable income from other sources. For example, the SSI benefit for an individual with countable income of $540 would be only $39 per month. The general rule also defines countable resources as cash or other property, including real property, that (a) were acquired at some time in the past, (b) the individual has the right to access, and (c) could be converted to cash and used to cover current basic living needs. Individuals with up to $2000 ($3000 for a couple) in countable resources can qualify for SSI.18 SSI resource limits often serve as the basis for Medicaid resource eligibility.
Exceptions to the General Rule
There are two major exceptions to the general SSI income and resource eligibility rules: the state 209(b) option and protection for certain former SSI beneficiaries.
State 209(b) option19
Medicaid for the Aged, Blind, and Disabled historically had always been linked to receipt of cash assistance benefits. When SSI replaced state-only programs of aid for older persons and people with disabilities in 1972, it was expected to lead to large increases in the number of beneficiaries. The 209(b) option was enacted along with SSI in 1972 to allow states to avoid similarly large increases in Medicaid enrollment and costs. At present, there are eleven 209(b) option states.
Many Medicaid eligibility rules under the 209(b) option follow SSI rules. But states may choose, instead, to use some or all of the more restrictive Medicaid rules that were in effect in their state on January 1, 1972, shortly before SSI was enacted. Typically these states have retained at least some of their pre-SSI rules concerning countable income or resources. Only a few use more stringent criteria for determining blindness or disability.20
In general, 209(b) states have lower income and/or resource standards than states that key eligibility to the SSI FBR. Federal rules require that all 209(b) states counterbalance the potential negative effects of the 209(b) option on SSI beneficiaries. Any residents who are elderly, blind, or have disabilities -- including those with too much income for SSI -- must be allowed to spend down to the states Medicaid income standard if their expenses for medical services so erode their income that their net remaining income would be less than a standard set by the state. This requirement creates a medically needy-like program for this population, even in states that have not chosen specifically to cover the medically needy as an option, as is the case in Indiana, Missouri, and Ohio. Spend-down rules for 209(b) are virtually identical to spend-down rules for the medically needy (discussed below).
Medicaid protection for certain former SSI beneficiaries
Federal law also requires all states, including 209(b) states, to provide Medicaid to former SSI beneficiaries who would, but for increases in their Social Security benefits, continue to be eligible for SSI.21 Congress passed this provision in 1986 to ensure that annual Social Security increases -- intended to improve peoples lives -- did not harm this group by causing them to lose Medicaid as well as SSI.22 These individuals are treated as if they are still receiving SSI. Most of the individuals affected have incomes just marginally above the income levels at which they might qualify for SSI and Medicaid. In fact, many persons who could qualify for Medicaid under these provisions do not apply for the program, most likely because they are not aware of them. Improved understanding of these protections may help increase the Medicaid enrollment of this group.
Countable Income or Resources
The concept of countable income and resources may seem arcane but is important. As noted previously, neither SSI nor Medicaid determine eligibility by comparing a persons total income and resources to the dollar thresholds that apply in the persons eligibility category. Rather, both programs count only certain types and amounts. For this reason, an individual can have total income or resources that are higher than the nominal eligibility limits (i.e., higher than $579 in total income or $2000 in total resources for SSI) and still qualify for benefits.
SSI Rules
SSI rules reduce a persons gross income in calculating countable income in three important ways. First, SSI disregards the first $20 of every applicant/recipients income, regardless of source. Second -- and of great significance to people with disabilities who work -- SSI provides an additional disregard of earnings from work, amounting to the first $65 plus one-half of the remaining earnings amount. This disregard of earned income contrasts with the treatment of unearned income (e.g., pensions or SSDI payments). Except for the basic $20 disregard, in general all unearned income is countable and reduces a persons SSI payment.
Unearned income in excess of $599 (the $579 FBR plus the $20 universal disregard) precludes eligibility for SSI and thereby Medicaid, unless the state has another disability-related eligibility group for which the person qualifies. In the case of earned income, however, a significant portion is disregarded. SSI rules also contain additional work incentives, which are described in SSI and People with Disabilities Who Work on the next page.
Third, spouses or children with disabilities in families with other non-disabled members who are ineligible can qualify for SSI at higher gross amounts of family income. In such households, SSI counts only the portion of the non-disabled family members income that is left after SSI subtracts amounts to cover their basic needs. SSI also may apply several other special-purpose reductions.
| Example: SSI Treatment of Earned Income | |
If an individual with a disability has a job that pays $700 per month and has no other unearned income, then SSI rules treat the person's earnings in the following fashion: Gross income: $700 Disregards:
|
SSI rules also reduce gross resources in determining whether resources are below the SSI $2,000/$3,000 thresholds, by exempting the home (regardless of value) and (within limits) such things as an auto, household goods, surrender value of life insurance, burial funds, and property that is essential to self-support.23
Additional Eligibility Options for People with Disabilities
SSI cash beneficiaries can secure Medicaid: (a) automatically in most states by virtue of their cash assistance status; (b) by applying for it in SSI- criteria states; or, (c) satisfying the rules employed in 209(b) states. There are other eligibility options available to states that permit them to extend Medicaid eligibility to people who have disabilities (based on SSA criteria) but who are not SSI cash beneficiaries. The following sections describe these options. These options often (but not exclusively) benefit SSDI beneficiaries whose SSDI entitlement disqualifies them from SSI. These individuals, of course, must meet the same disability impairment tests as SSI beneficiaries. Also, with respect to these optional eligibility groups, federal policy gives states additional latitude to depart from SSI rules concerning countable income and resources. This latitude (contained in §1902(r)(2) of the Social Security Act and described in more detail on the following page) may be used by a state to (1) extend Medicaid eligibility to low-income people with disabilities who might not qualify under SSI rules, and (2) to encourage such persons to obtain employment.
| SSI and People with Disabilities Who Work | |
Eligibility for SSI (and SSDI) is assessed by whether a person can engage in "substantial gainful activity" (SGA). SGA is measured in part by whether a person's earnings, after deducting work expenses, are $830 or less per month. A concern is that, once a person's earnings exceed $830 per month, she or he will be dropped from SSI and, thereby, potentially lose Medicaid benefits. As a result of changes enacted in 1986, which added Section(§)1619(a) and §1619(b) to the Social Security Act, federal SSI policy provides opportunities for SSI beneficiaries to obtain work and still retain SSI benefits even if their earnings exceed the SGA level, and to retain Medicaid benefits at even higher levels of earned income.24
|
The majority of eligibility pathways for individuals with serious mental illnesses are based, at least in part, on their disability status. Table 3-1 on the following page shows these different eligibility options and the number of states that use them, as well as basic financial and other requirements. Omitted from this table are the few options for enrolling persons with serious mental illnesses based on non-disability criteria. However, all relevant options are discussed in this section.
Many working-age individuals who are eligible for Medicaid under the options described in this section are also eligible for Medicare benefits. Dual eligibility is described in the Medicare-Medicaid Dual Eligibles section on the following pages.
State Supplemental Payments
Many states supplement the basic SSI payment and pair these state supplementary payments (SSP) with automatic Medicaid eligibility. These states have elected to spend state-only, unmatched money to supplement the basic SSI FBR in circumstances where they have determined that rate to be insufficient to cover living expenses necessary for minimally adequate living standards. These state supplements are state-determined and vary widely by state. Some states provide across-the-board supplements to SSI-eligible persons. Several states provide supplements to individuals who live in designated types of community residences or for other reasons. In states that provide supplements, the effect of the supplement is to increase the income standard from the SSI FBR to the SSI FBR plus the amount of supplement for which a person qualifies. Some individuals have too much income to qualify for SSI cash assistance but may qualify for an SSP benefit only. States can elect to make such persons automatically eligible for Medicaid, just as they can for SSI beneficiaries. Automatic Medicaid eligibility for state supplement beneficiaries provides an additional measure of assistance in paying for needed medical services. States have broad flexibility with respect to not only the level of SSP support but also the criteria under which supplements are offered. Individuals with serious mental illnesses who receive SSP benefit from this expansion of Medicaid eligibility.
| TABLE 3-1: Medicaid Eligibility Options for Working-Age Adults with Disabilities | ||||||
|---|---|---|---|---|---|---|
| Medicaid Eligibility Option | # of states | Income Limit | Required Age Limits | Resource/ Asset Limit | Can Apply 1902(r)(2) | Disability Definition |
| State Supplement Group (SSP) | 35 | No Federal limits; state can set | None | State can set | Yes | SSI |
| 100% of Poverty | 19 | State defines, no more than 100% FPL | None | At least as much as SSI | Yes | SSI |
| Medically Needy | 31 | Less than 133.33% of pre-TANF AFDC level | None | SSI | Yes | SSI |
| BBA 97 | 12 | 250% FPL net income | None | SSI | Yes | SSI |
| TWWIIA Basic | 16 | No Federal limits; state can set | 16 - 64 | No Federal limits; state can set | Yes | SSI |
| TWWIIA Medical Improvement | 7 | No Federal limits; state can set | 16 - 64 | No Federal limits; state can set | Yes | Previously eligible for SSI |
| §1902(r)(2): Medicaid Exceptions to SSI Rules on Counting Income and Resources27 | |
| §1902(r)(2) of the Social Security Act permits a state to adopt more liberal rules than SSI concerning countable income and resources for optional eligibility groups. Federal rules concerning this provision were extensively revised in January 2001 and CMS has issued technical assistance to guide states in using the latitude under §1902(r)(2), especially with respect to people with disabilities. This provision cannot be invoked for most mandatory categorical eligibility groups (e.g., SSI beneficiaries).28 These rules allow states to redefine countable income or assets so that statutory eligibility limits, while still theoretically applicable, can be greatly exceeded. This flexibility comes with certain restrictions. First, the different counting methods must not disadvantage anyone, even if relatively more people would benefit than would be disadvantaged. Second, although a state may restrict its more liberal methods to eligibility groups it selects, the eligibility group(s) must be specifically defined in Medicaid law. A state cannot carve out a subgroup of its own definition (e.g., one based on medical diagnosis or place of residence). While the federal rules give states broad flexibility to expand eligibility, the adoption of more generous methods must, of course, conform to a state's budget considerations and political decisions. The rules allow establishing higher resource limits for optional groups above the $2,000 SSI resource standard. The rules also may be used to completely exempt certain resources (e.g., retirement accounts). A state may also disregard specified sources of income. For example, a work incentive can be provided by disregarding some or all of the earned income of working-age adults with disabilities. The net effect of a state's invoking this flexibility is to broaden who may qualify for Medicaid in the categories where more liberal rules are applied. For example, in a state with the 100 percent of poverty option, more liberal disregards widen the number of individuals who meet the income standard for this option. More liberal disregards can assist more people to qualify as medically needy (especially more liberal resource standards) or reduce the amount that medically needy individuals must "spend down" in order to qualify. |
| Medicare-Medicaid Dual Eligibles | |
| Working-age adults with disabilities qualify for the Medicare program if they have received SSDI benefits for a period of two years. People who receive both SSI and SSDI benefits, and individuals who receive only SSDI benefits but also qualify for Medicaid in an optional eligibility category, are called "dual eligibles" because they are eligible for both Medicare and Medicaid benefits. States pay the premiums, co-insurance and deductibles for services that dual eligibles receive through Medicare (e.g., physician services). Federal law also requires states to pay Medicare premiums, co-insurance and/or deductibles for certain low-income individuals, including SSDI beneficiaries, who do not qualify for Medicaid. Low-income people with serious mental illnesses benefit from Medicare coverage, but Medicare covers only a limited package of mental health services (described in Chapter 4). Medicaid's benefit package is broader than Medicare's, especially with respect to long-term care services. With respect to dual eligibles, Medicaid is often said to "wrap around" Medicare benefits. Consequently, those who require a wider-range of mental health services benefit much more when they also qualify for Medicaid. In states where there is limited use of Medicaid eligibility options, low-income working-age adults with serious mental illnesses are more likely to have only the more limited Medicare benefit package to fall back on, and the availability of critical community mental health services will hinge on the availability of state funding. |
100 Percent of Poverty Option
In 2004, the federal SSI FBR was approximately 73 percent of the Federal Poverty Level (FPL) for one person. States have the option to raise the income level at which any person who meets SSI disability criteria can qualify for Medicaid to as high as 100 percent of FPL ($9,310 for one person in calendar year 2004, increasing incrementally for additional family members).29 In states that employ this option, SSDI-only beneficiaries are more likely to qualify for Medicaid because many of them receive SSDI payments that are too high for SSI cash assistance but less than 100 percent of FPL. States using this option may not set limits on countable resources lower than SSI levels ($2000 for one, $3000 for a couple) but may disregard additional resources under §1902(r)(2) of the Act.
It bears repeating here that what is compared to these eligibility levels is countable (not total) income and resources. Under the 100 percent of poverty option, at the very least, states must disregard the same kinds and amounts of income and resources that SSI disregards, but they may also use more liberal income disregards than SSI. Because there is no spend down requirement associated with this option, beneficiaries do not have to spend their own funds on medical services in order to qualify (unlike the medically needy option described below). Nineteen states have selected this option.30 Most have tied their income standard to 100 percent of FPL, although some have pegged that standard to a lower amount (between 80 to 95 percent of FPL.)
Medically Needy Option31
States can cover people who have too much income to qualify in any other eligibility group under the medically needy option. Under this option, a person must still fit into one of the Medicaid-coverable categories -- for example, meet SSI/SSDI disability criteria. If not, they cannot qualify as medically needy no matter how low their income or how extensive their medical need. There is no specified ceiling on how much income a person can have and still potentially qualify as medically needy if their medical bills are high enough. Under the medically needy option, a state establishes income standards (also called the medically needy income limit) and resource standards that apply to individuals who cannot otherwise qualify for Medicaid. Once individuals incur sufficient medical expenses to reduce their income to the states standard (that is, they spend down to the medically needy income limit), they become eligible for Medicaid payment of covered services.
| A Hypothetical Spend-Down Situation | |
| If a state's medically needy income standard for an individual is $450 per month and the person has countable income of $800 per month, then the person becomes eligible for Medicaid after incurring $350 in medical expenses. |
With respect to working-age adults with disabilities, the medically needy option can be beneficial for persons who have high prescribed drug or other medical expenses. It also is a Medicaid eligibility pathway for persons who require Medicaid-reimbursable institutional care (e.g., nursing facility services) in states that cover nursing facility care in their medically needy program. In 2000, about 3.6 million Medicaid beneficiaries were in the medically needy category, including approximately 1.3 million older persons and persons with disabilities. Medically needy is also a pathway to Medicaid eligibility for SSDI beneficiaries (including those with mental disorders) who cannot otherwise qualify for Medicaid.
Thirty-two states and the District of Columbia have medically needy programs that include individuals with disabilities. The income and resource standards that apply to these programs vary considerably among states. Some income standards are less than $200 per month while others are over $500.
However, it is important to keep in mind that states may disregard income and resources when they employ the medically needy option (as they can with other optional eligibility categories). When income is disregarded, the effect is that individuals can qualify for Medicaid as medically needy at lower levels of incurred medical expenses.
The role that the medically needy option plays in enabling working-age adults with disabilities to qualify for Medicaid hinges on the other optional coverages that a state has in place. For example, in states that have adopted the 100 percent of poverty option, medically needy eligibility comes into play only for higher income individuals who do not qualify under that option. Where a state has not adopted the 100 percent of poverty option, medically needy may be the only pathway to Medicaid eligibility for non-SSI beneficiaries.
It is important to note that under the medically needy option, a state is not required to offer its full package of Medicaid benefits. A state may limit its coverage for the medically needy to certain mandatory Medicaid benefits (e.g., physician services). In general, most states that operate medically needy programs offer their full Medicaid package. However, some exclude significant benefits.32
There are additional features of the medically needy option that warrant mention:
- A state may not restrict eligibility based on medical condition, type of services needed, or place of residence.
- Except for 209(b) states, a state must use a single eligibility level for income and resources for all the medically needy groups that it covers.33 In the case of income levels, this single level may not exceed 133 1/3 percent of the states pre-welfare reform AFDC payment levels. As noted above, in some states, these medically needy income levels are quite low, typically less than the SSI level. This can mean that individuals with the same disability may find themselves in very different situations depending on whether they qualify for Medicaid as an SSI beneficiary (or through another option) or under the medically needy option. The former group receives Medicaid benefits without charge while the latter group must spend down their income on medical services to qualify for Medicaid and, thereby, has fewer dollars left over to meet other basic living expenses than SSI beneficiaries.
- Medically needy persons with incomes above the states threshold must spend down before becoming eligible for Medicaid benefits. This spend-down requirement can be problematic. The reason is that medically needy persons with countable incomes above the states Medicaid income threshold must spend down to that threshold on a periodic basis in order to remain eligible for Medicaid funding of the services they need.34 Until their spend-down limit is reached, they are responsible for their own medical expenses. There is no federal or state requirement that individuals spending down actually pay their bills. But as a practical matter, providers are unlikely to continue serving them if they fail to pay. Alternatively, states can offer people the opportunity to meet their spend-down obligation by paying it directly to the state in exchange for immediate coverage of all their medical expenses. In either case, however, persons with incomes above the state threshold may have a spend-down liability that leaves them little income available to meet living expenses.
The medically needy option permits a state to extend Medicaid eligibility to individuals whose income is higher than the amount that would permit them to qualify for other optional eligibility categories that a state may have in effect. With respect to individuals with serious mental illnesses, when this option is available, it will principally enable SSDI-only beneficiaries to qualify for Medicaid if their SSDI benefit and other income otherwise disqualifies them from Medicaid.
300 Percent of SSI Income Option
This option -- also called the special income standard -- is available for persons who meet a states criteria for Medicaid institutional services (nursing facilities and ICFs/MR) and HCBS waiver programs. Under this option, a state can establish a special income threshold up to 300 percent of the maximum SSI benefit ($1,737 in 2005). This income standard is tied to a persons gross income rather than countable income. Individuals with income up to the threshold qualify for Medicaid without spending down, but, when institutionalized, such individuals may have a share of cost obligation that requires them to turn over some or all their income except for a personal needs allowance to offset the cost of institutional services.35
This option was originally created so that states that did not wish to cover the entire category of medically needy could at least cover higher income persons residing in a medical institution. Some states employ this option in tandem with the medically needy option for persons served in institutional settings. States may employ this financial eligibility option for individuals in 1915(c) HCBS waiver programs in order to level the playing field between institutional and non-institutional services. Persons receiving waiver services may also have a share of cost obligation that requires them to contribute to the cost of waiver services.36
Medicaid "Buy-In" Options for Workers with Disabilities37
Any benefit program that uses an income cutoff to determine eligibility may pose a powerful disincentive for beneficiaries to return to work, if the earnings from work put them above the financial eligibility threshold level for benefits. To the extent that Medicaid coverage is needed in order to live, the problem becomes an absolute barrier to employment rather than simply a disincentive.
As discussed above, SSI rules contain a work incentive by disregarding a significant portion of earned income, and the SSI §1619(a) and §1619(b) provisions enable SSI beneficiaries who work and earn more than the SGA standard to retain Medicaid. In addition, states may employ §1902(r)(2) to create additional work incentives by disregarding earned income in the case of people with disabilities who work but are not SSI beneficiaries.
In 1997 and 1999, Congress enacted two options for states to extend Medicaid eligibility to workers with disabilities who have significant earnings but may not qualify for Medicaid for various reasons; (including some of the limitations inherent in SSI work incentives, e.g., the low SSI limits on resources, or the contingency that a person must have previously received an SSI cash assistance payment). As shown in Table 3-2, the majority of states have elected to employ at least one of these options. Indications are that working-age adults with mental illnesses have significantly benefited when these options are made available.
In addition to employing these options (which are described in detail below) to secure Medicaid eligibility for people with disabilities who work, states have taken additional steps to address employment barriers. Some of these steps are described in Supporting Workers with Disabilities on the following page.
BBA of 1997 Eligibility Group
Section 4733 of the Balanced Budget Act of 1997 (BBA-97) permits states to extend Medicaid eligibility to working individuals with disabilities who, because of their earnings, cannot qualify for Medicaid under other statutory provisions. States that have employed these provisions have implemented more liberal income and resource methodologies than used in SSI. Under this option:
| TABLE 3-2: State Coverage of BBA and TWWIIA Eligibility Groups | |||
|---|---|---|---|
| BBA Eligibility Group | |||
| Alaska | Maine | New Mexico | Utah |
| California | Mississippi | Oregon | Vermont |
| Iowa | Nebraska | South Carolina | Wisconsin |
| TWWIIA Eligibility Groups | |||
| State | Basic Group | Medically Improved | Income Limit |
| Arkansas | X | 250% FPL | |
| Arizona | X | X | 250% FPL |
| Connecticut | X | X | Up to $36,990 |
| Illinois | X | 20% FPL | |
| Indiana | X | X | 350% FPL |
| Kansas | X | X | 300% |
| Louisiana | X | 250% FPL | |
| Michigan | X | No limit | |
| Minnesota | X | No limit | |
| Missouri | X | X | 250% FPL |
| New Hampshire | X | 450% FPL | |
| New Jersey | S | 250% FPL | |
| New York | X | 250% FPL | |
| North Dakota | X | 225% FPL | |
| Pennsylvania | X | X | 250% FPL |
| Washington | X | X | 220% FPL |
| Wyoming | S | 100% FPL | |
- A state extends Medicaid eligibility to individuals in households with a net family income of less than 250 percent of the Federal Poverty Level, based on family size (in 2004, 250 percent of poverty for a one-person household is $23,275);
- Except for earned income (which is completely disregarded), the individual must meet all SSI eligibility criteria, including: (a) unearned income that does not exceed the SSI FBR ($579 per month); (b) resources that do not exceed the SSI resource standard; and, (c) SSI disability criteria.
- However, a state also may employ §1902(r)(2) to disregard both income and resources that would be counted under SSI methodologies.
In addition, under this option, a state may charge a premium and require beneficiary cost-sharing.
| Supporting Workers with Disabilities38 | |
| Fear of losing Medicaid benefits is a major employment disincentive to individuals with disabilities. Federal policy now offers states several options that permit people with disabilities who work to retain their Medicaid benefits. Several states have accompanied the "roll out" of new work-related Medicaid eligibility options with additional steps to address employment barriers. For example, features of Kansas' "Working Healthy" initiative include: (a) a TWWIIA Medicaid buy-in eligibility option so that people with disabilities who work can keep their earnings and have assets well-above standard Medicaid resource standards; (b) "benefit specialists" out-stationed around the state to help individuals understand how work affects their benefits and navigate the eligibility process; and, (c) outreach to people with disabilities and employers to increase awareness of new employment opportunities. In order to pursue these strategies, Kansas applied for and received a Medicaid Infrastructure Grant through CMS.39 Individuals with mental illnesses comprised about one-half of the first group of Working Healthy participants.40 Follow-up consumer surveys found that Working Healthy participants with mental illnesses have experienced significant improvements in their quality of life and health status as a result of their participation.41 Elsewhere, states that have adopted a Medicaid "buy-in" option have also pursued comprehensive strategies to address employment barriers. For example, some states employ benefit specialists to work with individuals. Some states (e.g., Utah and California) have modified their coverage of Medicaid personal assistance services in order to support individuals with disabilities at locations outside their homes, including the workplace; (the use of personal assistance to support employment is described in Chapter 4). In states that offer peer support, peer support specialists can also play an important role in supporting individuals with serious mental illnesses to return to work. The adoption of Medicaid buy-in options has also been linked to cross-agency employment initiatives to promote employment for people with disabilities. These initiatives frequently include vocational rehabilitation, program agencies (e.g., state mental health authorities), and state employment agencies. |
TWWIIA Options
The Ticket to Work and Work Incentives Improvement Act of 199942 created two new optional eligibility groups: (a) the Basic Coverage Group and (b) the Medical Improvement Group. The key differences between the TWWIIA eligibility groups and the BBA-97 eligibility group are as follows43:
- Basic Eligibility Group. There is no 250 percent of poverty income limit as under the BBA-97. Instead, a state may set its own income limit. This group is limited to persons between the ages of 16 and 64. In addition, there are no required income and resource standards. Like the BBA-97 eligibility group, individuals must meet SSI disability criteria.
- Medically Improved Group. The difference between this group and the Basic Eligibility Group (and the BBA-97 group) is that it may include individuals whose disability has improved to the extent that they no longer meet SSI disability criteria. This determination is made by the Social Security Administration as a result of a regularly scheduled continuing disability review.44 These individuals must have met SSI disability criteria before the review was conducted.
Like the BBA-97 group, states may require beneficiaries to pay premiums and share the cost of services. In addition, with respect to the TWWIIA groups, states also may employ §1902(r)(2) in order to use more liberal income and resource methodologies for these groups.
In many respects, the TWWIIA option provides states more flexibility in crafting work incentives than the predecessor BBA-97 option. While there are differences between the BBA-97 and TWWIIA eligibility options, both give states the latitude to extend Medicaid eligibility to people with disabilities who are successfully employed. These expansions potentially can benefit both SSI and SSDI beneficiaries who return to work. It is important to point out that the SSDI program has weaker basic work incentive provisions than the SSI Program.45 These options (or the use of income disregards in other optional coverage groups) can provide important assistance to SSDI beneficiaries who work but also need access to Medicaid benefits. One important result of the BBA-97 and TWIAA work provisions is that individuals who formerly could only qualify for Medicaid via the medically needy option can now receive benefits under these options. By avoiding the spend down requirements associated with the medically needy option, these individuals can retain more of their work income and, thus, be more independent.
For SSI recipients who work, eligibility for Medicaid benefits hinges on the extent to which a state has selected other Medicaid options and how those options have been structured.
TANF/AFDC Group and Pregnant Women
As noted previously, the 1996 welfare reform legislation severed the direct and long-standing tie between the receipt of cash assistance and Medicaid eligibility for low-income dependent children and their parent(s) or caretaker relatives. The Aid to Families with Dependent Children (AFDC) program was replaced by the Temporary Aid to Needy Families (TANF) program. However, states were required to continue their AFDC-based Medicaid eligibility criteria for this group.
States must also extend Medicaid eligibility to low-income pregnant women in households with incomes up to 133 percent of poverty, and include pregnant women if they operate a medically needy program. Under current Medicaid eligibility provisions for parent(s) and caretaker relatives with children, approximately nine million adults are Medicaid beneficiaries for reasons not directly linked to disability.46
While these eligibility categories are not tied to disability, studies have revealed that a significant number of parents in very low income families and pregnant women (who are or would likely be eligible for Medicaid under non-disability related eligibility groups) have serious mental illnesses. Indeed, especially with respect to parents in very low income families, significant numbers of individuals have been found to qualify for SSI because they have disabilities, including those caused by mental impairments.47 There are other adult members in such families whose mental impairments are significant, but these individuals do not qualify for SSI. In addition, it is estimated that between three and four percent of pregnant women have serious mental illnesses.
Medicaid mental health services are often provided to SSI beneficiaries or persons who qualify for Medicaid through other options but still meet SSI disability criteria. However, adults in Medicaid-eligible low-income families can also make up a significant portion of the pool of individuals who may benefit from Medicaid mental health services.
Medicaid Eligibility for Individuals with Serious Mental Illnesses: Added Challenges
There often are added challenges in securing and maintaining Medicaid eligibility for working-age adults with serious mental illnesses. Some of these challenges are shared by people with other disabilities but many are experienced more frequently by individuals with serious mental illnesses.
Qualifying for SSI/SSDI
The processes and steps involved in securing and maintaining SSI/SSDI eligibility are by no means simple and frequently are time-consuming. They can be especially challenging for individuals with mental impairments, regardless of type. For persons with serious mental illnesses, it is often important that they have assistance in navigating the application and eligibility determination process. When such assistance is not available from involved family members or other allies, it may be provided by the public mental health system or local advocacy organizations and peer support networks. For example, many mental health agencies employ benefit specialists to assist individuals in the application process. Such assistance is a critical capability in programs that serve homeless individuals. Connecting individuals with serious mental illnesses to public benefits is also a central function of service coordinators (case managers). Especially in states that do not automatically link Medicaid and SSI eligibility, assistance may be necessary to help individuals to secure Medicaid eligibility once SSI eligibility has been obtained.
Equally important is a persons maintaining eligibility once it has been secured. There are reporting requirements that both SSI and SSDI beneficiaries must meet in order to continue their benefits. Again, especially in states that do not interlock Medicaid and SSI eligibility, there also are periodic reporting requirements that individuals must fulfill in order to maintain their Medicaid eligibility. In the case of individuals who are eligible for Medicaid, Medicaid-funded case management services (discussed in Chapter 4) can be employed to assist individuals in maintaining their eligibility (as well as access to other benefit programs).
Individuals who receive SSI or SSDI benefits are subject to periodic continuing disability review. Neither SSI nor SSDI eligibility is granted on a permanent basis. Continuing disability reviews assess whether individuals continue to meet eligibility criteria. The frequency of such reviews varies, but they usually take place every three to five years, depending on the nature of the persons disability. A review may result in a determination that a person is medically improved. Such a determination results in a termination of SSI/SSDI benefits, which in turn leads to a loss of Medicaid benefits unless the individual is covered under the TWWIIA medically improved group. This occurs because, in the disability eligibility group, Medicaid eligibility is interlocked with SSI/SSDI disability criteria. Some individuals with serious mental illnesses experience improvements but episodically encounter problems. Individuals who have been determined by the Social Security Administration to be medically improved can apply for reinstatement in the event that their situation worsens. However, after the reinstatement period runs out, they must re-apply for benefits.
Individuals with Dual Disorders
As previously noted, individuals whose impairment is assessed as stemming from alcohol or drug abuse cannot qualify for SSI/SSDI. A high percentage of individuals with serious mental illnesses have dual disorders (i.e., they both have a serious mental illness and experience substance abuse). In the case of these individuals, there are special challenges in securing eligibility for SSI/SSDI. Substance abuse that accompanies a serious mental illness does not necessarily disqualify an individual from SSI/SSDI. In order to secure or maintain SSI/SSDI eligibility for these individuals, it is necessary that the persons physician or psychiatrist indicate that mental illness is the contributing factor to the persons impairment.48
Incarceration49
Numerous individuals with serious mental illnesses experience incarceration. In general, incarceration causes benefits like SSI or Medicaid to be terminated or suspended. When a person is released (whether on parole or probation), reconnecting to benefits can be very important so that the individual can obtain supports in order to resume life in the community.50
When an SSI beneficiary is incarcerated, his/her benefits generally cease immediately. When incarceration is for fewer than twelve consecutive months, the person is placed in suspended status. Individuals in this status may have their benefits reinstated upon release. If the Social Security Administration is notified in advance of release, the persons SSI benefit can be reinstated quickly. However, people incarcerated for more than twelve months must re-apply for SSI. In the case of SSDI, benefits are suspended following conviction and confinement in jail for 30 or more days. SSDI benefits are immediately reinstated once release has been verified. In the case of persons who were not receiving SSI/SSDI before they were incarcerated, they may apply for benefits prior to release. In some states and localities, offender programs work with these individuals prior to release to assist their obtaining benefits.
Because of the linkage between Medicaid eligibility and receipt of SSI assistance, incarceration also poses challenges with respect to securing Medicaid for individuals who have been incarcerated. Federal law prohibits states from making Medicaid payments for services furnished to incarcerated individuals. There also are issues concerning Medicaid eligibility when a person is released. If a person was eligible for Medicaid before being incarcerated, a state may suspend the persons eligibility during the period of incarceration and reinstate it once the person is released (provided, of course, that the person meets applicable eligibility criteria). However, the practice in many states is to terminate eligibility outright when a person is incarcerated. In the case of individuals who receive SSI after release, Medicaid eligibility will be reinstated automatically once SSI benefits are authorized, but only in states where Medicaid eligibility is automatic for SSI beneficiaries. Elsewhere, and in the case of individuals who obtain Medicaid eligibility via other optional groups, securing Medicaid eligibility requires the person to reapply.
There are a variety of steps that states take to reconnect incarcerated persons to benefits as soon after release as possible. Some of these steps include jails and prisons entering into pre-release agreements with the Social Security Administration, continuing involvement with incarcerated individuals by community agencies and offender programs, and simplifying Medicaid eligibility determination processes.51
Effects of Institutionalization on Medicaid Eligibility
When a person with a serious mental illness is institutionalized, additional challenges can arise. Federal law governing the SSI program prohibits the payment of SSI benefits to inmates of public institutions. Under this policy, individuals between the ages of 22-64 in long-term stay status at state mental health facilities may not receive SSI benefits (however, SSDI beneficiaries continue to receive benefits in these facilities).52 SSI eligibility is unaffected in the case of persons who are served in other Medicaid-funded settings (e.g., nursing facilities), in some other types of residential settings, or when persons are institutionalized for short periods (up to three months). Once SSI benefits stop, the connection between receipt of SSI benefits and Medicaid can be disrupted. When a person is discharged from a facility, the steps necessary to reinstate both SSI payments and Medicaid eligibility are similar to those involved in securing benefits for incarcerated persons.
Conclusion
In the case of working-age adults with serious mental illnesses, the main pathway to Medicaid eligibility is via the SSI program, either by being a SSI cash assistance beneficiary or by meeting SSI-disability criteria and securing eligibility through another optional eligibility group (e.g., medically needy). Meeting SSI disability criteria is decisive (except for individuals who are medically improved in TWWIIA states that include such individuals). Because of the stringency of SSI/SSDI disability criteria, low-income individuals with serious mental illnesses who qualify for Medicaid through the SSI pathway have especially challenging impairments and, therefore, would benefit from the provision of rehabilitative and other services. The same is true of adults in TANF households who have serious mental illnesses, even though they might not meet SSI disability criteria.
Federal Medicaid law and policy give states important latitude in extending Medicaid eligibility beyond SSI cash assistance beneficiaries. In particular, individuals who are SSDI beneficiaries but do not receive SSI can be included in a states Medicaid program in various ways, including the 100 percent of poverty option or the medically needy option. These SSDI beneficiaries must meet the same disability tests as SSI beneficiaries. A large proportion of SSDI beneficiaries have mental disorders, including serious mental illnesses.
Medicaids overall role in meeting the needs of working-age adults with serious mental illnesses in any particular state hinges to a significant degree on a states policies concerning the coverage of people with disabilities. In states that have broadened Medicaid eligibility for people with disabilities, a greater proportion of individuals with serious mental illnesses are able to receive Medicaid-funded services. As a result, other resources can be used to meet the needs of a greater number of persons who do not qualify for Medicaid, and other investments can be made in community mental health services. To the extent that a states Medicaid eligibility policies also help overcome disincentives to work (either by invoking the options for workers with disabilities or the flexibility available under §1902(r)(2)), individuals can be encouraged to enter the workplace because they can maintain Medicaid coverage and thereby have ongoing access to Medicaid community mental health services.
For people who obtain Medicaid eligibility, a state may offer vital benefits that will assist their recovery and address other important needs. Chapter 4 describes the types of benefits that states may offer to individuals with serious mental illnesses.
Annotated Bibliography
Cinsavich, S. & Rado, G. (2002). Medicaid Buy-In: Concept and Implementation. Institute for Community Inclusion Policy Brief, 4(2).
This policy paper sheds light on the history leading up to the passage of TWWIIA in 1999 and describes the most important provisions of Medicaid buy-in policy. Current state policies and potential policy actions are also described. Available at communityinclusion.org/publications/text/pb9text.html
Hanes, P. & Folkman, J. (2003). State Medicaid Options that Support the Employment of Workers with Disabilities. Center for Health Care Strategies, Inc. (24 pages).
This paper describes the experiences of seven states in implementing Medicaid Buy-In for people with disabilities. The authors present a summary and history of the Medicaid Buy-In and then address several policy questions related to its implementation such as the intended scope of the Buy-In, its early signs of success/failure, and the role of both employers and employees in facilitating its implementation. Available at chcs.org/usr_doc/BuyIn.pdf
Jensen, A., Silverstein, R., Folkemer, D., & Straw, T. (2002). Policy Frameworks for Designing Medicaid Buy-In Programs and Related State Work Incentive Initiatives. U.S. Department of Health and Human Services. (45 pages).
This publication provides information for state policymakers and administrators in the design and implementation of Medicaid Buy-In and other work incentive programs for individuals with disabilities. It focuses on the issues of cost, enrollment, and the relationship between cash assistance programs (SSI, SSDI, and state supplements) and health care entitlement programs (Medicaid and Medicare). The report details experiences in nine states that were among the first to implement Medicaid Buy-In programs and outlines decision pathways that states can use to guide them through the buy-in design process. Available at aspe.hhs.gov/daltcp/reports/polframe.htm
Wiener, J. (2003). Medicaid and Work Incentives for People with Disabilities: Background and Issues. Washington, DC: The Urban Institute. (76 pages).
This paper explains in detail the relationship between SSI and Medicaid, as well as employment incentive programs, including the Balanced Budget Act of 1997, the Ticket to Work Act, and the 1619(b) provision of the Social Security Act. It offers examples of how states have implemented various employment incentives, and issues they have or may face, including horizontal equity, fiscal pressures and shortfalls, sufficient breadth and depth of coverages, and developing a reasonable and fair definition of disability. The paper includes several state-by-state charts with information about eligibility criteria, 1619(b) thresholds, and buy-in policies. Available at urban.org/UploadedPDF/410814_Medicaid_Incentives.pdf
Endnotes
-
This chapter is based in large part on the especially clear description of Medicaid eligibility authored by Letty Carpenter in Chapter 2 (Financial Eligibility Rules and Options) in Gary Smith, Janet OKeeffe, Letty Carpenter, Pamela Doty, Gavin Kennedy, Brian Burwell, Roberta Mollica, and Loretta Williams (2000). Understanding Medicaid Home and Community Services: A Primer. George Washington University, Center for Healthy Policy Research. Available at http://aspe.hhs.gov/daltcp/reports/primer.htm (accessed February 22, 2005).
-
Based on: Andy Schneider, Risa Elias, and Rachel Garfield (2002). "Chapter 1: Medicaid Eligibility" in: Schneider, A., Elisa, R., Garfield, R., et al. (2002). The Medicaid Resource Book. Menlo Park CA: The Kaiser Commission on Medicaid and the Uninsured.
-
Legal immigrants who entered the U.S. before August 22, 1996 must also meet the definition of a "qualified immigrant" in order t be eligible for Medicaid. A qualified immigrant is one whose category of immigration status is (a) Legal Permanent Resident (LPR), (b) Refugee, (c) Asylee, or one of several other categories. Immigrants deemed "nonqualified" are not eligible for basic Medicaid services regardless of legal status. Non-qualified immigrants are either (a) a Person Residing Under Color of Law (PRUCOL), (b) undocumented or (c) a non-immigrant such as a student or foreign visitor. For more detailed information, please see the National Health Law Program paper Immigrant Access to Health Benefits: A Resource Manual, available at www.accessproject.org/downloads/Immigrant_Access.pdf
-
In particular, please see the following: (a) United States Government Accounting Office (2002). Welfare Reform: Outcomes for TANF Recipients with Impairments. (GAO-02-884); (b) National Council on Disability (2003). TANF and Disability -- Importance of Supports for Families with Disabilities in Welfare Reform; (c) Office of Inspector General, U.S. Department of Health and Human Services (2002). State Strategies for Working with Hard-to-Employ TANF Recipients. (OEII-02-00-00630); and, (d) Eileen P. Sweeney (2000). Recent Studies Indicate that Many Parents Who are Current or Former Welfare Recipients have Disabilities or Other Medical Conditions. Washington DC: Center on Budget and Policy Priorities. Some studies have found that the incidence of mental impairments among adults in TANF households ranges from 30 to 40 percent.
-
Federal law concerning the Supplemental Security Income program is in Title XVI of the Social Security Act.
-
The Adult Listings are contained in the Social Security Administrations publication Disability Evaluation Under Social Security (also known as the Blue Book). The publication is available at ssa.gov/disability/professionals/bluebook. Mental disorders include mental retardation, organic brain disorders and mental illnesses, among others.
-
The Diagnostic and Statistical Manual (DSM) is updated periodically. The Listings of Mental Impairments parallels the DSM-III, which was used in the mid-1980s. The current version used by mental health professionals is the DSM-IV.
-
Children (individuals under age 18) are not subject to the substantial gainful activity test. Instead, they are evaluated on the basis of whether their impairment(s) result in marked and severe functional limitations.
-
From 1982 through June 1999, the SGA standard remained unchanged at $500 per month. In July 1999, the standard was increased to $700 per month and indexed to the year-over-year change in the national average worker wage index. The SGA standard also applies to SSDI beneficiaries.
-
Federal law concerning the Social Security Disability Insurance program is in Title II of the Social Security Act.
-
Social Security Administration (2002). Annual Statistical Supplement. Table 7.F2.
-
Social Security Administration (2002). Annual Statistical Supplement. Table 3.C61.
-
Information here and elsewhere in this chapter about state policies concerning Medicaid eligibility for adults with disabilities, is generally based on information compiled by the National Association of State Medicaid Directors (NASMD) and available at nasmd.org/eligibility/. The NASMD information was compiled in 2001 but is updated periodically.
-
§1634 of the Social Security Act permits the Social Security Administration to enter into an agreement with a state for this purpose.
-
Connecticut, Hawaii, Illinois, Indiana, Minnesota, Missouri, New Hampshire, North Dakota, Ohio, Oklahoma, and Virginia.
-
SSI payment amounts are adjusted annually in January based on changes in the consumer price index.
-
Unlike the FBR and SGA limits, the SSI resource limit is not indexed and has remained unchanged for many years.
-
Section 209(b) refers to the section of the Social Security Act Amendments of 1972 that gave states this option. This provision is contained in §1902(f) of the Social Security Act.
-
For example, SSI is based on whether a persons disability will cause substantial impairment for at least 12 months. In Indiana and New Hampshire, the expected duration of the impairment must be at least 48 months.
-
See also: CMS/CMSO/Disabled and Elderly Health Programs Group (June 2002). Groups Deemed to be Receiving SSI for Medicaid Purposes. See also: Robert Bohlman, National Alliance for the Mentally Ill -- Switch from SSI to SSDI Does Not Mean Loss of Medicaid at nami.org/Content/ContentGroups/Enews/1996/December_1996/Switch_From_SSI_To_SSDI_Does_Not_Mean_Loss_Of_Medicaid.htm
There are three eligibility groups for whom Medicaid must continue after SSI is lost: (a) People who lost SSI when they received automatic cost-of-living adjustments (COLAs) in Social Security (sometimes nicknamed Pickle people after Congressman Pickle, one of the sponsors of the original COLA legislation); (b) Adult children with disabilities who lose SSI when they become entitled to Social Security benefits based on a parents Social Security entitlement. Adult children with disabilities are individuals who have a disability before age 22.
When such a persons parent becomes disabled, retires or dies, the individual becomes eligible for SSDI. If an individual had an SSI benefit, then the SSDI benefit -- if sufficiently large -- completely replaces SSI. Federal law requires that these individuals continue to be considered SSI beneficiaries and receive Medicaid coverage; and, (c) Individuals ages 60-64 who lose SSI due to receipt of Social Security benefits for widows and widowers with disabilities.
-
The Employment Opportunities for Disabled Americans Act of 1986 (P.L. 99-643).
-
In January 2004, the Social Security Administration published proposed rules concerning the treatment of assets in determining SSI eligibility. These proposed rules would (a) exclude household goods and personal effects from countable resources and (b) remove the dollar value limit on a persons personal vehicle. Federal Register, Vol. 69, No. 3, pp. 554-558 (January 6, 2004).
-
Also in the Employment Opportunities for Disabled Americans Act of 1986. The enactment of these provisions followed demonstrations that began in 1980. In 1982, these options moved to full implementation nationwide. However, it was not until 1986 that these provisions were made permanent.
-
Center for Workers with Disabilities (2002). Work Incentives Development Report Series: Section 1619(b) Operational Challenges and Selected State Remedies. Washington DC: National Association of State Medicaid Directors. This series of reports contains extensive information concerning Section 1619(b) eligibility and some of the problems encountered in its implementation. The series is available at nasmd.org/disabilities/pubs/special.asp
-
Social Security Administration. 2002 SSI Annual Report.
-
More detailed information concerning the latitude afforded states under §1902(r)(2) may be found in the following publications: (a) Center for Workers with Disabilities (2002). Building Work Incentives Using Section 1902(r)(2) of the Medicaid Statute. Washington, DC: National Association of State Medicaid Directors, available at nasmd.org/disabilities/pubs/special2.pdf; and, (b) CMS (2001) Medicaid Eligibility Groups and Less Restrictive Methods of Determining Countable Income and Resources: Questions and Answers. Available at cms.hhs.gov/medicaid/eligibility/elig0501.pdf
-
Federal Register, January 11, 2001, pps. 216-2322. These rules are located at 42 CFR Part 435.
-
The Federal Poverty Level is higher in Alaska and Hawaii. ($11,210 and $10,330, respectively, in 2004 for one person).
-
California, District of Columbia, Florida, Hawaii, Illinois, Maine, Massachusetts, Michigan, Minnesota, Mississippi, Nebraska, New Jersey, North Carolina, Oklahoma, Pennsylvania, Rhode Island, South Carolina, Utah and Virginia.
-
For more information on the medically needy option, including the states that offer this option and the characteristics of their programs, please see: Jeff Crowley (2003). Medically Needy Programs: An Important Source of Medicaid Coverage. Washington DC: Kaiser Commission on Medicaid and the Uninsured, available at kff.org/medicaid/4096-index.cfm
-
For example, Louisiana has excluded mental health services as well as others; some states do not include prescribed drugs.
-
A 209(b) state may elect to use a different income or resource standard for the aged, blind and disabled than the standard that is used for AFDC-related individuals.
-
Typically this is every month. In some states, it is every six months. But in the latter case, the person must be able to spend-down an amount that equals six times their monthly excess income before becoming eligible.
-
A persons share of cost obligation is reduced when the person has a spouse or other dependents.
-
States at their option may disregard a certain amount of income for waiver beneficiaries to support themselves and any dependents in the community. This amount is typically called a personal maintenance allowance. The amount of income remaining after subtracting the personal maintenance allowance and the allowance for dependents is the cost-sharing obligation. States vary in the amount of the maintenance allowance they allow, from $800 to $1,737 (the full 300 percent of SSI standard).
-
There is extensive information concerning these options at the CMS web site cms.hhs.gov/twwiia/default.asp. There also are considerable resources available on the Center for Workers with Disabilities web site: nasmd.org/disabilities/about/altdefault.asp
-
More information concerning state initiatives to promote employment for people with disabilities through Medicaid buy-in options and other strategies is available from the National Association of State Medicaid Directors Center for Workers with Disabilities at nasmd.org/disabilities/taskforces/altdefault.asp
-
More information concerning these grants is located at cms.hhs.gov/twwiia/infrastra.asp
-
Jean P. Hall and Michael H. Fox (2002). Working Healthy -- A Medicaid Buy-In for Kansas. Univesrity of Kansas Department of Health Policy and Management.
-
Jean P. Hall and Michael H. Fox (2003). Early Enrollment in Working Healthy: Program Features Make A Difference. Univesrity of Kansas Department of Health Policy and Management.
-
P.L. 106-170.
-
For a table comparing the features of BBA and TWWIIA (Basic and Medical Improvement), please see: cms.hhs.gov/twwiia/comchart.asp
-
Periodic continuing disability reviews assess whether individuals still meet SSI/SSDI eligibility criteria.
-
SSDI beneficiaries whose earnings exceed the SGA standard enter what is termed a Trial Work Period. Once that Trial Work Period is completed and the persons earnings continue to exceed the SGA standard, the person faces the potential termination of SSDI. SSDI does not have a provision similar to 1619(a) that benefits SSI beneficiaries.
-
Contained in §1931 of the Social Security Act.
-
In particular, please see the following: (a) United States Government Accounting Office (2002). Welfare Reform: Outcomes for TANF Recipients with Impairments. (GAO-02-884); (b) National Council on Disability (2003). TANF and Disability -- Importance of Supports for Families with Disabilities in Welfare Reform; (c) Office of Inspector General, U.S. Department of Health and Human Services (2002). State Strategies for Working with Hard-to-Employ TANF Recipients. (OEII-02-00-00630); and, (d) Eileen P. Sweeney (2000). Recent Studies Indicate that Many Parents Who are Current or Former Welfare Recipients have Disabilities or Other Medical Conditions. Washington DC: Center on Budget and Policy Priorities. Some studies have found that the incidence of mental impairments among adults in TANF households ranges from 30 to 40 percent.
-
Dee Mukherjee, National Association for the Mentally Ill. New Law Denies SSI, SSDI to Those with Alcoholism and Drug Addictions.
-
A complete discussion of the effects of incarceration on SSI, SSDI and Medicaid benefits is found in the following publication: Bazelon Center for Mental Health Law. Finding the Key to Successful Transition from Jail to the Community -- An Explanation of Federal Medicaid and Disability Program Rules. Washington, DC.
-
More information on the interplay between SSI, Medicaid, and incarceration can be found in the Bazelon Center for Mental Health Law publication, Arrested? What Happens to Your Benefits If You Go to Jail or Prison?, (2004). Washington, DC. Available at bazelon.org/issues/criminalization/publications/arrested/index.html
-
As an example, in November 2004 Utah allowed inmates to re-apply for Medicaid six weeks before their anticipated release date in order to facilitate a smooth transition into Medicaid services. In addition, Utah provides presumptive Medicaid eligibility to inmates who normally must wait until a 90-day disability evaluation is completed, if they were deemed disabled prior to being incarcerated. This covers a large number of individuals with serious mental illnesses.
-
Individuals in this age cohort are affected by the IMD exclusion, as discussed in Chapter 4.
CHAPTER 4: MEDICAID COVERAGE OF MENTAL HEALTH SERVICES
| States may offer a wide range of services to Medicaid beneficiaries. Commonly, states employ certain Medicaid coverages to support working age adults with serious mental illnesses in the community. Other Medicaid coverages can also play a vital role in assisting individuals. This chapter provides basic information concerning Medicaid service coverages that are especially relevant for supporting persons with serious mental illnesses in the community. |
Medicaids role in supporting working age adults with serious mental illnesses hinges on the services that a state includes in its Medicaid program. Federal Medicaid law does not spell out a predefined set of distinct mental health services. Instead, mental health services may be furnished under several general coverage categories, some of which are mandatory and others optional. For example, psychiatrist services fall under the broad mandatory physician services category. Services such as Assertive Community Treatment may be furnished under the optional rehabilitative services coverage. Three optional Medicaid coverage categories -- clinic (outpatient) services, rehabilitative services, and targeted case management -- figure prominently in the provision of community mental health services. Other Medicaid coverages (e.g., prescribed drugs) also play vital roles in meeting the needs of individuals with serious mental illnesses.
This chapter begins with a brief discussion of Medicaid coverage policies. It then provides an overview of pertinent Medicaid coverages for supporting people with serious mental illnesses in the community. Next, it provides more detail concerning federal policies that apply to these coverages, including the types of services that may be furnished under them, as well as coverage requirements and limitations. Examples illustrate how individual states have employed these coverages. Chapter 5 further illustrates how states have fashioned their Medicaid coverages of community mental health services under the rehabilitative services and targeted case management options.
Medicaid Coverage Policies
Coverage refers to the services that a state includes in its Medicaid state plan. The federal Medicaid statute (principally in §1905) lists the services for which federal financial participation is available. When a state covers a service in its Medicaid state plan, it commits to making that service available to all beneficiaries who require it.
The extent of federal policies concerning the coverage of specific services varies. In the case of certain coverages, Congress has enacted detailed requirements. For example, federal statutory and regulatory requirements regarding nursing facility services are quite detailed. In other cases, however, Medicaid law describes relatively broad coverage parameters and, thereby, states have considerable latitude in fashioning the services that they offer under these coverage categories. This is especially the case with respect to rehabilitative services where federal law and regulations spell out the essential features of the coverage but otherwise do not prescribe their exact scope.
As discussed in Chapter 2, there are certain fundamental federal statutory requirements (e.g., comparability and statewideness) that apply to Medicaid state plan services, regardless of type. Unless a state is operating services under a waiver authority (see Chapter 6), its Medicaid coverage must comply with these requirements in order for the state to obtain federal financial participation for the costs of services it furnishes to beneficiaries. These requirements are discussed here.
Statutory Purpose
The federal Medicaid statute (along with federal regulations and, in some cases, additional CMS guidance) describes the intended purpose of each coverage. For example, in the case of targeted case management (TCM) services, the statute describes their purpose as assist[ing] individuals eligible under the plan in gaining access to needed medical, social, educational, and other services. In order for a state to gain CMS approval to offer TCM services, the specific services it intends to offer must comport with this expressed purpose. Because the TCM coverage is limited to assisting individuals to access various types of services, it may not be employed to furnish direct hands-on assistance to persons, conduct prior authorization activities, or determine eligibility. Such activities can be provided under other coverages or as a Medicaid administrative cost. Fundamentally, a states proposed coverage must align with the expressed statutory purpose. Sometimes, this causes a state to have to employ two or more coverages in order to furnish a desired array of services.
Coverage Content
When a state proposes a coverage, CMS expects that a state will spell out the services it intends to offer in reasonable detail in its Medicaid plan or related policies and procedures. This detail includes the specific services that will be furnished under the coverage, provider qualifications, and the criteria that a state will use in determining the medical necessity of the service. For example, a state may not simply indicate that it will cover rehabilitative services. Instead, the state must spell out the specific components of rehabilitative services that it will offer. These services must be defined in sufficient detail to make it clear what will be furnished to individuals and under what conditions.
CMS review of a proposed coverage is based on whether the coverage comports with federal law and regulations rather than on judgments concerning the appropriateness of the coverage. For example, some observers question the value of day treatment services as a means of supporting working-age adults with serious mental illnesses. However, as long as a states coverage of such services meets the essential requirements, CMS is obliged to approve the coverage.
CMS review of proposed coverages considers each states proposal on its own merits. In this vein, the coverages approved by CMS in other states may provide useful information when fashioning a coverage. However, CMS officials caution that replicating an existing coverage from another state will not necessarily expedite CMS review and approval. Nonetheless, CMS has expressed a strong interest in working with and assisting states in fashioning coverages that embrace the principles of recovery and reflect what works in effectively meeting the needs of beneficiaries, including working-age adults with serious mental illnesses.
It is important to keep in mind that Medicaid functions as a source of funding for services that meet federal statutory requirements rather than as a defined program. It is up to each state to determine what it will include in its coverage and the practice standards it will adopt. For example, a state has the latitude to establish clinical pathways in order to ensure that the correct mix and sequence of services are furnished to individuals based on their assessed needs. It is up to each state to craft its coverage in the context of its own programmatic goals and objectives for mental health services.
Medical Necessity
As previously discussed, Medicaid operates within a medical necessity framework. That is, services must be necessary to address a beneficiarys health condition or fulfill a rehabilitative purpose. With respect to many Medicaid services, states have latitude to establish medical necessity criteria and institute processes for determining when such criteria are met. One way that states define medical necessity is to establish what are sometimes termed service eligibility criteria. For example, in the case of ACT (Assertive Community Treatment) services, service criteria often include a history of frequent psychiatric emergencies. For other mental health services, service eligibility criteria may include particular diagnoses, treatment history (e.g., frequent hospitalization), whether an individuals assessed needs and level of functioning meet a predefined threshold level, and others. Service eligibility criteria are a means for states to assure that individuals receive appropriate services and to manage utilization.
In a somewhat similar vein, medical necessity criteria also may include what are termed step-downs. That is, an individual might be approved to receive especially intensive services for a limited period of time and then shift to a lesser intensity service once his or her condition is stabilized and/or improved.
A state also can establish various processes to determine medical necessity. These processes may include prior authorization and utilization review by the state itself or a contracted third party entity. In some cases, states permit a service to be furnished for a limited period of time or a fixed number of units without prior authorization, but require review for service continuation once the initial period is up or the unit limitation has been reached. In other cases, the provision of intensive services (e.g., those that constitute ACT) may be subjected to periodic review and reauthorization. Again, the rationale for these processes is to assure that individuals are receiving appropriate and necessary services.
Medical necessity is also frequently assessed in the context of the review and approval of an overall treatment plan developed by mental health professionals. In other words, the services that are furnished to the individual must be shown to address assessed needs identified during the treatment planning process.
Benefit Limits
Related to but distinct from medical necessity criteria are limits that a state may impose on the benefits that it offers. Federal law requires that each service that a state covers in its Medicaid program must be sufficient in amount, duration and scope to reasonably achieve its purpose. However, there is no specific federal standard defining this requirement. Some states impose limitations on the amount, duration and scope of services, including the number of times that a beneficiary can be seen by a physician in a month or the number of drugs that may be prescribed and paid for a person each month.
For mental health services, states often impose limits on the number of outpatient visits or how many units of a service a person may receive each month or over a more extended period. However, states must provide a mechanism for individuals to seek additional care when needed over and above any limits. The imposition of such limits has been the subject of considerable litigation over the years and often is controversial. Such limits frequently are used as cost-containment devices. Some argue they can be counterproductive when they prevent an individual from obtaining vital services and contribute to preventable hospitalization or other negative outcomes. Effective utilization review techniques usually are more effective methods for ensuring that services are cost-effective.
Direct Benefit
Medicaid is a beneficiary-centered program and the services that a state offers must be furnished for the direct benefit of the beneficiary. For example, Medicaid state plan personal assistance services cannot be furnished for the sole purpose of providing respite to family caregivers. While family caregivers might benefit when personal assistance is furnished, the provision of this assistance must be based on the beneficiarys needs rather than those of the family caregivers. In mental health services, this requirement must be taken into account when a state offers family psychosocial education, as discussed in Chapter 5.
Providers
Finally, in proposing a coverage, a state must specify the providers of the service and their required qualifications. Especially with respect to rehabilitative services, states have substantial latitude in establishing provider qualifications.1 A state may require that providers possess and demonstrate critical competencies and capabilities by establishing provider standards and certification processes. Such standards obviously must comport with state law, and at the same time, be reasonably related to the requirements of the service itself, and must not arbitrarily disqualify otherwise qualified providers and individuals. For example, in the case of rehabilitative services, it is not permissible for a state to limit the providers of these services to community mental health centers or organizations that also receive funding from the state mental health authority. Any entity or individual who meets a states criteria and is willing to furnish Medicaid services must be allowed to become a provider.
Overview of Medicaid Coverages
As previously noted, federal Medicaid law does not specifically spell out a predefined set of community mental health services that a state may offer. States cover community mental health services under broad Medicaid coverage categories, none of which are reserved exclusively for community mental health services. Many types of services fit under these broad coverage categories. Table 4-1 on the following page links mental health and related services that states furnish to adults with serious mental illnesses to their typical Medicaid coverage categories.
It is useful to keep in mind that, in the Medicaid program (as with most types of health insurance), general practice physicians and other health care professionals frequently address the mental health care needs of beneficiaries apart from the mental health system. This care is not insignificant and plays an important role in addressing mental illnesses; however, it is not the primary focus of this Handbook. Basic coverages, such as psychiatrist services under the mandatory physician services category and psychologist services under the other practitioners category, can play an important role in supporting individuals with serious mental illnesses (e.g., medication management that requires the services of a health care professional). In the following sections, attention focuses on coverages that are most relevant in supporting working age adults with serious mental illnesses in the community: the rehab and clinic options, case management, prescribed drugs, inpatient hospital, and personal assistance. Substance abuse treatment services (for persons with co-occurring disorders) are discussed in detail in Chapter 5.
Not included in the list are institutional services. Federal law specifically prohibits Medicaid payment for ser-vices to individuals age 22 to 64 who reside in large mental health treatment facilities (labeled Institutions for Mental Diseases or IMDs) regardless of their length of stay in such settings. The IMD exclusion is described in more detail on the following page.
Medicaid will pay for services for individuals age 21 or younger who are served in psychiatric hospitals or psychiatric residential treatment facil-ities.
Many individuals with serious mental illnesses reside in nursing facilities, and there are federal regulations concerning the services that must be furnished to them. These are discussed in Chapter 7.
Dual Eligibles: Medicare/Medicaid Coverage
A significant number of Medicaid beneficiaries are dually eligible for Medicare. Though Medicare and Medicaid are distinct programs, they intersect in their coverage of certain benefits for dual eligibles. In some instances, both Medicare and Medicaid cover the same services, but Medicare does not cover mental health services furnished outside a hospital, clinic or practitioners office and does not cover rehabilitative or case management services.
| TABLE 4-1: Mental Health Servcies and Medicaid Coverage Categories | |||
|---|---|---|---|
| Service | Coverage Category | Mandatory | Optional |
| Psychiatrist | Physician Services | X | |
| Psychologist | Other Practitioners' Services | X | |
| Clinical Social Work | Other Practitioners' Services | X | |
| Hospitalization (Under age 65 with specific exceptions) | Inpatient Hospital | X | |
| Medications | Prescribed Drugs | X | |
| Personal Assistance | Personal Care | X | |
| Diagnosis | Diagnostic, screening, rehabilitative and preventive services | X | |
| Outpatient Mental Health Services | Outpatient hospital services | X | |
| Clinic Services ("Clinic option") | |||
| Community Support Services | Diagnostic, screening, rehabilitative and preventive services ("Rehab option") | X | |
| Substance abuse treatment | Clinic Services | X | |
| Diagnostic, screening, rehabilitative and preventive services | |||
| Service Coordination/Case Management | Targeted case management | X | |
Medicare mental health benefits have not been updated for a considerable period of time and cover only limited mental health services, which are described below.
- Inpatient Psychiatric Hospital Services. Medicare (Part A) covers inpatient psychiatric hospital services. A lifetime cap of 190 days applies to these services.
- Outpatient Services. Medicare (Part B) also covers mental health outpatient services furnished in clinics, hospital outpatient departments or practitioners offices, including individual and group psychotherapy, family counseling, partial hospitalization2 and other services. Recognized practitioners include psychiatrists, clinical psychologists, social workers, nurse specialists; nurse practitioners; and, physicians assistants.
Medicare beneficiaries who are not eligible for Medicaid are subject to Part A deductible and co-insurance requirements for inpatient services.
For Medicare outpatient mental health services, beneficiaries must pay a co-insurance of 50 percent (as opposed to the 20 percent co-insurance that applies to all other Part B benefits). Medicaid pays the deductibles and co-insurance for dual eligibles -- those Medicare beneficiaries who are also eligible for Medicaid.
Under Medicaids third-party liability requirements, Medicare certified providers are obligated to seek Medicare payment for services furnished to dual eligibles when the service is covered by Medicare. The amount that Medicare does not reimburse may then be billed to Medicaid. It is advantageous for states to secure Medicare payment for mental health services for dual eligibles because it lowers their costs. However, it causes problems for providers because of the length of time it takes to be reimbursed for their charges by both programs.
| The IMD Exclusion3 | |
| When the Medicaid program was launched in 1965, Congress intentionally excluded federal payment for services furnished to residents of large mental health facilities (termed "Institutions for Mental Disease" - IMDs), except, at state option, individuals age 65 and older with mental disorders.4 An IMD is defined as a hospital, nursing facility or other institution that is primarily engaged in providing diagnosis, treatment, or care of persons with "mental diseases," including medical attention, nursing care, and related services.5 The "IMD exclusion" stemmed from the longstanding view that the states - rather than the federal government - should have principal responsibility for the funding of specialized mental health hospital services.6 Congress also was concerned that permitting states to capture Medicaid dollars to underwrite the costs of their mental health facilities would lead immediately to higher federal Medicaid outlays.7 In 1972, federal law was changed to permit states to cover inpatient psychiatric hospital services (including residential treatment facilities) for children and youth under age 21.8 In 1988, federal law was again modified to define an IMD as a facility that had more than 16 beds.9 This change permitted individuals with mental illnesses who reside in smaller specialized mental health facilities and residences to receive Medicaid services, including mental health services. In sum, federal law does not allow Medicaid payment for services of any type furnished to any individual under age 65 who resides in an IMD, except for persons under age 21 who are served in a psychiatric hospital or private residential treatment facility. The IMD exclusion applies not only to the mental health services rendered by the IMD but also all other Medicaid services (including health care) for which individuals would be eligible if they were not in an IMD. The classification of a facility as an IMD includes assessing the character and purpose of the facility, its size and the make-up of its resident population. A facility (including a nursing facility) is deemed to be an IMD if more than 50 percent of its residents have mental disorders.10 While federal law prohibits Medicaid payment for the direct services furnished to IMD patients, states may make Medicaid disproportionate share hospital (DSH) payments to IMDs. These are lump sum payments rather than payments for services rendered to specific IMD residents. Between 1997 and 2002, DSH payments to IMDs averaged approximately $3.3 billion annually.11 These payments are subject to federal ceilings and flow principally to public (state and local) IMDs. In the past, CMS permitted states to purchase services from IMDs through Medicaid managed care waiver programs. However, CMS now is requiring these states to end such payments when these waiver programs are renewed because of the IMD exclusion. The IMD exclusion has several implications over and above removing IMDs as a setting where Medicaid reimbursable services may be furnished. One effect is that Medicaid payments for the hospitalization of working age adults are limited to short-stay acute care services furnished in inpatient psychiatric units of general hospitals, so long as such units themselves are not IMDs. Larger state or locally-operated mental health facilities cannot receive Medicaid payment when they furnish similar services to individuals because of the IMD exclusion. Of possibly greater importance is that the IMD exclusion limits states' ability to make use of the Medicaid 1915(c) HCBS waiver authority as a means of underwriting services and supports for working age adults with serious mental illnesses. The §1915(c) waiver authority permits a state to offer home and community services to persons who otherwise would qualify for services in a Medicaid-covered institutional setting (a nursing facility, ICF/MR, or hospital). As a consequence of the IMD exclusion, it is not possible for a state to operate an HCBS waiver program to serve as an alternative to mental health institutional services for working age adults with serious mental illnesses. As discussed in Chapter 6, the use of the HCBS waiver authority can be employed to support adults with serious mental illnesses who meet nursing facility level of care criteria. The HCBS waiver authority has been used more extensively to furnish home and community services to children and youth with severe emotional disturbances12 because Medicaid payment is allowable for services furnished to children and youth in inpatient psychiatric hospitals. |
Detailed Discussion of Medicaid Mental Health Coverages
This section describes in detail federal policies that apply to the principal coverage categories through which community mental health services are furnished to working age adults with serious mental illnesses. It includes information on applicable federal law, regulations, and other CMS guidance concerning each coverage category. State examples are also provided.
As a general matter, a full-featured, comprehensive approach to employing Medicaid funding in support of working-age adults in the community could include: (a) a robust rehabilitative services benefit; (b) targeted case management services; (c) ready access to prescribed drugs associated with the treatment of mental illnesses; (d) inpatient hospital services as necessary; and, (e) personal assistance services to address dimensions of community living that are outside the scope of the rehabilitative services benefit. The linchpin of a full-featured Medicaid mental health services strategy is the rehabilitative services option.
Clinic vs. Rehab Option: Differences
The main Medicaid coverages that states employ to furnish community mental health services are (a) clinic services (often referred to as the clinic option and (b) rehabilitative services (the rehab option). Each is described in more detail below. Here, these two coverages are compared and contrasted. While either option can serve as a vehicle for securing Medicaid funding for mental health treatment, there are important differences between the coverages, as summarized in the insert below. It is worth noting that services which can be provided under the clinic option also may be furnished under the rehab option but not necessarily vice versa.
One of the main differences between the options is the location of services. Except for services furnished to homeless individuals, clinic services must be furnished on-site at the clinic. Under the rehab option, services may be furnished to individuals in their own home, a community living arrangement and other community locations as well as at fixed mental health program sites or locations. It is for this reason that the rehab option is regarded as more congruent with the principles of Community Support Services (CSS) and recovery.
| Clinic v. Rehab Option13 | |
|---|---|
| Clinic Option | Rehabilitative Services Option |
| Medical model | Recovery model |
| Stabilization | Active treatment and participation |
| Clinic based | Community based |
| Licensed and higher degreed professionals | Professionals, mental health technicians, and peer specialists |
| Organized clinics/outpatient programs | Organizations that provide one or more covered services |
Also, the clinic option requires a high level of direct physician (e.g., psychiatrist) involvement in the provision of services, either by direct service provision or close supervision of staff-furnished services. Under the rehab option, licensed medical and mental health professionals play important roles (through the development and monitoring of individual program plans and the provision of services reserved to them under state law), but they need not always be directly involved in day-to-day service delivery, which may be carried out by a variety of qualified personnel, including Qualified Mental Health Professionals (QMHPs), appropri-ately qualified community workers, and peer specialists. Under the rehab option, a state can draw from a larger provider pool, thereby improv-ing consumer choice and overall system capabilities.
Finally, the clinic option is more or less confined to the provision of a relatively narrow array of psychiatric services and, thereby, is often portrayed as a medical model. In contrast, the rehabilitative services option spans a broader range of services and supports, including psychosocial rehabilitation and other key components often associated with recovery.
Federal law does not dictate that a state must choose between the clinic and rehabilitative services options. The two can and do operate side-by-side in many states. Many states reserve the provision of rehabilitative services for individuals with serious mental illnesses while making clinic services more broadly available to Medicaid beneficiaries whose mental health treatment needs can be addressed on an outpatient basis. Alternatively, some states (e.g., Georgia) have elected to unify their coverage of mental health services under the rehab option.
Outpatient Mental Health Services
In the past, many states used either the optional clinic coverage or the mandatory outpatient hospital coverage, or both, as their main vehicle(s) to qualify outpatient mental health services for Medicaid payment. Many states retain the clinic option, but several have dropped it in favor of the more comprehensive and flexible rehabilitative services option.14 The clinic option is a broad Medicaid coverage. It is not reserved solely for mental health services. Other health care services may be furnished under the clinic option as well, including ambulatory services, surgical care, and substance abuse treatment.
| Clinic Services | |
| Social Security Act: §1905(a)(9) "clinic services [are those] furnished by or under the direction of a physician, without regard to whether the clinic itself is administered by a phys-ician, including such services furnished outside the clinic by clinic personnel to an eligible individual who does not reside in a permanent dwelling or does not have a fixed home or mailing address." |
The primary distinction between the mandatory outpatient hospital coverage15 and the optional clin-ic coverage16 relates to the nature of a provider entity. Outpatient hospital services are operated as an adjunct to an inpatient hospital. A typical outpatient service is partial hospitalization. Clinics, on the other hand, are freestanding entities. States commonly employ the clinic option to provide outpatient mental health services, often through their network of community mental health centers and/or other similar organizations.
CMS has issued guidance (in the State Medicaid Manual -- included in Appendix A) concerning the provision of outpatient psychiatric services that applies equally to services furnished under the out-patient hospital coverage and the clinic option coverage. This guidance clarifies that
- Psychiatric services rendered to Medicaid beneficiaries must be closely related to the persons psychiatric condition;
- Admission for services must be based on an intake evaluation that evaluates the recipient's mental condition and, based on the patient's diagnosis, determines whether treatment in the outpatient program would be appropriate. Moreover, the assessment should include a certification by the evaluation team that the program is appropriate to meet the recipient's treatment needs;
- Services must be furnished as specified in an individual plan of care (POC). This consists of a written, individualized plan to improve the patient's condition to the point where the patient's continued participation in the program (beyond occasional maintenance visits) is no longer necessary. The POC contains a written description of the treatment objectives for that patient. The plan also should describe: (a) the treatment regimen; (b) projected service delivery schedule; (c) the personnel who will furnish services; and (d) when reevaluations will be conducted to update the POC;
- The POC must be reviewed no less frequently than every 90 days by an evaluation team; and,
- Any services furnished to an individual that depart from the treatment plan (e.g., emergency services) must be thoroughly documented when billed.
This CMS guidance makes it clear that outpatient psychiatric services are limited to the provision of treatment for the persons psychiatric disorder rather than to support broader rehabilitative purposes.
Treatment services provided under the clinic option (e.g., therapeutic services) must be performed directly or supervised by qualified professionals, and federal rules require that ultimate responsibility for services provided lies with a licensed physician. Virginia, for example, requires that services be rendered or supervised by (a) licensed physicians who have completed three years of post-graduate residency training in psychiatry; or (b) licensed clinical psychologists, clinical social workers, licensed professional counselors and clinical nurses with a psychiatric specialty. Unlicensed personnel may furnish services but must be supervised by qualified professionals.
Virginias coverage of mental health clinic services illustrates how this coverage is often fashioned.17 (Virginia also covers an array of community rehabilitative services for persons with serious mental illnesses.) In particular:
- Clinic services are available for persons with a psychiatric diagnosis who exhibit deficits in four areas that result in functional limitations;18
- The services that may be furnished include: (a) individual psychotherapy; (b) group psychotherapy; (c) pharmacologic management; (d) family therapy (provided that it is not furnished to groups of families); and, (e) testing and diagnosis. Services must be spelled out in a plan of care that is signed by a qualified professional, and the plan of care must be reviewed no less frequently than every 90 days or every sixth session, whichever time frame is shorter;
- Specifically excluded from coverage is the teaching of life-related skills because they are not considered psychotherapy;
- Virginia limits outpatient mental health services to 26 visits per year and services must be pre-authorized.
Virginias mental health clinic services coverage is roughly similar to mental health services offered under commercial health insurance plans. Parallel requirements attach to services provided by freestanding mental health practitioners (e.g., psychiatrists) who are not associated with a clinic. Virginias coverage of clinic services is a basic mental health benefit. The states rehab option is designed to serve individuals who require more intensive services. Outpatient mental health/ psychiatric services are frequently needed to treat individuals with serious mental illnesses. The main drawback to using the clinic option to provide them is the limited scope of services that may be furnished, and the inability to provide them in a wide range of home and community settings.
Rehabilitative Services
The coverage of rehabilitative services is the most important Medicaid option for working-age adults with serious mental illnesses. This coverage (§1905(a)(13) of the Social Security Act; 42 CFR 440.130(d)) permits a state to offer a wide range of services throughout the community. In many states, this coverage is reserved for and underwrites community support services for individuals with serious mental illnesses who require especially intensive supports to aid their recovery. Mental health rehabilitative services generally are not employed in support of individuals whose needs can be met through the provision of basic counseling and psychotherapy services.
| Rehabilitative Services | |
| Social Security Act: §1905(a)(13) "Other diagnostic, screening, preventive, and rehab-ilitative services, including any medical or remedial services (provided in a facility, a home, or other setting) recommended by a physician or other licensed practitioner of the healing arts within the scope of their practice under State law, for the maximum reduction of physical or mental disability and restoration of an individual to the best possible functional level." |
A full-featured, comprehensive coverage of rehabilitative services for individuals with serious mental illnesses will include:
- Diagnosis and assessment
- Individual and group clinic outpatient mental health services
- Crisis services
- Family psychosocial education
- Peer support19
- Life skills training and support across a variety of community living dimensions
- Assertive Community Treatment with the capability to step down yet maintain intensive support as needed
- Medication education and management
- Community residential services and supports
- Illness and disability management
- Supported employment
In Chapter 5, more information is provided concerning many of these key components of comprehensive coverage. This array of rehabilitative services should be complemented by other Medicaid services: i.e., inpatient hospital as needed, case management/service coordination, substance abuse treatment, and access to prescribed drugs used in the treatment of mental illnesses (as well as medication management). Providing a comprehensive array of mental health rehabilitative services equips a system with wide-ranging capabilities that can be tailored to meet the specific needs of each individual. Individualized assessment and planning identify the specific rehabilitative services (along with other Medicaid and non-Medicaid supports) that will best address the needs of each person.
The Medicaid statute does not limit the coverage of rehabilitative services solely to mental health services. States offer other types of rehabilitative services in their Medicaid programs, including substance abuse treatment and physical rehabilitation services (e.g., occupational therapy and physical therapy.) However, the coverage of mental health services is among the most common uses of the rehabilitative services coverage. Today, nearly every state employs the rehabilitative services option to underwrite services and supports for individuals with mental illnesses. However, states vary in the scope of services that they offer under the rehab option.
The statutory and parallel regulatory provisions regarding rehabilitative services are brief. They have the following practical meanings:
- A rehabilitative service must involve the treatment or remediation of a condition that results in an individuals loss of functioning and, therefore, the service must be restorative or remedial. Federal policy distinguishes between rehabilitative and habilitative services. Habilitative services typically are furnished to individuals with intellectual or cognitive disabilities (e.g., mental retardation). Persons who have experienced a brain injury may also benefit from habilitation. Habilitative services are designed to assist individuals in acquiring, retaining, and improving the self-help, socialization, and adaptive skills. Habilitation services are not restorative or remedial because they are intended to aid individuals to gain new skills rather than restore previous functioning levels. Habilitation may not be covered as a rehabili-tative service.
- In the case of rehabilitative services for persons with serious mental illnesses, licensed practitioners of the healing arts (LPHAs) include psychiatrists, psychologists, licensed clinical social workers, registered nurses and advance practice nurses. Federal law allows LPHAs to recommend services. This recommend clause is generally interpreted by states to involve activities such as: (a) evaluation and diagnosis; (b) development and/or approval of a persons service plan; and, (c) ongoing review to determine the continued need for services.20 It is important to note that neither the statute nor the regulations mandate that a psychiatrist or psychologist directly furnish or oversee the day-to-day provision of a rehabilitative service. This contrasts with the clinic option where a qualified professional (e.g., a psychiatrist or other licensed practitioner) must furnish the service directly or closely supervise its provision by unlicensed personnel, and a licensed physician retains ultimate clinical responsibility.
- The statute specifically provides that rehabilitative services may be furnished in a variety of community locations, including an individuals home. Unlike the clinic option, the provision of rehabilitative services is not tethered to a clinic site. This is one reason why the rehabilitative services option is so well suited to implementing the community support services concept, where the emphasis is on bringing services to individuals in their homes and elsewhere in the community. For example, in the provision of crisis services, under the rehabilitative services option, a crisis team may be dispatched to assist a person in his or her living arrangement and continue to support the person until the crisis has abated. Under the clinic option, a team may be dispatched to assist the person but the person must be transported to the clinic for ongoing services.
To date, CMS has not published additional guidance in the form of a State Medicaid Manual transmittal concerning the coverage of mental health rehabilitative services. However, it has issued other guidance.
In 1992, the Director of the HCFA Medicaid Bureau (now CMS) issued an information memorandum to Regional Administers concerning services for persons with mental illnesses that could be included under the optional rehabilitation benefit. (This letter is included in Appendix A).
The main points made in this memorandum include the following.
- In deciding whether a service could be offered under this coverage, states were advised that while it is not always possible to determine whether a specific service is rehabilitative by scrutinizing the service itself, it is more meaningful to consider the goal of the treatment. Services necessary for the treatment of mental illness may be coverable as rehabilitative services.
- Examples of services that could potentially be covered as rehabilitative services were provided, including:
- Basic Skills Training -- the restoration of those basic skills necessary to independently function in the community, including food planning and preparation, maintenance of living environment, community awareness and mobility skills.
- Social Skills -- Redevelopment of those skills necessary to enable and maintain independent living in the community, including communication and socialization skills and techniques.
- Counseling and Therapy -- Services directed toward the elimination of psychosocial barriers that impede the development or modification of skills necessary for independent functioning in the community.
- The memorandum cautioned that services unrelated to the treatment of mental illnesses fall outside the scope of rehabilitative services. For example, the provision of personal assistance services to assist a person in an activity of daily living may not be covered as a rehabilitative service. Such services must be covered elsewhere in the state plan as personal care services. This guidance means that a states coverage of rehabilitative services cannot mix treatment with other non-treatment or unrelated services. This does not mean that such services cannot be provided to individuals but, in order to do so, they must be covered through alternative means. The memorandum distinguished between providing assistance (such as meal preparation) for the individual (personal assistance) as opposed to teaching meal preparation skills to the person (rehabilitation).
- States were advised that job training, vocational and educational services may not be provided as rehabilitative services. This exclusion arises from the long-standing federal policy prohibition against Medicaid funding for purely vocational services. However, this prohibition does not preclude the provision of services that might assist individuals to function in the work place, provided that the services furnished are not directly associated with specific job performance.
- The memorandum noted that case management-type services could be covered as rehabilitative services so long as they were confined to managing Medicaid covered services (e.g., coordinating the provision of several rehabilitative services). However, where case management involves assisting individuals to obtain non-Medicaid services (e.g., housing), it cannot be covered as a rehabilitative service (although it could be covered as targeted case management services -- see the discussion of service coordination/ case management below). For this reason, states commonly cover targeted case management services side-by-side with rehabilitative services.
- The memorandum also pointed out that rehabilitative services must be furnished exclusively for the benefit of the individual with the mental illness. While such services could include consultation and training of others who are important in the persons life (e.g., spouse and/or other family members), the memorandum cautioned that services could not include the treatment of these other individuals except to the extent that they also qualify for rehabilitative services.
- Additionally, the memorandum cautioned that a state may not arbitrarily limit the providers of rehabilitative services (e.g., only permit community mental health centers to provide services) except when the state has an approved freedom of choice waiver. A state may specify reasonable provider qualification standards that it deems appropriate.
Although more than a decade old, this memorandum is the last official broad federal policy guidance issued concerning rehabilitative services coverage of mental health services. It remains in effect and continues to reflect fundamental CMS policy concerning the coverage of mental health services as rehabilitative services.
There are several facets of the coverage of rehabilitative services that warrant additional discussion. In particular:
- There is no federally prescribed array of mental health rehabilitative services that a state may offer. It is up to each state to fashion its own array. The specific mental health rehabilitative services that states cover vary considerably. Some states have confined their coverage to just a few services; others have crafted broader arrays. For example, in the past, Minnesota limited its coverage of mental health rehabilitative services solely to day treatment. Recently, the state expanded its coverage to include other elements of community support services that were previously funded exclusively with state dollars. Decisions concerning which services to cover, obviously, should reflect the states own policy goals and objectives with respect to supporting individuals with serious mental illness-es.
- Similarly, there are no federally prescribed definitions of the services that a state may offer as rehabilitative services. Each state may craft its own definitions to reflect its goals and objectives. While some services (e.g., psychosocial rehabilitation) are commonly covered by states under the rehabilitative services coverage, CMS has not prescribed the scope of these services or issued definitions for them. States are free to propose to cover new types of services, so long as the proposed service fits within the statutory parameters of rehabilitative services. CMS has avoided issuing prescriptive guidance that would have the effect of narrowing a states latitude to craft a coverage that comports with statutory provisions.
- Federal policy is also silent concerning the a-mount, duration and scope of mental health rehabilitative services. In other words, it does not dictate that such services be time limited or dictate that their use be capped or otherwise limited. A state may impose its own limits on the provision of such services, as long as these limits comply with the requirement that a service be sufficient in amount, duration and scope to reasonably achieve its purpose.
- Like other Medicaid services, the provision of rehabilitative services revolves around a medical necessity determination. States have latitude in establishing their own medical necessity criteria for rehabilitative services. Some states have relatively broad, general criteria. Others employ more sophisticated, sometimes two-tiered approaches to determine who may receive rehabilitative services. For example, Nevada requires that, in order to receive mental health rehabilitative services, individuals must meet level of care criteria based on the extent of their functional and other limitations. Once individuals meet level of care criteria, the authorization of specific rehabilitative services hinges on whether the person meets the service eligibility criteria associated with each service. Another way states define medical necessity is by using step down criteria. This applies when individuals who require intensive supports later step down to a less intensive service level when their condition improves.
- As with other Medicaid services, a state may employ prior authorization and other utilization management methods in order to ensure that mental health rehabilitative services are being employed appropriately. These managed care-like methods may be applied in fee-for-service delivery systems and it is increasingly common practice for states to contract with private entities to conduct such utilization management activities. For example, utilization management is a central feature in the operation of Georgias mental health rehabilitative services. It also is employed in other states, for example, Montana and Nebraska.
Fundamentally, the rehabilitative services coverage option gives states considerable flexibility in aligning Medicaid-funded mental health services with system goals in supporting working age adults with serious mental illnesses. Among the states, there is considerable variety in the services offered under this coverage option; this variety is evidence of the flexibility of the coverage. There are no major federal policy obstacles to states employing the rehabilitative services coverage as a vehicle for promoting recovery or underwriting evidence-based practices.
This coverage option -- like any other -- has its limitations. It does not include services that are not rehabilitative in nature. But, it may be used to combine services that have similar elements or goals (e.g., individual and group therapies, peer supports, medication management). Like any other Medicaid coverage, payment for services is subject to generic Medicaid requirements, including documentation and fee-for-service billing.
The following two pages illustrate how Georgia and Minnesota have crafted their rehabilitative services coverage.
Case Management/Service Coordination
Federal Medicaid law permits a state to obtain federal financial participation in the cost of two distinct types of case management services. One type is targeted case management which is used to assist beneficiaries to access both Medicaid and non-Medicaid services, as well as to coordinate and monitor service provision. Targeted case management is a separately coverable service under a states Medicaid plan.
The other type can be termed services case management, since it involves the internal coordination of the delivery of Medicaid health care services to meet an individuals needs. Care management activities may also be conducted during the course of furnishing a covered service. For example, ACT features close coordination of a skilled, multi-disciplinary team in support of an individual. Such coordination is reimbursable as part of the provision of ACT. Similarly, the coordination by a mental health professional of mental health rehabilitative services is reimburs-able as a rehabilitative service since it is integral to the provision of such services.
Targeted case management is distinguished from services case management mainly in its scope and focus (assisting individuals to obtain and access a wide variety of services). CMS guidance concerning Medicaid case management services is spelled out in the State Medicaid Manual (included in Appendix A). The Manual describes the scope and purpose of targeted case management and also the circumstances when case management may be furnished as a component service under another coverage category. The Manual also discusses claiming case management costs as an administrative expense. In mental health, this is not a common practice.
| Georgias Coverage of Mental Health Rehabilitative Services | |
Until 2001, Georgia relied on a very limited rehabilitative services option to obtain federal Medicaid funding for community mental health services. In order to bolster funding for such services as well as adopt a recovery framework across its community mental health service system, Georgia enhanced its coverage. Georgia's rehabilitative services coverage is comprehensive. It spans mental health services for persons of all ages and includes substance abuse services (which may be furnished to individuals who have a mental illness as well as those who do not). The coverage allows for the provision of services to individuals who have serious mental illnesses (or, in the case of children, a severe emotional disturbance) as well as individuals who need less intensive mental health services. A copy of Georgia's plan - including its service definitions may be found in Appendix B. The following services may be furnished to adults with mental illnesses.21
|
| Minnesota's Coverage of Mental Health Rehabilitative Services23 | |
Until recently, Minnesota confined its community mental health rehabilitative services coverage to day treatment for adults. Like some other states, Minnesota funded community support services for individuals with serious and persistent mental illnesses principally through state-funded grants to its network of county mental health organizations. In 2001, the Minnesota legislature authorized the expansion of Medicaid services to cover a broader array of rehabilitative services in order to increase the resources available to support people in the community. This was the first step in a multi-year strategy to expand and enhance community services so that they would be more flexible and less site-based. It was estimated that approximately 15,000 Minnesotans would receive expanded services and an additional 5,000 individuals would be able to receive services for the first time as a result of this change. Under the rehab option, somewhat broader eligibility criteria are employed than the state's definition of serious and persistent mental illnesses. Minnesota structured this expansion so that its added costs would be borne by state rather than county-funds. This freed up state grant funds to serve individuals not eligible for Medicaid who needed the same types of services, thus avoiding the emergence of a two-tiered system. Under its amended 2001 rehabilitative services coverage option (in addition to day treatment and the state's general purpose outpatient mental health services coverage), Minnesota added the following services for individuals age 18 and older who have a "substantial disability and functional impairment" in three or more areas:24
|
Targeted Case Management
Until 1986, the only practical avenue available for a state to secure Medicaid funding for freestanding case management services was through the HCBS waiver program. In 1986, Congress -- by enacting §1915(g) of the Social Security Act -- gave states the option to cover what were termed targeted case management services under their Medicaid plans.25
| Targeted Case Management | |
| Social Security Act: §1915(g): (1) A State may provide, as medical assistance, case management services under the plan without regard to the requirements of section 1902(a)(1) [statewideness] and section 1902(a)(10)(B) [comp-arability]. The provision of case management ser-vices under this subsection shall not restrict the choice of the individual to receive medical assistance in violation of section 1902(a)(23) . The State may limit the case managers available with respect to case management services for eligible individuals with developmental disabilities or with chronic mental illness in order to ensure that the case managers for such individuals are capable of ensuring that such individuals receive needed services. (2) For purposes of this subsection, the term "case management services" means services which will assist individuals eligible under the plan in gaining access to needed medical, social, educational, and other services. |
The expressed statutory purpose of targeted case management is to assist Medicaid recipients in gaining access to needed medical, social, educational and other services. This option is unique among Medicaid state plan coverages because it is not subject to the comparability requirement that services must be available to all beneficiaries. A state may limit its coverage of targeted case management services to a specified group of Medicaid recipients (hence the term targeted). These groups may be defined by condition or diagnosis (e.g., individuals with developmental disabilities) or their situation (e.g., persons who are homeless). A state may also offer these services on a less-than-statewide basis. Targeted case management is the sole Medicaid service that is exempt from the statutory comparability and statewideness requirements without a states having to obtain a federal waiver.
States are free to define the groups of Medicaid beneficiaries to whom they will provide targeted case management services and there is no limit on the number of groups that may be served under distinct coverages of targeted case management. For example, a state may have a distinct coverage for Medicaid beneficiaries with mental illnesses, and another for individuals with AIDS or HIV-related disorders. It is not uncommon for states to have multiple targeted case management coverages. A state may define a target population broadly (e.g., all Medicaid-eligible individuals with a mental illness) or more narrowly (e.g., Medicaid-eligible individuals with serious and persistent mental illnesses). As with other state plan services, once a state establishes its target population, case management services must be furnished to all beneficiaries who require them. A state may not limit the number of eligible individuals who may receive these services.
States have the option of limiting the entities that may furnish targeted case management services to individuals with developmental disabilities or mental illnesses. This provision permits a state to link these services to its single point of entry system, so that states can maintain a unified approach to service delivery. For example, Minnesota limits the providers of targeted case management services to its county human services agencies; however, they are authorized to contract with other qualified providers.
The services a state offers under targeted case management can be described as planning, linking, and monitoring direct services and supports obtained from various sources (the Medicaid program itself, other public programs, and private sources) -- making their scope potentially very broad. As cited by CMS, services and supports that case managers may assist a person to obtain include food stamps, energy assistance, emergency housing, and legal services. As noted above, this type of assistance may not be furnished under the rehabilitative services option.
Permissible targeted case management activities also may include facilitating service/support planning (including assessment), and monitoring the delivery of direct services and supports to ensure they meet the persons needs. In the mental health arena, targeted case management activities frequently include:
- Arranging for necessary assessments;
- Facilitating and participating in the development of individual treatment plans;
- Assisting individuals to obtain the mental health services in their plan and other public services (income assistance, housing, employment) that will further the achievement of personal goals;
- Monitoring the provision of services and individuals well-being, including identifying and resolving emerging problems;
- Serving as a point of contact in crisis and emergency situations and arranging the re-sponse to such situations; and,
- Advocating on behalf of individuals.
South Dakotas coverage of targeted case management services on behalf persons with serious mental illnesses spans many of these activities.
Targeted case management activities may be conducted face-to-face with the individual (e.g., visiting the person to conduct an interview), over the telephone with the person, and/or on a collateral contact basis (e.g., arranging for an appointment for the person with a local housing program or contacting providers who serve the person to obtain current information about her/his progress). Case manager activities must be specific to the individual beneficiary in order to qualify for Medicaid payment. As with other Medicaid services, individuals have the choice of accepting or rejecting targeted case management services.
| Example: South Dakota | |
South Dakota furnishes targeted case management (TCM) services to adults age 18 and older who are severely and persistently mentally ill (as defined by the state.) The services that may be furnished to individuals in this target population include:
|
Although a wide range of activities on behalf of beneficiaries may be included within the scope of targeted case management (at state discretion), some cannot. In particular:
- Activities related to the authorization and approval of Medicaid services. Targeted case management may not be employed as part of a prior authorization/utilization management system, or to direct beneficiaries to specific service providers. The statute expressly prohibits targeted case management activities that would have the effect of abridging a beneficiarys free choice of Medicaid provider. Prior authorization functions are eligible for federal payment as administrative expenses; if a states aim is to direct beneficiaries to a designated network of providers, then it must seek a 1915(b) freedom of choice waiver.
- Activities related to making basic Medicaid eligibility determinations. Such activities are eligible for federal payment as administrative expenses.
- Activities that constitute direct services to the consumer. For example, the activity of transporting an individual to and from a doctors appointment is outside the scope of targeted case management. The persons case manager may certainly transport the individual to a physicians appointment. Although the costs involved cannot be claimed as case management (because the service is direct), they may be reimbursed as a transportation service under the Medicaid state plan or as an administrative expense. There is not a bright line drawn in federal policy between targeted case management and direct services. Planning, linking and monitoring, however, describe the essential features of targeted case management. States may not claim federal funds for targeted case management activities that clearly fall under other coverage categories (e.g., driving a Medicaid beneficiary to a doctors appointment, which can be covered under transportation or personal assistance).
- Activities that overlap or duplicate similar services that a person receives through other means. For example, home health agencies are required to develop care plans for the individuals they serve. Targeted case management services cannot include development of these care plans. But they may include activities to ensure that the care plans are carried out and meet the consumers needs.
Targeted case management services may not be provided to individuals who reside in Medicaid-funded institutional settings (e.g., a nursing facility or an ICF/MR) except that they are reimbursable when furnished -- for up to 180 days in advance of discharge -- in order to facilitate a persons return to the community. This restriction on targeted case management services arises because: (a) federal regulations concerning Medicaid institutional services require that facilities themselves provide care coordination services to residents, and (b) Medicaid prohibits duplicate payments for the same service. The exception to this policy was specifically spelled out by CMS in 2000 as part of its initiatives to facilitate the community placement of institutionalized persons.26
Targeted case management services are not eligible for federal financial participation when furnished to individuals served in an IMD (because no services furnished to such persons may be claimed while the person is in an IMD). However, as in the case of other institutional settings such as hospitals, such services are eligible for federal financial participation when furnished up to 180 days prior to the discharge of a Medicaid beneficiary from an IMD. In this scenario, federal financial participation may only be claimed once the discharge has taken place. Targeted case management services may be furnished to Medicaid beneficiaries who are homeless or reside in homeless shelters. They may also be furnished to residents of community residential living arrangements that are not IMDs.
Because successfully supporting working age adults with serious mental illnesses in the community often involves not only addressing their treatment needs but also assisting them in other areas (e.g., finding affordable housing or securing employment), the coverage of targeted case management services is a means to support linkages to other services, as well as to monitor the well-being of individuals and assist them to address problems that they might encounter in community living.
Services Case Management
Services case management is an integral part of other services in a states rehabilitative services coverage, albeit not as a separate, distinct coverage. It is typically delivered in conjunction with service/treatment planning, periodic review of treatment plans, coordination and referral, monitoring, and/or advocacy. Again, it is important to keep in mind that, while these types of case management activities are eligible for federal financial participation since they are integral to the delivery of many services, their scope is limited to the management and coordination of activities and benefits covered as rehabilitative services. When the aim is to obtain or coordinate with other community resources, including non-Medicaid services, federal financial participation is only available under the targeted case management option.
Prescribed Drugs
Medications frequently play an important role in addressing mental illnesses. When individuals have appropriate medications, they are less likely to require other costly services. While prescribed drugs are an optional Medicaid benefit, they are covered by all states because they play such a critical role in contemporary health care, including mental health.27
| Medicare Coverage of Prescribed Drugs | |
| In 2003, Congress enacted the Medicare Prescription Drug, Improvement, and Modernization Act (P.L. 108-173). This legislation provides for Medicare coverage of prescribed drugs, starting January 1, 2006. The law also shifts the coverage of prescribed drugs for Medicare/Medicaid dual eligibles from Medicaid to Medicare, also effective in 2006. Once the law takes effect, states may no longer claim federal financial par-ticipation in the costs of furnishing prescribed drugs to dual eligibles. Dual eligibles must obtain their medica-tions through Medicare "Part D" plans.28 This change has substantial potential ramifications for dual eligibles. Within federal parameters, each Part D plan may establish its own coverage policies. It remains to be seen whether Part D plans will offer more or less extensive coverage of medications (in comparison to Medicaid coverages) that are critical for persons with serious mental illnesses. |
While Medicaid coverage of prescribed drugs is optional, there are important statutory requirements that states must observe in choosing to provide this benefit. Congress enacted provisions in 1990 specifically intended to ensure access to necessary medications by Medicaid beneficiaries, including a requirement that states include in their formularies all prescribed drugs produced by manufacturers that sign rebate agreements. Congress also allowed states to exercise some control over prescribed drug formularies through implementation of prior approval/prior authorizations processes and generic substitutions. How-ever, states may not keep a completely closed formulary. Medicaid beneficiaries must be permitted to obtain necessary medications.
In 1998, the Centers for Medicare and Medicaid Services sent a letter to state Medicaid Directors urging states to update their formularies to include the new atypical antipsychotics because they have fewer side effects, thereby increasing treatment compliance. Mental health advocacy organizations (e.g., NAMI and NMHA) have adopted policy positions urging states to maintain open access to these new medications.
There is clinical evidence that individuals with certain mental illnesses do not respond to some medications but will respond to others. As a consequence, an open formulary approach that permits trials using various medications is important for finding the right drug for a person. Additionally, the use of some types of medications must be accompanied by periodic testing. Medicaid payment for such testing is available through the mandatory laboratory and x-ray services benefit. Services such as medication education and medication management may be covered under either the rehabilitative services or clinic services options. Chapter 5 discusses effective practices that combine medication and other treatments.
In recent years, state Medicaid expenditures for all prescribed drugs have risen. State expenditures for medications related to the treatment of mental illness have also climbed rapidly during this period. In response to upwardly spiraling pre-scribed drug spending, states have resorted to a variety of cost containment and utilization manage-ment measures, including caps on the number of drugs that a beneficiary may receive, prior approval processes, fail-first policies,29 dosage and refill limits, the imposition of co-payments, the use of preferred drug lists and formularies, and mandatory substitution of generic for brand-name drugs when available.30 Because some of these strategies can be problematic, many states grant exceptions from them. For example, when states employ preferred drugs lists and formularies, non-listed medications remain available, although they may require prior authorization or approval. While states may establish prior authorization and other utilization management processes, their effect cannot be to deny medically necessary medications to beneficiaries. Additional strategies that states are employing (i.e., medication algorithms) are discussed in Chapter 5.
While a number of these strategies have been somewhat effective in containing prescribed drug costs, they can have the unintentional adverse effect of driving up health care costs through increased emergency room utilization. An October 2003 Bazelon Center survey of changes to state prescribed psychiatric drug policies indicates that many states are utilizing a variety of cost containment strategies whose impact is not yet fully known.31
Given the rapidly changing landscape of state prescribed drug policies, it is difficult to pin down the exact effects they have had on access to and the availability of critical medications for individuals with serious mental illnesses. In a few states, some classes of individuals have been exempted from prior authorization or other pharmaceutical restrictions. For example, Colorados generic substitution rule exempts medications used to treat mental illnesses with biological bases. New Mexico is implementing a preferred drug list that exempts atypical and typical antipsychotics for individuals with serious mental illnesses.
The Medicaid program provides access to critical medications for individuals with mental illnesses. In general, states may not refuse to reimburse for medications except for non-indicated uses or when an equally efficacious, but lower cost substitute is available. Many states have adopted the sound policy of providing unrestricted access to more efficacious second-generation antipsychotic medi-cations with favorable safety and side effect profiles, even though these medications can be substantially more costly than conventional antipsychotics.
Inpatient Hospital Services
A central goal of community mental health services is preventing institutionalization or hospitalization. The provision of effective rehabilitative and other services can help to avoid hospitalization. For example, ACT is designed specifically with this aim in mind. In many cases, states have structured their managed behavioral health plans to create financial incentives to reduce hospitalization. However, under some circumstances, individuals may need to be treated in a hospital setting.
Medicaid payment is not available for the services furnished to individuals age 22 to 64 in IMDs, but is available for inpatient hospital services furnished to individuals who are admitted to general hospitals as a result of a psychiatric condition, including the psychiatric units of such hospitals, as long as they are not classifiable as IMDs. The coverage of psychiatric inpatient hospitalization falls under the mandatory Medicaid inpatient hospital benefit rather than as a distinct coverage category. States have the option of covering inpatient psychiatric services for children and youth under age 22 as a distinct coverage category.32
As with other hospital services, states can manage the utilization of inpatient hospital services through prior approval processes, including requiring admission approval. In addition, it is common for states to limit length of stay and/or restrict how many times an individual may be admitted. A state may also require continued stay review. In general, states require that individuals be discharged once they have stabilized. In most instances, state policies concerning inpatient psychiatric hospitali-zation more or less parallel their policies for other types of hospitalization.
Personal Care/Assistance
Personal care services include the performance of daily tasks that individuals without disabilities can perform on their own but individuals with disabilities cannot as a result of functional impairments. Daily tasks include activities of daily living (ADLs) such as bathing, dressing, eating, toileting, and transferring from a bed to a chair, and instrumental activities of daily living (IADLs) such as cooking, grocery shopping, and medication management. Personal assistance may also include supervision and oversight.
| Personal Care/Assistance | |
| Social Security Act: §1905(a)(24) Personal care services furnished to an individual who is not an inpatient or resident of a hospital, nursing facility, [ICF/MR], or [IMD] that are (A) authorized for the individual by a physician in accordance with a plan of treatment or (at the option of the State) otherwise authorized for the individual in accordance with a service plan approved by the State, (B) provided by an individual who is qualified to provide such services and who is not a member of the individual's family, and (C) furnished in a home or other location |
Since the mid-1970s, states have had the option to offer personal care services under the Medicaid state plan, making these services one of the longest standing Medicaid home and community benefits. This option was first established administratively under the Secretarys authority to add coverages over and above those spelled out in §1905 of the Social Security Act, if such services would further the Acts purposes.33 In 1993, Congress formally added personal care to the list of services spelled out in the Medicaid statute.
When the option for states to offer personal care was created, it had a decidedly medical orientation. The services had to be prescribed by a physician, supervised by a registered nurse, and delivered in accordance with a care plan. Moreover, they could be provided only in the persons place of residence. Generally, the personal care services that a state offered included assisting individuals with ADLs. Other forms of assistance, such as laundry and housekeeping were offered on a limited basis, i.e., only when they were incidental to ADL assistance.
Starting in the late 1980s, some states sought to broaden the scope of personal care services, providing them outside the individuals home in order to enable beneficiaries to participate in community life. In 1993, Congress not only formally incorporated personal care services into federal Medicaid law but also authorized their provision outside the individuals home. Congress went a step further in 1994, allowing states to: (1) use means other than nurse supervision to oversee the provision of personal care services, and (2) establish means other than physician prescription for authorizing such services. In November 1997, CMS issued new regulations concerning optional Medicaid state plan personal care services to reflect these statutory changes.
Personal care/assistance services are most commonly provided to individuals with physical disabilities. Federal Medicaid policy concerning personal care/assistance services does not forbid their provision to persons with serious mental illnesses, but states do not usually provide them. Some individuals with serious mental illnesses have difficulty performing certain types of activities of daily living and may benefit from the provision of personal care/assistance. When such assistance is needed, it cannot be covered under the rehabilitative services option. Under that option, individuals may be taught -- if needed -- basic life skills so that they are able to be more independent. However, performing or assisting the individual to perform essential life tasks falls outside the boundary of rehabilitative services.
In January 1999, CMS released a State Medicaid Manual Transmittal (included in Appendix A) that significantly revised and updated the Agencys guidelines concerning the coverage of personal care services. This guidance made it clear that personal care services may span the provision of assistance not only with ADLs but also with instrumental activities of daily living (IADLs), such as personal hygiene, light housework, laundry, meal preparation, transportation, grocery shopping, using the telephone, medication management, and money management.
The guidance further clarified that, for persons with cognitive impairments (including persons with mental illnesses as well as persons who have Alzheimers disease or other dementias), personal care may include cueing along with supervision to ensure the individual performs the task properly. In other words, a person might be able to physically perform a task but has limitations in actually performing the task because of his/her mental condition. The guidance also explicitly recognized consumer direction of personal care services.
A little more than one-half of the states offer personal care/assistance under their Medicaid state plans. In recent years, states have tended to employ the Medicaid HCBS waiver program rather than Medicaid state plan coverage of personal assistance to expand the availability of personal assistance for individuals of all ages with various disabilities. Personal assistance is a common feature of HCBS waiver programs. Individuals with mental illnesses are not precluded from participating in HCBS waiver programs. However, they can only receive waiver services if they meet the states institutional eligibility criteria for hospital, nursing facility, or ICF/MR services.
Relatively few states furnish personal care/assist-ance routinely to support significant numbers of individuals with mental illnesses. Like other Medicaid services, a state may not discriminate on the basis of disability when it offers a service under the state plan. Consequently, a state may not deny personal care/assistance services to individuals who have mental illnesses but otherwise meet the states criteria for such services. At the same time, a state may not reserve personal care/assistance solely for such individuals. Personal care/assistance services cannot be targeted by specific type of disability.
Often, there are impediments to obtaining personal care/assistance for people with serious mental illnesses. Despite the changes in federal policy during the 1990s that permitted states to de-medicalize these services, some states have not changed their policies. Also, in many states, the threshold service eligibility criteria for personal care/assistance continue to focus on difficulties in performing activities of daily living, giving lesser weight to IADL needs. Additionally, some states continue to circumscribe the scope of personal care/assistance services by limiting it to the provision of services in the individuals living arrangement. Finally, securing personal care services on behalf of individuals with mental illnesses requires coordination between systems of care because personal care services are managed through different networks and programs than those that provide mental health services.
| West Virginia's Personal Assistance State Plan Amendment | |
In 2002, West Virginia amended its Medicaid state plan coverage of personal assistance to provide that such services could be (a) furnished outside the beneficiary's home and (b) used in support of individuals to obtain and retain competitive employment. In particular, West Virginia's coverage specifies that
|
In a few states, personal care funding has been used to partly underwrite the costs of community residences, including residences that support individuals with mental illnesses. Personal care funding was employed extensively by Michigan in the late 1980s as a means of financing community residential services for persons with mental illnesses and developmental disabilities. Michigans approach recognized that many of the supports that people receive in residential settings included personal care and that Medicaid funding could be employed to pay for a portion of the costs of operating such residences. In some states, personal care funding pays for some of the costs of operating domiciliary-type residential settings where individuals with mental illnesses may reside. However, in many instances, these settings do not furnish mental health services and supports for such individuals.
Recently, a few states have started to use personal assistance services to support the employment of individuals with disabilities. This development has been spurred on by the passage of the federal Ticket to Work and Work Incentives Improvement Act, Medicaid buy-in eligibility options (as discussed in Chapter 3), and CMS Medicaid Infrastructure Grants, which include a requirement for states to assess and strengthen personal assistance services to support people with disabilities who work.
At least three states -- California, West Virginia34 and Utah -- have augmented their existing Medicaid state plan coverage of personal assistance services specifically to support people with disabilities who work, including individuals with serious mental illnesses.35 In each instance, the state plan amend-ments take advantage of the 1993 amendments that allow for the provision of personal assistance outside the persons home to include the provision of employment-related personal assistance.
In 2003, California amended its Medicaid state plan to give individuals the option of receiving personal care services in the workplace to the same extent they are provided in the home.36 Utah has recently added innovative employment-related personal care coverage, which is discussed in more detail in Chapter 5.
Personal care/assistance potentially offers an avenue for underwriting non-treatment supports for individuals with serious mental illnesses, including those that support employment. Not all states offer personal care and, in some that do, individuals may not qualify for services based on the states eligibility criteria, or there may be other barriers to obtaining these services.
Conclusion
The Medicaid program provides states with a means to obtain federal financial participation in the costs of supporting working-age adults with serious mental illnesses in the community. The principal option available to states for mental health services is the rehabilitative services option. This option is flexible and can span a wide range of services in the community, at a states discretion. It is the option that aligns best with recovery as the central philosophy in supporting individuals with mental illnesses. Targeted case management can be an important adjunct to rehabilitative services. While the personal assistance coverage also might make important contributions in supporting individuals in the community, employing such services hinges on whether a state has included personal assistance in its state plan and the parameters of its coverage.
Annotated Bibliography
OBrien, J., Lanahan, P., and Jackson, E. (2003). Recovery in the Community: Volume II: Program and Reimbursement Strategies for Mental Health Rehabilitative Approaches Under Medicaid. Washington, DC: Bazelon Center for Mental Health Law. Available for purchase from the Bazelon Center: bazelon.org
This joint Technical Assistance Collaborative and Baz-elon Center report contains a wealth of very useful information concerning provider qualifications for rehabilitative services.
Rosenbaum, S., Teitelbaum, J., & Mauery, D.R. (2002). An Analysis of the Medicaid IMD Exclusion. Washington, DC: Center for Health Services Research and Policy, Department of Health Policy, George Washington University School of Public Health and Health Services. (18 pages).
This report discusses the IMD exclusion in considerable detail.
Kaiser Commission on Medicaid and the Uninsured (2004). Implications of the New Medicare Law for Dual Eligibles: 10 Key Questions and Answers. (Author) Washington, DC. Available at kff.org/medicaid/4160.cfm
This issue brief provides a more detailed explanation of the new Medicare drug coverage policy and its implications for dual eligibles.
Endnotes
-
See OBrien, J., Lanahan, P., and Jackson, E. (2003). Recovery in the Community: Volume II: Program and Reimbursement Strategies for Mental Health Rehabilitative Approaches Under Medicaid. Washington, DC: Bazelon Center for Mental Health Law. Available for purchase from the Bazelon Center: bazelon.org.
-
Partial hospitalization is a structured program of active treatment. The program may be furnished in hospital out-patient settings or by community mental health centers. A physician or therapist must certify that partial hospitalization is necessary in order to avoid more costly inpatient hospitalization.
-
Federal policies and guidance concerning the IMD exclusion is contained in the State Medicaid Manual, Part 4 (Services), Sections 4390-4390.1.
-
The exclusion is located ni §1905(a) (paragraph B) of the Social Security Act. The authority for a state to furnish services to residents age 65 and older in an IMD is in §1905(a)(14) of the Act.
-
§1905(i) of the Act; 42 CFR 435.1009
-
Prior to the enactment of Medicaid, the Social Security Act had excluded payments for services furnished to state mental health facility residents.
-
At the time Medicaid was enacted, state mental health facility outlays exceeded the estimated initial costs of the Medicaid program.
-
P.L. 92-603; §1905(a)(16) of the Social Security Act.
-
P.L. 100-360, §1905(i) of the Social Security Act.
-
State Medicaid Manual, op. cit.
-
Burwell, B., Sredl, K., & Eikan, J. (2003). Medicaid long-term care expenditures in FY 2002. Cambridge, MA: The MEDSTAT Group, Inc.
-
Five states now operate HCBS waiver programs for children with serious emotional disturbances.
-
This table was developed by Steve Day at the Technical Assistance Collaborative.
-
CFR Outpatient services: 42 CFR 440.20(a). Clinic services : 42 CFR 440.130(d).
-
§1905(a)(2)(A) of the Social Security Act.
-
§1905(a)(9) of the Social Security Act.
-
Virginia Department of Medical Assistance Services (June 2000). Mental Health Clinic Manual.
-
Ibid. Beneficiary must meet all of the following criteria: (1) Requires treatment in order to sustain behavioral or emotional gains or to restore cognitive functional levels which have been impaired; (2) Exhibits deficits in peer relations, deficits in dealing with authority, hyperactivity, poor impulse control, clinical depression, or demonstrates other dysfunctional symptoms having an adverse impact on attention and concentration, the ability to learn, or the ability to participate in employment, educational, or social activities; (3) Is at risk for developing or requires treatment for maladaptive coping strategies; and (4) Presents a reduction in individual adaptive and coping mechanism or demonstrates extreme increase in personal distress.
-
Peer support is a component rehabilitative service that is just beginning to be included in state plans. While it is a recommended part of comprehensive coverage, states must be sure they work closely with CMS in obtaining coverage approval. See the description of Georgias approved coverage of peer support in Chapter 5.
-
OBrien et al. (2003), op. cit.
-
Several of these services are also available to children with SED (severe emotional disturbance).
-
Available at www2.state.ga.us/departments/dhr/mhmrsa/pdf/Provider-ManFY04.pdf
-
Based in part on personal communication from Sharon Autio, Minnesota Department of Human Services. Information about mental health services in Minnesota is at dhs.state.mn.us/Contcare/mentalhealth/default.htm Information concerning the rehab option is at dhs.state.mn.us/main/groups/disabilities/documents/pub/dhs_id_004956.hcsp
-
Minnesota does not have a close-ended list of areas, but provides examples such as "interpersonal communication skills, community resource utilization and integration skills, crisis assistance, relapse prevention skills, health care directives, budgeting and shopping skills, healthy lifestyle skills and practices, cooking and nutrition skills, transportation skills, medication education and monitoring, mental illness symptom management skills, household management skills, employment-related skills, and transition to community living services."
-
P.L. 99-272
-
CMS Letter to State Medicaid Directors: July 25, 2000. Olmstead Update #3. Available at cms.hhs.gov/states/letters/smd725a0.asp
-
42 CFR 440.120(a).
-
For a discussion of the potential implications of this change, Please see: Jeffrey S. Crowley (2004). The New Medicare Prescription Drug Law: Issues for Dual Eligibles with Disabilities and Serious Conditions. Washington DC: Kaiser Commission on Medicaid and the Uninsured. Available at kff.org/medicaid/7119.cfm.
-
Fail-first policies require that certain medications only be available if alternative, lower cost medications are found ineffective.
-
For information on the measures that states have taken to slow down prescribed drug spending, see: Crowley, J, Ashner, D., and Elam, L. (2003) Medicaid Outpatient Prescription Drug Benefits: Findings from a National Survey, 2003. Kaiser Commission on Medicaid and the Uninsured: Washington DC.
-
Bazelon Center for Mental Health Law (October 2003). Medicaid Policies on Outpatient Prescription Psychiatric Drugs: A Survey.
-
42 CFR 440.10.
-
42 CFR 440.167.
-
The description of West Virginias plan amendment is based on the National Association of State Medicaid Directors Center for Workers with Disabilities Project Directors Alert (April 2002). WV Wins PAS State Plan Approval.
-
A state may not cover personal assistance in its Medicaid program for the sole purpose of supporting the employment of individuals. Hence, this type of change is limited to states that already offer personal assistance.
-
In particular, California provides that Services in support of work are only available to the extent that service hours used at work are included in the total personal care service hours authorized for the recipient based on the recipients need for services in the home. Authorized personal care services utilized by a recipient for work shall be services that are relevant and necessary in supporting and maintaining employment and shall not supplant any reasonable accommodations required under the Americans with Disabilities Act or other legal entitlements or third-party obligations.
CHAPTER 5: MEDICAID COVERAGE OPTIONS AND COMMUNITY SERVICES
| Finding the fit between Medicaid coverage options and effective community services for working-age adults with serious mental illnesses involves aligning a state's goals and objectives for community support with Medicaid coverage requirements. This chapter describes how several states have used Medicaid to underwrite components of community support services for adults with serious mental illnesses, focusing on the rehabilitative services option. |
So far, the Handbook has described the essential features of community support, and the general federal policy parameters that affect how states can use Medicaid to support working-age adults with serious mental illnesses. This has included a description of evidence-based practices and the components of the community support system, along with an in-depth discussion of Medicaid eligibility and coverage options. This chapter illustrates how states have crafted coverages to secure Medicaid funding for important components of community support. As noted in Chapter 4, states have considerable latitude in shaping mental health services under the rehabilitative services and other Medicaid coverage options. Examining actual state coverages provides useful information about practical and realistic applications of Medicaid to underwrite the costs of community mental health services.
Finding the Fit
Finding the fit between the mental health services that a state wishes to offer and Medicaid coverage requirements can be challenging. Mental health practices and treatment approaches frequently (and appropriately) are described in terms that may not readily lend themselves to translation into Medicaid coverage. Important concepts such as recovery involve supports that are individualized, consumer-driven, and geared toward helping individuals live successfully in the community. Promoting a recovery-oriented system of services and supports through Medicaid involves selecting services that promote independence and focus on assisting individuals to take progressively greater control over their lives (e.g., skill building, illness management and peer services). Service planning approaches that focus on the individual and stress rehabilitation are also ways of promoting recovery.
Translating mental health practices, approaches, and concepts into covered Medicaid services requires states to fashion benefits in the context of the Medicaid coverage framework depicted on the next page. This framework requires a state to answer in concrete, practical operational terms several questions about the services it intends to offer. Mental health approaches and practices must be described in coverage terms in order to secure Medicaid funding.
As noted in Chapter 4, there is no pre-established, federally defined array of Medicaid community mental health benefits that a state must include in its coverage. Federal policy defines the terms under which federal payments flow to the states and a state must conform to those terms. But, it is up to each state to decide how to meld Medicaid funding into its mental health system, taking into account coverage requirements and limitations on what Medicaid will pay for. Fundamentally, a state's overarching goals and objectives for supporting its citizens with serious mental illnesses should serve as the basis for deciding which Medicaid services it will offer. In this context, Medicaid is properly regarded as a tool for advancing important state policy aims by enabling a state to leverage and amplify its own financial resources.
| Stressing Recovery in Service Planning | |
Maine stresses rehabilitation and recovery in its coverage of community support services for persons with severe and disabling mental illnesses. Maine's rules concerning the rehabilitation/service plan provide that1 "An individualized rehabilitation/service plan is developed for and with a person receiving community support services by a designated community supports provider.
An individualized rehabilitation/service plan
|
"Finding the fit" starts with a state's identifying the service capabilities it wants to establish, and sorting out which services can be underwritten in whole or in part by Medicaid. At the same time, a state must recognize that there may be service capacities or components that have to be underwritten with other non-Medicaid funds, or secured through other public programs. It is also important to recognize that coverage design is multi-dimensional and necessitates decisions about provider qualifications, services eligibility criteria, medical necessity criteria, and other dimensions. Coverage should be approached holistically, identifying how each component will work in tandem with others. For example, securing coverage of Assertive Community Treatment (ACT) under the rehabilitative services option has proven to be relatively straightforward for states. However, ACT is but one component of an overall system of supports, many of which are needed to effectively support individuals when they no longer require intensive ACT services.
Because Medicaid has distinctive requirements, an important consideration for states is to avoid the creation of a two-tiered service system where Medicaid-funded services differ markedly from the services that a state offers to non-Medicaid eligible individuals who are members of the same priority population. Medicaid eligibility limitations can result in a portion of the priority population of individuals with serious mental illnesses not qualifying for Medicaid even though they may have relatively low incomes. A more seamless system for serving individuals in the priority population is achieved when a state's Medicaid coverages are derived from and mesh with a state's design of its service system. To the extent possible, this result is advanced when Medicaid and state funding streams employ:
- Common service definitions, recognizing that some components of a service may not qualify for Medicaid funding;
- The same provider qualifications;
- Equivalent payment rates;
- A similar approach to utilization management;
- Common quality management and improvement practices; and,
- Shared data systems.
The latitude afforded states in designing Medicaid coverages and managing Medicaid services means that the use of Medicaid financing need not lead to a bifurcated approach to serving individuals with serious mental illness.
| Medicaid Coverage Framework | |
|
In deciding whether to cover services through Medicaid, many factors need to be weighed beyond the technical feasibility of securing Medicaid. One factor, for example, can be the "readiness" of service providers to furnish a service, especially for an entirely new service, or imposing a higher standard of care on an existing service. In some respects, securing Medicaid funding for evidence-based practices is less a problem of the technical feasibility of covering them (since most fall well within Medicaid coverage boundaries) than a question of the capabilities of providers to meet the high standards that such practices envision. In addition, the initiation of a new service may need to be accompanied by technical assistance and training. Obviously, another practical but, nonetheless, critical factor is whether the state has the necessary matching dollars to underwrite the costs of adding a new service.
In addition, there is no doubt that the management of Medicaid services is demanding in its own right, especially when a state plans to employ prior authorization and active utilization review/management to ensure the appropriateness and effectiveness of services. Hence, managerial readiness also is a factor that may need to be weighed in deciding when to cover a service under Medicaid.
Coverage of Community Support Components
This chapter illustrates how states have employed Medicaid to cover several important components of community support. These examples are not presented as "ideal" or "model" coverages. Instead, they are intended to show the feasible range of services that can be covered through Medicaid, especially under the rehabilitative services option. The types of service capabilities/ capacities that are illustrated include:
- Crisis services
- Assertive Community Treatment (ACT)
- Illness/disability management
- Peer support/peer services
- Supports for community living
- Employment
- Family education
- Medication management
- Services for individuals with co-occurring conditions
States routinely employ Medicaid to cover many other types of community mental health services, including individual and group psychiatric therapy, and counseling. These essential core treatment services are included in nearly every state's Medicaid program. Service coordination/case management also plays a vital role in the provision of community mental health services. As discussed in Chapter 4, states most commonly cover case management by employing the targeted case management coverage option.
In this chapter, the focus is on coverages that can promote successful community living for working age adults with serious mental illnesses. These coverages prevent or reduce hospitalization and contribute to recovery. Additional information about these and other types of services that states offer may be found in Recovery in the Community, a Bazelon Center for Mental Health publication that includes extensive information on the full range of services that states principally cover under the rehabilitative services option.2
Crisis Services
| Crisis services are designed to meet the immediate needs of individuals experiencing a mental health emergency. They are flexible, mobile, and available 24 hours a day, 7 days a week. The need for crisis services may arise from a change in a person's living situation, emotional state, medication side effects, or a host of other reasons. Crisis services can range from telephone support to dispatching an on-site emergency team and following up with stabilization services. |
Crisis intervention is a critical component of the Community Support System and is covered under Medicaid in some form by every state. Effective crisis intervention is vital to the well-being of individuals with serious mental illnesses, who, in its absence, potentially face dislocation, institutionalization, and even more tragic outcomes. Effective crisis intervention reduces strains on a state's other health care resources, and can prevent unnecessary confinement. There is ample evidence demonstrating that the availability of crisis services reduces costly emergency hospitalization,3 making this coverage an especially wise, cost-effective investment for states. Crisis services may be provided under either the clinic or rehabilitative services options, but, as emphasized in Chapter 4, covering them as a rehabilitative service offers greater flexibility in responding to individual needs. Given the nature of mental health crises, crisis services should be available at any time and any place, and this capability is severely constricted under the clinic option, especially with respect to follow-up crisis stabilization services.
Thirty states cover crisis management/intervention as a distinct service under the rehabilitative services option.4 In addition, crisis services are frequently included as a component of other services (e.g., Assertive Community Treatment, where the ACT team is expected to respond round-the-clock to emergencies experienced by individuals whom the team supports). Where a state offers distinct coverage of crisis intervention but also includes crisis intervention as a component of other services, only one coverage may be billed for each intervention.5 Many states also assign case managers the responsibility to arrange for crisis intervention services in their coverage of targeted case management services.
Typically, crisis services usually have three components: assessment/first response, stabilization/ follow-up, and crisis residential services. Assessment/first response is the rapid, initial response to an individual who is experiencing a crisis, both to assess the nature of the crisis and identify next steps to address the crisis. Crisis stabilization occurs after assessment and involves the development of an individual crisis treatment plan that includes short-term goals and identifies the immediate services needed to achieve those goals. These services may be offered either at a mental health clinic or furnished by a mobile treatment team. For example, under its rehabilitative services coverage, Georgia provides for both "clinic-based crisis management" and "out of clinic crisis management," depending on where the crisis can be addressed most appropriately and effectively. Finally, crisis residential services are furnished when the crisis is sufficiently acute to require round-the-clock support in order to stabilize the person. Crisis residential services are time-limited and may span a variety of interventions, depending on the needs of the individual. Crisis residential services may mean providing a bed in a small group home or a facility with significant nursing and other medical coverage.
States that elect to use the rehabilitative services option to cover crisis services can incorporate all these elements and have the freedom to deliver all components of the service through mobile teams and in a variety of settings throughout the community. Crisis teams may include a peer specialist. West Virginia (below) and Minnesota (next page) provide examples of state coverage of crisis services under the rehabilitative services option.
Assertive Community Treatment (ACT)
| Assertive Community Treatment (ACT) is a mobile program of services that supports individuals who have especially intensive needs. ACT services are delivered by an interdisciplinary team that supports a limited number of individuals in any setting conducive to the individual. ACT services include monitoring, medication management, service referral, crisis intervention, short-term counseling and other interventions. ACT is provided under the rehabilitative services option. |
Many states have used the rehabilitative services option to cover the provision of (P)ACT services (Program of Assertive Community Treatment). As described in Chapter 1, ACT is a mobile, holistic, interdisciplinary approach to supporting people in the community who require especially intensive services. ACT is an evidence-based practice that is an integral component of the Community Support System and has demonstrated cost-effectiveness.6 The goal of ACT is to increase community tenure and reduce the incidence of crisis and hospitalization, enabling the individual to achieve greater integration and stability. ACT programs go by different names in different states (e.g., Intensive Community Treatment) but all are characterized by mobile, 24 hour a day, 7 day a week coverage9 and feature comprehensive treatment planning/ response, continuity of staff, one-on-one services and small caseloads. ACT sometimes is described as a form of case management.10 However, ACT teams are responsible for providing a full range of coordinated services to individuals, including crisis intervention, medication management, skill building and illness management. As of 2003, 18 states furnished ACT under the rehabilitative services option. However, it is challenging to fully cover all ACT services through Medicaid, and, as a result, ACT programs usually are supplemented with state-only dollars. In general, Medicaid funds finance 40-90 percent of the costs of ACT services.11
| West Virginia's Coverage of Crisis Services7 | |
West Virginia covers both crisis intervention and stabilization. It also provides crisis support in small community residential settings to support individuals who require a structured setting. West Virginia's crisis coverage is as follows: Crisis Services are based on a continuum of care ranging from the less restrictive setting (e.g., crisis intervention in the home/community) to a more restrictive setting (treatment in a residential facility).
|
| Minnesota's Coverage of Crisis Services8 | |
Minnesota's coverage of crisis services addresses three phases: crisis assessment, intervention, and stabilization. A crisis treatment plan must be prepared as soon as practical. The first two phases are provided to all persons; stabilization is provided as required. In Minnesota, county mental health programs or providers contracted by counties furnish crisis response services. Crisis response team members must complete at least 30 hours of crisis response training every two years. The following is excerpted from the Minnesota Medicaid state plan: Crisis Assessment is an immediate face-to-face appraisal by a physician, mental health professional, or a mental health practitioner under the clinical supervision of a mental health professional, following a determination that suggests the recipient may be experiencing a mental health crisis. The crisis assessment evaluates any immediate needs for which emergency services are necessary and, as time permits, the recipient's life situation, sources of stress, mental health problems and symptoms, strengths, cultural considerations, support network, vulnerabilities, and current functioning. Crisis Intervention is a face-to-face, short-term intensive service provided during a mental health crisis to help a recipient cope with immediate stressors, identify and utilize available resources and strengths, and begin to return to the recipient's baseline level of functioning. Crisis intervention must be available 24 hours a day, 7 days a week.
|
ACT is a high-end, intensive service that states reserve (via services eligibility and medical necessity criteria) for individuals with serious mental illnesses. It was originally developed specifically for individuals with schizophrenia or other psychotic disorders who exhibit a particularly high degree of functional impairment (e.g., inability to perform necessary tasks of daily living and/or incapacity to maintain a safe environment or avoid dangerous situations). ACT also is targeted to individuals who have a history of admissions to crisis residential, inpatient psychiatric, or other acute settings, and for whom less intensive mental health services have proven ineffective. ACT can also help to facilitate the transition of individuals from inpatient and other institutional settings to the community. Frequently, individuals who receive ACT have co-occurring disorders (mental illness and substance abuse) and thereby benefit from the integrated mental health/ substance abuse services.
ACT teams maintain frequent, consistent contact with the individuals they support, varying the frequency and duration of services based on the person's progress and needs.12 The composition of an ACT team includes a clinical/administrative team leader, a psychiatrist, registered nurses, a consumer/peer counselor, a qualified mental health professional (e.g., clinical social worker, licensed professional counselor), vocational specialist, and other qualified staff. This multi-disciplinary composition enables the team to address the full range of an individual's needs. ACT teams operate with a staff to consumer ratio in the range of 1:10 to 1:12. Extensive materials concerning (P)ACT are available from the National Alliance for the Mentally Ill.13
The mobile nature of ACT means that, if a state intends to offer ACT in its Medicaid program, the rehabilitative services coverage must be employed. Since ACT teams furnish the full-range of services required by each individual, other mental health services usually are not provided concurrently. Also, the provision of ACT is usually subject to prior authorization and reauthorization.
ACT has been covered under Medicaid by some states for several years. Examples of states with extensive ACT team provider networks include Wisconsin and Michigan. In 1999, HCFA (now CMS) issued a letter to state Medicaid directors (included in Appendix A) explicitly recommending that states seriously consider including ACT as a part of their community-based mental health services based on solid research concerning its efficacy. The letter urged that
"States should consider this recommendation in their plans for comprehensive approaches to community-based mental health services. Programs based on ACT principles can be supported under existing Medicaid policies, and a number of States currently include ACT services as a component of their mental health service package. Consumer participation in program design and the development of operational policies is especially key in the successful implementation of ACT programs."14
While several states now cover ACT in their Medicaid programs, many others have ACT teams that are not covered under the state's rehabilitative services option. In total, 28 states offer ACT in at least part of their state, regardless of funding source.15
Because ACT is interdisciplinary and teams furnish a wide range of services, payment for ACT services is sometimes misunderstood to require the billing of each specific service furnished by the team (e.g., separately billing for nursing services or skill build-ing). However, states are not required to un-bundle ACT services for billing purposes. Instead, ACT services may be billed by time unit (e.g., 15 minute units), provided that the services furnished by a team member are documented as falling under the scope of the state's ACT coverage.
Because ACT teams are operated by provider organizations, it is also not necessary that the billing be submitted by individual team members. The District of Columbia provides an example of a state that covers ACT. An in-depth profile of the operational features of Georgia's ACT coverage are provided in attachment A to this chapter.
| ACT Coverage Example: District of Columbia | |
The District specifically spells out the amount and scope of ACT services directly in its state plan, providing that "The consumer's ACT Team shall complete a comprehensive or supplemental assessment and develop a self care-oriented Individualized Service Specific Plan (ISSP) (if a current and effective one does not already exist). Services offered by the ACT team shall include:
|
Intensive Case Management
Some states cover a somewhat less exhaustive team-delivered service than ACT that is sometimes called "intensive case management" (ICM) (which should not be confused with targeted case management). ICM programs are structured similarly to ACT but are of a lower intensity, although there are similarities in the profiles of individuals served and the use of a team-based approach to service delivery. Making both ACT and ICM available can be a useful strategy for accommodating the diversity of the seriously mentally ill population as well as the changing needs of a given individual over time. Maine is an example of a state that offers both ICM and ACT under its rehabilitative services coverage. In Maine, ICM teams furnish "intensive interventions and supports to clients who otherwise might not be engaged in more traditional mental health services." ICM is also covered by some states that do not offer a standalone ACT program under Medicaid.
ICM (which can also go by other names such as mobile treatment teams) usually furnish services similar to ACT but often with higher consumer to staff ratios and more limited service availability (i.e., they may not be available around the clock). Services and supports are available wherever they are needed within the community. As is the case with ACT, ICM providers are expected to furnish a full range of services.
| Missouri's Coverage of Intensive Case Management | |
| Missouri's "Intensive Community Psychiatric Rehabilitation" provides an example of Intensive Case Management (ICM). There are many similarities between Missouri's ICM coverage and ACT; however, the ICM program is time-limited and does not have the same staffing ratio and requirements of ACT.17 Missouri's coverage is as follows: Intensive community psychiatric rehabilitation is a level of support designed to help recipients who are experiencing an acute psychiatric condition to be served in the community, thereby alleviating or eliminating the need to admit them into a psychiatric hospital or residential setting. It is a comprehensive, time limited, community-based service delivered to recipients who are exhibiting symptoms that interfere with individual or family life in a highly disabling manner. Intensive community psychiatric rehabilitation is intended for the following recipients:
|
Illness/Disability Management
| Illness management, an important evidence-based practice, involves educating the consumer to improve coping strategies, utilize medications more effectively, and reduce relapses and hospitalization. |
The ability to understand and self-manage one's own mental illness is central to recovery. Illness/ disability management is a recognized evidence-based practice. Individuals can be successfully educated about their own warning signs of relapse and can develop relapse prevention plans and strategies to guard against its occurrence.18 Illness management is sometimes referred to as disability or symptom management. The main thrust of illness management is to equip individuals with skills to help them manage all aspect of their illness and its impact on their lives. Its ultimate goal is to allow individuals to progressively take greater command of their own lives and recovery. The skills imparted include day-to-day coping skills, anticipating the need for services, evaluating treatment and clinical options, symptom management skills, and others needed to manage one's illness. Illness management can be covered under the rehabilitative services option.
Twenty-four states cover illness management under Medicaid for individuals with serious mental illnesses. New Hampshire provides an example of a state that offers illness management as a core community mental health service covering many dimensions of community support (e.g., skill development and psychotherapeutic interventions) and, hence, serves more ends than strictly illness management. However, the overall thrust of the coverage is illness management and recovery.
| New Hampshire's Coverage of Illness Management Services | |
New Hampshire stresses recovery-oriented illness management services. New Hampshire added Mental Illness Management Services (MIMS) to its Medicaid program in 1992. MIMS consists of a menu of services delivered in the community that are designed to enhance individuals' ability to manage their mental illness and live independently in the community. In 2002, over 900 adults received MIMS. The coverage spans several dimensions, including educating the person about coping mechanisms when symptoms emerge, developing skills to handle daily tasks and social/ professional/medical interactions, and assisting the person to develop stronger communication and conflict resolution skills. Individuals may receive one or several of these services depending on their needs and can receive them in either a clinic setting, the home, or work environment.19 New Hampshire's rules define MIMS as follows:20 MIMS shall be face-to-face interventions, and include the following elements and objectives:
|
Peer Support
| Peer support and peer-delivered services are central to the recovery movement and can cross a variety of service categories. Peer support services are delivered from consumer to consumer. Several states provide that individuals who have experienced a mental illness may qualify to furnish services such as community support and skills training. |
Because peer support is a hallmark of the recovery movement and an essential element of community support, more states are incorporating peer support and peer-delivered services into community mental health services. Peer support stresses that individuals -- with the assistance of peers -- should play an active and direct role in their own recovery, thereby promoting hope and empowerment and enhancing their own ability to live successfully in the community. Moreover, enlisting trained individuals who themselves have experienced serious mental illnesses to support their peers brings the consumer perspective to the front lines of recovery. Peers may furnish clubhouse-style peer counseling to support consumers in managing their illness, telephone support to ensure consumers are ready and on-time for work, on-site crisis management, and other relevant recovery supports. This support can greatly assist individuals by increasing their ability to self-manage their symptoms, advocate for themselves, and utilize effective coping skills to avert potential crisis situations.21`
Essentially, there are two avenues for covering peer support and peer-delivered services. Peer support may be covered as a distinct rehabilitative services benefit. States can also weave peer-delivered services into other covered rehabilitative services, such as living skills training or social support, by enabling individuals who have experienced a mental illness to qualify as practitioners. As previously noted (see Box p. 78), New Hampshire's MIMS coverage provides for qualified peers to furnish some services. In the case of ACT, program standards require that a peer be a member of the ACT team.
| "Studies show that consumer-run services and consumer-providers can broaden access to peer support, engage more individuals in traditional mental health services, and serve as a resource in the recovery of people with a psychiatric diagnosis. Because of their experiences, consumer-providers bring different attitudes, motivations, insights, and behavioral qualities to the treatment encounter."22 |
Currently, eleven states23 offer peer support services in some form, mostly by providing for peers to qualify as practitioners of rehabilitative services. Iowa provides an example of a state that enlists peers in the provision of services. At this point, only two states (Georgia and South Carolina24) have implemented a distinct Medicaid peer support coverage under the rehabilitative services option. Georgia's precedent setting coverage is described in Attachment B to this Chapter. Georgia also has incorporated peer-delivered services into many of its other rehabilitative services.
Supports for Community Living
| Many working-age adults with serious mental illnesses require skills restoration training to overcome the functional limitations that accompany their illness and live in the most integrated setting possible. This training is a vital component of recovery-oriented services and promotes independence. Services such as targeted case management also can play an important role in assisting individuals to secure stable housing. |
The fundamental purpose of Medicaid rehabilitative services coverage is the restoration of func tioning. Serious mental illness is accompanied by significant functional limitations in areas such as basic living and social skills. Furnishing rehabilitative services that address these limitations and equip individuals to function more independently is an essential ingredient in promoting successful community living for working age adults with serious mental illnesses. In order to qualify as a rehabilitative service, services furnished to improve living skills must have a restorative focus.
| Peer Support Counselors in Iowa25 | |
| Iowa has integrated peer-delivered services into the package of services it offers under the rehabilitative services option by providing that some services may be furnished by peer support counselors. A peer support counselor is defined as "a person who has been diagnosed with a chronic mental illness, who provides counseling and support services to other adults with the same or a similar diagnosed mental illness."26 A peer support counselor must meet five requirements: (1) Successfully complete training that is supervised by an LPHA (Licensed Professional of the Healing Arts - an MD or licensed psychologist); (2) Abide by professional ethics adopted by National Board of Certified Counselors that bind licensed mental health counselors; (3) Provide qualified services that are aligned with the rehabilitative portion of an individual's treatment plan, and that are supervised by an approved professional;(4) Demonstrate competency in service delivery as determined by meeting professional standards of a national organization overseeing that particular service area; and (5) Provide services through employment or by a contract with a Medicaid-approved provider.27 Peer support is not defined as a distinct service but is woven into other rehabilitative services, including (1) community living skills training; (2) employment-related services; and (3) day program services for skills training and development. |
A substantial majority of states cover the restoration of basic or daily living skills as a rehabilitative service. These services assist individuals to live more independently by enabling them to do more for themselves. Such services can include "training, guiding, supervising, cueing or reminding, or techniques to teach how to overcome barriers by changing how the person interacts with his/her environment."28 The span of basic or daily living skills addressed through these services can be quite wide-ranging, including IADLs such as food preparation, money management, grocery shopping, personal hygiene, medication self-administration and housekeeping. As discussed in Chapter 4, the actual performance of daily activities (e.g., meal preparation) for a person requires alternate coverage under the personal care/ assistance category. Iowa (below) and Minnesota (following page) provide examples of the coverage of basic living skills.
In a similar vein, the restoration of social and interpersonal skills focuses on developing interpersonal relationships, solving problems and resolving conflicts. Most states cover the restoration of these skills as a rehabilitative service.
Keeping in mind the broad goal of achieving maximum community integration, functioning, and recovery, sixteen states offer elements of social and recreational supports under the rehabilitative services option. States may provide certain services that facilitate the development of social networks, increase environmental adaptability, and ultimately strengthen an individual's ability to live independently. These services are aimed at employing recreational activities that focus on reducing isolation and withdrawal and that support goals identified in an individual's treatment plan. For example, Missouri's psychosocial rehabilitation coverage includes "participation in informal and organized group activities to help reduce stress and improve coping, which are normative to the community, such as exercise, self-education, sports, hobbies, supportive social networks, etc."29 However, social/recreational activities not aimed at recovery-related or therapeutic objectives may not be covered under Medicaid.
Some states have distinct coverages of services for the restoration of basic living skills, social, interpersonal and other skills; elsewhere, states combine these services with others.
Supporting Individuals in Community Living Arrangements
Promoting successful community living for working age adults with serious mental illnesses involves not only meeting their service needs but also aiding them to secure housing. Having a stable living arrangement is extremely important. There is a strong correlation between homelessness and mental illness -- 46 percent of U.S. adults who experience homelessness at least once in a given year have also had a mental health problem during that year.30 The importance of stable housing was underscored by the President's New Freedom Commission on Mental Health, which asserted that "The lack of decent, safe, affordable, and integrated housing is one of the most significant barriers to full participation in community life for people with serious mental illnesses."31
Medicaid and especially rehabilitative services can contribute significantly to successful community living by underwriting services and supports in a person's living arrangement. But, other resources must be tapped in order to secure housing for individuals who cannot afford it. Except in the case of Medicaid-funded institutional services (e.g., nursing facilities), Medicaid dollars cannot be used to pay for housing or other living expenses ("room and board") of Medicaid beneficiaries. This policy encompasses all types of Medicaid community services for people with disabilities. As in the case of some other services (e.g., employment) that contribute to recovery, successful community living strategies cannot rely solely on Medicaid funding. Tapping federal, state, local and private housing resources -- along with a person's own resources -- is critical to help individuals maintain stable housing. Medicaid funding can then be employed to bring services and supports into their living arrangements.
| Iowa's Coverage of Services for Restoration of Basic Living Skills | |
| Iowa offers a good example of a typical state's coverage, offering "services [that] are age-appropriate skills training or supportive interventions that focus on the improvement of communication skills, appropriate interpersonal behaviors, and other skills necessary for independent living or, when age-appropriate, for functioning effectively with family, peers, and teachers. Training for independent living may include, but is not limited to, skills related to personal hygiene, household tasks, transportation use, money management, the development of natural supports, access to needed services in the community (e.g., medical care, dental care, legal services), living accommodations, and social skills (e.g., communicating one's needs and making appropriate choices for the use of leisure time)."32 |
| Minnesota's Coverage of Services for `Living and Social Skills33 | |
Minnesota ties together training in living and social skills in its "Mental Health Basic Living and Social Skills" coverage: ARMHS [Adult Rehabilitative Mental Health Services] Basic Living and Social Skills are activities that restore a client's skills essential for managing his or her illness, treatment, and the requirements of everyday independent living. These skills need to be restored if recipients are to be able to leave inpatient or residential programs and live independently in the community. If these abilities are not developed clients may require inpatient or other intensive services. [Services are furnished to] Instruct, assist, and support a recipient in areas such as:
|
Community living is best exemplified through a supportive housing model, which assists individuals to live in community-integrated living arrangements. Supportive housing programs adhere to four basic tenets: permanence and affordability, safety and comfort, accessibility and stability, and empowerment and independence.35 Supportive housing for persons with serious mental illnesses includes several fundamental components -- assistance to tenants to help them understand and meet the requirements of tenancy, comprehensive assessment, coordination of psychiatric services, medication management, crisis services, connections to other community resources, and staff training.36 Several of these components (e.g., basic living/social skills training, assessment services/targeted case management, medication management, and crisis intervention) can be covered under Medicaid. It is estimated that Medicaid can underwrite anywhere from 25 to 80 percent of the services that fall under the "supportive housing" umbrella.37 The rehabilitative services option provides a means to fund many services that are integral to supportive housing. Assisting individuals to access housing support programs and/or locate affordable housing is Medicaid reimbursable through targeted case management. More information on the role that Medicaid can play in supportive housing is found at the Corporation for Supportive Housing web site.38
| Impact of Community Housing | |
| A 2003 survey by the Tennessee Department of Mental Health and Developmental Disabilities (TDMHDD) found that individuals with mental illnesses who were provided a community residential placement experienced a sharp reduction in their admissions to psychiatric hospitals. In the two years after relocating into homes, a sample of 105 individuals experienced a total of 10 hospital admissions, compared to 154 before placement. The state's Creating Homes Initiative, a targeted, grassroots, local community, multi-agency collaborative operated by the TDMHDD Office of Housing Planning and Development has spearheaded the department's efforts to develop and expand permanent housing options (including group homes, apartments, and home ownership) and services for people with mental illness and co-occurring disorders.34 |
The rehabilitative services option permits states to furnish therapeutic support services in the person's living arrangement. Such living arrangements can include the person's own home, his or her family's home if that is where the individual lives, and other living arrangements (e.g., supervised apartments, group homes, and other congregate arrangements) operated by mental health service providers. With respect to the latter, Medicaid services furnished at such sites are reimbursable as long as the living arrangement does not run afoul of the IMD exclusion (i.e., do not have more than 16 beds), and the services furnished have a rehabilitative purpose. The types of services and supports furnished at a person's living arrangement cover a wide array of typical rehabilitation services, including basic living skills training, medication management, illness management, and other therapeutic interventions.
State approaches to the provision of services and supports to people in their living arrangement vary. In some instances, states simply provide that rehabilitative services may be delivered in any community location, including a person's private residence. Some states explicitly cover rehabilitative services in licensed community residences as "residential services" or distinctly provide for their delivery in a variety of living arrangements. Often, the use of licensed community residences is reserved for individuals who require some level of continuous oversight and a more structured setting. Nebraska's residential services coverage provides an example of how a state can employ supervised community residences as a bridge to more independent living arrangements. Maine's coverage of "in-home support" (following page) illustrates another approach by furnishing services not only in licensed community settings but also a person's own home.
While Medicaid funding is not available to pay for housing and other everyday living expenses, the rehabilitative services option can be employed to bring critical services into a wide variety of community living arrangements. As pointed out by the President's Commission, the aim should be to create "flexible, mobile, and individualized support services to support and sustain consumers in their housing."39
Employment-Related Services
| Employment-related services that support entry into or maintenance of employment may be furnished under Medicaid. They can include onsite crisis supports, symptom management and others. Job searching services and job training and coaching are not eligible for Medicaid reimbursement. |
For individuals with serious mental illnesses, securing employment is an important step in their recovery and their living successfully in the community. Many adults with serious mental illnesses strongly desire to work, yet very few are in fact working. According to the President's New Freedom Commission, there is a 90 percent unemployment rate among this population.40 Anecdotal evidence of the importance of employment as a consumer service abounds. Each year, the Georgia Mental Health Consumer Network asks individuals about their top priorities, and the answer consistently is "wanting jobs better jobs."42
| Nebraska's Residential Services Coverage | |
The Psychiatric Residential Rehabilitation Program is designed to
|
| Maine's Coverage of In-Home Support | |
In Maine, community support rehabilitative services are furnished to individuals who have a "severe and disabling mental illness." In-home support is furnished to individuals who require some measure of personal supervision in addition to therapeutic supports services. The following description of in-home support is excerpted from the Maine Medical Assistance Manual: In-home support is personal supervision and therapeutic support services provided to an adult with major mental illness in his or her home or temporary living situation pursuant to an individual support plan (ISP). These services are provided in order to allow a person to maintain the highest level of independence possible. To the degree possible, persons using this service will participate in the hiring and training of the support worker. In-home support has two levels of service as indicated in A and B below.
|
Chapter 3 outlined the options available to states that permit individuals with disabilities to maintain Medicaid eligibility after they are successfully employed. State adoption of the Medicaid "buy-in" option is an important step in overcoming an important barrier to employment -- namely, the loss of Medicaid eligibility due to excess earnings. Many working-age adults with serious mental illnesses need supports in order to secure and maintain employment. Supported employment is a recognized evidence-based practice. Furnishing supports to individuals that lead to their employment can result in reductions in their utilization of mental health services and promotion of their self-esteem and recovery. In order to secure and maintain employment, individuals may need basic or daily skill development services along with other relevant skill training to function successfully in the work place (sometimes called social and interpersonal skills.) Illness management services can also help an individual to maintain employment. Additionally, peer supports can also be very helpful in aiding and encouraging individuals to work. Targeted case management services also can be useful in connecting individuals to employment services, including vocational rehabilitation.
Another dimension of employment is job-specific training. Federal Medicaid policy, however, prohibits the use of Medicaid funds to pay for "vocational" services (including sheltered workshops), except under limited circumstances.43 As a consequence, it is not possible to employ the rehabilitative services option to underwrite the costs of job-specific training (e.g., job coaches) in order to craft full-featured supported employment services. Consequently, when it is a state's aim to promote employment, it is necessary to complement the supports that fit under the rehabilitative services option by tapping other resources to secure job-specific training services for individuals. Those resources can include vocational rehabilitation services or funding, jobs programs, or other non-Medicaid state and local funds. Depending on the funding source, it can be especially important to coordinate mental health and vocational services.
Irrespective of funding source, at least 43 states provide some type of supported employment service to consumers with mental illness. In the context of the rehabilitative services option, however, about 30 states include employment-related services in their programs. Some states break these services out separately while others include them in other skills-related service coverages. Texas and Kansas provide examples of states that have specifically broken out employment-related services under the rehabilitative services option. Iowa's coverage qualifies supported employment providers to furnish these services in addition to mental health agencies.
Using Personal Care Services In the Work Place
As noted in Chapter 4, Utah (as well as other states) recently added the coverage of "employment-related personal care/assistance services. This coverage is available to support individuals with serious mental illnesses who are returning to work. Utah is working with a major mental health agency to employ personal care to support individuals in the Salt Lake City area, illustrating that supporting people with serious mental illness in their return to work need not necessarily be confined to the use of the rehabilitative services option. This effort is described on the following page.
Family Education
| Family psychosocial education and therapy services include educating the family about the nature of a person's mental illness and training family members how to support the person and to problem solve. |
Educating family members and significant others about the nature of an individual's mental illness and enlisting their active participation as members of the treatment team in support of the individual is an essential component of the Community Support System and a recognized evidence-based practice. According to SAMHSA, individuals whose families actively participate in a psychoeducation program show a significant decline in relapse rates and re-hospitalizations. In some cases, these rates can decrease by as much as 50 percent over the course of a year.44 As noted in Chapter 2, a substantial percentage of working-age adults with serious mental illnesses live with their families. Medicaid can play an important role in underwriting family-education. So long as these services focus on addressing the needs of the Medicaid beneficiary, they are eligible for Medicaid funding. For example, Ohio stipulates that these services must be "directed exclusively to the well-being and benefit of the person served and are assistive to maintaining independent living in the community."45 A wide range of family education activities meet this test.
Thirty-one states offer some type of family education services. In general, family support/ education includes educating the family about the nature of the individual's illness, resolving confusion about the family member's treatment plan and its goals, equipping the family with skills to help the person in managing his or her illness (e.g., symptom and medication management) and dealing with crises, and problem-solving. Family education services are only furnished when the individual agrees that the family member or significant other may participate.
| Texas' Coverage of Employment-Related Services | |
| Texas offers employment-related services that provide "age appropriate training and supports that are not job specific, and have as their focus the development of skills to reduce or overcome the symptoms of mental illness that interfere with the individual's ability to make vocational choices, attain, or retain employment. Included are activities such as skills training related to task focus, maintaining concentration, task completion, planning and managing activities to achieve outcomes, personal hygiene, grooming, communication, and skills training related to securing appropriate clothing, developing natural supports, and arranging transportation. Also included are supportive contacts in school, or on-or-off the work-site, to reduce or manage behaviors or symptoms related to the individual's mental illness that interfere with job performance, or progress toward the development of skills that would enable the individual to obtain or retain employment."46 |
| Kansas' Coverage of Employment-Related Services | |
| Kansas defines employment-related services as: "Assistance which shall have as its objective the development and implementation of a plan for assuring appropriate consumer community integration and the provision of both supportive counseling and problem-focused interventions in whatever setting is required to enable consumers to manage the symptoms of their illness. Services provided at the worksite must be focused on assisting the individual to manage the symptom of mental illness, and not to learn job tasks. These interventions will fall primarily in the areas of achieving the required level of concentration and task orientation, and facilitating the establishment and maintenance of effective communications with employers, supervisors and co-workers."47 |
| Utah's Coverage of Employment-Related Personal Assistance | |
| In 2003, Utah received CMS approval to furnish employment-related personal care services. Valley Mental Health - the behavioral health contractor for the Salt Lake City area - and the Utah Medicaid program are collaborating to employ this benefit to furnish people with mental illnesses a short-term personal care assistant to facilitate their return to work. Utilization data has shown that individuals with serious mental illnesses who do manage to secure employment often experience an immediate spike in their symptoms due to increased stress and anxiety, frequently leading to a rapid loss of employment, which thrusts them full-time back into high-intensity services. In an effort to combat this, the Utah Medicaid program is working through Valley to arrange for "frontloaded" personal assistance for individuals with serious mental illnesses to re-enter the job market. During the first 90 days of employment, consumers would receive intensive personal care services to help them ease into the new situation. As their stress level decreases and they become more accustomed to the job, personal care hours would taper off until the individual no longer requires them. The hope is that not only will the consumer be more likely to retain employment, but also that the use of crisis and other intensive services can be avoided.48 In addition to assistance with ADLs and IADLs, the Utah coverage provides for transportation to and from the workplace, case management support to access and coordinate services and supports available at the work site, and coordination of employment-related personal care with other Medicaid state plan services. These include home-based personal care and services "designed to assist an individual with a disability to perform daily activities on and off the job that the individual would typically perform if they did not have a disability." Employment-related personal care services are available through agencies or through individual personal assistants who are employed by the beneficiary. Utah requires that, for this arrangement, the beneficiary use the services of an approved intermediary to coordinate claims submittal and payments (including tax payments). |
Vermont offers "collateral contact" to family members or other significant individuals, which includes "meeting, counseling, training or consultation" services. The type of services needed are left up to the discretion of the family.49 Maine, in its rehabilitative services coverage, provides for "family education and consultation, if desired by a person receiving community support services and his or her family, in order to help family members develop support systems and help the person manage his or her mental illness."50
Family education is distinguishable from the "family therapy" psychiatric therapeutic treatment modality because it envisions an active role for the family in aiding the person's recovery.
Medication Management
| Medication management is a body of practice that stresses the selection of appropriate medications for individuals, along with continuing review and the provision of additional services that reinforce individuals' adherence their medication regimen. |
The emergence of evidence-based practices is beginning to influence state coverages of certain types of services. For example, states frequently cover medication management and education under Medicaid. As discussed in Chapter 4, medications can play an important role in the treatment of serious mental illnesses. The typical focus of medication management is to make sure that individuals follow their medication regimen and are educated about the importance of adhering to the regimen. Medication management as an evidence-based practice, however, envisions a more intensive course of treatment that is now beginning to be reflected in some state coverages. The District of Columbia (following page) provides an example of an especially comprehensive coverage of medication management services.
Medication "algorithms" have also emerged as an important medication management practice; at least 21 states utilize some type of algorithm in part or all of their state.51 A medication algorithm is a set of best-practice clinical procedures that physicians are encouraged to follow in treating consumers. Medication algorithms focus on specific types or classes of medications (i.e., newer atypical anti-psychotics) and also include other best practice procedures such as patient and family education. One state that has developed a noteworthy Medicaid medication algorithm program is Texas. The Texas Medication Algorithm Project (TMAP) began in 1996 and focuses on the implementation of public services, as well as to promote the cost-effective provision of services. Specifically, TMAP focuses on adults with schizophrenia, bipolar disorder, and major depressive disorder, and comprises four distinct parts:
| District of Columbia: Medication Management Coverage | |
| In the District of Columbia, medication treatment and management are combined. Medication/Somatic Treatment services encompass a full range of services related to the prescription and monitoring of the effects of medications as well as medication education. In particular: "Medication/Somatic Treatment services are medical interventions including physical examinations; prescription, supervision or administration of mental health-related medications; monitoring and interpreting results of laboratory diagnostic procedures related to mental health-related medications; and, medical interventions needed for effective mental health treatment provided as either an individual or group intervention. Medication/Somatic Treatment services include monitoring the side effects and interactions of medications and the adverse reactions a consumer may experience, and providing education and direction for symptom and medication self-management. Group Medication/Somatic Treatment shall be therapeutic, educational and interactive, with a strong emphasis on group member selection, facilitated therapeutic peer interaction and support.52" |
- Medication treatment algorithms derived from evidence-based, scientific practice;
- Supporting the provider with technical assistance and clinical guidance in algorithm implementation;
- Patient and family education; and
- Documentation of treatment provided and consumer outcomes.
TMAP stresses the importance of a global approach that enlists providers, physicians, consumers, and family members in maximizing treatment effectiveness and reducing inefficiencies in the service delivery system. According to state officials, adults who participated in TMAP fared better than those who did not in areas such as symptomatology, cognition, and need for hospitalization.
Missouri is currently implementing a program that is similar to TMAP but focuses specifically on a physician education approach to medication management. The Missouri Department of Mental Health and the Division of Medical Services (the state's Medicaid agency) have joined forces to pilot a privately-funded physician education/algorithm approach to Medicaid psychiatric drug management. The goals of the Collaborative Behavioral Health Project are to: (a) improve the quality and consistency of medication prescribing practice based on national best practice guidelines; (b) improve adherence to medication plans; and, (c) lower prescribed drug outlays.
Through the project, physicians are provided reports based on Medicaid claims data that profile and compare their practices to best practice guidelines and include: (a) psychiatric medications prescribed by a physician for each Medicaid beneficiary during a given month; (b) any other Medicaid psychiatric prescriptions filled by any beneficiaries on the provider's list (i.e., medications prescribed by another physician); and (c) indicators where the physician's prescriptions were not in accordance with clinical best practices (e.g., prescribing an outdated antipsychotic medication). This feedback is purely informative -- providers are not "punished" for their prescription habits. The aim is to give physicians a complete picture of their prescribing practices and prompt changes in accordance with best practices. Since these reports are generated monthly, the state can see whether or not changes are actually occurring.
This program began in January 2003 and each month, between one-third and one-half of providers are reported to be altering their prescription practices based on information they receive. In addition, physician feedback about the program has been overwhelmingly positive. While specific figures are unavailable, Missouri estimates that the program has provided a substantial cost-savings.53
Supporting Individuals with Co-Occurring Disorders
| Individuals with co-occurring disorders can pose a variety of service delivery challenges. This section provides information concerning services for individuals with co-occurring substance abuse disorders and co-occurring developmental disabilities. It describes efforts to effectively meet the needs of these individuals. |
A significant number of individuals with serious mental illnesses also have a co-occurring disorder.54 Substance abuse is a frequently co-occurring disorder among working-age adults with serious mental illnesses. There are also a significant number of individuals with developmental disabilities who have a co-occurring serious mental illness. Effectively supporting individuals with co-occurring disorders poses three principal challenges:
- Treatment/practice. One major challenge is identifying and applying integrated, effective treatment strategies that concurrently address both disorders. Parallel or sequential treatment of each disorder is frequently not effective in meeting individuals' needs.
- Service Delivery. State service delivery systems typically are organized to serve individuals who have a single "primary" disorder. Problems often arise in bringing to bear the necessary expertise and services to serve persons whose co-occurring disorders cross system lines.
- Finance. Disorder-specific "funding silos" can make it difficult to marshal the financial resources needed to serve persons with co-occurring disorders.
Surmounting these challenges often requires pursuing multiple strategies, including disseminating information about effective treatment strategies, cross-training provider staff, re-aligning service delivery system structures and policies, and promoting effective collaboration at the local level.
Federal Medicaid policies, of course, most directly bear on the question of financing services for individuals with co-occurring conditions. The following sections describe policies affecting services for persons with serious mental illnesses with co-occurring substance abuse disorders and developmental disabilities. Examples of how various states support these individuals using Medicaid dollars are provided.
Services for Individuals with Co-Occurring Substance Abuse Disorders
In 2001, an estimated 20 percent of adults with serious mental illnesses were dependent on or abused alcohol or illicit drugs.55 An estimated 3 million adults had both a serious mental illness and a substance abuse disorder.56 It also is estimated that more than one-half of all individuals with serious mental illnesses served through the public mental health system have co-occurring substance abuse disorders. There is a growing recognition that co-occurring substance abuse disorders are the "expectation, not an exception" among individuals with serious mental illnesses.57
Individuals with mental and substance abuse disorders pose major challenges for public systems. They experience high rates of homelessness, hospitalization, and criminal justice system involvement. The costs of serving these individuals are estimated to be about twice as great as persons with a single disorder. However, only about 19 percent of individuals with serious mental illnesses who have a co-occurring substance abuse disorder are treated for both disorders and many are not treated for either.58 When individuals with co-occurring disorders receive effective services, they experience substantially better outcomes, and the high costs associated with frequent hospitalization and incarceration are significantly reduced.
A consensus exists that integrated treatment, which combines mental health and substance abuse services within the same, multidisciplinary system of care, is the most effective approach to successfully serving persons with co-occurring substance abuse disorders. As noted in Chapter 1, "Integrated Dual Disorder Treatment" is a recognized body of evidence-based practice that leads to demonstrably higher rates of dual recovery and thereby reduced costs. In 2001, the majority of states were implementing this practice statewide or in some parts of their states.59
Several barriers have been identified to effectively serving individuals with co-occurring mental illnesses and substance abuse disorders. Two major barriers are:
- Mental health and substance abuse services usually are delivered through distinct service delivery systems at the state and local levels. This can result in fragmented services and clouded lines of responsibility for serving persons with co-occurring disorders, sometimes causing individuals to bounce between systems or be denied services by one system due to the presence of the other disorder. Accompanying funding and regulatory silos frequently make it difficult to coordinate and integrate the delivery and financing of needed services.
- The lack of clinicians and other mental health professionals who are cross-educated and trained and have expertise in serving individuals with co-occurring disorders.
Several states have taken steps to address these problems. In about one-half of the states, a single state agency (often termed a "behavioral health" authority) administers both mental health and substance abuse services; many states have carried consolidation of service delivery down to the regional or local level.60 For example, New Mexico created a behavioral health authority in 1997 and, since, has taken several additional steps aimed specifically at improving services for individuals with co-occurring disorders, including integrating such services at the regional level.61
Elsewhere, state mental health and substance abuse authorities are collaborating to strengthen services for individuals with co-occurring disorders, including implementing "no wrong door" policies. In 2003, for example, the Texas Department of Mental Health and Mental Retardation (TDMHMR) and the Texas Commission on Alcoholism and Drug Abuse concurrently issued rules specifically to ensure that individuals with co-occurring psychiatric and substance abuse disorders are not denied services in their respective systems because of a co-occurring disorder. The TDMHMR rules include standards to "ensure the effective and coordinated provision of services to individuals who require specialized support or treatment due to co-occurring psychiatric and substance abuse disorders." These standards apply to community mental health services underwritten with Medicaid and other funds. They spell out both knowledge and technical competencies that provider staff must possess, as well as standards of care.62
In a similar vein, the Missouri Department of Mental Health's Divisions of Comprehensive Psychiatric Services and Alcohol and Drug Abuse jointly developed and implemented "Core Rules for Psychiatric and Substance Abuse Programs" that identify common treatment principles, outcomes and administrative standards.63 The Divisions also have promulgated practice guidelines for the treatment of individuals with the most severe co-occurring disorders.64
States are also implementing innovative strategies for financing integrated services for individuals with co-occurring disorders, blending together state and local tax dollars, mental health and substance abuse block grant funds, and Medicaid dollars.65
Effectively supporting people with co-occurring substance abuse disorders frequently requires states to pursue strategies that fall outside the direct purview of federal Medicaid policy. In this arena, states must often invest dollars to create new system capabilities by financing services' start-up costs. Many states have used federal mental health and substance abuse block grant dollars to do so, as well as to underwrite necessary provider training.66
Federal Medicaid Policies Affecting Services for Persons with Co-Occurring Substance Abuse Disorders
States may offer substance abuse treatment services under the Medicaid clinic and/or rehabilitative services coverage categories. Federal policies concerning Medicaid coverage of substance abuse services are not different from those that apply to the coverage of mental health services. Under the rehabilitative services option, for example, states may elect to cover treatment services, counseling and other services that promote the recovery of persons who have a substance abuse disorder.
In general, states make markedly less extensive use of Medicaid to underwrite substance abuse services than mental health services.67 Only about one-half the states offer substance abuse services under the Medicaid rehabilitative services option and several of these cover only limited outpatient services. There are several states that do not cover substance abuse services for adults at all under either the clinic or rehabilitative services options. At the same time, many states have implemented more robust coverages of substance abuse services. For example, Minnesota's coverage spans a wide-array of substance abuse rehabilitation services.68
In the case of individuals who have co-occurring disorders, assorted problems have arisen in integrating Medicaid substance abuse treatment with mental health treatment. One problem stems from the practice of targeting services by "primary" disorder. For example, individuals who have "primary" mental disorders might be prevented from receiving substance abuse services when services eligibility criteria limit services to persons who have a "primary" substance abuse disorder (and vice versa). As services for individuals with co-occurring disorders have evolved, limiting services by "primary" disorder has given way to the recognition that there is no hierarchy of disorders because both exist independently. Along these lines, state policy changes, such as those made in Texas and Missouri, aid in avoiding this problem. Another problem often arises in the arena of provider qualifications. When provider qualifications that apply to substance abuse and mental health services differ significantly, it can be difficult for a provider in one system of care to employ Medicaid dollars that are tied to the other system of care that has different provider qualifications. In order to integrate services within one system or the other, states should consider strategies to cross-certify providers to furnish services. The foregoing problems, of course, parallel some of the generic challenges previously described in serving individuals with co-occurring disorders. Federal Medicaid policy does not dictate that the coverage of mental health and substance abuse services must be constructed in a silo-like fashion (i.e., the coverage of substance abuse services must be completely distinct from the coverage of mental health services). Some states have crafted interlocking rehabilitative option coverages of mental health and substance abuse services. For example, Georgia's rehabilitative services coverage (see Appendix B) spans both mental health and substance abuse services. Some of the services included in Georgia's coverage (e.g., ACT) are available for persons who have a mental illness, a substance abuse disorder, and/or co-occurring disorders. Defining services in this fashion avoids creating silos. As one would expect, some services that Georgia offers are specific to the treatment of substance abuse or mental illnesses (because not everyone who has a substance abuse disorder also has a mental illness, and vice versa.) In addition, Georgia's provider specifications require that community agencies have the capability to serve both populations, another means of avoiding silos.
Missouri's substance abuse rehabilitative services coverage (Comprehensive Substance Abuse and Rehabilitation -- CSTAR) specifically incorporates services for individuals with co-occurring disorders. Services include individual and group counseling, psychosocial education, residential support, family therapy and co-dependency counseling. CSTAR provides for the management of co-occurring disorders and mental health services.69 It builds on the previously described steps that Missouri has taken to adopt common principles for the treatment of substance abuse and mental health services. In Missouri, providers who meet applicable requirements can be cross-certified to furnish both mental health and substance abuse services.
When a state has elected not to cover substance abuse treatment services as a distinct coverage under its state plan, it may still provide for their provision as components of the rehabilitative services that it furnishes to individuals with serious mental illnesses. Many states have incorporated substance abuse/addictive services into their coverage of mental health rehabilitative services and, thereby, created a framework for furnishing integrated treatment for individuals with co-occurring disorders through a single treatment team, or a program using a single service plan.70 For example, ACT teams must have the capacity to address the needs of individuals who also have a substance abuse disorder.
State coverages of ACT services include the treatment of both disorders, employing an integrated, multidisciplinary approach. Even when a state separately covers substance abuse services, these services still may be incorporated into mental health rehabilitative services provided there is no duplicate billing for services. In addition, if a state's coverage of substance abuse services provides only for limited outpatient benefits, additional services can be incorporated into the coverage of mental health services (e.g., furnishing substance abuse counseling as part of illness management services).
In some states where Medicaid mental health services are furnished through a 1915(b) or 1115 waiver program, the program encompasses both mental health and substance abuse services. For example, as discussed in Chapter 6, Iowa elected to pull together both types of services together under a single 1915(b) waiver program rather than continue to operate each type of service under a distinct waiver program. While spanning both categories of services in a waiver program does not necessarily resolve all the problems associated with integrating services for persons with co-occurring disorders, it offers the potential for avoiding or mitigating funding silo problems.
Federal coverage policies do not preclude the integration of mental health and substance abuse services for persons with co-occurring disorders. States may craft rehabilitative services coverages that provide for such integration. More challenging for states may be creating and expanding the capacity to deliver integrated treatment services for individuals with these co-occurring disorders.
Services for Individuals with Co-Occurring Developmental Disabilities
Depending on the definition of mental illness used, there are varying estimates of the number of persons who have both a serious mental illness and a developmental disability such as mental retardation (sometimes referred to as persons with a "dual diagnosis").71 Some state administrators estimate that the rate of occurrence of major mental illness in individuals with a developmental disability is similar to the rate in the general population.72 In other words, probably between 5 to 7 percent of adults with developmental disabilities also have a major mental illness. Although in absolute terms the number of working-age adults who have a developmental disability and a major mental illness is relatively small, frequently they consume a disproportionate share of service system resources.
Serving individuals who have both a serious mental illness and a developmental disability is garnering increased attention. Such individuals frequently pose significant service delivery challenges. Problems arise in the arena of diagnosis, with mental illness sometimes misidentified as maladaptive behavior. Diagnosis is also more challenging among individuals with more severe mental retardation. Since this is a very low incidence population, and treatment can be complex, there are a limited number of providers and professional practitioners (especially psychiatrists) who have the requisite capabilities to serve these individuals.
For persons who have a both a mental illness and a developmental disability, systems issues frequently arise at both the state and local levels, stemming from lack of coordination between the mental health and developmental disabilities services sys-tems. As with substance abuse, these issues often revolve around questions concerning "primary diagnosis." In some states, a significant number of individuals with a co-occurring developmental disability have been institutionalized in state IMDs.73 In addition, these individuals frequently experience high rates of community hospitalization. Sometimes, they bounce between the mental health and developmental disabilities systems or unfortunately, fall between the cracks. These persons also experience involvement in the criminal justice system.
Several states have taken active steps to improve services for persons with serious mental illnesses and developmental disabilities. In 2002, the National Association of State Directors of Developmental Disabilities Services (NASDDDS) and the National Association of State Mental Health Program Directors (NASMHPD) surveyed state MRDD and mental health directors to identify elements important for effectively serving individuals with these co-occurring disorders. Department directors identified strategies that they regard to be important, including entering into written interagency agreements, creating interagency task forces, coordination of services and payments, cross-system provider training, and joint involvement in hospital discharge planning.74 In about one-third of the states, the administration of mental health and developmental disabilities services is located in the same state agency, a step that can potentially facilitate the delivery of services to individuals with these co-occurring conditions.
The Ohio Departments of Mental Health and the Department of Mental Retardation and Developmental Disabilities have forged an interagency agreement that spells out specific joint responsibilities as well as those for each agency. Each department is responsible for identifying individuals with co-occurring disorders within their own systems, cross-training local agencies and providers, and promoting communication across programs at the county level.75 In addition, the departments have collaborated in identifying clinical best practices in serving individuals with developmental disabilities and mental illness.76 At the local level, some county boards of mental retardation and developmental disabilities operate Program of Assertive Community Treatment (PACT) teams that serve individuals with these co-occurring disorders.
Pennsylvania's Office of Mental Retardation has promulgated a framework to be followed at the county level to assure service coordination between the mental health and mental retardation administrators. This framework includes provisions for:
- Engaging providers who have experience and expertise in treating individuals with co-occurring mental illness and mental retardation;
- Ensuring that a lead agency (MH or MRDD) is identified for each dually diagnosed individual that enters the system; and,
- Implementing cross-system trainings within each system at both the administrator and provider level77
In Arizona, an agreement has been forged between the state behavioral health and developmental disabilities authorities concerning the provision of services to individuals with co-occurring disorders. This agreement provides for the deployment of expert consultation to address the needs of such individuals.
Federal Medicaid Policies Affecting Services with Co-Occurring Developmental Disabilities
As in the case of individuals with co-occurring substance abuse disorders, federal Medicaid policy principally affects the financing of services on behalf of individuals with co-occurring developmental disabilities. This topic can be confusing. As discussed in Chapter 4, federal policy differentiates between the coverage of "rehabilitative" and "habilitative" services. Habilitative services are closely identified with services for persons with developmental disabilities and federal payment for them is limited to services furnished in ICFs/MR or through an HCBS waiver program that serves as an alternative to placement in an ICF/MR. Habilitative services may not be furnished under the rehabilitative services option except in a limited number of states.78
However, this does not mean that individuals with developmental disabilities may not receive mental health treatment and related services under the clinic or rehabilitative services options. Individuals with developmental disabilities who meet the "services eligibility" criteria that apply to a state's Medicaid mental health services may be furnished such services on the same basis as other Medicaid beneficiaries. As in the case of individuals with a co-occurring substance abuse disorder, limiting services to individuals with a "primary" mental illness diagnosis sometimes leads to the disqualification of individuals with developmental disabilities from receiving necessary mental health treatments. Emerging best practice is that "phrases such as 'primary diagnosis' no longer have relevance nor should they be used in determining service delivery to persons with mental illness and developmental disabilities."79 Integrated treatment approaches are also aided when provider qualifications are established that permit the cross-certification of providers. Ohio has taken this step and, hence, cleared the way for developmental disabilities providers to implement PACT teams.
In its rehabilitative services coverage (see Appendix B), Georgia has specifically provided that individuals with a co-occurring mental illness and mental retardation or other developmental disability are among those who may receive mental health treatment services. Services that they may receive include crisis residential services and community support services, which include rehabilitative, environmental support, and targeted case management, which is considered essential to assist individuals to obtain necessary services.
They may also receive: 1) evaluations and assessments to identify barriers that impede the development of skills necessary for independent functioning in the community; 2) assistance and support in crisis situations; 3) symptom monitoring and self management of symptoms; 4) assistance to increase social support skills that ameliorate life stresses resulting from the person's disability; and 5) coordination to gain access to necessary rehabilitative and medical services; and 6) coordination of services in the Individual Service Plan.80
In developmental disabilities services, the 1915(c) HCBS waiver program has emerged as the dominant Medicaid financing vehicle for community services. Through their HCBS waiver programs, states commonly cover "behavioral services" that include the treatment of co-occurring mental disorders. Because an HCBS waiver program cannot generally cover services that are otherwise available through a state's Medicaid program, it has not been common for states to include mental health services per se in their waiver programs.81 HCBS waiver participants, of course, are eligible for the mental health services that a state offers under its Medicaid state plan.
Some states have employed the HCBS waiver program to develop especially strong capabilities for serving individuals with co-occurring conditions. One such state is Vermont which created the Crisis Intervention Network as a critical element of its successful effort to shift all individuals with developmental disabilities to the community and close its only public institution. The aim of the Network is to avoid hospitalization.
Vermont recognized that, in order to close its institution, it had to establish effective services in the community to address the needs of persons who experience psychiatric or behavioral crises. The Network furnishes consultation to community agencies to support persons experiencing a crisis, including dispatching staff to work with the person. The Network also maintains a small crisis residential capacity. This especially effective capacity was developed independent of Vermont's mental health system but has the capacity to deliver critical mental health services to individuals.82
In summary, states can use Medicaid to serve adults with serious mental illness who also have a co-occurring developmental disability. Simply put, these individuals are eligible for any Medicaid clinic and rehabilitative mental health services that a state already provides, subject to the criteria that a state spells out in its Medicaid plan. The difficulties that lie in effectively supporting this population are very real, but generally lie outside of funding/eligibility issues. While challenges continue to exist in terms of system collaboration and service delivery, states are taking significant steps to build agency relationships, train providers, and generally integrate important services across systems to support dually diagnosed adults in the community.
Conclusion
While Medicaid can not provide the full range of services and supports needed by working-age adults with serious mental illnesses, it can be used to cover the costs of critical services. Sometimes Medicaid funding of mental health services is presumed to be exclusively reserved for professional treatment of the mental illness. However, as illustrated in this chapter, Medicaid funding can also be employed for rehabilitative services to support individuals in recovery. Medicaid services such as ACT and crisis intervention can improve the community tenure of individuals who might otherwise require costly hospitalization or institutionalization. People with serious mental illnesses can be supported to live successfully in the community through the provision of a variety of rehabilitative services and supports.
Annotated Bibliography
Chris Koyanagi and Rafael Semansky (2001). Recovery in the Community: Funding Mental Health Rehabilitative Approaches Under Medicaid. Washington DC: Bazelon Center for Mental Health Law.
This comprehensive report describes how states have covered rehabilitative and case management services for adults with mental illnesses under Medicaid. The report contains extensive information concerning Medicaid coverage policy and furnishes examples of state coverages of many critical community services. Available for purchase from the Bazelon store at store.bazelon.org/medicaid.html
Supporting Individuals with Co-Occurring Disorders Report to Congress on the Prevention and Treatment of Co-Occurring Substance Abuse Disorders and Mental Disorders (2002). Rockville MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration. Available at samhsa.gov/reports/congress2002/index.html
This comprehensive report contains in-depth information about state-of-the-art services for individuals with co-occurring substance abuse and mental disorders, including service delivery system challenges, evidence-based practices, and other important facets of supporting persons with co-occurring disorders. The report also profiles efforts in several states to improve services for individuals with co-occurring mental illnesses and substance abuse disorders.
National Association of State Mental Health Program Directors and National Association of State Alcohol and Drug Abuse Directors (2002). Exemplary Methods of Financing Integrated Service Programs for Persons with Co-Occurring Disorders. Final Report of the NASMHPD-NASADAD Task Force on Co-Occurring Disorders. Alexandria Virginia and Washington DC. Available at alt.samhsa.gov/reports/congress2002/App_III.pdf.
This report identifies critical issues in serving individuals with co-occurring mental illnesses and substance abuse disorders. It includes in-depth profiles of exemplary programs in several states for such persons, concentrating on the financing of such programs through multiple funding sources, including Medicaid.
Endnotes
-
Maine Medical Assistance Manual, Chapter II, Section 17.01
-
Koyanagi and Semansky (2001). Op. cit.
-
Catalano, R., et al. Psychiatric Emergency Services and the System of Care. Psychiatric Services, 54(3): March 2003.
-
As with all other references to the number of states offering a particular coverage, this figure is as of January 2004.
-
Wisconsin Medicaid Provider Handbook -- Part H, Division VI: Mental Health Crisis Intervention Services.
-
NAMI has been an influential force in advocating and maintaining standards for ACT programs. Additional materials regarding ACT can be found on its web site at nami.org/Template.cfm?Section=ACT-TA_Center
-
West Virginia Medicaid State Plan (edited for clarity).
-
For additional information concerning Minnesota's policies, please see: Department of Human Services Bulletin 03-53-01 -- "Medical Assistance Adult Mental Health Crisis Response Services" (March 2003), available at dhs.state.mn.us/main/groups/publications/documents/pub/DHS_id_004835.pdf
-
For rural ACT programs, ACT standards provide for slightly lower coverage.
-
Koyanagi and Semansky (2001). Op. cit.
-
Key Findings on States' Use of Medicaid to Finance ACT Services. (2003). The Lewin Group.
-
According to the NAMI PACT standards, ACT teams shall average at least 3 contacts per consumer per week. However, "the ACT team shall have the capacity to provide multiple contacts a week with clients experiencing severe symptoms, trying a new medication, experiencing a health problem or serious life event, trying to go back to school or starting a new job, making changes in living situation or employment, or having significant ongoing problems in daily living. These multiple contacts may be as frequent as two to three times per day, seven days per week and depend on client need and a mutually agreed upon plan between clients and program staff."
-
Rehabilitation Services for the Mentally Ill. State Medicaid Directors Letter (1992).
-
National Association of State Mental Health Program Directors Research Institute, Inc (2002). Implementation of Evidence-Based Services by State Mental Health Agencies: 2001. Alexandria VA. Available online at nri.rdmc.org/Profiles01/02EBP2001.pdf
-
District of Columbia Medicaid State Plan
-
Missouri Medicaid Provider Manual -- Community Psychiatric Rehabilitation Program, Section 13.15 (Intensive Community Psychiatric Rehabilitation Program). Available online at medicaid.state.mo.us/lpBin22/lpext.dll?f=templates&fn=main-j.htm&2.0
-
Liberman, R.P., Wallace, C.J., et al. (1998). Skills training versus psychosocial occupational therapy for persons with persistent schizophrenia. American Journal of Psychiatry, 155, 1087-1091.
-
Susan Langley, CMS Teleconference, October 2002.
-
New Hampshire Department of Human Services, He-M 426.11 Mental Illness Management Services.
-
Copeland, M. Evaluation of the Vermont Recovery Education Project Available online at mentalhealthrecovery.com/vtrecovery.html
-
PNFCMH (2003)
-
In February, 2004, South Carolina was just beginning to implement its peer support specialist program, with the goal of having 34 peer specialists by the end of 2004. For more information, please see: dhhs.state.sc.us/NR/rdonlyres/equ5biagewnmf5y3kacydzruenoxz62yyd5fraoxrhsvmaaurn7b2dyu53bw2mbbdzi2rj3dhvc6ka/BullNewMedicaidReimbursableServiceMHPeerSupport1.pdf
-
Under its 1915(b) specialty mental health services waiver program, Iowa also requires its contractor to foster the development of peer support groups.
-
Iowa Human Services Rules. 441-78.48(249a): Rehabilitation services for adults with chronic mental illness. Available online at dhs.state.ia.us/policyanalysis/PolicyManualPages/Manual_Documents/Rules/441-78.pdf
-
Ibid.
-
Ibid.
-
Missouri Rules of Department of Mental Health: Chapter 4 -- Mental Health Programs. Available online at sos.mo.gov/adrules/csr/current/9csr/9c30-4.pdf
-
Burt, M. (2001). What will it take to end homelessness? Urban Institute Brief. Washington, DC: Urban Institute.
-
PNFCM (2003)
-
Iowa Department of Human Services Rules. 78.48(6)(a)(1). Available online at www.dhs.state.ia.us/policyanalysis/PolicyManualPages/Manual_Documents/Rules/441-78.pdf
-
Minnesota Rehab Policy. Available online at dhs.state.mn.us/main/groups/publications/documents/pub/DHS_id_003917.pdf
-
"Homes Keep Mentally Ill Stable" Associated Press, January 30, 2004.
-
Hannigan, T. & Wagner, S. (2003). Developing the "Support" in Supportive Housing: A Guide to Providing Services in Housing. Center for Urban Community Services . Available online at documents.csh.org/documents/pubs/DevelopingSupport-full.pdf
-
Ibid.
-
Medicaid in Supportive Housing: Lessons for Policy-Makers. (2003). Corporation for Supportive Housing. Available online at documents.csh.org/documents/policy/Med/MedicaidLessons.pdf
-
Go to: csh.org/index.cfm?fuseaction=Page.viewPage&pageID=458
-
President's New Freedom Commission on Mental Health. Achieving the Promise: Transforming Mental Health Care in America. DHHS Pub. No. SMA-03-3832. Rockville, MD: 2003.
-
New Freedom Commission Interim report. Available online at mentalhealth.org/publications/allpubs/NMH02-0144/unemployment.asp
-
Nebraska Department of Social Services Manual: Rehabilitative Psychiatric Services. Available online at sos.state.ne.us/local/regsearch/Rules/Health_and_Human_Services_System/Title-471/Chapter-35.pdf
-
Georgia's Consumer-Driven Road to Recovery: A Mental Health Consumer's Guide for Participation in and Development of Medicaid Reimbursable Peer Support Services. Georgia Division of Mental Health, Developmental Disabilities, and Addictive Diseases. March 2003.
-
In a home and community-based waiver program, states may cover supported employment services as an "extended habilitation service." A second exception is when a state furnishes mental health services under a "freedom of choice" waiver. Some states that operate such waiver programs cover vocational services by invoking the Section 1915(b)(3) "savings" provision (described in Chapter 6). Also states may furnish vocational services in a behavioral health carve-out in a comprehensive health care reform waiver program (also described in Chapter 6).
-
Family Psychoeducation Implementation Resource Kit: Information for Public Mental Health Authorities. Available online at mentalhealthpractices.org/fam_pmha.html
-
Koyanagi and Semansky (2001). Op. Cit.
-
Texas Medicaid State Plan
-
Kansas Medicaid State Plan
-
Personal communication with Valley Mental Health Director, July 2003.
-
Vermont Medicaid State Plan
-
Maine Medical Assistance Manual, Chapter II, Section 17.04-3
-
NASMHPD Research Institute (2001). Op. Cit.
-
DC Medicaid State Plan
-
Personal communication: Dr. Joseph Parks, Missouri Department of Mental Health Medical Director, January 2004.
-
There are, of course, other co-occurring disorders beyond those discussed here. There also is a relatively high incidence of mental illness among individuals who have HIV/AIDS or have experienced a brain injury.
-
SAMHSA (2002). Op. cit.
-
Ibid.
-
Ibid.
-
PNFCMH (2003).
-
National Association of State Mental Health Program Directors Research Institute (2002). Implementation of Evidence-Based Services by State Mental Health Agencies: 2001. Alexandria VA. NRI reported that four states were implementing evidence-based co-occurring disorder treatment practices statewide and another 26 in parts of their states. Another 11 were piloting or planning to implement these practices.
-
National Association of State Mental Health Program Directors Research Institute (2002). State Mental Health Agency Organization and Structure: 2001. Alexandria, VA.
-
New Mexico's efforts along these lines are profiled in: Christine A. Cline, MD, MBA and Kenneth Minkoff, MD (2002). A Strength-Based Systems Approach to Creating Integrated Services for Individuals with Co-occurring Psychiatric and Substance Abuse Disorders. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Administration. Available at alt.samhsa.gov/reports/NewMexico/main.htm.
-
Texas Administrative Code, Rules of the Texas Department of Mental Health and Mental Retardation, Title 25, Part II. Standards for Services to Persons with Co-Occurring Psychiatric and Substance Abuse Disorders, Chapter 411, Subchapter N. Available at treatment.org/Topics/word/TDMHMRCOPSDRule.doc
-
SAMHSA (2002), op. cit. Missouri's practice guidelines are located at dmh.missouri.gov/cps/issues/codisorders.pdf
-
See especially: National Association of State Mental Health Program Directors and National Association of State Alcohol and Drug Abuse Directors (2002). Exemplary Methods of Financing Integrated Service Programs for Persons with Co-Occurring Disorders. Final Report of the NASMHPD-NASADAD Task Force on Co-Occurring Disorders. Alexandria Virginia and Washington DC. See also SAMHSA (2002), op. cit.
-
SAMHSA (2002), op. cit.
-
Ibid. In 1997, state-federal Medicaid spending for substance abuse services was only about $1 billion compared to $20 billion for mental health services.
-
Minnesota covers: (a) primary rehabilitation (intensive therapeutic services for individuals who do not require detoxification); (b) outpatient rehabilitation (services furnished in a supervised living facility, another community facility or the person's own home); (c) extended rehabilitation (individual and group counseling and education); (d) transitional rehabilitation (services in a transitional semi-independent living arrangement with an emphasis on after-care and securing employment); and, (e) collateral counseling.
-
See: dmh.missouri.gov/ada/facts/cstar.htm.
-
Koyanagi, C. and Semansky, R. (2001). Op. cit.
-
Fletcher, R. Information on Dual Diagnosis. (2001). National Association of Dual Diagnosis. Available online at www.thenadd.org/content/aboutnadd/ddinfo.shtml
-
Teleconference -- Meeting the Needs of Individuals with Co-Occurring Developmental Disabilities and Mental Illness. November 20, 2003. Sponsored by: National Association of State Directors of Developmental Disabilities Services.
-
However, the number of such individuals has declined considerably in the past decade, in part due to litigation concerning the adequacy and appropriateness of the services such individuals receive.
-
Chas Moseley (2004). Survey on State Strategies for Supporting Individuals with Co-existing Conditions [NASDDDS Technical Report]. Available online at http://www.nasddds.org/pdf/NTR-CoexistingConditions.pdf.
-
This agreement is located at odmrdd.state.oh.us/Includes/Press_Releases/MH_InterAgy_Agreement.pdf.
-
Ohio Department of Mental Health -- Ohio Department of Mental Retardation and Developmental Disabilities Advisory Council. (2001). Clinical Best Practices for Serving People with Developmental Disabilities and Mental Illness. (2001). (Author) Available online at mh.state.oh.us/reference/mimr-02282002.pdf
-
Pennsylvania Office of Mental Retardation Bulletin 00-02-16. December, 2002.
-
Some states are permitted to provide habilitation services under the provisions of the Omnibus Budget Reconciliation Act of 1989. States that did not cover such services prior to the enactment of OBRA '89 are not permitted to add the coverage of habilitation services under the rehabilitation services option.
-
Ohio Department of Mental Health et al. (2001). Op. cit.
-
Georgia Department of Human Resources (2003). Community Mental Health Provider Manual. Available online at www2.state.ga.us/departments/dhr/mhmrsa/pdf/ProviderManFY04.pdf
-
However, under an HCBS waiver program, a state can provide "extended state plan" services. This permits a state to cover additional services over and above any limits that may be in effect in the state plan.
-
For a more detailed discussion see: Frawley, P. & Vecchione, E. (2001) Ten Years of Prevention: The Vermont Crisis Intervention Network. Impact 14:1 (University of Minnesota, Institute on Community Integration). Available at ici.umn.edu/products/impact/141/prof1.html
Attachment A: Operational Features of Georgia's Coverage of ACT
Georgia includes ACT as part of its wide-ranging continuum of rehabilitative services for adults with serious mental illnesses. Georgia’s rehabilitative services Medicaid state plan provisions are contained in Appendix C. As its most intensive community service, Georgia reserves ACT for individuals with especially high needs. Georgia provides for step-downs from ACT for individuals who may no longer require the intensity of ACT but who can benefit from continuing supports. Once approved for services, consumers are re-evaluated every six months and may be re-authorized to remain in ACT or step down, based on their progress. ACT consumers and team members develop an individual treatment plan, including personalized goals. Among the services that the ACT team may provide are: crisis assessment and intervention; personal social and interpersonal skill training; medication management and education; psycho-educational support for the individual and family; substance abuse counseling; symptom management; skill development and others. The specific operational features of Georgia’s ACT coverage are detailed below:1
Services Eligibility Criteria
Georgia reserves ACT for individuals with severe and persistent mental illnesses that seriously impair their functioning. Priority is given to people with schizophrenia, other psychotic disorders (e.g., schizoaffective disorder), or bipolar disorder. Significant functional impairments can include: the inability to consistently perform the range of practical daily living tasks required for basic adult functioning in the community; the failure to recognize and avoid common dangers or hazards to self and possessions; persistent or recurrent failure to perform daily living tasks except with significant support or assistance from others such as friends, family, or relatives; and the inability to be consistently employed at a self-sustaining level or inability to consistently carry out homemaker roles (e.g., household meal preparation, washing clothes, budgeting, or child-care tasks and responsibilities). ACT also may be appropriate for persons who are unable to maintain a safe living situation; are high users of psychiatric hospital or crisis emergency services; have persistent or very recurring major symptoms; have a high risk or a recent history of criminal justice involvement; are unable to meet their basic survival needs; and/or are served in an inpatient or other closely supervised setting and could live more independently with more intensive community support. In addition, candidates for ACT are individuals for whom a lower level of care has been tried and found to be ineffective.
Service Requirements:
Georgia specifies that
- Assertive Community Treatment must include a comprehensive and integrated set of medical and psychosocial services provided in non-office settings by a mobile multidisciplinary team. The team provides community support services that are interwoven with treatment and rehabilitative services and regularly scheduled team meetings. Team meetings must be held a minimum of three times a week.
- Services and interventions are highly individualized and tailored to the needs and preferences of the consumer, with the goal of maximizing independence and supporting recovery. Sixty percent (60%) of all services involve face-to-face contact with consumers. The majority of face-to-face services (80% or more) are provided in locations other than the office (including the consumer’s home), according to individual need, preference and clinical appropriateness.
- It is recommended that the ACT Team provides at least three face-to-face contacts per week with most consumers on an ongoing basis and all individuals participating in ACT must receive a minimum of four face-to-face contacts per month. The Team must see each consumer once a month for the purpose of symptom assessment/ management and management of medications.
- Services may be delivered by a single team member to two ACT consumers at the same time if goals are compatible; however, this should not be a standard practice. Services should never be offered to a group of more than two individuals.
Staffing Requirements include:
- A full-time Team Leader who is the clinical and administrative supervisor of the team and also functions as a practicing clinician on the team.
- A Psychiatrist on a full-time or part-time basis. The psychiatrist provides clinical and crisis services to all team consumers, works with the team leader to monitor each consumer’s clinical status and response to treatment, and directs psychopharmacologic and medical treatment.
- One full-time equivalent Registered Nurse who provides nursing services for all team consumers and who works with the team to monitor each consumer’s clinical status and response to treatment.
- One-half to one full-time equivalent Substance Abuse Professional (SAP) who works on a full-time or half-time basis and provides or accesses substance abuse services for team consumers.
- A clinically trained practitioner who is either a Mental Health Professional or a Licensed Clinician and who provides individual and group supportive therapy to team consumers.
- One certified Peer Support Specialist who carries out rehabilitation and support functions and who should be a person in recovery
- Three paraprofessionals (or professionals) who provide services under the supervision of a Licensed Clinician; one of these staff must be a vocational rehabilitation specialist.
- The SAP, MHP, Peer Support Specialist and two paraprofessionals function as primary practitioners for a caseload of consumers. The Team Leader, Registered Nurse, and vocational rehabilitation specialist also function as primary practitioners for a partial caseload of consumers.
- The ACT team maintains a small consumer-to-clinician ratio, usually no more than ten to twelve consumers per staff person.
Provider Qualifications
- ACT Teams must have the ability to deliver services in various environments, such as homes, schools, jails, homeless shelters, street locations, etc.
- The organization has policies which govern the provision of services in natural settings and can document that it respects consumers’ and/or families’ right to privacy and confidentiality when services are provided in these settings.
- Each ACT Team provider has policies and procedures governing the provision of outreach services, including methods for protecting the safety of staff who engage in outreach activities.
- The organization has established procedures/protocols for handling emergency and crisis situations which describe methods for triaging consumers who require psychiatric hospitalization.
- The organization must have an Assertive Community Treatment Organizational Plan that addresses the following:
- description of the particular rehabilitation, recovery and case management models utilized, types of intervention practiced, and typical daily schedule for staff;
- description of the staffing pattern and how staff are deployed to ensure that the required staff-to-consumer ratios are maintained, including how unplanned staff absences, illnesses, etc. are accommodated;
- description of the hours of operation, the staff assigned and types of services provided to consumers, families, and/or guardians; and
- description as to how the plan for services is modified or adjusted to meet the needs specified in each consumer’s Individual Service Plan; and
- description of inter-team communication regarding consumer support (e.g., email, team staffings, etc.)
- Services must be available 24 hours a day, seven days a week with emergency response coverage, including psychiatric availability. The team must be able to rapidly respond to early signs of relapse and decompensation and must have the capability of providing multiple contacts daily to consumers in acute need. On call coverage must be provided by staff that is skilled in crisis intervention.
Attachment B: Peer Supports in Georgia
Georgia provides for both peer-delivered and peer support services.
Certified Peer Specialists. The state incorporates “certified peer specialists” (CPS) into many of the services furnished under its rehabilitative services coverage. Peer specialists “perform a range of tasks to assist consumers in regaining control over their own lives and over their recovery processes. Peer specialists model competence and the possibility of recovery and assist consumers in developing the perspective and skills that facilitate recovery.”2 Moreover, according to the official job description, a CPS “provides peer services; serves as a consumer advocate; and provides consumer information and peer support for consumers in emergency, outpatient, or inpatient settings.” Certified peer specialist candidates must meet stringent criteria and demonstrate that they have the necessary skills and philosophy to furnish effective supports. First, specialists must be current or former recipients of mental health services. They also must have had some prior involvement or training in an advocacy or advisory capacity. Candidates go through a two-weeks training program that culminates in written and oral examinations in order to be certified.3 Certified peer specialists are required members of community support and ACT teams and woven into other services. Peer specialists work side-by-side with other program staff and bring a consumer-driven recovery philosophy to services.
Peer Supports. Distinct from but intimately tied to Georgia’s peer specialist initiative is its unique rehabilitative services coverage of peer supports, a consumer-driven and consumer-led service. Georgia’s coverage is as follows:
This service provides structured, scheduled activities that promote socialization, recovery, self-advocacy, development of natural supports, and maintenance of community living skills, under the direct supervision of a mental health professional. Consumers actively participate in decision-making and program operation. Services are directed toward achievement of the specific goals defined by the individual and specified in the Individual Service Plan (ISP), and provided under the direct supervision of a Mental Health Professional. The interpersonal interactions and activities within the program are directed, supervised, guided and facilitated by the Mental Health Professional (MHP)in such a way to create the therapeutic community or milieu effect required to achieve individual treatment goals within a controlled environment. This concept is similar to the manner in group therapy sessions in which the staff leader or therapeutic community setting utilizes the interactions of the group members to achieve the desired individual therapy goals.4
| Principles of Peer Supports and Recovery | |
Peer supports program must actively incorporate the Georgia Consumer Council’s recovery principles into their services and activities:
|
Launched in late 2001, the peer supports program now uses 130 peer specialists who support about 3,000 consumers. The program affords individuals the opportunity to exercise control over their own recovery and provide mutual support to each other. The purpose of peer supports is to “provide an opportunity for consumers to direct their own recovery and advocacy process and to teach and support each other in the acquisition and exercise of skills needed for management of symptoms and for utilization of natural resources within the community.”5 Peer supports are intended for adults with serious and persistent mental illness who:
- “Require and would benefit from support of peers for the acquisition of skills needed for management of symptoms and for utilization of natural resources in the community AND
- Need assistance to develop self-advocacy skills in order to achieve decreased dependency on the mental health system OR
- Need assistance and support to prepare for a successful work experience OR
- Need peer modeling in order to take increased responsibilities for his/her own recovery OR
- Need peer support in order to maintain daily living skills.”6
Peer support is incorporated into a person’s Individualized Service Plan (ISP). Through Peer Support, “each consumer should set his or her own individualized goals and assess his or her own skills and resources related to goal attainment. Goals are set by exploring strengths and needs in the consumer’s living, learning, social and working environments …. Each consumer must be provided the opportunity for peer assistance in the development and acquisition of needed skills and resources necessary to achieve stated goals.”7
Peer supports programs are based at a program site but activities also may take place in natural community settings. Peer support programs may be freestanding or affiliated with another organization. In either case, 75% of the members of governing boards/advisory boards for peer support programs must be consumers. Furthermore, individuals who receive peer supports “must be given the opportunity to participate in and make decisions about the activities that are conducted or services offered within the Peer Supports program.”8 In addition, a Peer Supports program must offer a range of skill-building and recovery activities developed and led by consumers. These activities must include those that will most effectively support achievement of the individual consumer’s rehabilitation and recovery goals.”9
A peer supports program must be under the clinical supervision of a mental health professional (preferably one who is also a certified peer specialist) and a peer specialist must lead and manage day-to-day program operations. Additionally, services must be provided and/or activities led by peer specialists or other consumers, supervised by a peer specialist. Peer support centers are open for a minimum of four hours a day, three days per week, and provide an opportunity for consumers to come together and support one another through formal group activities as well as more informal social and recreational endeavors. Programmatic supports are built into center activities such as community outings, art and other leisure activities, community meals, and educational seminars.
-
Georgia Medicaid Community Mental Health Center Program Manual. Op. cit.
-
Recovery in the Community.
-
Sabin, J. & Daniels, N. (2003). Strengthening the consumer voice in managed care: VII. The Georgia Peer Specialist program. Psychiatric Services, 54 (4). 497-498.
-
Georgia Medicaid Community Mental Health Center Program Manual. Op. cit.
CHAPTER 6: MEDICAID WAIVERS
| By obtaining waivers of federal Medicaid law, a state may reconfigure the delivery of Medicaid services. States have employed Medicaid waivers to implement managed care service delivery models for mental health services. Such models have potential advantages for improving the delivery of mental health services but can also pose challenges. About 30 percent of the states deliver mental health services for working-age adults with serious mental illnesses through a managed care delivery system. |
Federal Medicaid law contains numerous requirements with which a state must comply in order to obtain federal financial participation in the costs of providing services to beneficiaries. Some of these requirements dictate the use of fee-for-service payment methods and prevent a state from selectively contracting with preferred vendors to deliver services. However, the Social Security Act also gives the Secretary of Health and Human Services the authority to waive statutory requirements under certain conditions; such waivers include those necessary to permit a state to depart from the conventional Medicaid service delivery organizational and financing framework. There are two waiver authorities in Title XIX of the Act that permit the Secretary to waive specific provisions of federal Medicaid law. In addition, Title XI of the Act contains a broader authority that permits the waiver of a wider range of statutory provisions.
Several states have employed these waiver authorities to restructure Medicaid mental health services in order to implement managed care service delivery models and other system reforms. These states furnish mental health services under "freedom of choice" waivers granted under §1915(b) of the Act, or as part of broader demonstration programs operated under §1115 of the Act. In the case of individuals with serious mental illnesses, states have made limited use of the third waiver authority contained in §1915(c) of the Act. This authority permits a state to offer alternative community services to individuals who would otherwise qualify for services in a Medicaid-reimbursable institutional setting.
This chapter discusses the basic features of these waiver authorities. It also describes how states have employed these authorities in the delivery of Medicaid mental health services. To provide the context for understanding these waiver authorities, the chapter first provides a brief overview of how states have used managed care generally in their Medicaid programs, followed by a brief discussion of managed mental health services, and Medicaid waivers and managed care.
Background: Medicaid and Managed Care
In the early 1990s, states began shifting the delivery of Medicaid services to managed care service delivery models. The rationale and essential features of managed care are outlined in "Managed Care in Brief" on the following page.
During this period, states had to obtain federal waivers in order to expand their use of managed care arrangements. Waivers were necessary for states to mandate that beneficiaries enroll in a managed care plan and selectively contract with managed care organizations to deliver services. Federal waivers also were necessary in order for a state to expand services to uninsured populations that could not be covered using existing statutory authorities.
Managed care has taken hold more slowly in Medicaid than in the private sector but its use has grown rapidly. Some states implemented broad state "health care reform" initiatives designed to extend health services to uninsured individuals who could not otherwise qualify for Medicaid (e.g., low-income childless adults). These initiatives were coupled with extensive use of managed care in order to secure cost savings that could be used to underwrite services for additional individuals. Massachusetts (Mass Health) and Oregon (Oregon Health Plan) were among the states that pioneered such initiatives. Other states saw managed care mainly as a cost containment device to slow the rapid increase in Medicaid spending and/or address other issues in the delivery of services to beneficiaries. These states also shifted significant numbers of beneficiaries to managed care. Between 1991 and 1996, the percentage of all Medicaid beneficiaries who received some or all of their services through a managed care arrangement grew from 9.5 percent to 40.1 percent.1 By 2003, 59.1 percent of beneficiaries were enrolled in managed care plans.2
| Managed Care in Brief | |
| Generically, managed care involves a health care purchaser (a state on behalf of Medicaid beneficiaries or a private-sector employer on behalf of its employees) contracting with an organization to provide services to a specified group of individuals. The purchaser pays a fixed fee to the managed care organization (MCO) to furnish all the services spelled out in the contract, rather than paying the MCO for the specific services that they provide, as in a fee-for-service arrangement. This fixed fee is called a "capitation" payment and is paid for each individual enrolled in the managed health plan. Capitation payments are established prospectively and usually paid monthly to the managed care organization. MCOs may furnish contracted services directly or enter into agreements with other providers to do so. Managed care arrangements usually put the MCO at full or partial financial risk. If the costs of furnishing contractually required services exceed payments, then the MCO may have to absorb the full difference as a loss (full risk contract) or the purchaser and the organization may share the loss (partial risk). Similarly, if the MCO furnishes services for less than the amount it receives from the purchaser, it may keep the difference (full risk) or be required to share the savings with the purchaser (partial risk). The chief rationale for using managed care arrangements is the assumption that risk-based financial incentives will spur the MCO to hold down costs by negotiating lower prices with health care providers, substituting less costly for more costly services, employing effective care management, or taking other steps to lower service utilization (e.g., by supplying free flu vaccine to avoid the costs of treatment. |
Congress enacted major changes in federal Medicaid law related to managed care in the Balanced Budget Act of 1997 (BBA-97).3 In BBA-97, Congress took two important steps. One was to provide states with a method to shift Medicaid services into managed care without having to apply for waivers, provided that certain conditions are met (including, among others, that beneficiaries would have the choice of at least two service delivery arrangements).4 The second major step was to spell out stronger quality requirements and safeguards for Medicaid beneficiaries who are enrolled in managed care arrangements, particularly those with special health care needs.5 This second step ultimately resulted in CMS promulgating extensively revised Medicaid managed care regulations in 2002 and 2003.6 The main thrusts of the BBA-97 provisions were: (a) to acknowledge that managed care had become a common Medicaid service delivery model and (b) to concurrently strengthen statutory requirements governing the use of managed care arrangements. However, as will be discussed below, the BBA-97 changes did not completely eliminate the need for waivers to implement managed care models or address other state policy aims.
Medicaid mental health services were also affected by the expanded use of managed care. Again, starting in the 1990s, a number of states shifted the delivery of Medicaid mental health services to managed care arrangements. Some states contracted with private sector behavioral health companies to take over the provision of Medicaid mental health services. Elsewhere, states coupled managed-care contracting to their community mental health systems, with public and/or non-profit mental health organizations (sometimes in partnership with private sector companies) becoming managed care contractors.
Some states have shifted Medicaid mental health services to managed care through the use of a "specialty" 1915(b) Medicaid waiver program, where mental health services are delivered through specialized behavioral health organizations. Other states have included mental health services in a broader waiver program that covers both physical and mental health services, where mental health services may or may not be integrated with the provision of other health services. States vary considerably in how they have reconfigured their service delivery systems using managed care delivery models.
The rationale for the application of managed care to the delivery of mental health services is much the same as for other health services: namely, contracting for the full range of mental health services through an umbrella organization that bears economic risk will lower costs and potentially result in better coordination of care. Medicaid mental health services delivered through a managed care arrangement often span clinic/outpatient and rehabilitative services, inpatient hospitalization, individual practitioner, and case management services. The contractor is paid a fixed amount per enrollee or "member" to delivery the full scope of medically necessary services specified in its contract. The contractor has an incentive to hold down or reduce the use of inpatient and other costly services by furnishing effective community-based substitutes. Managed mental health arrangements also seek to reduce costs by relying on utilization management and prior authorization to verify the need for services and direct individuals to the most cost-effective treatment alternatives. The managed care contractor has the latitude to negotiate prices with providers and exclude higher cost providers.
Managed mental health care is designed to address issues that often arise in conventional fee-for-service delivery systems, including problems in coordinating services across multiple providers, the lack of financial incentives to deliver care cost-effectively, and the inappropriate or excessive use of costly services, including inpatient hospitalization. Managed mental health care seeks to substitute a comprehensive, integrated approach to managing service delivery in place of a more fragmented system of care.
Applying managed care to the delivery of public mental health services offers potential advantages to a state, which may include those described below:
- Because contractors receive a single capitated or case rate payment7 rather than payment for each service delivered, funds can be used to purchase the most cost-effective mix of services and supports. Managed care funding mechanisms create incentives to shift hospital dollars to community services. In addition, managed care contracting may allow for the delivery of alternative services (e.g., supported employment);
- Through contracting, a state may be able to make service delivery system changes that would be more difficult to accomplish in a conventional fee-for-service system. Such changes can include adopting standardized treatment protocols, advancing the use of evidence-based practices, or promoting peer-delivered services.
- Consumers can access the full range of services through a single point-of-entry organization, potentially improving access;
- A managed care arrangement offers opportunities to integrate the delivery of mental health and substance abuse services;
- Managed care features comprehensive care and utilization management, something that a state agency may be unable to implement on its own; and,
- A state's expenditures for Medicaid mental health services can be more stable and predictable when capitated payments are employed.
At the same time, operating a managed care delivery system can pose significant challenges. Converting to managed care is a major system change and, thus, daunting in its own right. Some of the major challenges that may arise include:
- The economic framework of managed care may create incentives to under-serve individuals, particularly those with serious mental illnesses;
- Consumers, providers and advocates may resist the conversion to managed care;
- Managed care systems sometimes have relatively high administrative costs that may divert dollars from direct consumer services;
- Generally speaking, cost savings stemming from more tightly managing hospital costs are realized during the initial stages of managed care implementation. In other words, the initiation of managed care tends to yield near-term savings. Over time, costs stabilize and additional savings are more difficult to achieve;
- Where a managed care contract includes only Medicaid funds, the danger arises of splitting a state's service delivery system, wherein the Medicaid and non-Medicaid systems may operate quite differently, even for individuals with similar needs; and,
- Finally, in order to realize the potential benefits of managed care while ensuring that individuals receive necessary and high quality services, a state must have the knowledge and expertise to "manage managed care." To form a positive relationship with a managed care contractor, states must strike the right balance between contracting out services and retaining ultimate responsibility for their delivery. Managed care contracting and contractor oversight can be challenging, as many states have discovered.
The experience with managed care service delivery models in public-sector mental health services has been mixed. In some cases, there have been major problems and states have had to either terminate the use of managed care or substantially restructure their approach. In some instances, the private behavioral health companies that states selected as the managed care contractor lacked sufficient expertise to serve public sector consumers, especially individuals with serious mental illnesses.8
However, other states have had positive experiences in using managed care to deliver Medicaid mental health services. In these states, managed care has been in place for several years and appears to have yielded positive results (e.g., improved access and service quality for individuals with mental illnesses.) Over time, states have become more expert in managing managed care. Private sector behavioral health organizations also have become more skillful in serving public sector consumers, and public sector mental health agencies have acquired the expertise needed to assume the managed care organization role.
Shifting to managed care entails a major restructuring of the organization and financing of services. Adopting managed care may yield positive results -- including more efficient delivery of services, better access to services and positive outcomes for consumers -- but such results are achieved only when the transition to managed care is carefully planned and implemented. The distilled experience with managed mental health services points to the importance of a state's having a clear concept of how managed care will advance its overarching system goals and objectives. Employing managed care effectively requires expertise in crafting contracts with managed care organizations and a commitment to monitor their performance.
| The expansion of managed care to people on Medicaid who have a significant disability due to serious mental illness has been controversial - both reviled as a system of unreasonable rationing that hurts those most in need, and held up as the solution to a series of long-standing and difficult problems in public mental health systems. According to state officials with several years' experience, neither of these assessments … is accurate. Many states that have already adopted managed care approaches in their public mental health systems report considerable success, but they also warn of limits on the extent to which reform can be accomplished by changing organizational structures and financing.9 |
Today, approximately fifteen states operate distinct Medicaid managed care delivery systems that serve working age adults with serious mental illnesses along with other Medicaid beneficiaries who require mental health services.10 These individuals are served through specialty "behavioral health" 1915(b) waiver programs or "carved out" managed care arrangements that are part of 1115 Demonstration waiver programs. In some cases, managed care delivery systems operate only in some parts of a state rather than statewide. In recent years, there has been less activity on the part of states to shift the provision of mental health services to managed care.
Rather than operate a managed care delivery system, some states have implemented hybrid arrangements that incorporate some functions (e.g., utilization review and management) that are often identified with managed care models, but keep the state in the position of managing services directly. For example, some states maintain fee-for-service delivery systems but have engaged private sector firms or organizations (called Administrative Services Organizations or ASOs) to conduct these functions or have assumed these functions themselves. As discussed in Chapter 4, for example, Georgia decided to contract with a private sector ASO to conduct utilization review and management activities for its expanded rehabilitative services. Nebraska also employs an ASO, as do several other states. Utilization review is a basic Medicaid administrative function, and contracting with an ASO can aid a state in acquiring the necessary expertise to conduct this function. Employing an ASO arrangement does not require a Medicaid waiver.
Other features and functions usually attributed to managed care models can also be incorporated into fee-for-service systems without a Medicaid waiver. These include: (1) service planning requirements structured to ensure the coordinated provision of the full range of mental health services, (2) targeted case management to coordinate services, (3) prior authorization mechanisms to assure that services match consumer needs, and (4) the establishment of well-defined medical necessity criteria.
There is a misperception that a state must shift to managed care in order to limit providers to only those that are highly qualified. Medicaid law does dictate that, absent a waiver, a state must enter into a provider agreement with all qualified providers. In some cases, this provision has posed difficulties for states that want to avoid contracting with low quality vendors. But, as previously stated, under current Medicaid law, states may establish standards to ensure that only capable providers/ vendors furnish services. Shifting to a managed care service delivery system is not necessary to secure this result. However, it is worth noting that limiting the number of providers has not been a central feature of managed behavioral health programs. Indeed, state contractual requirements typically encourage managed care organizations to expand provider networks to include non-traditional providers and minority provider organizations.11
In sum, managed care is an alternative way to furnish Medicaid mental health services. Federal policy permits a state to shift the service delivery to managed care by securing a waiver. However, some features of managed care also may be implemented in fee-for-service systems.
Medicaid Waivers and Managed Care
The BBA-97 gave states an avenue to implement managed care without having to obtain federal waivers, but requires that beneficiaries have a choice of two health plans. Some state officials perceive this as an obstacle to a state's operating a unified mental health service delivery system. Consequently, managed behavioral health services most commonly continue to be furnished under waivers since services are furnished through single specialty mental health organizations.12 Waivers also continue to be necessary in order for a state to expand Medicaid eligibility to cover persons who do not meet usual Medicaid financial and categorical eligibility criteria.13
While the use of managed care in the delivery of Medicaid services has been associated very closely with obtaining waivers, a waiver is only necessary when a state wishes to mandate the enrollment of individuals to a managed care plan or otherwise limit providers. Managed care service delivery models may be employed without a waiver so long as beneficiaries may opt in or out of the arrangement.14
The following two sections describe the two applicable federal waiver authorities that states have used to implement managed mental health services. These waiver authorities differ in significant ways. When reviewing the sections on 1915(b) and 1115 waivers, it is important to keep in mind some fundamental provisions governing their use. In particular:
- The use of a waiver authority does not override the state's obligation to ensure that beneficiaries receive the services covered in its Medicaid state plan. The use of a waiver authority permits a state to implement an alternative service delivery method. Employing a waiver authority to implement managed care does not nullify the underlying coverage of services contained in the state plan; instead, it affects how they are delivered and reimbursed. Under a waiver authority, a state may elect to furnish additional services over and above those contained in the state plan.
- Operating services under a waiver authority can be administratively burdensome for a state because of the extensive Medicaid managed care requirements. In addition, meeting federal financial tests also can be a major challenge.
- Except in the case of 1115 demonstration waiver programs, the use of a waiver authority does not permit a state to modify Medicaid eligibility rules. When employed as an alternative to conventional Medicaid fee-for-service delivery ar-rangements, neither the 1915(b) nor 1115 demon-stration waiver authorities permit a state to im-pose limitations on how many beneficiaries may receive services.15
- Regardless of the type of waiver authority employed, state contracts with managed care organizations must meet basic federal requirements. Moreover, states must oversee the quality of services furnished through managed care arrangements, as required by federal regulations.
In sum, many basic Medicaid requirements continue to apply. Indeed, in many respects, states must meet more stringent and varied requirements to operate 1915(b) and 1115 waiver programs than when services are furnished under conventional fee-for-service arrangements.
Section 1915(c) Waiver Authority
Section 1915(b) of the Social Security Act permits the Secretary of HHS to grant waivers of certain specific provisions of the Medicaid Act. Waivers granted under this section are sometimes called "freedom of choice" waivers because they permit a state to limit the providers of Medicaid services and require that beneficiaries obtain services through a managed care arrangement. Section 1915(b) contains four distinct authorities:
- §1915(b)(1) permits a state to mandate that beneficiaries enroll in a managed care plan.
- §1915(b)(2) authorizes a state to establish a "central broker" to assist beneficiaries to select among health plans.16
- §1915(b)(3) provides that a state may employ savings derived from managed care to furnish additional services to beneficiaries over and above those in its state plan.17 These services must be furnished for medical or health-related reasons. It is important to note that the additional services furnished under this provision do not permit a state to secure additional federal Medicaid funding because such services must be financed out of savings.18
- §1915(b)(4) permits a state to limit the number of service providers, including engaging in "selective contracting" with preferred providers.
In the mental health arena, states usually combine the §1915(b)(1) and §1915(b)(4) authorities to implement a managed care arrangement. Several states have also used the §1915(b)(3) authority to broaden the array of services available to enrollees.19
A 1915(b) waiver program must also meet a "cost-effectiveness" test. A state must be able to show that the average per beneficiary costs of services furnished under the waiver program are no greater than under a fee-for-service arrangement. A 1915(b) waiver program may be approved for an initial period of two years and renewed for two-year periods thereafter, provided that CMS deems the state's performance in operating its program has been satisfactory.
Under §1915(b), the specific provisions of Medicaid law for which a state may request waivers in order to operate a managed care arrangement include:
- §1902(a)(1) -- Statewideness. A waiver of this provision permits a state to operate its 1915(b) waiver program in some but not all parts of a state. For example, Utah's 1915(b) mental health waiver program operates under such a waiver. Beneficiaries who reside in very rural areas of Utah receive mental health services through alternative service delivery arrangements.
- §1902(a)(4) -- A waiver of this provision permits a state to mandate that beneficiaries enroll with a single managed care organization;
- §1902(a)(10)(B) -- Comparability. When some but not all Medicaid beneficiaries are served through the managed care arrangement, a waiver of this provision is necessary. This waiver is also necessary when the services people receive through a managed care arrangement differ from the services available to non-enrollees (e.g., when a state provides additional services by invoking the §1915(b)(3) savings provision); and,
- §1902(a)(23) -- Free Choice of Provider. A waiver of this provision permits a state to mandate that individuals obtain services through the managed care organization's provider network.
When requesting a 1915(b) waiver, a state also may request waivers of other provisions of the Social Security Act; however, such waivers are infrequently granted.
In order to secure a 1915(b) waiver, a state must submit a detailed waiver application to CMS. The requirements that a state must satisfy in order to operate a 1915(b) waiver program are far more extensive than states must meet in order to add a coverage to their Medicaid state plan. There are also greater ongoing administrative requirements once a program is implemented. States must address a wide range of topics, including:
- The state plan services that would be furnished through the managed care arrangement and, as appropriate, the additional services that would be furnished under the provisions of §1915(b)(3). For illustration, Michigan's 1915(b)(3) waiver services are described on the following page.
- How the state would assure enrollee access to services and sufficient service providers.
- The state's definition of medical necessity. This definition is important as it contains the conditions under which services will be furnished to enrollees, thereby determining when the managed care contractor is obligated to furnish or arrange for services. Colorado's 1915(b) waiver illustrates a medical necessity definition.
- The groups of Medicaid beneficiaries who would be required to obtain services through the managed care arrangement and, as appropriate, beneficiaries who would be excluded (e.g., nursing facility residents or Medicaid-Medicare dual eligibles) and, thereby, continue to receive state plan services on a fee-for-service basis.
- The type of delivery system that a state would operate (e.g., the number and types of organizations with which it would contract and the extent to which they will bear financial risk).20
| Colorado's Medical Necessity Definition21 | |
"A covered service shall be deemed medically or clinically necessary if, in a manner in accordance with professionally accepted clinical guidelines and standards of practice in behavioral health care, the service:
The authorization process shall take into consideration other factors, such as the need for services and supports to assist a consumer to gain new skills or regain lost skills that support or maintain functioning and promote recovery. The contractor shall not deny services based on medical or clinical necessity solely because the consumer has a poor prognosis or has not shown improvement, if the covered services are necessary to prevent regression or maintain the present condition." |
| Michigan's 1915(b)(3) Services22 | |
Michigan's waiver program provides for the following "alternative services and supports" that its contractors may authorize for adults with mental illnesses from their capitated payments. These alternative services extend the range of services and supports available to individuals beyond those spelled out in Michigan's state Medicaid plan.
|
- How the state would implement the safeguards and other protections spelled out in the CMS managed care regulations, including (a) appeal, grievance and fair hearing procedures, and (b) furnishing information to enrollees, including information about their rights;
- The state's quality assurance and program improvement (QAPI) plan. This plan must address how the state intends to measure performance under the managed care arrangement and where it intends to devote attention to improve performance. In addition, effective August 2003, all waiver programs must provide for an external quality review system;23
- The demonstration of the program's cost effectiveness by comparing the projected costs of furnishing services without the waiver to the costs of furnishing services through the managed care arrangement. These projections must be actuarially sound and based on actual utilization and expenditure information during prior periods, as well as administrative costs. In the case of 1915(b) waiver programs, cost-effectiveness is calculated on a per beneficiary basis. States are not financially at risk for expenditure increases that stem from growth in the number of beneficiaries. They are at risk if per beneficiary costs exceed approved levels.
- When capitated payments are made to managed care organizations, a state must also spell out how it will capture "encounter data" in order to compile information about the services actually furnished to beneficiaries.24
With respect to the 1915(b) waiver authority (as well as the 1115 authority), it is important to point out that states generally must bid and periodically re-bid contracts for managed care providers. This competitive bidding requirement arises from 45 C.F.R. Part 74 rather than the Medicaid Act itself. States meet this requirement by issuing a Request for Proposal (RFP) that requires bidders to provide detailed information concerning the organization's capabilities and willingness to abide by the state's performance and other requirements.25 It is standard practice to incorporate the successful bidder's response into its contract with the organization. In almost all cases, CMS must review and approve contracts with managed care organizations. Managed behavioral health care contracts usually cover multi-year periods (3-5 years).26
Characteristics of 1915(b) Managed Behavioral Health Waiver Programs
Several states have used the 1915(b) waiver authority to restructure the delivery of mental health services. The table in Appendix C summarizes the features of eleven states' "specialty" mental health/ behavioral health 1915(b) waiver programs that include working-age adults with serious mental illnesses in the population served by the program.27 As can be seen from the table:
- Most of these programs operate on a statewide or nearly statewide basis;
- California's 1915(b) waiver program is a §1915(b)(4) "selective contracting" waiver program. It is designed to align contracting for services with the organizational structure of the state's mental health system. In particular, the state contracts with a mental health plan in each county that directly furnishes Medicaid services, or subcontracts for their provision from other providers. Medicaid beneficiaries must obtain mental health services through the county plan. The program does not provide for capitated payments nor are the county plans classified as managed care organizations.
- All these programs furnish services to both children and adults; some exclude certain groups of Medicaid beneficiaries (e.g., nursing facility residents, medically needy beneficiaries, Medicare-Medicaid dual eligibles).
- Five programs include substance abuse services;
- Prescription drugs are not covered by these programs; they are furnished to beneficiaries under standard Medicaid fee-for-service arrangements or by a "physical health" MCO if the beneficiary is served by such an organization and the organization is responsible contractually to provide prescribed drugs.28
- Only one program (New Mexico) contracts with health services managed care organizations that, in turn, subcontract for the provisions of mental health services. However, the state has announced that it plans to end this arrangement and contract separately for mental health services, carving them out from other Medicaid services delivered by MCOs.29 The other programs are distinct, specialized arrangements specifically designed to furnish mental health services and are not tied directly to the delivery of other health services.
- Most states contract with public mental health agencies, some of whom partner with private behavioral health organizations to serve as managed care organizations. Only one statewide program (Iowa) contracts exclusively with a private behavioral health organization.
- Most states use the §1915(b)(3) authority to cover additional services through savings.
Despite some commonalities, there is considerable variation across the states' programs. Colorado's30 and Iowa's31 1915(b) waiver programs are profiled on the following pages.
In addition to these specialty mental health services programs, a few states operate 1915(b) managed care waiver programs where funding for behavioral health services (usually basic inpatient and outpatient benefits) is combined with funding for other health services. In such arrangements, managed care contractors may furnish such services directly or contract with behavioral health organizations to provide services. It is not typical for states to include rehabilitative services for persons with serious mental illnesses in general purpose managed care contracts and persons with serious mental illnesses in these states continue to receive these services on a fee-for-service basis.32
Section 1115 Waiver Authority
Section 1115(a) of the Social Security Act permits the Secretary of Health and Human Services to authorize experimental, pilot, or demonstration projects that, in the judgment of the Secretary, are likely to assist in promoting the objectives of the Act, including those of the Medicaid statute.33 The authority's principal purpose is to foster the testing and researching of innovative new approaches to the provision of services and benefits under the Social Security Act. In particular, this provision allows the Secretary to waive any of the requirements of §1902 of the Medicaid Act as are necessary to permit the state to carry out its proposed project. §1902 contains the fundamental federal statutory provisions that govern the Medicaid program.
Under the 1115 Demonstration waiver authority, the Secretary may permit a state to offer services under Medicaid that are not otherwise eligible for FFP and to expand eligibility to persons who would not otherwise be eligible for the Medicaid program. HHS also has employed the 1115 Demonstration authority to test new approaches to the delivery of Medicaid services in partnership with interested states.34 When a state furnishes services under this authority, it must propose a research program and agree to conduct an evaluation of the project. Projects authorized under this authority generally are approved for a five-year period and may be extended under certain circumstances. Demonstration projects must be budget neutral over their life. This means that the expected total cost of the demonstration to the federal government cannot exceed the total cost without the waiver.35 This financial test can be challenging to meet. Also, when mental health services are furnished through a managed care arrangement under an 1115 waiver, the state also must meet the requirements of BBA-97.
| Colorado Medicaid Mental Health Capitation and Managed Care Program | |
| This program was launched in 1995 and extended statewide in 1998. Through this program, the state contracts with eight single point-of-entry "mental health assessment and services agencies" (MHASAs) serving designated regions. Services furnished include inpatient hospital, case management, outpatient clinic services, and rehabilitative services. Prior to this program, Medicaid mental health services were delivered through a fee-for service system which had "no central gatekeeper determining the need for services and no single clinician or case manager coordinating all aspects of an individual's mental health care." In 2000, the state modified its program to place a stronger emphasis on recovery as the program's central aim. MHASAs are community mental health centers, consortia or partnerships of centers, which may also partner with a pri-vate sector behavioral health company that functions as an Administrative Services Organization. MHASAs are responsible for assessing service need and coordinating service delivery (by providing services directly or referring individuals to subcontracted providers) and monitoring service delivery. Under this program, capitated payments are made to each MHASA. Colorado limits MHASA administrative costs and profit. The program is administered by the Colorado Division of Mental Health in the Department of Human Services under an interagency agreement with the Department of Health Care Policy and Finance, the state's Medicaid agency. The program's goals are:
Colorado has used the §1915(b)(3) "savings" provision to cover additional services not offered under the state plan, including (for adults) intensive case management, residential services, and vocational services to assist persons to gain skills necessary to secure employment. In addition, the state expects MHASAs to develop and offer "optional services" over and above the core services included in the waiver program. Some optional services furnished by MHASAs include ACT, peer counseling and support, clubhouses, consumer-operated "warm lines," family support and education, supported living, supported employment, recovery/self-help groups, and peer-run employment services. In conjunction with this program, the state has established the Mental Health Ombuds program. This program is operated by an independent organization that provides advocacy, assistance, and education for consumers and families enrolled in the program. |
| The Iowa Plan | |
| The Iowa Plan integrates the delivery of mental health and substance abuse treatment services. Approved in 1998, the Iowa Plan replaced two separate 1915(b) mental health and substance abuse waiver programs. The plan uses a single statewide private-sector contractor (Magellan Behavioral Health). Nearly all adult and child Medicaid beneficiaries are required to obtain mental health and substance abuse services through the Iowa Plan. Services offered through this program include basic inpatient and outpatient mental health and substance abuse services. In addition, Iowa employs the §1915(b)(3) "savings" provision to add coverage of:
|
There is no pre-formatted application for states to use when seeking waivers under the 1115 authority. The process for obtaining a demonstration waiver usually starts with a state's submitting a general outline of its proposal to CMS and proceeds to the development of a formal proposal. CMS and the state then negotiate the "terms and conditions" (i.e., the specific parameters) under which the demonstration will operate. Once CMS is confident that the state is prepared to implement the demonstration, the state may proceed.
In Medicaid, a major use of the 1115 waiver authority (but not the exclusive use) has been to permit states to launch what are termed "health care reform demonstrations." Through these demonstrations, several states have substantially restructured the delivery of Medicaid services, principally by employing managed care as a means to secure cost savings that can be applied to extend health care to additional populations. Several of these demonstrations include mental health and/or substance abuse services.
Delivery of Mental Health Services Under 1115 Demonstration Projects
There are no stand-alone 1115 demonstrations that solely concern the provision of mental health services. Instead, mental health services have been included as part of broader health care reform demonstrations. About twelve states operate broad scale 1115 health care reform demonstrations.36 How mental health services are organized and financed in these demonstrations varies considerably, but they employ two basic approaches to deliver mental health services: (1) carve out mental health services but maintain fee-for-service delivery, or (2) carve out and implement a managed care service delivery model for mental health services. Both approaches are described below.
Carve out mental health services but maintain fee-for-service delivery. While 1115 demonstration waiver programs usually make extensive use of managed care arrangements, states may elect to exclude some Medicaid services and/or eligibility groups from the scope of such arrangements. When services are excluded from capitated managed care organizations, they are said to have been "carved out" and continue to be provided on a fee-for-service basis. Fee-for-service delivery is also employed when groups of beneficiaries (e.g., SSI recipients) are excluded from mandatory enrollment in a managed care arrangement. Sometimes, states include a basic inpatient/outpatient mental health benefit in the managed care arrangement but pay for more intensive services on a fee-for-service basis and/or continue to serve some populations (e.g., individuals with serious mental illnesses) through a traditional fee-for-service model. Where mental health services have been carved out and are furnished outside the managed care delivery system, a state may still restructure its provision of mental health services, taking advantage of the flexibility afforded in a demonstration waiver. Several states that operate 1115 demonstrations have carved out intensive mental health services for working-age adults with serious mental illnesses. Maryland and Vermont (profiled below) are two states that operate health care reform demonstrations but continue to provide mental health services on a fee-for service or other basis.39
| Section 1115 Carved Out Fee-For-Service Arrangements | |
| Maryland Maryland's HealthChoice 1115 Demonstration waiver was implemented in 1997. Medicaid beneficiaries must enroll to receive health care services through a comprehensive health care benefits MCO. These MCOs are responsible for furnishing "primary" outpatient mental health and substance abuse services. Carved out from MCO delivery are more intensive "specialty mental health services." These services are furnished through the Public Mental Health System (PMHS) administered by Maryland's Mental Hygiene Administration in the Department of Health and Mental Hygiene. Maryland's network of Core Service Agencies (CSAs) are responsible for planning, managing, and monitoring the delivery of publicly-funded mental health services at the local level. CSAs, in turn, contract with mental health providers to furnish services on a fee-for-service basis. Maryland has engaged an ASO (Maryland Health Partners) to provide support to the state and the CSAs. The ASO determines whether a person qualifies for PMHS services, refers the person to providers, pre-authorizes non-emergency services, conducts utilization review, compiles data, and processes claims and remits payments to providers. The PMHS serves both Medicaid eligible and non-eligible individuals who meet the state's eligibility criteria for mental health services. Vermont37 In 1996, Vermont implemented the Vermont Health Access Plan (VHAP), its 1115 health care reform demonstration. Through VHAP, the state has expanded Medicaid eligibility for both children and adults. VHAP uses a primary care case management service delivery model rather than an MCO service delivery model.38 Under VHAP, basic mental health benefits are furnished on a fee-for-service basis. The state also operates its long-term behavioral health program (Community Rehabilitation and Treatment (CRT) Program) under the demonstration. The CRT Program serves approximately 3,300 adults with severe and persistent mental illnesses, of whom about 88 percent are Medicaid beneficiaries. Due to the nature of their mental illnesses, CRT consumers have varying needs for services over the long-term. Core CRT services include:
State officials have found several advantages in delivering services under an 1115 demonstration waiver. A relatively high percentage of adults with serious mental illnesses qualify for Medicaid funding. The adoption of the case rate payment method has simplified administrative procedures for providers because they do not need to submit fee-for-service claims or keep track of encounter data. The waiver has also given providers more flexibility to furnish the most appropriate services rather than being confined to the traditional Medicaid services menu. In Vermont, the use of day treatment has declined substantially as a result of this flexibility. About 28 percent of CRT consumers are employed in the community, a rate significantly above the national average. This flexibility has also aided in the adoption of evidence-based practices, most of which are used in varying degrees by designated agencies. The state is expanding the use of evidence-based practices throughout its service system. |
Carve out and implement a managed care service delivery model for mental health services. Five 1115 health care reform demonstration waiver states have elected to carve out mental health services and deliver them through a behavioral health managed care arrangement. These carve out arrangements are similar to those that other states have established through 1915(b) waiver programs. That is, the state contracts with one or more entities to furnish mental health (and sometimes substance abuse services) to beneficiaries using a capitated payment arrangement. These arrangements are subject to the same federal managed care regulations as similar arrangements implemented under a 1915(b) waiver. Five states that operate behavioral health managed care arrangements under an 1115 demonstration waiver are described below.
Arizona. The Arizona Health Care Cost Containment System (AHCCCS) 1115 Demonstration has operated since 1982.40 The demonstration has three main components: (a) acute care services provided through MCOs; (b) long-term care services; and, (c) behavioral health services. Arizona phased in the coverage of behavioral health services between 1990 and 1995. The managed behavioral health carve out provides comprehensive mental health and substance abuse services to all adult and child Medicaid eligibility groups.41 The carve-out is managed by the Division of Behavioral Health Services at the Arizona Department of Health Services under an agreement with the state Medicaid agency. The division contracts with Regional Behavioral Health Authorities on a capitated basis to furnish services. Three tribal authorities furnish services to Native Americans.
Hawaii operates a small behavioral health carve-out (Behavioral Health Managed Care Plan, or BHMCP) for adults as part of its Hawaii QUEST 1115 demonstration. Individuals with a serious mental illness have the option to participate in the carve-out, but may instead elect to receive services from the standard Medicaid plan, although the waiver offers a greater array of services. BHMCP also provides services to individuals with co-occurring substance abuse disorders. Beneficiaries have access to services including crisis, residential treatment, prescription drugs, inpatient/outpatient mental health and substance abuse treatment, and mental health support services.
Massachusetts implemented a 1915(b) waiver Medicaid behavioral health managed care program in 1992. In 1997, it implemented Mass Health, a statewide 1115 health care reform demonstration waiver. When Mass Health was implemented, 1915(b) waiver behavioral health services were folded into it. For health services, beneficiaries select between a primary care case management (PCCM) arrangement or enroll with a comprehensive benefits managed care organization. Adult beneficiaries with serious mental illnesses usually are enrolled in a PCCM arrangement and receive mental health (and substance abuse) services through the Massachusetts Behavioral Health Partnership managed care carve out program.42 The Partnership program is operated by a private-sector behavioral health managed care organization and is responsible for furnishing the full range of inpatient and outpatient mental health and substance abuse services to enrolled members.
Oregon. The Oregon Health Plan 1115 health care reform demonstration waiver was implemented in 1994. The mental health/substance abuse carve-out managed care arrangement employs multiple types of providers (private behavioral health MCOs, CMHCs, county-operated entities, and regional authorities). The carve out program includes crisis, inpatient/outpatient mental health services, rehabilitative services, mental health support, and outpatient substance abuse services.
Tennessee. The Tenncare 1115 health care reform demonstration waiver was implemented in 1994. Since the program's inception, mental health and substance abuse services have been carved out and are now delivered by a single behavioral health managed care organization (BHO). The services furnished by the BHO include crisis, inpatient/outpatient mental health and substance abuse, rehabilitative services, mental health and substance abuse residential services, mental health support, and detoxification.
The table in Appendix C contains additional information about these managed behavioral health carve outs.
When a state operates its Medicaid program under the 1115 demonstration authority, it gains the flexibility to expand eligibility and employ alternative service delivery models. Some states that operate 1115 demonstrations have elected to continue to provide services to working-age adults with serious mental illnesses using a traditional fee-for-service delivery system. Others have used the flexibility afforded by the demonstration authority to restructure their provision of mental health services, but not all have done so by employing a managed care service delivery arrangement.
Section 1915(c) Waiver Authority
Section 1915(c) of the Social Security Act was enacted in 1981.43 It permits the Secretary of Health and Human Services to grant waivers to states so they can furnish home and community-based services (HCBS) as an alternative to institutional services for those individuals who qualify for Medicaid-reimbursable institutional services. Through the HCBS waiver program, states have substantially expanded home and community services and supports for people with disabilities of all ages. In 2002, over 800,000 individuals nationwide received services through HCBS waiver programs at a state-federal cost of $16.3 billion. Nationwide, states operate approximately 275 HCBS waiver programs. However, only a few waiver programs target services specifically to individuals with mental illnesses.
HCBS Waiver Program in Brief
The major provisions of Section 1915(c) of the Social Security Act are described below.
- States may offer home and community services to individuals who qualify for services furnished in a nursing facility, intermediate care facility for the mentally retarded,or a hospital. When a state operates an HCBS waiver program, individuals who meet the level-of-care requirements for these Medicaid institutional settings may instead be offered home and community services. Individuals must affirmatively elect to receive home and community services in lieu of institutional services.
- §1915(c) identifies several services that a state may offer through an HCBS waiver program, such as case management, personal care, habilitation, adult day health care, homemaker, home health aide and respite. States may cover additional services and supports as long as they assist individuals to avoid institutionalization. The services that a state may offer in a 1915(c) waiver program include: 1) optional services it can cover under its state plan but has chosen not to; 2) additional services that can not be offered under the state plan; and 3) services that the state offers under its state plan with limitations on amount, duration and scope, but wishes to offer on an "extended basis" to waiver participants, i.e., with less stringent limitations.
A state is barred from claiming the costs of "room and board" (e.g., housing and other routine living expenses) furnished to waiver participants. Such expenses must be met from the participants' own resources (e.g., SSI payments) or other funds. - §1915(c) permits the Secretary of Health and Human services to waive three provisions of the Social Security Act to permit a state to operate an HCBS waiver program: (a) §1902(a)(1) for the purpose of operating a program on a less than statewide basis; (b) §1902(a)(10)(B) in order to furnish waiver services to specified groups of beneficiaries (e.g., older persons, working-age adults with disabilities, persons who have experienced a traumatic brain injury); and, (c) §1902(a)(10)(C)(i)(III) to permit a state to offer waiver services to individuals who would qualify financially for Medicaid only if institutionalized. As noted in Chapter 3, state Medicaid financial eligibility standards for institutional services are often more generous than community standards.
All other provisions of the Medicaid Act apply to HCBS waiver programs. For example, §1915(c) does not authorize a waiver of beneficiary's free choice of service provider as required by §1902 (a)(23) of the Act. In order to link the provision of waiver services to a managed care strategy, a state must request a combination 1915(b)/1915(c) waiver program and meet the requirements for each.45 - §1915(c) dictates that the services provided through a waiver program be spelled out in a "plan of care." The plan of care also identifies other services and supports (paid and unpaid) that are needed to support the waiver participant in the community.
- Individuals who participate in an HCBS waiver program are eligible to receive all other services that a state offers under its Medicaid state plan. HCBS waiver services complement the services that a state offers in its state plan. Waiver services cannot be furnished to individuals who are institutionalized. However, some waiver services may be furnished to facilitate the transition of institutionalized persons to the community.46
- In order to obtain CMS approval for an HCBS waiver program, a state must demonstrate that its proposed program will be "cost-neutral." A state must show that the average per person cost of furnishing waiver and other Medicaid state plan services to individuals would not exceed the average cost of furnishing institutional and other Medicaid services to these individuals in the absence of a waiver program. The program must meet this cost-neutrality test for the duration of its operation. A state may elect to limit its program to individuals for whom the cost of community services will not exceed the cost of institutional services. Alternatively, a state may operate its program on an "aggregate" basis, balancing individuals who have higher costs with those whose costs are lower.
- In proposing to operate a waiver program, a state specifies the number of individuals it plans to serve. A state is not obligated to furnish services to additional persons once it reaches its self-imposed enrollment cap. The ability of states to limit the number of people receiving waiver services is a feature unique to this waiver authority. States may elect to serve as few or as many individuals as they chose.47
- A state must assure that it has necessary safeguards to assure the health and welfare of individuals served through the waiver program.
- There is no federal limitation on the number of waiver programs a state may operate. Some states operate as many as ten programs.
- Waivers may be granted for an initial period of three years. If a state's performance in operating a program is acceptable, then the program may be renewed thereafter for successive five-year periods.
States have employed the HCBS waiver program extensively to promote the cost-effective delivery of long-term care services to many Medicaid beneficiary target population groups. The cost of furnishing community services has been demonstrated to be considerably lower than institutional services. In addition, the program is very flexible. States have wide-ranging latitude both in selecting the populations to whom they will furnish services and in selecting the services that they will offer.
States must apply to CMS to operate an HCBS waiver program. CMS has issued a standard waiver application template that a state may employ in seeking approval to operate an HCBS waiver program.48
HCBS Waiver Program and Working Age Adults with Serious Mental Illnesses
Working-age adults with serious mental illnesses may receive services through an HCBS waiver program. Like other individuals with disabilities, such persons must meet a waiver program's applicable eligibility criteria, including the determination that the person requires the level-of-care furnished in a Medicaid-reimbursable institutional setting and that waiver services are necessary to assist the person to remain in the community. In various states, individuals with serious mental illnesses qualify for broader HCBS waiver programs for persons with disabilities, even though a state's program may not have explicitly specified that they are members of the target population.
But, there are challenges in operating an HCBS waiver program designed to serve only individuals with serious mental illnesses. The main difficulty in designing an HCBS waiver program to exclusively serve individuals with serious mental illnesses is the linkage between the operation of a waiver program and Medicaid institutional services. HCBS waiver programs operate as alternatives to Medicaid institutional services. In the case of individuals with developmental disabilities, for example, persons are eligible for waiver services if they meet ICF/MR level-of-care criteria and, thus, waiver services are furnished as an alternative to ICF/MR services.
In the case of working-age adults with serious mental illnesses, due to the IMD exclusion discussed in Chapter 4, there is no distinct Medicaid-reimbursable mental health institutional setting for which a waiver program may serve as an alternative. In contrast, because inpatient psychiatric hospital services for individuals under 21 are a reimbursable Medicaid institutional setting, crafting HCBS waiver programs for children with serious mental and emotional disorders is technically more feasible.
Although the IMD exclusion poses an obstacle to developing an HCBS waiver program for adults with serious mental illnesses, it remains possible for a state to operate an HCBS waiver program that targets such individuals. In particular, a state may (as Colorado does) operate an HCBS waiver program for individuals with serious mental illnesses who also meet the state's level of care criteria for nursing facility services.
At present, Colorado operates the only HCBS waiver program for adults with serious mental illnesses. Colorado's program is profiled on the following page. Five HCBS waiver programs specifically target services for children with serious mental and emotional disorders (in Indiana, Kansas, New York, Vermont and Wisconsin).49
| Colorado's HCBS Waiver Program for Persons with Mental Illness50 | |
| Since 1995, Colorado has operated an HCBS waiver program for adults (persons age 18 and older) who have a major mental disorder (e.g., schizophrenia, major affective disorder) and also meet nursing facility level of care criteria. This program is operated by the Department of Health Care Policy and Financing, the state's Medicaid agency. In 2000-01, this program served 1,706 individuals at an average per person cost of $5,505. Colorado's nursing facility level of care criteria are based on a functional needs assessment that evaluates a person functioning in several ADLs areas. One of the areas evaluated is the person's need for supervision that results from challenging behaviors or memory/cognition deficits. Individuals, of course, must also meet Colorado's financial eligibility standards. In the case of this (and other Colorado waiver programs), Colorado extends eligibility to individuals who have incomes up to 300 percent of the SSI federal benefit rate. Colorado offers the following services through this HCBS waiver program:
Case management services are furnished by Colorado mental health centers and organizations that hold contracts under the state's 1915(b) waiver. These services are reimbursed as a Medicaid administrative expense. Case management responsibilities include intake, case planning, coordinating waiver services with mental health services, and monitoring service provision and the person's well-being. |
State nursing facility level-of-care criteria vary considerably, but generally are based on various combinations of medical and nursing needs, as well as functional limitations. In some states, however, persons may be eligible for nursing facility services on the basis of functional limitations only. In these states, individuals with serious mental illnesses may meet a state's nursing facility level of care criteria. State mental health authorities, by virtue of the role that they play in conducting assessments of individuals for nursing facility pre-admission screening and resident review (discussed in Chapter 7), may be able to gauge the extent to which persons with serious mental illnesses might qualify for an HCBS waiver program. Those who qualify may be offered services through a waiver program limited to serving individuals with serious mental illnesses. Operating an HCBS waiver program for persons with serious mental illnesses offers some potential advantages for a state, which are listed below.
- States have the option of using Medicaid institutional financial eligibility criteria for HCBS waiver programs. Because these criteria typically are more generous than "community" financial eligibility criteria, a larger proportion of individuals may be able to qualify for Medicaid services. This will be especially true in states that employ the "special income standard" of 300 percent of the SSI federal benefit rate for institutional and HCBS waiver services (described in Chapter 3).
- There is no federal requirement that a waiver program be limited solely to current nursing facility residents transitioning to the community (although such individuals clearly may be offered services). Individuals in the community who meet nursing facility level of care criteria also may be offered waiver services, irrespective of whether they are seeking admission to a nursing facility.
- The operation of an HCBS waiver program would permit states to furnish services that cannot readily be covered under the rehabilitative services or other state plan options. Such services can include personal care/assistance and respite. The coverage of personal care/assistance may aid in promoting supported housing and employment, especially in states that do not offer personal assistance in their Medicaid programs or that impose significant restrictions on the use of such services. Operating an HCBS waiver program for adults with serious mental illnesses may provide opportunities for a state to complement the mental health services that it offers under its Medicaid state plan.
- Since HCBS waiver participants are also eligible to receive all the other services that a state offers under its state plan, a state generally would not include mental health services in its HCBS waiver program except to include services that are not offered under the state plan or when a state wishes to offer some of its state plan services on a modified basis in the HCBS waiver program.51 For example, a state may modify state plan limitations on the number of prescription drugs by providing for "extended state plan" coverage of prescription drugs in its HCBS waiver program. In states that offer personal care/assistance services under their Medicaid state plans but limitations on such services make it difficult for individuals with serious mental illnesses to utilize them, such services in modified form can be offered in an HCBS waiver program in order to overcome those limitations.
- Because HCBS waiver programs operate under state-determined participant caps, they can be less challenging to manage fiscally than state plan services. HCBS waiver programs can be sized to match the dollars available, making expenditures more predictable.
- Case management services play a central role in the operation of HCBS waiver programs. Such services include working with the participant to identify providers of services and supports, coordinating waiver services with other Medicaid and non-Medicaid services, and conducting on-going monitoring of the person's health and welfare. In states that already furnish targeted case management services to individuals with mental illnesses, HCBS waiver case management functions (such as preparing the individual's plan of care) may be conducted under the targeted case management coverage through existing providers.
The operation of an HCBS waiver program for working-age adults with serious mental illnesses may pose challenges for states. In particular:
- Because waiver services may be furnished only to individuals who meet institutional (nursing facility) level-of-care requirements, the proportion of working-age adults with serious mental illnesses who might qualify for an HCBS waiver program may be difficult to determine. Individuals whose functional limitations qualify them for Medicaid mental health services may not meet waiver eligibility criteria. Creating two categories of eligibility for Medicaid services (waiver criteria and mental health system criteria) could fragment the state's mental health system.
- A state might have difficulty securing matching funds to operate an HCBS waiver program, especially if the program would offer services and supports not currently furnished.
- Meeting HCBS waiver cost-effectiveness requirements might be another challenge. In the case of an HCBS waiver program that would target individuals with serious mental illnesses, the costs of waiver services plus other state plan services (e.g., prescription drugs and rehabilitative services) could not exceed the costs of nursing facility plus state plan services. Depending on a state's nursing facility payment levels, the target population for the waiver program, and the services offered in the waiver program, meeting the HCBS waiver cost-effectiveness requirement might be difficult.
- To some extent, the advantages of operating an HCBS waiver program for individuals with serious mental illnesses might also be realized through the operation of a managed care waiver program, especially one that provides for the coverage of additional services under the §1915 (b)(3) savings provision or one that operates under the §1115 waiver authority. However, as previously noted, a state cannot expand eligibility when it operates a 1915(b) waiver. Such expansion would potentially be permitted if a 1915(c) waiver is operated in states where institutional financial eligibility criteria are more generous than community criteria. A 1915(c) waiver may operate side-by-side with a 1915(b) waiver program. In such a case, individuals who gain Medicaid eligibility by virtue of their participation in the 1915(c) waiver program would receive their specialized mental health services through the 1915(b) waiver program.
Conclusion
The most common use of the Medicaid waiver authorities in mental health services has been to permit states to implement managed behavioral health service delivery systems. In a few states where 1115 demonstration waiver programs are operated, states have used the broader flexibility afforded in such waivers to restructure the delivery of services to individuals with serious mental illnesses but not to implement managed care delivery models.
Annotated Bibliography
Bazelon Center for Mental Health Law and Milbank Memorial Fund (2000). Effective Public Management of Mental Health Care: Views from States on Medicaid Reforms That Enhance Service Integration and Accountability. New York: Milbank Memorial Fund. Available at milbank.org/bazelon/
This report distills the experiences of senior state and local government officials in adapting managed care techniques to meet the needs of persons with mental illnesses, especially severe and chronic illnesses. The report provides especially balanced perspectives concerning the application of managed care to mental health services, including its potential positive contributions and drawbacks. The report also identifies how managed care techniques can be employed in mental health services while stopping short of a state's contracting services out to a behavioral health organization.
U.S. General Accounting Office (1999). Medicaid Managed Care: Four States' Experiences with Mental Health Carve Out Programs. Washington, D.C. GAO Report: GAO/HEHS-99-118
This report examined the Colorado, Iowa, Massachusetts and Washington Medicaid mental health carve out programs. The report provides useful information concerning operational issues in such programs.
Forquer, S.L, and Sabin, J.E. (2002). Medicaid Behavioral Managed Care: What Lies Ahead. Princeton, NJ: Center for Health Care Strategies, Inc. Available at chcs.org/usr_doc/bhforecasting.pdf
This Working Paper summarizes interviews with 33 national experts on managed behavioral health care, outlining lessons learned from the last decade of managed care and offering predictions for the future. The Center for Health Care Strategies has conducted extensive examinations of Medicaid managed care delivery systems.
Savela, T., Robinson, G. and Crow, S. (2000). Contracting for Public Mental Health Services: Opinions of Managed Behavioral Health Care Organizations. (DHHS Publication No. [SMA] 00-3438). Rockville, MD: Center for Mental Health Services, Substance Abuse and Mental Health Services Administration. Available at mentalhealth.org/publications/allpubs/SMA00-3438/default.asp#toc
This publication distills the experiences and recommendations of private sector behavior health organizations concerning Medicaid managed care carve outs for behavioral health services.
Web Resources
Medicaid Managed Care and Waivers
CMS provides extensive information on Medicaid managed care at cms.hhs.gov/medicaid/managedcare/default.asp
Information about the waiver authorities employed to implement managed care arrangements is at cms.hhs.gov/medicaid/waivers/
Information concerning the waiver programs each state operates is at cms.hhs.gov/medicaid/waivers/waivermap.asp
CMS makes extensive information concerning the 1915(c) HCBS waiver program available at cms.hhs.gov/medicaid/1915c/default.asp
Many states provide fact sheets describing the program. In some cases, the state's entire waiver application and related documents are available.
Center for Health Services Research and Policy at George Washington University has compiled extensive information concerning state Medicaid managed care contracting. A portion of its web site is devoted to topics related to behavioral health, at gwhealthpolicy.org/behavioral.html
Endnotes
-
CMS Medicaid Managed Care Enrollment Report at cms.hhs.gov/medicaid/managedcare/mmcss03.asp
-
Ibid.
-
P.L. 105-33. The Medicaid Act has long provided that states could contract with HMOs and other managed care entities to furnish services to beneficiaries. States did not have to request waivers for these types of arrangements so long as beneficiaries could freely elect to receive services from such entities. §1915(b) was added to the Act in 1981 (P.L. 97-35) and allowed the Secretary to grant waivers to permit states to mandate that beneficiaries receive their services through a managed care arrangement. The extensive use of the §1115 waiver authority to mandate the enrollment of beneficiaries into managed care arrangements started in the early 1990s.
-
These provisions are contained in §1932(a) of the Social Security Act. A state may satisfy the requirements concerning beneficiary choice by contracting with two or more managed care organizations and/or contracting with one such organization but offering beneficiaries the alternative of selecting a primary care case manager (PCCM). PCCM services may be covered under the provisions of §1905(t) of Act.
Under a PCCM arrangement, each beneficiary must select a primary care physician or other health professional to manage his or her care. The underlying rationale for PCCM arrangements is to make sure that beneficiaries have a primary care "medical home." The goal is to reduce emergency room utilization and avoid over-utilization of services. PCCMs are usually paid a monthly stipend for each beneficiary on their caseload. PCCMs are not financially at risk and beneficiaries receive services through traditional fee-for-service arrangements. Prior to BBA-97, states had to request 1915(b) waivers in order to implement a PCCM arrangement.
§1932(a) prohibits a state from mandating the managed care enrollment of certain children (including children who receive SSI) and Medicare/ Medicaid dual beneficiaries. So far, relatively few states have employed this authority to implement system-wide managed care. Most states continue to employ waiver authorities to mandate the enrollment of beneficiaries into a managed care arrangement. One reason is that §1932(a) does not provide an avenue for states to expand Medicaid eligibility, which may only be accomplished through the 1115 demonstration waiver authority.
-
The safeguards are contained in §1932(b) of the Act and concern: (a) assuring coverage of emergency services; (b) protection of enrollee-provider communications; (c) grievance procedures; (d) assurances that managed care organizations have adequate capacity and offer sufficient services; (e) anti-discrimination; and, (f) others. Provisions concerning quality assurance standards are in §1932(c) of the Act and dictate that a state develop and implement a "quality assessment and improvement strategy" for services furnished through managed care arrangements that address access standards and monitoring procedures.
States are also required to arrange for an annual external independent review of the operation of the managed care program. §1932(d) contains provisions concerning fraud and abuse; §1932(e) authorizes states to sanction poorly performing managed care organizations; and, §1932(f) establishes standards for timely payment by managed care organizations to providers. In general, the provisions of §1932(b) -- (f) apply to all Medicaid managed care arrangements, not just those that operate under the provisions of §1932(a).
-
Located in 42 CFR 438.
-
A "case rate" is an amount paid for each individual who actually receives services. Case rates differ from "capitation rates" which are paid for each enrollee, regardless of whether an enrollee utilizes services.
-
In the private sector, it is relatively commonplace for purchasers to use private-sector companies to manage inpatient/outpatient mental health and substance abuse benefits (included in Employee Assistance Programs), or alternatively, for managed health plans to sub-contract with such organizations to furnish mental health services. However, the experience of these companies did not equip them with the expertise to serve individuals with serious mental illnesses, who make up a significant proportion of adult Medicaid beneficiaries. When some of these companies entered the public-sector managed mental heath services arena, problems arose because they lacked the necessary expertise. The companies that have survived are those that improved their capability to manage public sector services.
-
Bazelon Center for Mental Health Law and Milbank Memorial Fund (2000). Effective Public Management of Mental Health Care: Views from States on Medicaid Reforms That Enhance Service Integration and Accountability. New York: Milbank Memorial Fund. Available at milbank.org/bazelon/
-
A greater number of states furnish mental health services through managed care arrangements. However, in many cases, these states exclude SSI recipients from mandatory enrollment in a managed care plan and/or include only basic inpatient and outpatient mental health services in the scope of benefits provided through the managed care plan.
-
This practice recognizes that the public sector mental health marketplace is different than the physical health market place. The problem often is that there are too few rather than too many providers.
-
At the time this report was prepared, 12 states were furnishing Medicaid services under the provisions of §1932(a). In almost all instances, these states excluded SSI recipients from mandatory enrollment or excluded mental health services from the scope of services furnished through arrangements permitted under §1932(a). The §1932(a) authority most typically was employed in furnishing services to TANF and TANF-related groups. State-by-state information concerning the use of the §1932(a) authority is at cms.hhs.gov/medicaid/1932a/default.asp.
-
The BBA-97 provisions did not provide a mechanism for states to expand eligibility to include the uninsured.
-
There are many examples of states that contract with managed care organizations for the provision of Medicaid services but give beneficiaries the option of obtaining services on a fee-for-service basis instead. One example is the ICare program in Wisconsin where individuals with disabilities may voluntarily elect to obtain services through a managed care entity.
-
In some cases, limited-purpose demonstration waiver programs may limit the number of beneficiaries who can participate in the demonstration. In health reform demon-strations, states may limit the number of uninsured individuals who are served but not Medicaid beneficiaries.
-
A central broker is employed to provide information to beneficiaries about their choices of managed care arrangements. Brokers are most commonly employed in conjunction with managed health plans.
-
All savings must be devoted to enhancing services for Medicaid beneficiaries. In the past, states could use savings to underwrite services for non-Medicaid eligible individuals. This is no longer allowed.
-
A state may also require contractors to identify additional services that they will furnish out of savings they realize in serving beneficiaries. However, the provision of these additional services is an obligation of the contractor rather than the state. Services that a state adds under the provisions of §1915(b)(3) must be available to all enrolled ben-eficiaries.
-
In the past, states had the latitude to redirect savings to underwrite services for non-Medicaid eligible individuals. This is no longer the case. States must apply savings to furnish additional services to Medicaid beneficiaries or apply savings in a fashion that will benefit beneficiaries (e.g., by establishing a community reinvestment fund). In addition, previously some states were permitted to redeploy savings under the provisions of §1915(a) of the Act rather than identify the additional uses under §1915(b)(3). This practice also has been terminated.
-
BBA-97 resulted in the creation of new classifications of managed care organizations (MCOs). Organizations that furnish managed mental health services usually are classified as Prepaid Inpatient Health Plans (PIHPs). A PIHP furnishes a limited range of Medicaid services. When a behavioral health organization's contract includes inpatient hospital services, it is classified as a PIHP. Organizations that furnish a fuller range of health services are classified as MCOs. Organizations that furnish a limited range of services and are not responsible for inpatient hospital services are classified as Prepaid Ambulatory Health Plans or PAHPs.
-
Colorado Departments of Health Care Policy and Financing and Human Services (2003). Medicaid Mental Health Capitation and Managed Care Program: Proposal for Section 1915(b) Capitated Waiver Program Renewal.
-
Michigan Department of Community Health, 1915(b) Renewal Application (September 2003).
-
CMS rules concerning external quality review are located at 42 CFR 438.300 and were promulgated in final form in January 24, 2003 Code of Federal Regulations. The CFR materials are available at cms.hhs.gov/medicaid/managedcare/eqr12403.pdf
CMS has also released protocols to guide external quality review. These protocols are located at cms.hhs.gov/medicaid/managedcare/mceqrhmp.asp
In addition, states are expected to identify and conduct quality improvement projects for the duration of the waiver program.
-
Encounter data include services actually furnished to beneficiaries. Encounter data serve as a substitute for detailed information derived from Medicaid claims in a fee-for-service system.
-
The October 2003 RFP soliciting a contractor for the Iowa Plan (a behavioral health specialty managed care plan) was 450 pages.
-
These relatively long contract periods recognize that a contractor incurs considerable costs in establishing its operations and, thereby, need an extended period to recover such costs. In addition, changing contractors frequently can be disruptive to client-provider relationships. Issues surrounding the procurement and re-procurement of contractors to furnish managed behavioral health services are discussed in: Richard H. Dougherty (2003). Informed Purchasing Series Resource Paper. Re-procurement: The Role of Competition in Changing Public Managed Behavioral Health Systems. Princeton NJ: Center for Health Care Strategies
-
The table does not include 1915(b) waiver programs that furnish a limited range of outpatient and inpatient services.
-
In general, only a few states include prescription drugs in the scope of services contracted through managed care organizations of any type. However, in evaluating the cost effectiveness of a managed behavioral health program, CMS requires that states take into account prescription drug costs because such costs may be affected by the practices of managed behavioral health programs.
-
Hyde, Pamela. (2004). State Mental Health Policy: A unique approach to designing a comprehensive behavioral health system in New Mexico. New York: American Psychiatric Assocation. New Mexico is undertaking a broad restructuring of its mental health system. Restructuring the delivery of Medicaid mental health services is one element of this restructuring. Additional is available at state.nm.us/hsd/bhdwg/index.htm
-
The material in this section is based on Colorado's 2003-2005 1915(b) waiver renewal application and its 2000 RFP to solicit agencies to serve as contractors. Both documents are located at cdhs.state.co.us/ohr/mhs/Medicaid%20Program%20Folder/Index.htm. Also located at the same address are responses to this RFP submitted by MHASAs, as well as other materials. Additional information concerning Colorado's mental health service delivery system is located at cdhs.state.co.us/ohr/mhs/
-
The material in this section is based on Iowa's May 2003 waiver renewal application and the state's October 2003 Request for Proposal to solicit bids for a contractor to operate the Iowa Plan.
-
For example, the District of Columbia includes mental health benefits in the scope of its 1915(b) DC Managed Care waiver program. These basic benefits are managed by a private-sector behavioral health company. Medicaid mental health rehabilitative services, however, have been excluded from this program and are managed by the District of Columbia Department of Mental Health. Individuals with serious mental illnesses who qualify for and would benefit from rehabilitative services are referred by the behavioral health company and other provider agencies to receive rehabilitative services, which are reimbursed on a fee-for-service basis.
-
This authority also extends to other specified parts of the Social Security Act, including Title XVI.
-
For example, HHS, the Robert Wood Johnson Foundation and three states (AR, FL, NJ) collaborated in a demonstration of consumer-directed Medicaid services. The 1115 authority was used to permit the states to implement "cash and counseling" demonstrations. The CMS New Freedom Independence Plus initiative is an outgrowth of this demonstration project.
-
In 2001, CMS announced the Health Insurance Flexibility and Accountability (HIFA) Demonstration Initiative. This initiative encourages states to seek waivers of provisions of Titles XIX and XXI (the State Children's Health Insurance Program (SCHIP)) of the Social Security Act to expand basic health care coverage to groups not currently eligible to receive benefits. This initiative derives from the 1115 demonstration authority. Through this initiative a state may propose changes in its program that enable it to extend a limited package of basic health care benefits to additional groups of individuals. Such changes may include limiting services for optional eligibility groups and imposing cost-sharing on certain groups.
-
AZ, DE, HI, KY (not statewide), MD, MA, MN, NY, OK, OR, RI, VT. Other states operate 1115 demonstrations that are narrower in scope. The number of states that operate these demonstrations has not changed appreciably in recent years.
-
The material in this section is based on: (a) personal communication with Beth Tanzman, MSW, Director, Adult Community Mental Health Programs, Vermont Division of Mental Health, Department of Developmental and Mental Health Services; (b) Vermont Department of Developmental and Mental Health Services (2003). The Statewide System of Care Plan for Adult Mental Health in Vermont: Update -- Fiscal Years 2003-2003. Waterbury, VT; and, (c) Vermont Department of Developmental and Mental Health Services (2002). Description of Programs and Services. Waterbury Vermont.
-
Originally, there were two MCOs that furnished primary health care services to VHAP beneficiaries. In 1999, both withdrew from the market place and Vermont switched to a PCCM service delivery model.
-
For example, the Oklahoma Sooner Care demonstration includes mental health benefits in the scope of services that contracted MCOs must furnish. Sooner Care specifically excludes individuals with serious mental illnesses from mandatory enrollment. These individuals continue to receive services on a fee-for-service basis.
-
Prior to 1982, Arizona did not participate in the Medicaid program. It entered the program under an 1115 demonstration waiver and continues to operate all its Medicaid services under this authority. Mental health services were not originally part of the demonstration. In a similar vein, long-term care services were not originally included but were added in the late 1980s.
-
More information concerning the operation of Arizona's system is available at the Division of Behavioral Health Services web site: hs.state.az.us/bhs/index.htm.
-
The default managed care enrollment for SSI beneficiaries is PCCM. SSI beneficiaries may elect to receive their services through a comprehensive MCO.
-
Section 2176 of P.L. 97-35.
-
Federal regulations concerning the operation of HCBS waiver programs are located in 42 CFR Subpart G (Sections 441.300 et seq.). State Medicaid Manual materials concerning the operation of HCBS waiver programs are located in Part 4, Sections 4440 et. seq.
-
At present, there are four 1915(b)/(c) combination waiver programs. One, in Michigan, covers mental health, substance abuse and developmental disabilities services, and a second one covering the same services (Piedmont Cardinal Health Plan) will go into effect in April 2005. A third (Star Plus) is operated by Texas in the Houston area (but is being expanded to other areas). Star Plus furnishes integrated health and long-term care services to older persons and individuals with disabilities. The forth is the Wisconsin Family Care program that integrates health and long-term care services for older persons and individuals with disabilities in five counties. Information about these programs is at cms.hhs.gov/medicaid/1915b/1915bc.asp
-
In order to facilitate the community transition of institutionalized persons, a state may arrange for various services in advance of the person's actual transition and obtain federal financial participation in the costs of those services once a person enters the waiver program. Such services include necessary home modifications, equipment, and certain costs associated with a living arrangement for the person. CMS has spelled out how states can facilitate community transition in various letters to State Medicaid Directors. These letters are located on the CMS web site at cms.hhs.gov/states/letters/. Specifically, this is addressed in the following letters: (a) Olmstead letter Number 3, dated July 25, 2000; (b) letter #02-008, dated May 9, 2002; and (c) letter # 03-006, dated July 14, 2003.
-
In the past, states were required to show that operating an HCBS waiver program would reduce institutional utilization and/or avoid growth in institutional services. This requirement was known as the "cold bed rule." When HCFA (now CMS) issued revised HCBS waiver regulations in 1994, the Agency clarified that a state could serve as many individuals as it desired, irrespective of the impact on institutional utilization.
-
The template is available at cms.hhs.gov/medicaid/1915c/cwaiverapp.pdf
-
A publication that discusses the use of the HCBS waiver program to support children with serious mental or emotional disorders is: Bazelon Center (2003). An Advocate's Guide to Overcoming State Barriers and Obtaining a Home- and Community-Based Waiver for Children with Mental Health Needs. Washington DC. This publication is available at bazelon.org/issues/children/publications/3statewaivers/index.htm
-
The material here summarizes Colorado's rules for the operation of this program and has benefited from personal communications with Denise Ellis at the Colorado Department of Human Services.
-
§1915(c) specifically provides that a state may offer "day treatment or other partial hospitalization services, psychosocial rehabilitation services, and clinic services (whether or not furnished in a facility) for individuals with chronic mental illness." However, these services are rarely covered as waiver services because many states already cover them as Medicaid state plan services.
CHAPTER 7: ADDITIONAL DIMENSIONS OF USING MEDICAID
| This chapter covers several additional topics related to supporting working-age adults with serious mental illnesses in the community. These include community integration of institutionalized persons, consumer-directed services, advance directives, and telemedicine. The chapter also explores topics related to the management of Medicaid services. |
Successfully supporting people with serious mental illnesses in the community has many aspects. This chapter explores several of them in the context of their relationship to the Medicaid program. One aspect is the community integration of persons who were institutionalized, which has drawn increased attention in the wake of the U.S. Supreme Court’s landmark 1999 Olmstead decision. Another is consumer-directed services, which has garnered substantial interest at the federal and state levels, and especially among people with disabilities who want more control over their services and supports. Related to consumer-directed services are psychiatric advance directives that enable individuals to specify their preferences about treatment and services in the event they are incapacitated. Yet another aspect is the use of telemedicine to provide services.
The chapter also discusses several topics related to the management of Medicaid services, including interagency agreements between the state Medicaid agency and the state mental health authority, and federal financial participation in the costs of administering Medicaid services.
Community Integration
Community living is the overarching goal for all individuals with disabilities. The U.S. Supreme Court’s landmark 1999 Olmstead v. L.C. & E.W. decision has sparked considerable activity at both the federal and state levels to identify policy and other changes to reduce institutionalization and facilitate the transition of institutionalized persons to the community. The Court’s decision affirmed that individuals with disabilities must be served in the most integrated setting appropriate to their needs and that states must make “reasonable modifications” in their programs to foster community integration, provided that such changes do not require a “fundamental alteration” in their programs. As an outgrowth of the decision, the majority of states have developed “Olmstead” plans to identify barriers to community integration and potential remedies.1
There is growing awareness that institutionalization can be avoided when community systems have the capacity to support individuals, regardless of the severity of their disability or condition. Moreover, it is increasingly evident that many of the major barriers to community living are structural rather than programmatic. These barriers include the lack of funding portability (e.g., impediments to “money following the person” from institutional to community services) and limitations or restrictions placed on community services that leave individuals no choice but to accept institutionalization. Many states are examining their policies with an eye toward rebalancing their service systems by strengthening community services to reduce reliance on institutional services.
Along these lines, several federal initiatives have aimed at promoting community integration. President Bush’s New Freedom Initiative directed federal agencies to identify how their policies could be altered to promote community living for people with disabilities.2 An important outgrowth of the New Freedom Initiative was the formation of the President’s New Freedom Commission on Mental Health. As part of the New Freedom Initiative, each year since 2001, CMS has made federal Real Choice Systems Change grants to states and other entities.3 The purpose of these grants has been to provide states with additional resources to make essential system changes that promote community living and strengthen community services.
CMS has also stepped up its guidance and technical assistance to states concerning Medicaid community services. For example, CMS clarified that case management services for institutionalized persons to facilitate their community transition may be eligible for federal financial participation.4
There has been a steady decline in the number of individuals served in large state and county psychiatric facilities. Between 1996 and 2001, the number of individuals served in state psychiatric facilities declined by about one-third5 and many facilities were closed.6 Facility stays have become shorter as the focus shifts to short-stay treatments and quickly returning individuals to the community.
Nonetheless, unnecessary institutionalization con-tinues to affect people with serious mental illnesses. In several states there are many individuals in public psychiatric facilities whose return to the community is hindered by a lack of community services and supports. In addition, a significant percentage of nursing facility residents has a mental disorder.7 Many are working-age adults with serious mental illnesses, although estimates of the number of these individuals vary widely.8 In 1987, Congress enacted the Nursing Home Reform Act (described below) that included provisions aimed at preventing the inappropriate admission of individuals with serious mental illnesses into nursing facilities. However, the legislation’s effectiveness has been questioned.9 In some states, many individuals with serious mental illnesses reside in other types of large congregate settings, often called “board and care.”
Coordinated strategies are needed to promote community integration. Medicaid funding can underwrite the costs of the direct services that people require to live in the community. States are modifying their management of long-term care services to allow nursing facility dollars to follow individuals into the community. However, the lack of affordable housing remains one of the most challenging barriers to community integration for people with all types of disabilities, including individuals with serious mental illnesses. This problem, of course, affects not only the transition of institutionalized persons to the community but also people in the community who lack housing or are in substandard housing. Present federal policy, however, does not permit states to receive federal financial participation in the costs of housing except in Medicaid-reimbursable institutional settings. As a consequence, in order to succeed, community integration strategies must combine services funding with housing support.
States can pursue a variety of strategies to promote community integration. In particular:
- Shift State Facility Dollars to Community Services. In states that continue to have relatively large financial commitments to state facilities, opportunities exist to shift state dollars from non-Medicaid IMD settings to community services which may be matchable with federal Medicaid dollars. In 2004, Nebraska and Virginia announced that they would be closing facilities and shifting the dollars to community services. Nebraska also intends to revamp its coverage of Medicaid mental health services in order to strengthen community services.
- Nursing Home Transition Strategies. Aided by CMS grants, several states have launched initiatives to develop individualized strategies to assist nursing facility residents to return to the community. The Wisconsin Homecoming Project demonstrated substantial success in transitioning individuals with disabilities to the community, including younger adults with serious mental illnesses.12 Based on its success, Wisconsin has launched a follow-up Homecoming II project. Over 30 states have received Nursing Facility Transition Grants from CMS under the Real Choice Systems Change Grants Program.
| Nursing Facility Preadmission Screening and Resident Review (PASRR) | |
| In 1987, Congress enacted the Nursing Home Reform Act (NHRA) of 1987.10 This legislation substantially changed Medicaid law regarding the provision of nursing facility services. NHRA included provisions affecting nursing facility services for individuals with mental retardation and mental illnesses. These provisions stemmed from widespread concern about the inappropriate admission of such individuals to nursing facilities and the lack of appropriate services for them once admitted. Under NHRA, states are required to screen individuals for mental illnesses and developmental disabilities before admission to a nursing facility [Preadmission Screening (PAS)] and review their status post admission when their condition changes [Resident Review (RR)].11 A two-stage screening process is employed. Individuals suspected of having a serious mental illness after a “Level I” screen is conducted are referred for a more comprehensive “Level II” screen. Based on the results of the Level II screen, the State Mental Health Authority (SMHA) must make a determination whether nursing facility services alone will meet the person’s needs or whether such services must be augmented by “specialized services” to address the person’s mental health service needs. Absent such a determination, the person may not be admitted to the nursing facility. Specialized mental health services are eligible for federal financial participation to the extent that such services are covered under the state’s Medicaid plan. States have the latitude to define specialized services. NHRA did not foreclose the admission of individuals with serious mental illnesses to nursing facilities but established a framework for assuring that their needs would be met if they were admitted. Nursing facility admission is not confined to individuals whose need for care stems from physical health problems or conditions. Individuals with mental illnesses may qualify for nursing facility admission due to other functional limitations. In the case of many individuals with serious mental illnesses who could live in the community, a lack of community mental health services and residential options results in their admission to nursing facilities. |
- Community Transition Funding. CMS has issued guidance to states that they may furnish “community transition services” through their HCBS waiver programs.13 Such services include making rent and utility deposits for individuals transitioning to the community, along with purchasing other goods and services that enable a person to move into a community living arrangement. In its 1915(b)/(c) waiver program, Michigan is making this service available to individuals with mental illnesses and those with developmental disabilities. While the use of such services is limited to waiver programs, it provides a potential avenue to facilitate community transition. Some states make such funding available from state resources.14
- HCBS Waiver Program. Finally, the HCBS waiver program -- though not generally em-ployed for persons with mental illnesses -- is another potential tool that can be used on their behalf to facilitate community integration; either in the form of a program that targets individuals with serious mental illnesses, or through a state’s HCBS waiver programs for people with disabilities who meet the level of care criteria.
Effective strategies to promote community integration require marshaling many types of resources and, frequently, changes in state policies. Federal Medicaid dollars can play an important role in underwriting services for people returning to the community; however, they frequently must be supplemented with funds from other sources.
Consumer-Directed Services
The principals of recovery are reshaping services for individuals with serious mental illnesses by emphasizing consumer choice and empowerment. State community mental health policies, including those that apply to Medicaid services, increasingly embody these principles. Peer support and peer-run services are becoming more commonplace, thereby affording adults with serious mental illnesses more opportunities to both take charge of their own recovery and support other individuals in their recovery.
More broadly, services for people with disabilities are in the initial stages of a major transformation toward a system that allows progressively greater numbers of individuals to take direct control of their services. For example, consumer-directed personal assistance services (CD-PAS) are designed so that people with disabilities can directly hire, train, supervise, and fire the workers who support them. Many states have incorporated CD-PAS into their Medicaid programs, either for Medicaid state plan personal care/assistance services or in their HCBS waiver programs. In the arena of developmental disabilities services, the principles of self-determination have prompted states to create new options for individuals and families to manage service dollars directly, including making decisions about what to buy and from whom.
Federal Medicaid policy is increasingly accommodating consumer-directed services. During the 1990s, CMS sponsored “cash and counseling” 1115 demonstration waiver projects that enabled states (AR, FL and NJ) to test allowing Medicaid beneficiaries to take control of their personal assistance dollars by becoming the direct employer of their support workers and/or using these dollars to purchase other goods and services needed to remain in the community.15 Due in part to the success of these projects, in 2002 CMS issued “Independence Plus” waiver templates to facilitate states obtaining necessary waivers so that individuals could have the option of directing and managing their own Medicaid-funded services.16
CMS released two templates: (a) a 1915(c) waiver template for states that want to implement consumer direction under the HCBS waiver authority, and (b) an 1115 demonstration waiver template for states that want to implement consumer direction for Medicaid state plan services and/or a combination of state plan and HCBS waiver services. The 1115 template is also designed to facilitate the implementation of consumer direction across multiple beneficiary target populations. Both waiver authorities permit states to assign Medicaid service dollars to “individual budgets” for beneficiaries to directly purchase services identified in a person-centered plan. States may support beneficiaries in managing the individual budget and their services by providing for (a) “financial management services” to position the beneficiary to be the direct, supervising employer of their support workers as well as handle the disbursement of funds to purchase other consumer-designated goods and services, and (b) “support brokerage” to aid the beneficiary (as necessary) to manage their services and access other supports.
Consumer-directed services are closely identified with long-term community services and supports for individuals with physical and developmental disabilities. State-operated CD-PAS programs provided the foundation for the adoption of consumer direction in Medicaid state plan personal assistance programs and HCBS waiver programs. To date, there has been less activity in translating consumer-directed models or approaches into mental health services for working age adults with serious mental illnesses; although there clearly is mounting interest among consumer/ survivor groups and others in exploring this new approach. Through the President’s New Freedom Initiative, CMS and SAMHSA are working with constituent representatives on how a consumer self-direction initiative can be configured for individuals with mental disorders.17 Consumer-directed models embody recovery’s choice and empowerment principals but go a step further by giving individuals the explicit authority to directly manage their own services and resources.
A few states have taken steps to introduce consumer-directed models into community mental health services. In 2003, the Michigan Department of Community Health promulgated a systemwide self-determination policy and practice guideline that encourages the use of consumer-directed arrangements throughout its community mental health system. The guideline spans services for individuals with mental ill-nesses and developmental disabilities (including Medicaid services funded through Michigan’s 1915b/c waiver program).18 In October 2002, Florida launched an innovative program to pilot self-directed care for persons with severe and persistent mental illness. This program (described below) is firmly anchored in recovery principles.
So far, no state has used the Independence Plus templates as a vehicle to implement consumer--directed mental health services that provides for direct consumer management of Medicaid service dollars. Because coverage of mental health services falls largely under the Medicaid state plan (as opposed to HCBS waiver programs), the implementation of consumer-directed mental health services (including use of an individual budget and the authority to move money from one service to another) would likely require an 1115 waiver, or provide for such services as an alternate service delivery mechanism under a 1915(b) waiver program (as Michigan has done).
| Florida’s Adult Mental Health Self-Directed Care Program19 | |
| In October 2002, Florida implemented the Adult Mental Health Self-Directed Care Program on a pilot basis in the Jacksonville area. The impetus for launching this program came from consumers and NAMI affiliates interested in employing a “Money Follows the Client” service model. In 2001, a task force issued a report that described the program’s design and a business plan for a pilot self-directed care program for persons with severe and persistent mental illnesses. The design benefited from Florida’s experience with self-directed services for people with developmental disabilities. That same year, the legislature approved implementation of the pilot program. Under the pilot, 100 adults with severe and persistent mental illness can opt to self-direct their own services. The Florida Mental Health Institute is conducting an independent evaluation of the pilot. Depending on the results of the evaluation, the pilot program may be continued and/or expanded to other areas in Florida. The program’s goal is to support individuals to take more personal control of their recovery by becoming more active in the treatment and recovery process. In order to participate in the program, individuals “must be able and willing to define their own personal recovery goals, choose appropriate services, select providers, and take responsibility for personal progress.” Individuals transfer from the “case management-based service delivery system” into the self-directed care program and may transfer back to the conventional system if self-directed care does not work out for them. In lieu of case management, individuals may voluntarily elect to receive assistance in managing their services by a recovery or a recovering coach. Individuals are assigned a dollar budget and direct the purchase of services in accordance with their recovery plan. There are a variety of self-directed care services, including supported employment, supportive housing/living, chore services, psychosocial education, psychotherapy, respite, and transportation. In addition, project participants continue to have access through the mainstream service delivery system to crisis support, emergency, residential, and other services. When needed, these services are paid for with service system dollars not through the participant’s individual budget. Self-directed care services may be obtained from mental health system providers or others, as identified by the person, who meet basic qualifications. The program is also encouraging the use of “preferred providers”--client-owned and operated businesses or client-operated services affiliated with a service provider. An Administrative Services Organization (ASO) is responsible for tracking the person’s budget and paying for services included in the individual’s recovery plan. |
Advance Directives
Advance directives are legal documents based on state laws. Psychiatric advance directives function in much the same way as physical health advance directives. Psychiatric advance directives are consistent with the principles of recovery, consumer choice and empowerment. They afford individuals the opportunity to specify their preferences concerning treatment and services in the event that they are incapacitated. The majority of states have enacted advance directive statutes that specifically provide for psychiatric advance directives or sup-port their preparation under general purpose ad-vanced directive statutes.20 However, these statutes vary state-to-state.
Federal Medicaid law contains provisions regarding advance directives. The Social Security Act (§1902(a)(57) and §1902(a)(58)) requires that each state’s Medicaid plan provide for the distribution of a written description of state laws or policies concerning advance directives.21 Section 1902(w) of the Act spells out in more detail the requirements that states must follow to ensure that providers inform individuals of their rights under state law to execute an advance directive, and to ensure that providers comply with state statutory requirements. This provision specifically applies to hospitals and managed care organizations, as well as nursing facilities, hospice and home health providers. Medicaid law, then, contains an affirmative expectation that a state’s policies will require specified classes of Medicaid providers to conform their services to the treatment preferences of in-dividuals who have executed advance directives.
More broadly, state laws concerning advance directives (including psychiatric advance directives) are as binding on Medicaid providers (including those not specified in federal law) as any other health care providers. In this arena, state law takes precedence. Consequently, when specified in state law, the provisions of an advance directive apply to community providers as well as hospitals. Some states have incorporated provisions into their rehabilitative services rules that encourage staff to discuss advance directives with individuals. The topic of advance directives may be addressed during the development of an individual’s treatment plan, and individuals may be assisted in learning about advanced directives as a targeted case management activity.
Telemedicine
As treatment options progress, technology will play an ever greater role in the delivery and administration of mental health services to individuals with serious mental illnesses. The President’s New Freedom Commission on Mental Health pointed out that “in a transformed mental health system, advanced communication and information technology will empower consumers and families and will be a tool for providers to deliver the best care.”22 One important component of such technology is the use of telemedicine to deliver services. While virtually all states use telemedicine for general medical purposes (e.g., it is extremely common in radiology), telemedicine as a mental health services delivery mechanism in Medicaid has been slower to evolve. However, some states are capitalizing on telehealth technologies to provide mental health services, especially in difficult-to-serve rural, outlying areas.
CMS recognizes telemedicine as a legitimate method for delivering Medicaid services.23 Telemedicine is not treated as a distinct Medicaid coverage but rather as an allowable method for delivering a service a state already offers in its Medicaid program. Telemedicine, in the form of phone and/or videoconferencing, can be a cost-effective option for providing mental health consultations, examinations, or even routine services. Explicitly providing for telemedicine entails a state’s recognition that services may be furnished on a basis other than a literal physical face-to-face encounter between a practitioner and individual, a requirement frequently found in state coverage specifications.
Generally, telehealth programs consist of a “hub” site, where the physician or other provider is located and transmits a service by phone or video, and a “spoke” site, generally home to administrative staff, where the individual receives telehealth services. In rural areas where there may be a shortage of providers and access to specialists is often a problem, telemedicine can be a valuable tool in meeting individuals’ needs. Currently, at least eighteen states26 povide for the use of telemedicine as a general Medicaid delivery mechanism and six27 of them specifically address its use for the provision of mental health services.
| Utah and Colorado Telemedicine Provisions | |
| Utah’s rehabilitative services coverage provides that “Telehealth mental health is a complementary method of delivering traditional mental health services. The telehealth mode of delivery is reserved for rural clients where distance and travel time create difficulty with access to needed psychiatric and other mental health therapy services. Telehealth is designed to improve client access to mental health care in rural areas of Utah.”24 Utah limits the use of telehealth services as follows:
“Telemedicine is defined as the delivery of medical services, and any diagnosis, consultation, treatment, transfer of medical data, or education related to health care services using interactive audio, interactive video, or interactive data communication instead of in-person contact. No Mental Health Assessment and Services Agency, on or after January 1, 2002, may require face-to-face contact between a provider and a client for services appropriately provided through telemedicine if the client resides in a county with a population with one hundred fifty thousand residents or fewer, and if the county has the technology necessary for the provision of telemedicine. The use of telemedicine may not be required of an enrolled client when in-person care by a participating provider is available to the enrolled client within the service area of the community mental health center serving the client’s place of residence.”25 |
In providing for the use of telehealth as a Medicaid mental health service delivery mechanism, a state should consider the types of services it wishes to provide, provider qualifications and locations, and the types and quality of equipment used. As with any Medicaid service, states must comply with the federal principles of economy, efficiency, and quality of care. States can choose to reimburse for both “hub” and “spoke” locations or only “hub” sites, although most states do allow payments for both. Additionally, states can obtain Medicaid FFP dollars for expenses such as line-connection charges and hub-related administration as long as they meet all other Medicaid reimbursement requirements. Utah and Colorado provide examples (see above) of how states use telemedicine as a delivery method for mental health services.
Effective, Economical and Efficient Management of Medicaid Mental Health Services
Managing Medicaid services is a complex undertaking. Managing Medicaid services effectively, economically and efficiently requires states to (a) forge solid, collaborative working relationships between the state mental health authority and Medicaid agency, (b) select appropriate rate setting methods, (c) recruit sufficient numbers of providers to assure access to services, (d) conduct quality management and improvement activities, and (e) marshal information that supports oversight, and aids in understanding the extent to which critical system goals and objectives are attained. Some aspects of federal Medicaid policy affect the management of Medicaid mental health services. But, as in other policy dimensions, states have considerable latitude in crafting effective system management strategies. Medicaid can also contribute resources to underwrite the administrative infrastructure for managing Medicaid services.
Managing the Costs of Mental Health Services
An important concern for policy makers is that mental health services are delivered efficiently and economically. Since Medicaid is an entitlement, it can be difficult to manage expenditures for services. Spending for Medicaid mental health services can fluctuate as a result of changes in the number of eligible individuals and service utilization patterns.
Managing Medicaid mental health spending is complicated. Expenditures for community mental health services affect expenditures for costly in-patient hospital and other emergency services. In general, when the community system has solid capabilities, inpatient hospital expenditures are lower. One reason that some states employ managed care models is that they afford the opportunity to manage both community and inpatient services within a single system of care.
A related problem is that public expenditures outside of Medicaid--especially in the criminal justice system--can be affected if community mental health services are not adequately funded. For example, lack of community funding and services may cause individuals to be incarcerated longer than necessary. Hence, the decisions that a state makes about funding community mental health services can have significant consequences elsewhere in the Medicaid budget, as well as on state and local spending for other services. Especially for individuals with serious mental ill-nesses, the pathway to efficient and economical delivery of services includes the following:
- Putting in place solid crisis response and ACT capabilities in order to intercept inpatient admissions and effectively support individuals in the community who are at high risk of hospitalization. Absent such capabilities, a state faces the prospect of higher than necessary inpatient hospital spending.
- Wider dispersion of evidence-based practices that have proven track records in promoting positive outcomes for individuals and are demonstrably cost-effective. These practices and other emerging practices can lead to lower costs over the long term.
- Emphasizing rehabilitative services that enable individuals to gain skills, promote recovery, and lead to independence and self-sufficiency. Rehabilitation coupled with appropriate treat-ment also point the way toward lower long-term costs.
- Implementing a solid utilization management and review system to ensure that individuals are receiving the services that best meet their needs, and are in accordance with best practice standards.
- Complementary funding for housing and job-specific employment training. Such funding promotes stability and self-sufficiency.
Managing Medicaid mental health spending hinges on investing in critical community services in order to avoid costly, frequently repeated and inappropriate use of inpatient hospital and emergency services by individuals with serious mental illnesses.
Rate Setting and Provider Payments28
A state’s rate setting and payment policies are central elements in managing mental health services. In this arena, as others, states have considerable discretion in determining the amounts that they pay for Medicaid-funded community mental health services. Federal policy concerning provider payments lays down a few fundamental parameters that states must observe. These parameters are generally applicable to services furnished through the Medicaid state plan (as opposed to furnishing such services through a waiver or managed care arrangement29), including mental health services.30 In particular,
- The state plan must describe the policy and methods that are used to set rates for each service.
- The method that a state employs must be "consistent with efficiency, economy and quality of care" and result in payments that are sufficient to enlist enough providers so that beneficiaries can access services.31 This broad statutory requirement has not been further elaborated upon in federal rules or CMS guidance.32
- When a state bases its payments on provider costs, it must have procedures to audit those costs.
- In the case of residential services, the state's payment must exclude the costs of "room and board.
- The Medicaid agency must provide proper advance notice when it proposes to make a major change in its methodology.
- Providers must accept the Medicaid payment as "payment in full" for the services they provide. In other words, they may not "balance bill" recipients for an amount over and above the Medicaid payment.
When mental health services are furnished under the Medicaid state plan (rather than through a waiver program), payments are usually structured on a fee-for-service basis. That is, a pre-determined amount is paid for each unit of service provided. States have latitude in defining what constitutes a unit of service and in specifying the different def-initions that may be applied to each service. Units of practitioner services may be defined as a "visit," "session" or in time increments. Residential services may be reimbursed on a per diem rate or on a monthly basis.33
In order to be reimbursed, a provider must submit a "claim" that details the units of services furnished to a specific beneficiary by date. The provider must maintain documentation that supports its claim (e.g., evidence that the covered service was provided to the beneficiary) and, depending on a state's requirements, also show that the service was authorized in the person's treatment plan and/or properly pre-authorized. Provider claims for services must be processed through the states' Medicaid Management Information System (MMIS) in order to verify that they are allowable before payment is issued.34 Claims must also comply with the requirements of the Health Insurance Port-ability and Accountability Act (HIPAA) of 1996.35
Within the foregoing federal payment parameters, states employ a variety of methods to determine provider rates. Different methods may be employed for each service. In general, states use two basic methods, described below.
- Uniform Fee Schedule. A state may adopt a uniform fee schedule that reimburses each provider the same amount for a service. Such schedules are commonly employed for practitioner services but are also used for other types of services. Fee schedules may be based on an analysis of provider costs, amounts paid by other payers, and/or benchmarked against Medicare payments for similar services. A state's fee schedule may take into account geographic differences in the costs of furnishing services.
- Provider-Specific Rates. Alternatively, a state may determine a specific payment rate for each provider, based on provider cost reports or budgets submitted by providers. These rates may be "prospective" (i.e., the rate paid to the provider is not adjusted after the fact by comparing payments to actual costs) or "retrospective" (i.e., an "interim rate" is set and payments are settled based on the provider's actual costs). When states determine rates provider-by-provider, usually allowable provider costs are subject to limits (e.g., costs are not allowed that exceed a "reasonableness" threshold), and some costs may be removed from the calculation because they are not allowable under federal policy.36 In addition, states may impose overall ceilings on rates based on "industry" norms.37
Each rate setting method has its pros and cons.38 In general, the trend among states is to adopt uniform fee schedules rather than set rates provider-by-provider because they are less burdensome to administer. In general, CMS defers to states concerning rate-determination methods, as long as the state's proposed method falls within federal parameters (described above). However, CMS may examine a state's proposed method in greater detail when it is uncertain whether the method will promote economy and efficiency.
| Reimbursement rates must strike a balance between offering adequate financial incentives for an agency or professional to provide the service and ensuring that states are not 'overpaying' for services.39 |
Whatever methods are employed, experts recommend that a state's payments for community mental health services contribute to advancing its overarching goals and objectives for these services, including promoting access, quality and effective service delivery. Experience has led state officials to recommend that payments should be sufficient to assure that an adequate number of providers will furnish the service, and that providers have the resources needed to employ skilled professionals and maintain a stable workforce. In addition, especially in the case of rehabilitative services, it frequently is important when setting rates to take into account the costs of activities that are integral to the delivery of effective services but cannot be directly billed to Medicaid. These costs may in-clude time spent traveling or making collateral con-tacts that are not billable as direct services to an individual. Such costs may be taken into account when setting payment rates.
Interagency Agreements
Federal Medicaid law dictates that Medicaid-funded services must be administered by a designated single state Medicaid agency (SSMA). Federal policy prohibits an SSMA from delegating its authority or responsibilities to other entities, including other state agencies40. This requirement is longstanding. Its purpose is to ensure that there is a direct and unequivocal accountability for the administration of Medicaid services between a state and the federal government.
The SSMA requirement potentially clashes with the state mental health authority's (SMHA) fundamental responsibility to manage mental health services and has been a source of tension in some states. For example, SMHAs and SSMAs may have different objectives (e.g., maximizing federal funding to increase the total resources available for mental health services versus containing Medicaid spending). Clearly, absent collaboration and cooperation between the two agencies, the result can be fragmentation in the management of mental health services.
Medicaid policy supports the execution of cooperative arrangements between a state's SMHA and SSMA. While federal policy does not permit a SMHA to exercise direct authority over Medicaid-funded services, it does permit the SMHA and SSMA to enter into an interagency agreement concerning the delivery of mental health services. Under such an agreement, an SMHA may conduct specified administrative activities on behalf of the SSMA, provided that the SSMA retains the ultimate authority and responsibility for such activities. In 2001, 31 states had such agreements.41 When a SMHA conducts administrative activities on behalf of the Medicaid agency, its costs of performing such activities may be eligible for federal financial participation via administrative claiming (see next page). In some states, the SMHA is considered to be part of the SSMA and, hence, can play a more direct role in the administration of Medicaid services.42
For example, Georgia's policy aim is to implement a unified approach to utilization management, and employ common provider and service standards across its community system, regardless of funding source. To do this, it has established an interagency agreement between the Georgia Division of Mental Health/Mental Retardation/Substance Abuse (DMH /MR/SA) and the Georgia Department of Com-munity Health (DCH -- the state Medicaid agency), which provides that DMH/MR/SA will verify that providers meet the qualifications set forth in the state's rehabilitative services coverage, in part by pre-screening provider applications to ensure that new providers are qualified. The agreement also provides that DMH/MR/SA will contract with an external utilization review organization (ERO) to conduct utilization management and prepare reports for both agencies. The agreement also provides for DMH/MR/SA to monitor ERO performance and conduct additional activities on behalf of DCH. The agreement also spells out var-ious DCH responsibilities.
In addition to Medicaid administrative activities, interagency agreements may also provide for the collaboration of both agencies in addressing topics of mutual interest. For example, Florida's interagency agreement between the Agency for Health Care Administration (the state Medicaid agency) and the Department of Children and Family Services (the state mental health authority designated under Florida state law) provides for the "collaboration and joint development of all policy, budgets, procurement documents, contracts, and monitoring plans that have an impact on state and Medicaid community mental health, substance abuse and targeted case management programs."43 A goal of the agreement is that both agencies will work together to promote recovery for adults and family-based care for children. The agreement also provides that the agencies will "establish monitoring and quality assurance standards and protocols … that meet best practices standards."44 The main thrust of this agreement is to establish common principles for the delivery of mental health services across funding sources.
In some Medicaid waiver programs, the SMHA has major responsibilities for the direct operation of a managed care Medicaid waiver program with the SSMA exercising its program oversight responsibilities. This is the case in the Colorado and Michigan 1915(b) waiver programs, as well as Vermont's 1115 waiver program (described in Chapter 6).
The SSMA requirement notwithstanding, federal Medicaid policy clearly does not stand in the way of collaborative relationships between the SMHA and the SSMA and, in most states, the SSMA relies heavily on input from the SMHA in crafting and implementing Medicaid coverages and policies.
Data Systems
Information technology (IT) is vital to the effective management of complex service delivery systems, including mental health services. A solid IT system is the foundation for effective quality management and improvement. IT is also essential in managing costs and gauging the extent to which effective services are being furnished to individuals.
In mental health services, utilization data are critical to effective service management. It is important to keep in mind that underutilization of services can be as problematic as overutilization. When services authorized in a treatment plan are not being utilized or are underutilized, then it is unlikely that the individual's goals and recovery are being advanced. Where such underutilization is taking place, conducting more in-depth analysis and furnishing technical assistance can pay dividends. As discussed in Chapter 5, the application of IT to analyze the utilization of medications can not only aid in cost containment efforts, but can also assist in promoting better practitioner prescribing practices and better medication management. Since mental health services typically are delivered through county or regional service networks, data collection and information technology can also assist in ident-ifying interregional differences in utilization patterns as well as other disparities.45
Conducting such activities is virtually impossible without solid IT capabilities. Such capabilities include the capacity to store and retrieve information about consumers, link it to data concerning services utilization, and generate a wide variety of outputs. In support of such activities, Medicaid paid claims data are a robust source of information. Roughly one-half of the states have Medicaid paid claims data sharing arrangements between the Medicaid agency and the SMHA.46 Such data sharing permits an SMHA to link Medicaid service usage to its consumer data base and other information in order to develop an overall picture of utilization.
Quality Management and Improvement
Contemporary best practice in securing the best value for the health care dollar is for payers to focus on quality and continuously seek improvement in service delivery processes. In recent years, CMS has placed greater emphasis on quality manage-ment and improvement in the delivery of Medicaid services. In addition, Congress incorporated stronger quality provisions into federal law when it enacted the Balanced Budget Act of 1997 (see Chapter 6). For example, states that operate managed care waiver programs -- including behavioral health programs -- must select and implement quality improvement projects as a condition of federal approval of the waiver request. In addition, they must contract with an External Quality Review Organization (EQRO) to evaluate the services furnished under the managed care plan.
There are no parallel requirements that apply to "fee-for-service" delivery arrangements, but states have the latitude to implement quality manage-ment and improvement programs in fee-for-service systems. The costs of such programs may be claimed as an administrative expense to the extent that they are directed toward promoting efficient and effective Medicaid service delivery. Such programs may be conducted directly by the Medicaid agency, the SMHA under an agreement with the SMHA, or a third-party contractor. Again, to the extent that such analysis supports Medicaid-related quality management and improvement activities, it can potentially be financed, at least in part, with Medicaid funds through administrative claiming.
Claims for Administrative Costs
Federal financial participation (FFP) is also available to underwrite a state's costs "for the proper and efficient administration of the [Medicaid] State plan." The rate of federal financial participation in necessary state administrative costs varies depend-ing on the nature of the administrative activity. The base administrative claiming rate is 50 percent but higher rates are available for certain activities.47
In order for an activity to qualify for administrative cost claiming, its performance must be directly related to and necessary for the administration of Medicaid services. Commonly allowable administrative activities for which a state may claim administrative FFP include (among others) eligibility determination, prior authorization of services and utilization management, claims payment, provider audit, rate setting, and quality management/improvement. In general, federal financial participation is not allowable for the costs of conducting general state or local government functions. For example, FFP is not available for the costs of licensing providers (e.g., psychologists) under the provisions of state law. Such activities are considered a state responsibility because they arise from the requirements of state law. However, FFP may be available for the costs of determining whether providers meet Medicaid requirements that are over and above the possession of a license required under state law.
Claims for administrative costs can be complicated, especially when personnel and functions span Medicaid and other non-Medicaid services. When this is the case, a state must apportion costs so that Medicaid administrative FFP is only claimed for that portion of an activity's costs that is reasonably attributable to Medicaid. This is usually done by conducting time studies. When personnel and/or a function are dedicated solely to administering Medicaid services their full costs are eligible for FFP. Federal policy also permits the reimbursement of indirect costs, provided the state has a federally-approved indirect cost plan.
Federal policy does not allow a state to claim administrative activities as services. For example, the costs of eligibility determination may not be included in targeted case management and claimed at the often higher "services" or federal medical assistance percentage matching rate. Such costs must be claimed as administrative expenses.
Claims for administrative costs are not limited to activities performed directly by the Medicaid agency. Such claims also may be made for the costs incurred by other entities that perform activities on behalf of the Medicaid agency to the same extent that they would be allowable if the Medicaid agency were to perform them. For example, utilization management may be contracted to a third-party and the costs claimed as an administrative expense, because such costs would be allowable if the Medicaid agency performed the task itself. Entities that may perform tasks on behalf of the Medicaid agency include other state agencies (e.g., the SMHA), local agencies, and private entities. Whether an activity is performed by the Medicaid agency or another entity, the test of whether the costs are allowable is the same.
When another entity performs an activity on behalf of the Medicaid agency, a written agreement must spell out the nature of the activity, and the agreement must provide that the Medicaid agency oversees the entity's performance and retains ultimate responsibility. Depending on the dollar amount of the agreement, it is subject to the review and approval of the CMS Regional Office. When an administrative activity is contracted out to a private entity, competitive procurement procedures gen-erally must be followed.
In the context of Medicaid mental health services, administrative claiming potentially can assist a state in obtaining federal financial participation in the costs of managing community mental health services. For example, utilization review and management can help to assure that individuals are receiving appropriate, effective services and, thereby, that public dollars are used efficiently. Similarly, conducting periodic reviews of individual treatment plans and assessing whether individuals are receiving necessary services contributes to the long-term effectiveness of services. Both types of activities may qualify for administrative claiming when they are found necessary for the proper and efficient administration of the state plan.
Claims for administrative costs may also be used to cover the costs of outreach activities. Outreach covers the set of activities that a state undertakes to identify and inform potential applicants about the availability of services, and provide information about where and how individuals can get services. Activities can include reaching out to other community networks to which individuals might turn for assistance (e.g., faith-based organizations and homeless shelters). Outreach may also include making information available in relevant languages and/or contracting with individuals and community organizations to conduct outreach in a cul-turally appropriate and sensitive manner.
A state may also contract with community agencies to perform initial intake activities that support final decisions concerning Medicaid eligibility. Alternatively, eligibility workers may be out-stationed to take Medicaid applications and answer potential applicants' questions. Entities that receive Medicaid funds (including public agencies and service providers) must take affirmative steps to accommodate the needs of individuals with limited English proficiency, whether in obtaining Medicaid services or during the provision of such services. FFP may be available for state expenditures related to the provision of oral and written translation administrative activities and services provided to Medicaid beneficiaries.48
Administrative FFP may also be available to underwrite the costs of conducting various training and informational activities (e.g., conducting sessions for providers to provide information about revised billing procedures, changes in utilization review procedures, or to introduce a new service delivery practice). Additionally, administrative FFP may be available for activities designed to help current beneficiaries understand the benefits that are available to them. These activities may be conducted in collaboration with consumer and advocacy organizations. Administrative FFP, how-ever, is not available to train provider agency personnel in the skills that they might require to meet minimum qualifications. The costs of such training must be borne by provider agencies or underwritten with other resources.
While there are limitations on administrative cost claiming, it can assist states to meet the costs of promoting effective delivery and management of Medicaid services.
Conclusion
Promoting the community integration of working age adults with serious mental illnesses remains an important goal and challenges states to develop strategies to facilitate individuals' return to and maintenance in the community. Also, the emergence of consumer-directed services will have a significant impact on the delivery of Medicaid services to individuals with disabilities of all types. The management of Medicaid services is multi-faceted. Within the broad parameters of federal policy, states have considerable latitude in the selection of payment strategies, the application of information technology, and the design of quality management and improvement strategies. Federal funding may be available to underwrite the costs of many Medicaid administrative and management functions.
Annotated Bibliography
RATE SETTING AND PAYMENTS
O'Brien, J., Lanahan, P. and Jackson, E. (2003). Recovery in the Community. Volume II. Program and Reimbursement Strategies for Mental Health Rehabilitative Approaches Under Medicaid. Washington DC: Bazelon Center for Mental Health Law.
This publication contains considerable information concerning rate setting and payments. It is a companion publication to Recovery in the Community: Funding Mental Health Rehabilitative Approaches Under Medicaid (2001), also published by the Bazelon Center.
PASRR
Linkins, K. et al. (2001). Screening for Mental lllnesses in Nursing Facility Applicants: Understanding Federal Requirements. Rockville MD: Substance Abuse and Mental Health Services Administration, Center on Mental Health Services. Available at mentalhealth.org/publications/allpubs/SMA01-3543/default.asp
This publication contains a thorough discussion of federal PASRR requirements and some of the challenges in implementing them.
Endnotes
-
See: Fox-Gage, W., Folkemer, D. and Lewis, J. (2003). The States' Response to the Olmstead Decision: How Are States Complying. Denver: National Conference of State Legislators.
-
The President's June 2001 Executive Order 13217 called upon the federal government to assist states and localities to swiftly implement the Olmstead v. L.C. decision, stating: "The United States is committed to community-based alternatives for individuals with disabilities and recognizes that such services advance the best interests of the United States." See: whitehouse.gov/news/freedominitiative/freedominitiative.html. For additional information, also see: hhs.gov/newfreedom/eo13217.html.
-
The 2004 Consolidated Appropriations Act (P.L. 108-199) provided for a fourth round of grants in 2004. In this round, states had the opportunity to apply for grants to implement evidence-based mental health practices.
-
CMS State Medicaid Director Letter 02-008. Available at cms.hhs.gov/states/letters/smd50902.pdf
-
NASMHPD Research Institute (2002). Length of Stay in State Psychiatric Hospitals. Alexandria VA.
-
NASMHPD (2000). Closing and Reorganizing State Psychiatric Hospitals: 2000. Alexandria VA.
-
By one count, about 7.8 percent of nursing facility residents of all ages (approximately 110,000 individuals) has bipolar disorder or schizophrenia. Steve Gold (2003). MR/DD, MI and Nursing Facilities -- Information Bulletin #62.
-
DHHS Office of the Inspector General (2001). Younger Nursing Facility Residents with Mental Illness: An Unidentified Population. (OEI-05-99-00701).
-
DHHS Office of the Inspector General (2001). Younger Nursing Facility Residents with Mental Illness: Preadmission Screening and Resident Review (PASRR) Implementation and Oversight. (OEI-05-99-00700). The report found that there was wide variation in how states have implemented PASRR.
-
The NHRA was part of P.L. 100-203, the Omnibus Budget Reconciliation Act of 1987. These provisions are located in §1919 of the Social Security Act. The PASRR provisions are in §1919(e)(7). The legislation was modified in the Omnibus Budget Reconciliation Act of 1990 (P.L. 101-508).
-
The original legislation required states to conduct annual resident reviews of nursing facility residents with mental illnesses and mental retardation. In the Balanced Budget Amendment of 1996 (P.L. 104-315), the requirement to conduct annual reviews was removed. Reviews are now required only when there is a major change in a nursing facility resident's condition.
-
Eiken, S., Stevenson, D., and Burwell, B (2002). The Homecoming Project: Wisconsin's Nursing Home Demonstration Project. Cambridge MA: The MEDSTAT Group. Available at aspe.hhs.gov/daltcp/reports/WItrans.htm#section2
-
CMS State Medicaid Director Letter 02-008. Available at cms.hhs.gov/states/letters/smd50902.pdf
-
E.g., Washington State provides a "Resident Discharge Allowance" to individuals who return to the community from nursing facilities.
-
See: Phillips et al. (2003). Lessons from the Implementation of Cash and Counseling in Arkansas, Florida, and New Jersey: Final Report. Princeton, NJ: Mathematica Policy Research. Available at hhp.umd.edu/AGING/CCDemo/Products/Complete3state.pdf or [from ASPE at aspe.hhs.gov/daltcp/reports/cclesson.htm]
-
Information about Independence Plus is available at www.cms.hhs.gov/independenceplus/
-
The President's New Freedom Initiative for People with Disabilities: The 2004 Progress Report (March 2004). Available at whitehouse.gov/infocus/newfreedom/toc-004.html
-
Michigan Department of Community Health -- Mental Health and Substance Abuse Services (2003). Self-Determination Policy and Practice Guideline. Available at michigan.gov/documents/SelfDeterminationPolicy_70262_7.pdf
-
This section summarizes various materials, including the history of the SDC program, contained in: Self-Directed Care Task Force Report (2001). Self-Directed Care: A Model for Giving Choice and Control To Adult Mental Health Consumers In Baker, Clay, Duval, Nassau, and St. Johns Counties and others available at floridasdc.info/Pages/Welcome.html
-
In 2001, according to the NASMHPD Research Institute, 14 states had statutes that expressly provide for or encourage the use of advanced directives specific to mental health services. Another 20 states had general advance directive statutes.
-
These provisions were enacted in the Federal Patient Self-Determination Act, included in P.L. 101-508. Federal regulations concerning these provisions are at 42 CFR 489.102.
-
President's New Freedom Commission on Mental Health. Achieving the Promise: Transforming Mental Health Care in America. DHHS Pub. No. SMA-03-3832. Rockville, MD: 2003.
-
CMS has outlined its policy regarding telemedicine services as they relate to Medicaid on its website at cms.hhs.gov/states/telemed.asp
-
Colorado Department of Health Care Policy and Financing rules: 8.212.18. Available online at chcpf.state.co.us/HCPF/Pdf_Bin/212mhcap.pdf
-
AR, CA, CO, GA, IA, IL, KS, LA, MT, NE, NC, ND, OK, SD, TX, UT, VA, and WV.
-
CA, CO, KS, MT, UT, and VA
-
This section of the report relies heavily on O'Brien et al. (2003). Op. Cit.
-
Under a managed care arrangement, the state makes capitated payments to the managed care organization. The managed care organization establishes its own fee schedule. and provider rates.
-
The main provision in the Medicaid Act concerning payments for services is located in §1902(a)(30)(A) of the Social Security Act. In its state plan, a state must: "provide such methods and procedures relating to the utilization of, and the payment for, care and services available under the plan … as may be necessary to safeguard against unnecessary utilization of such care and services, and to assure that payments are consistent with efficiency, economy, and quality of care, and are sufficient to enlist enough providers so that care and services are available under the plan at least to the extent that such care and services are available to the general population in the geographic area."
-
Access is defined with reference to the extent to which similar services are available in a region or locality.
-
However, the interpretation of this statute has been the subject of considerable litigation over the years.
-
In the case of residential services (but others as well), a mixture of covered rehabilitative services and other supports are provided. To establish a per diem or monthly rate, the state may need to conduct a time study in order to identify costs that are attributable to Medicaid services.
-
In order to be paid, the claim must be checked to determine that the individual was eligible for Medicaid and the provider has been enrolled to furnish Medicaid services. An MMIS system also checks utilization limits (if any) and the amount charged for the service.
-
The Administrative Simplification provisions of HIPAA mandated the adoption of uniform coding and formatting of electronic health claims across all health care payors, including Medicaid. Additional information concerning this topic is at cms.hhs.gov/hipaa/hipaa2/default.asp
-
The federal Office of Management and Budget has circulated announcements that apply government-wide to federal "grant" funds, including Medicaid. These announcements establish that certain costs may not be paid using federal funds (e.g., lobbying costs). In addition, states frequently apply Medicare principles concerning "reasonable and necessary costs."
-
In the case of some services, payments also are subject to an Upper Payment Limit test.
-
For a more complete discussion of this topic, see O'Brien, J., Lanahan, P. and Jackson, E. (2003). Recovery in the Community. Volume II. Program and Reimbursement Strategies for Mental Health Rehabilitative Approaches Under Medicaid. Washington DC: Bazelon Center for Mental Health Law..
-
Ibid.
-
Federal regulations concerning the authority of the SSMA are located at 42 CFR 431.10(e).
-
NASMHPD Research Institute (2002). State Mental Health Agency Relationship to Medicaid for Funding and Organizing Mental Health Services.
-
In many states, the SMHA is a separate department or is located in a different agency than the SSMA. In these cases, an interagency agreement is required in order for the SMHA to conduct (and receive payment for) Medicaid administrative activities. In some states (e.g., Pennsylvania), the designated SSMA is a cabinet-level umbrella department and the SMHA is thereby a part of the SSMA.
-
Interagency Agreement between the Agency for Health Care Administration and the Department of Children and Family Services for the Administration of Community Mental Health, Substance Abuse and Targeted Case Management Services (November 1, 2004). This agreement is required by Florida state statute.
-
Ibid.
-
For a discussion of regional profiling, see: Technical Assistance Collaborative (2002). Behavioral Health Needs and Gaps in New Mexico. Chapter VIII: Regional Profiles of New Mexico's Service Delivery Systems. Boston MA.
-
NASMHPD Research Institute (2004). State Mental Health Agency (SMHA) Relationship to Medicaid for Funding and Organizing Mental Health Services: 2002-2003. Alexandria, VA.
-
Provisions concerning federal financial participation rates are located in §1903 of the Social Security Act (Payments to States). The Act provides for a 75 percent rate of federal financial participation for the costs of skilled professional medical personnel and support staff involved in the administration of the plan (e.g., medical personnel who evaluate requests for prior authorization of health care services) but only to the extent their expertise is necessary to perform an administrative activity. There are also higher rates for the costs of the development of information systems to process claims and perform other related functions (90 percent) and for their ongoing operation (75 percent).
-
See the CMS State Medicaid Director letter dated August 31, 2000 available at cms.hhs.gov/states/letters/. Federal policies concerning accommodations for persons with Limited English Proficiency include Presidential Executive Order #13166 issued August 11, 2000, and guidance issued by the Civil Rights Division of the U.S. Department of Justice. Additional information is available at lep.gov/ .
APPENDIX A: State Medicaid Information
This Appendix contains the following documents:
- CMS State Medicaid Manual:
- Outpatient Psychiatric Services
- Case Management
- Personal Care Services
- HCFA (CMS) Informational Memorandum (1992): Rehabilitation Services for the Mentally Ill
- 1999 State Medicaid Director Letter: Coverage of ACT
1a. State Medicaid Manual: Outpatient Psychiatric Services
4221. OUTPATIENT PSYCHIATRIC SERVICES.
A. General.--Medicaid provides coverage of various types of organized outpatient programs of psychiatric treatment. These programs are covered primarily as either outpatient hospital services (42 CFR 440.20(a)) or as clinic services (42 CFR 440.90). Problems have sometimes arisen regarding outpatient programs which inappropriately billed Medicaid for chance, momentary social encounters between a therapist and a patient as if they were valid therapeutic sessions. There have also been instances of billing for services without sufficient documentation to establish that the services were clearly related to the patient's psychiatric condition. With the ongoing effort to encourage furnishing psychiatric treatment in the least restrictive setting possible, there is an increasing need for coverage guidelines specifically directed at outpatient programs. The following guidelines can help to ensure appropriate utilization with regard to outpatient psychiatric programs.
B. Outpatient Program Entry.--An intake evaluation should be performed for each recipient being considered for entry into an outpatient psychiatric treatment program. This applies to any organized program or course of treatment that a recipient enters or attends to receive scheduled or planned outpatient psychiatric services. The evaluation is a written assessment that evaluates the recipient's mental condition and, based on the patient's diagnosis, determines whether treatment in the outpatient program would be appropriate.
The evaluation team should include, at a minimum, a physician and an individual experienced in diagnosis and treatment of mental illness (both criteria can be satisfied by the same individual, if appropriately qualified). For each recipient who enters the program, the assessment should include a certification by the evaluation team that the program is appropriate to meet the recipient's treatment needs. The assessment should be made a part of the patient records.
C. Treatment Planning.--For each recipient who enters the outpatient program, the evaluation team should develop an individual plan of care (PoC). This consists of a written, individualized plan to improve the patient's condition to the point where the patient's continued participation in the program (beyond occasional maintenance visits) is no longer necessary. The PoC is included in the patient records, and contains a written description of the treatment objectives for that patient. It also describes:
- the treatment regimen--the specific medical and remedial services, therapies, and activities that will be used to meet the treatment objectives;
- a projected schedule for service delivery--this includes the expected frequency and duration of each type of planned therapeutic session or encounter;
- the type of personnel that will be furnishing the services; and
- a projected schedule for completing reevaluations of the patient§s condition and updating the PoC.
D. Documentation.--The outpatient program should develop and maintain sufficient written documentation to support each medical or remedial therapy, service, activity, or session for which billing is made. This documentation, at a minimum, should consist of material which includes:
- the specific services rendered;
- the date and actual time the services were rendered;
- who rendered the services;
- the setting in which the services were rendered;
- the amount of time it took to deliver the services;
- the relationship of the services to the treatment regimen described in the PoC and
- updates describing the patient's progress.
For services that are not specifically included in the recipient's treatment regimen, a detailed explanation of how the services being billed relate to the treatment regimen and objectives contained in the patient's PoC should be submitted with bills. Similarly, a detailed explanation should accompany bills for a medical or remedial therapy, session, or encounter that departs from the PoC in terms of need, scheduling, frequency, or duration of services furnished (e.g., unscheduled emergency services furnished during an acute psychotic episode), explaining why this departure from the established treatment regimen is necessary in order to achieve the treatment objectives.
E. Periodic Review.--The evaluation team should periodically review the recipient's PoC in order to determine the recipient's progress toward the treatment objectives, the appropriateness of the services being furnished and the need for the recipient's continued participation in the program. The evaluation team should perform such reviews on a regular basis (i.e., at least every 90 days) and the reviews should be documented in detail in the patient records, kept on file and made available as requested for State or Federal assessment purposes.
1b. State Medicaid Manual: Case Management
4302. OPTIONAL TARGETED CASE MANAGEMENT SERVICES - BASIS, SCOPE AND PURPOSE
The Consolidated Omnibus Budget Reconciliation Act (P.L. 99-272, COBRA) added §§1915(g)(1) and (g)(2) to the Act. These sections add optional targeted case management services to the list of services that may be provided under Medicaid. Section 1895(c)(3) of the Tax Reform Act of 1986 (P.L. 99-514) added case management services to the list of services in §1905 of the Act. Section 4118(i) of OBRA 1987 (P.L. 100-203) added a section discussing the qualifications of case managers for individuals with developmental disabilities or chronic mental illness. Both the Tax Reform Act and OBRA 1987 amendments are effective as if included in COBRA and are considered effective on April 7, 1986.
A. Background.--Case management is an activity which assists individuals eligible for Medicaid in gaining and coordinating access to necessary care and services appropriate to the needs of an individual. Prior to the enactment of P.L. 99-272, States could not provide case management as a distinct service under Medicaid without the use of waiver authority. However, aspects of case management have been an integral part of the Medicaid program since its inception. The law has always required interagency agreements under which Medicaid patients may be assisted in locating and receiving services they need when these services are provided by others. Prior to the enactment of P.L. 99-272, Federal financial participation (FFP) for case management activities may be claimed in any of four basic areas:
1. Component of Another Service.--Case management may be provided as an integral and inseparable part of another covered Medicaid service. An example of this type of case management is the preparation of treatment plans by home health agencies. Since plan preparation is required as a part of home health services, separate payment for the case management component cannot be made, but is included in the payment made for the service at the Federal Medical Assistance Percentage (FMAP) rate.
2. Administration.--Case management may be provided as a function necessary for the proper and efficient operation of the Medicaid State plan, as provided in §1903(a) of the Act. Activities such as utilization review, prior authorization and nursing home preadmission screening may be paid as an administrative expense. The payment rate is either the 50 percent matching rate or the 75 percent FFP rate for skilled professional medical personnel, when the criteria in 42 CFR 432.50 are met.
3. Section 1915(b) Waivers.--Case management may be provided in a waiver granted under §1915(b) of the Act. Section 1915(b) provides that a State may request that the Secretary waive the requirements of §1902 of the Act, including the freedom of choice requirements in §1902(a)(23), if necessary to implement a primary care case management system as described in 42 CFR 431.55(c).
To qualify for such a waiver, the case management project must be cost effective, efficient, and consistent with the objectives of the Medicaid program. The waiver is needed to restrict the provider from (or through) whom an eligible individual can obtain medical care services (other than in emergency circumstances), provided the restriction does not substantially impair access to services of adequate quality, and that the statutory and regulatory requirements for waiver approvals are met. Upon the written request of the State, case management services furnished on or after April 7, 1986 pursuant to a waiver granted under §1915(b)(1) may be reimbursed at the FMAP rate when these services are performed by a vendor. Because of the nature of case management services under a §1915(b)(1) waiver, this activity, when performed by an employee of the Medicaid agency, is construed as necessary for the proper and efficient administration of the State plan and is therefore an administrative expense
4. Section 1915(c) Waivers.--Case management may be provided as a service in a waiver granted pursuant to §1915(c) of the Act. Section 1915(c)(4)(B) specifically enumerates case management as a service which may be provided as part of a home and community-based services waiver. In order to provide this service, you must define it as part of a waiver request, and identify the qualifications of the providers. Under such a waiver, case management services must be provided under a written plan of care which is subject to the approval of the State Medicaid agency. Services provided in this fashion are reimbursed at the FMAP rate. Section 4440 supplies additional information concerning home and community-based services waivers.
NOTE: The enactment of P.L. 99-272 and P.L. 99-514 has not altered your authority to provide any of the previous categories of case management.
B. Legislation.--P.L. 99-272 adds case management to the list of optional services which may be provided under Medicaid. Section 9508 of P.L. 99-272 adds a new subsection (g) to §1915 of the Act. This subsection, as amended by P.L. 100-203, provides that:
"(g)(1) A State may provide, as medical assistance, case management services under the plan without regard to the requirements of section 1902(a)(1) and section 1902(a)(10)(B). The provision of case management services under this subsection shall not restrict the choice of the individual to receive medical assistance in violation of section 1902(a)(23). A State may limit the provision of case management services under this subsection to individuals with acquired immune deficiency syndrome (AIDS); or with AIDS-related conditions, or with either, and a State may limit the provision of case management services under this subsection to individuals with chronic mental illness. The State may limit the case managers available with respect to case management services for eligible individuals with developmental disabilities or with chronic mental illness in order to ensure that the case managers for such individuals are capable of ensuring that such individuals receive needed services.
(2) For purposes of this subsection, the term 'case management services' means services which will assist individuals eligible under the plan in gaining access to needed medical, social, educational, and other services."
In authorizing States to offer case management services, Congress recognized that there was some potential for duplicate payments because the same or similar services have often been provided by other programs or under the Medicaid program itself. H. Rep. No. 453, 99th Cong., 1st Session 546 (1985), which accompanies this portion of P.L. 99-272, emphasizes that payment for case management services under §1915(g) must not duplicate payments made to public agencies or private entities under other program authorities for this same purpose.
FFP is available at the FMAP rate for targeted case management services rendered on or after April 7, 1986, when these services are included in the State plan.
C. Technical Statutory Change.--Section 1895(c)(3) of the Tax Reform Act of 1986 adds case management services to §1905(a)(19) of the Act. In so doing, it defines §1905(a)(19) in terms of §1915(g)(2).
D. Purpose.--The purpose of these instructions is to implement these sections of the statute, and to provide clarification regarding the requirements of the statute and how they may be met.
4302.1 Case Management Services - Process.--
A. Applicability.--The process described in this section applies to case management services, as described in §1905(a)(19) and §1915(g) of the Act.
B. Submission and Timeframes.--Case management under either §1905(a)(19) or §1915(g) is an optional service under Medicaid. To provide the service, incorporate it into your Medicaid State Plan by means of a State plan amendment submitted to your servicing regional office. As with all State plan amendments that provide additional services, the effective date may be no earlier than the first day of the calendar quarter in which the amendment is submitted. In no case may FFP be claimed for case management services under §1915(g) provided prior to April 7, 1986.
In order to provide services under §1915(g), submit a separate amendment for each target group. There is no limit to the number or size of target groups to whom you may provide case management services. The target group may be the State's entire Medicaid population.
4302.2 State Plan Amendment Requirements.--Any State plan amendment request to provide optional case management services must address all of the requirements of this section.
A. Target Group.--Identify the target group to whom case management services will be provided. This targeting may be done by age, type or degree of disability, illness or condition (e.g., Acquired Immune Deficiency Syndrome (AIDS) or Chronic Mental Illness), or any other identifiable characteristic or combination thereof. The following examples are target groups currently receiving case management services under §1915(g) of the Act:
- Developmentally disabled persons (as defined by the State);
- Children between the ages of birth and up to age 3 who are experiencing developmental delays or disorder behaviors as measured and verified by diagnostic instruments and procedures;
- Pregnant women and infants up to age 1;
- Individuals with hemophilia;
- Individuals 60 years of age or older who have two or more physical or mental diagnoses which result in a need for two or more services; and
- Individuals with AIDS or HIV related disorders.
In defining the target group, you must be specific and delineate all characteristics of the population.
B. Comparability.--Unless you intend to provide case management services in the same amount, duration and scope to all eligible recipients, indicate that §1915(g)(1) of the Act is invoked to provide these services without regard to the requirements of §1902(a)(10)(B) of the Act. (See 42 CFR 440.240.) The exception to comparability requirements applies only to case management services under §1915(g) of the Act.
Comparability requirements relating to all other Medicaid services are unaffected by this section.
C. Statewide Availability.--Indicate whether case management services are available to the target group statewide or whether the authority of §1915(g)(1) of the Act is invoked to provide case management services to the target group on a less than statewide basis. If case management services are not to be provided on a statewide basis, indicate the geographic areas or political subdivisions to be served. The provision of targeted case management services on a less than statewide basis does not excuse you from the requirements of §1902(a)(1) of the Act (see 42 CFR 431.50) in regard to the statewide availability of other Medicaid services.
D. Freedom of Choice.--Section 1915(g)(1) of the Act specifies that there shall be no restriction on free choice of qualified providers, in violation of §1902(a)(23) of the Act. Assure that there will be no restriction on a recipient's free choice of qualified providers of case management services. In addition, assure that case management services will not restrict an individual's free choice of providers of other Medicaid services.
In order to meet the freedom of choice requirements, you must provide for the following:
1. Option to Receive Services.--The receipt of case management services must be at the option of the individual included in the target population. A recipient cannot be forced to receive case management services for which he or she might be eligible.
2. Free Choice of Providers.--Except as indicated for individuals with developmental disabilities or chronic mental illness, an eligible individual must be free to receive case management services from any qualified provider of these services. The recipient may not be limited to case management providers in a clinic, even if the individual receives all other Medicaid services through that clinic. However, in situations where the State has chosen to provide case management services on a less than statewide basis, free choice of the qualified providers is limited to those providers located within all of the identified geographic areas or political subdivisions, as specified in the State plan.
When providing case management services to individuals with developmental disabilities or with chronic mental illness, you may limit the case managers available. This ensures that the case managers for these individuals are capable of providing the full range of needed services to these targeted recipients. This limitation is permissible only with regard to the target groups of developmentally disabled or chronically mentally ill, or any subgroups that you choose to define. If you choose to target a subgroup of individuals who are developmentally disabled or chronically mentally ill, the targeted group (e.g., based on age, degree of impairment) must continue to fit the definition of chronic mental illness or developmental disability. The requirements discussed in items D.1, D.3, and D.4 continue to apply to all target groups.
3. Provider Participation.--Any person or entity meeting State standards for the provision of case management services who wishes to become a Medicaid provider of those services must be given the opportunity to do so. However, the State is not required to extend provider participation to providers located outside the geographic areas in which case management is targeted.
4. Unrestricted Access.--Case management services under §1915(g) of the Act may not be used to restrict the access of the client to other services available under plan. This option is, however, available through waivers granted pursuant to §1915(b) of the Act. (See §2100.)
E. Qualifications of Providers.--The statute does not set minimum standards for the provision of case management services. Therefore, establish the minimum qualifications for the providers of case management services. The qualifications set must be reasonably related to the case management functions that a provider is expected to perform. While reasonable provider qualifications are necessary to assure that case managers are capable of rendering services of acceptable quality, use caution in determining the acceptable degree of such qualifications. With the exception of providers of case management services to individuals with developmental disabilities or chronic mental illness, provider qualifications must not restrict the potential providers of case management services to only those viewed as most qualified. Individuals within the specified target group must be free to receive case management services from any qualified provider.
Except as discussed in item D.2, you may not limit the provision of these services to State or other public agencies, but must permit any person or entity that meets the established qualifications in accordance with 42 CFR 431.51(b) to become a Medicaid provider.
F. Nonduplication of Payments.--Payment for case management services under §1915(g) of the Act may not duplicate payments made to public agencies or private entities under other program authorities for this same purpose.
In general, payment may not be made for services for which another payer is liable. Exceptions to this general rule include payments for prenatal or preventive pediatric care, including Early and Periodic Screening, Diagnostic and Treatment (EPSDT) services; payments for services covered under a plan for an individual for whom child support enforcement is being carried out; or any payments made through a waiver granted under the cost effectiveness provisions of 42 CFR 433.139(e). Another major exception is that payments may be made to State education agencies to cover the costs of services provided under a recipient's Individualized Education Program.
Payment may not be made for services for which no payment liability is incurred. Similarly, separate payment cannot be made for similar services which are an integral and inseparable part of another Medicaid covered service.
G. Differentiation Between Targeted Case Management Services and Case Management Type Activities for Which Administrative Federal Match May Be Claimed.--You must differentiate between case management services which may properly be claimed at the service match under §1915(g) and case management activities which are appropriate for FFP at the administrative match under the State plan, based upon the appropriate criteria. These two payment authorities do not result in mutually exclusive types of services.
There are certain case management activities which may appropriately be eligible for FFP at either the administrative or the service match rate. Examples of case management activities that may be claimed at either the administrative or the service match rate entail providing assistance to individuals to gain access to services listed in the State plan, including medical care and transportation. In cases where an activity may qualify as either a Medicaid service or an administrative activity, you may classify the function in either category. This decision must be made prior to claiming FFP because of the different rules which apply to each type of function under the Medicaid program.
1. Case Management as a Service Under §1915(g).--FFP is available at the FMAP rate for allowable case management services under §1915(g) when the following requirements are met:
- Expenditures are made on behalf of eligible recipients included in the target group (i.e., there must be an identifiable charge related to an identifiable service provided to a recipient);
- Case management services are provided as they are defined in the approved State plan;
- Case management services are furnished by individuals or entities with whom the Medicaid agency has in effect a provider agreement;
- Case management services are furnished to assist an individual in gaining or coordinating access to needed services; and
- Payment for services is made following the receipt of a valid provider claim. Providers must maintain case records which indicate all contacts with and on behalf of recipients. The case records must document name of recipient, the date of service, name of provider agency and person providing the service, nature, extent, or units of service, and the place of service delivery. In addition, providers must develop a billing system to appropriately identify and bill all liable third parties.
Because §1915(g) of the Act defines case management services as services which assist individuals eligible under the plan in gaining access to needed medical, social, educational, and other services, recipients may obtain access to services not included in the Medicaid State plan. The costs of case management services provided under §1915(g) that involve gaining access to non-Medicaid services are eligible for FFP at the service match rate.
Examples of case management services provided under §1915(g) of the Act may include assistance in obtaining Food Stamps, energy assistance, emergency housing, or legal services. All case management services provided as medical assistance pursuant to §1915(g) of the Act must be described in the State plan. In addition, they must be provided by a qualified provider as defined in the State plan.
When case management is provided pursuant to §1915(g) of the Act, the service is subject to the rules pertaining to all Medicaid services. If you choose to cover targeted case management services under your State plan, as defined in §1915(g) of the Act, you cannot claim FFP at the administrative rate for the same types of services furnished to the same target group.
NOTE: Although FFP may be available for case management activities that identify the specific services needed by an individual, assist recipients in gaining access to these services, and monitor to assure that needed services are received, FFP is not available for the cost of these specific services unless they are separately reimbursable under Medicaid. Also, FFP is not available for the cost of the administration of the services or programs to which recipients are referred.
2. Case Management as an Administrative Activity.--Case management activities may be considered allowable administrative costs of the Medicaid program when the following requirements are met:
- They are provided in a manner consistent with simplicity of administration and the best interest of the recipient, as prescribed by §1902(a)(19) of the Act; and
- Documentation maintained in support of the claim is sufficiently detailed to permit HCFA to determine whether the activities are necessary for the proper and efficient administration of the State plan, as provided by §1903(a) of the Act.
The following list of functions provides examples of activities which may properly be claimed as administrative case management activities, but not as targeted case management services. The omission of any particular function from this list does not represent a determination on HCFA's part that the function is not necessary for the administration of the plan.
- Medicaid eligibility determinations and redeterminations;
- Medicaid intake processing;
- Medicaid preadmission screening for inpatient care;
- Prior authorization for Medicaid services and utilization review; and
- Medicaid outreach (methods to inform or persuade recipients or potential recipients to enter into care through the Medicaid system).
Because activities related to services which Medicaid does not cover are not considered necessary for the administration of the Medicaid plan, the accompanying costs are not eligible for Medicaid FFP at the administrative rate. For example, case management related to obtaining social services, Food Stamps, energy assistance, or housing cannot be considered a legitimate Medicaid administrative expense even though it may produce results which are in the best interest of the recipient. These services can be provided as medical assistance if described in the State plan.
Similarly, setting up an appointment with a Medicaid participating physician and arranging for transportation for a recipient may be considered case management administrative activities necessary for the proper and efficient administration of the Medicaid plan. However, arranging for baby sitting for a recipient's child, although beneficial to the recipient, is not an activity for which administrative FFP can be claimed.
In addition, when a caseworker suspects that physical abuse of a recipient has occurred, the referral to medical care could be considered a reimbursable administrative activity under the Medicaid program. However, assisting the victim in obtaining emergency housing and legal services, although in the best interest of the recipient, is not an activity for which administrative FFP may be claimed. In cases where workers perform activities funded under multiple auspices, careful records must be kept to document the State§s claims for Federal funds under the appropriate authorities.
Administrative case management activities may be performed by an entity other than the single State agency. However, there must be an interagency agreement in effect.
When a State expects to claim FFP for Medicaid administrative case management activities, the costs for these activities must be included in a cost allocation plan submitted to and approved by your HCFA RO. HCFA reserves the right to evaluate the activities for which FFP is claimed to determine whether they meet the requirements (either administrative or service match) for payment. When FFP is claimed for any functions performed as case management administrative activities under §1903(a) of the Act, documentation must clearly demonstrate that the activities were provided to Medicaid applicants or eligibles, and were in some way connected with determining eligibility or administering services covered under the State plan.
H. Case Management Under the Early and Periodic Screening, Diagnostic and Treatment (EPSDT) Program.--Care coordination, including aspects of case management, has always been an integral component of the EPSDT program, as described in 42 CFR 441.61. OBRA 1989 (P.L. 101-239) modified the EPSDT program by adding §1905(r) to the Act. Section 1905(r) requires that States provide any services included in §1905(a) of the Act, when medical necessity for the service is shown by an EPSDT screen, whether such services are covered under the State plan. While case management is required under the expanded EPSDT program when the need for the activity is found medically necessary, this does not mean §1915(g) targeted case management services. Therefore, when the need for case management activities is found to be medically necessary, the State has several options to pursue:
1. Component of an Existing Service.--Case management services may be provided to persons participating in the EPSDT program by an existing service provider such as a physician or clinic referring the child to a specialist.
2. Administration.--Case management services may be provided to EPSDT participants by the Medicaid agency or another State agency such as title V, the Health Department or an entity with which the Medicaid agency has an interagency agreement. Administrative case management activities must be found necessary for the proper and efficient administration of the State plan and therefore must be limited to those activities necessary for the proper and efficient administration of Medicaid covered services. FFP is available at the administrative rate.
3. Medical Assistance.--Case management services may be provided under the authority of §1905(a)(19) of the Act. The service must meet the statutory definition of case management services, as defined by §1915(g) of the Act. Therefore, FFP is available for assisting recipients in gaining access to both Medicaid and non-Medicaid services. FFP for case management services furnished under §1905(a)(19) of the Act is available at the FMAP rate.
Any combination of two or more of the above is possible, as long as FFP is not available for duplication of services.
I. Service Limitations.--The following are not allowable targeted case management services as defined in §1915(g)(2) of the Act.
1. Other Medicaid Services.--When assessing an individual's need for services includes a physical or psychological examination or evaluation, bill for the examination or evaluation under the appropriate medical service category. Referral for such services may be considered a component of case management services, but the actual provision of the service does not constitute case management.
2. Referral for Treatment.--When an assessment indicates the need for medical treatment, referral or arrangements for such treatment may be included as case management services, but the actual treatment may not be considered.
3. Institutional Discharge Planning.--Discharge planning is required as a condition for payment of hospital, NF and ICF/MR services. Therefore, this cannot be billed separately as a targeted case management service.
4. Client Outreach.--Outreach activities in which a State agency or a provider attempts to contact potential recipients of a service do not constitute case management services. The statute defines case management services as, "services which will assist individuals eligible under the plan in gaining access to needed medical, social, educational and other services" (emphasis added). The attempt to contact individuals who may or may not be eligible for case management services does not fall under this definition. However, such outreach activities may be considered necessary for the proper and efficient administration of the Medicaid State plan. When this is the case, FFP is available at the administrative rate.
J. Coordination With Home and Community-Based Services Waivers.--Case management services continue to be available under home and community-based services waivers approved pursuant to §1915(c) of the Act. However, since approval for §1915(c) waiver services may only be granted for services not otherwise available under the State plan, the addition of case management services under the State plan may necessitate the modification of a home and community-based services waiver. In order to comply with the nonduplication of services requirements discussed in §4302B, the following elements apply to waivers under §1915(c).
1. Service Not Included in Waiver.--Home and community-based services waivers (and requests for waivers) which do not contain case management as a waiver service are not affected by this section.
2. Different Target Population.--Home and community-based services waivers (and requests for waivers) which are targeted at a population different from the group(s) to whom targeted case management services are provided are not affected by this section.
3. Duplication of State Plan Service.--When a home and community-based services waiver contains case management as a waiver service and the State adds case management services to the State plan, the following apply:
- Same Target Population and Service Definition.--If the target population and the service definitions are the same, delete the case management services from the waiver through an amendment request, and make appropriate cost and utilization adjustments to the waiver cost effectiveness formula.
- Same Service Definition.--If the definition of services is the same, but only a portion of waiver recipients (who receive waiver case management) are now eligible for the State plan service, the service may remain in the waiver. Adjustments must be made to the cost effectiveness formula to reflect the fact that a number of recipients now receive the State plan service.
4. Same Target Population.--If you have targeted case management services in your State plan for a particular group, and you submit a waiver request for the same targeted group, the request for waiver may not include case management services through the waiver under the same definition used in the State plan. If the case management is provided under an identical definition, it must be provided under the State plan and not under the waiver.
K. Payment Methodology.--The amendment must specify the methodology by which payments and rates are made. Indicate the payment methodology for public as well as private providers. Enter this information on attachment 4.19-B of the State plan.
L. Documentation of Claims for Case Management Services.--In order to receive payment for case management services under the plan (i.e., at the FMAP rate), fully document your claim as you do for any other Medicaid service. If you pay for case management services through capitation or prepaid health plans, the requirements of 42 CFR Part 434 must be met. With the exception of claims paid under capitation or prepaid health plan arrangements, you must document the following:
- date of service,
- name of recipient,
- name of provider agency and person providing the service,
- nature, extent, or units of service, and
- place of service.
NOTE: While forms of documentation such as time studies, random moment sampling and cost allocation plans may be appropriate for claiming administrative FFP for activities in support of the State plan, these modes of documentation are not acceptable as a basis for Federal participation in the costs of Medicaid services. There must be an identifiable charge related to an identifiable service provided to a recipient.
4302.3 Instructions For Completing Preprint Supplement.--
A. State Plan Amendment.--To include case management services in your State plan, indicate your intentions on Attachment 3.1-A and 3.1-B of the State plan preprint. In addition, complete one preprint supplement for each target group to whom the services will be provided. (OMB approval is required under the Paper Work Reduction Act of 1980 and will be obtained.)
B. Supplement 1 to Attachment 3.1-A.--Exhibit 1 is a copy of supplement 1 to Attachment 3.1-A. Each item must be completed for the amendment to be approved.
Item 1. Define the target group. Indicate any limitations of disease or condition, age, institutional or noninstitutional status or other characteristic(s) by which the target group is identified.
Item 2. Check one category. If services are provided on a less than statewide basis, specify the geographic areas or political subdivisions to which the services will be provided.
Item 3. Check one category.
Item 4. Define case management services as they apply to the target population. Specify any limitations that apply. Indicate the unit(s) of service. Identify any coordination with non-Medicaid programs or agencies.
Item 5. Specify the qualifications of the providers. These qualifications must be reasonably related to the case management function(s) that the providers are expected to perform.
Item 6. No information necessary.
Item 7. No information necessary.
| EXHIBIT I: STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT | |
| State/Territory: CASE MANAGEMENT SERVICES A. Target Group: B. Areas of State in Which Services Will Be Provided: Entire State Only in the following geographic areas (authority of §1915(g)(1) of the Act is invoked to provide services less than statewide): C. Comparability of Services: Services are provided in accordance with §1902(a)(10)(B) of the Act. Services are not comparable in amount, duration and scope. Authority of §1915(g)(1) of the Act is invoked to provide services without regard to the requirements of §1902(a)(10)(B). D. Definition of Services: E. Qualifications of Providers: F. The State assures that the provision of case management services will not restrict an individual's free choice of providers in violation of §1902(a)(23) of the Act.
|
1c. State Medicaid Manual: Personal Care Services
4480. PERSONAL CARE SERVICES
A. General.--Effective November 11, 1997, HCFA published a final regulation in the Federal Register that removed personal care services from regulations at 42 CFR 440.170 and added a new section at 42 CFR 440.167, A Personal Care Services in a home or other location. The final rule specifies the revised requirements for Medicaid coverage of personal care services furnished in a home or other location as an optional benefit. This rule conforms to the Medicaid regulations and to the provisions of '13601(a)(5) of the Omnibus Budget Reconciliation Act (OBRA) of 1993, which added '1905(a)(24) to the Social Security Act to include payment for personal care services under the definition of medical assistance
Under '1905(a)(24) of the Act, States may elect, as an optional Medicaid benefit, personal care services furnished to an individual who is not an inpatient or resident of a hospital, nursing facility, intermediate care facility for persons with mental retardation (ICF/MR), or institution for mental disease. The statute specifies that personal care services must be: (1) authorized for an individual by a physician in a plan of treatment or in accordance with a service plan approved by the State; (2) provided by an individual who is qualified to provide such services and who is not a member of the individual's family; and (3) furnished in a home or other location.
B. Changes Made by Final Regulation.--Personal care services may now be furnished in any setting except inpatient hospitals, nursing facilities, intermediate care facilities for the mentally retarded, or institutions for mental disease. States choosing to provide personal care services may provide those services in the individual's home, and, if the State so chooses, in settings outside the home.
In addition, services are not required by Federal law to be provided under the supervision of a registered nurse nor does Federal law require that a physician prescribe the services in accordance with a plan of treatment. States are now permitted the option of allowing services to be otherwise authorized for the beneficiary in accordance with a service plan approved by the State.
C. Scope of Services.--Personal care services (also known in States by other names such as personal attendant services, personal assistance services, or attendant care services, etc.) covered under a State's program may include a range of human assistance provided to persons with disabilities and chronic conditions of all ages which enables them to accomplish tasks that they would normally do for themselves if they did not have a disability. Assistance may be in the form of hands-on assistance (actually performing a personal care task for a person) or cuing so that the person performs the task by him/her self. Such assistance most often relates to performance of ADLs and IADLs. ADLs include eating, bathing, dressing, toileting, transferring, and maintaining continence. IADLs capture more complex life activities and include personal hygiene, light housework, laundry, meal preparation, transportation, grocery shopping, using the telephone, medication management, and money management. Personal care services can be provided on a continuing basis or on episodic occasions. Skilled services that may be performed only by a health professional are not considered personal care services.
- Cognitive Impairments.--An individual may be physically capable of performing ADLs and IADLs but may have limitations in performing these activities because of a cognitive impairment. Personal care services may be required because a cognitive impairment prevents an individual from knowing when or how to carry out the task. For example, an individual may no longer be able to dress without someone to cue him or her on how to do so. In such cases, personal assistance may include cuing along with supervision to ensure that the individual performs the task properly.
- Consumer-Directed Services.--A State may employ a consumer-directed service delivery model to provide personal care services under the personal care optional benefit to individuals in need of personal assistance, including persons with cognitive impairments, who have the ability and desire to manage their own care. In such cases, the Medicaid beneficiary may hire their own provider, train the provider according to their personal preferences, supervise and direct the provision of the personal care services and, if necessary, fire the provider. The State Medicaid Agency maintains responsibility for ensuring the provider meets State provider qualifications (see E below) and for monitoring service delivery. Where an individual does not have the ability or desire to manage their own care, the State may either provide personal care services without consumer direction or may permit family members or other individuals to direct the provider on behalf of the individual receiving the services.
D. Definition of Family Member.--Personal care services may not be furnished by a member of the beneficiary's family. Under the new final rule, family members are defined to be legally responsible relatives. Thus, spouses of recipients and parents of minor recipients (including stepparents who are legally responsible for minor children) are included in the definition of family member. This definition necessarily will vary based on the responsibilities imposed under State law or under custody or guardianship arrangements. Thus, a State could restrict the family members who may qualify as providers by extending the scope of legal responsibility to furnish medical support.
E. Providers.--States must develop provider qualifications for providers of personal care services and establish mechanisms for monitoring the quality of the service. Services such as those delegated by nurses or physicians to personal care attendants may be provided so long as the delegation is in keeping with State law or regulation and the services fit within the personal care services benefit covered under a State's plan. Services such as assistance with taking medications would be allowed if they are permissible in States' Nurse Practice Acts, although States need to ensure the personal care assistant is properly trained to provide medication administration and/or management.
States may wish to employ several methods to ensure that recipients are receiving high quality personal care services. For example, States may opt to a criminal background check or screen personal care attendants before they are employed. States can also establish basic minimal requirements related to age, health status, and/or education and allow the recipient to be the judge of the provider's competency through an initial screening. States can provide training to personal care providers. States also may require agency providers to train their employees. States can also utilize case managers to monitor the competency of personal care providers. State level oversight of overall program compliance, standards, case level oversight, attendant training and screening, and recipient complaint and grievance mechanisms are ways in which States can monitor the quality of their personal care programs. In this way, States can best address the needs of their target populations and develop unique provider qualifications and quality assurance mechanisms.
2. HCFA (CMS) Informational Memorandum (1992): Rehabilitation Services for the Mentally Ill
DEPARTMENT OF HEALTH & HUMAN SERVICES, Health Care Financing Administration
Memorandum
Date June 1992
Refer to: FME - 42
From Director, Medicaid Bureau
Subject Rehabilitation Services for the Mentally Ill - - INFORMATION
To All Regional Administrators
We recently circulated a draft policy memorandum concerning rehabilitation services for the mentally ill which would be used in determining services that could be included under the optional rehabilitation benefit. Rather than finalizing this policy advice, we have decided to prepare a Notice of proposed Rulemaking (NPRM) as the vehicle to issue policy on rehabilitation services for the mentally ill. Therefore, this is to advise you that the policies reflected in the draft should not be enforced based on that memorandum. We are currently rethinking several of the policies discussed in the draft memorandum. We are providing the discussion below to reflect our current thinking on the rehabilitation benefit to assist you in evaluating issues which may arise prior to the publication of final rules.
The regulatory definition of rehabilitation is specific in its intent that rehabilitation services be medical or remedial in nature for the maximum reduction of physical or mental disability and restoration of a recipient of a recipient to his best possible functional level. While it is not always possible to determine whether a specific service is rehabilitation by scrutinizing the service itself, it is more meaningful to consider the goal of the treatment. Services necessary for the treatment of mental illness may be coverable as rehabilitative services. It is important to note, however, that exclusion of a service from the definition of covered rehabilitation services does not necessarily imply it is not coverable under Medicaid under other benefit categories.
Examples of services which we believe may be covered under the definition of rehabilitation are:
Basic Living Skills
Restoration of those basic skills necessary to independently function in the community, including food planning and preparation, maintenance of living environment, community awareness and mobility skills.Social Skills
Redevelopment of those skills necessary to enable and maintain independent living in the community, including communication and socialization skills and techniques.Counseling and Therapy
Counseling and therapy services directed toward the elimination of psychosocial barriers that impede the development or modification of skills necessary for independent functioning in the community.
Examples of services which we believe do not fall under the Definition of rehabilitation are:
Vocational Training
Job training, vocational and educational services.Personal Care Services
Grooming, personal hygiene, assisting with medications and the preparation of meals -- when performed for the recipient, as opposed to teaching the recipient, are not properly defined as rehabilitative services (but may be coverable under the separate personal care services benefit option).Case Management
While case management-type services directed at managing Medicaid covered services may be a covered component of rehabilitation services, case management services which are directed toward gaining access to and monitoring non-Medicaid services are not coverable under the rehabilitation option. The latter services may be covered under the separate case management benefit option.
In addition, we are concerned about some related problems in the State plans concerning rehabilitation. You should be aware of the following issues when reviewing State plan amendments:
Involvement of Family, Guardian, Significant Other
Under the rehabilitation option, meeting, counseling, etc., with the client, family, legal guardian and/or significant other may be covered provided that the services are directed exclusively to the effective treatment of the recipient. Consultation with, and training others, can be a necessary part of planning and providing care to patients in need of psychiatric services. Consultation can, however, devolve to a point where it becomes a means of treating others rather than, or in addition to, the primary recipient. State plan amendments must make clear that services are only provided to, or directed exclusively toward, the treatment of Medicaid eligible persons.Transportation
While coverage of transportation to receive Medicaid services can be covered as both an optional State plan service or an administrative cost to the State, transportation is not itself a rehabilitative service. This does not preclude a provider of transportation services.
In addition to the issue of covered and noncovered services, there are some other inherent issues in covering psychiatric and/or psychosocial rehabilitation. States may propose to limit providers of services to community mental health centers/clinics, alcoholism treatment centers, or other specific types of agencies licensed by the State and currently providing these types of services. States should be reminded that section 1902(a) (23) of the Social Security Act and regulations at 42 CFR 431.51 provide that Medicaid recipients may obtain medical services from any qualified Medicaid provider, unless the State has an approved section 1915(b) waiver or section 1915(a) exception which restricts recipient's free choice of provider. It does, however, remain within the State's purview to develop the criteria for setting reasonable standards relating to the qualifications of providers. These standards cannot, however, arbitrarily limit who may be a qualified provider.
Finally, while limiting the optional rehabilitation benefit to only mental health rehabilitation is an acceptable limit on the scope of service, a State may not limit the service to a particular group of recipients, e.g., the mentally ill or a subgroup. While this distinction may have little or no actual significance because of the comparability of services requirement. Regulations at 42 CFR 440.240 require, in part, that services must be equal in amount, duration, and scope for all categorically needy recipients. Therefore, limiting the services to, for example, children and adolescents only (unless as part of the EPSDT benefit) or to recipients with specific DSM-III-R diagnoses, is a violation of the Medicaid comparability requirements.
As indicated, there are a number of issues which must be considered in evaluating coverage under the rehabilitation option. The discussion above should be considered advisory in nature until the regulatory process is completed. Since this process may require some time to complete, we hope this discussion will be helpful in evaluating new state plan submissions. Should you have questions regarding a specific service, we will be happy to assist you in working with the States to develop an approvable State plan amendment to include such services.
Christine Nye
3. 1999 State Medicaid Director Letter: Coverage of ACT
DEPARTMENT OF HEALTH & HUMAN SERVICES
Health Care Financing Administration
Center for Medicaid and State Operations
7500 Security Boulevard
Baltimore, MD 21244-1850
June 7, 1999
Dear State Medicaid Director:
Mental illness affects millions of Americans, many of whom rely on Medicaid to cover their health and mental health care needs. In recognition of the White House Conference on Mental Health, I am writing to provide information about several issues related to mental health services.
Developments in Mental Health Treatment
Assertive Community Treatment (ACT) programs have been used to serve persons with serious and persistent mental illness for a number of years. Programs based on ACT principles employ interdisciplinary treatment teams, shared caseloads, 24-hour mobile crisis teams, assertive outreach for treatment in clients' own environments, individualized treatment, medication, rehabilitation and supportive services. Assertive Case Management (ACM) programs which incorporate shared caseloads also provide this array of individualized, community-based services.
The evidence base for a variety of treatment and service interventions for persons with schizophrenia, including ACT and ACM, has recently been reviewed by the Schizophrenia Patient Outcomes Research Team (PORT), with support from the Agency for Health Care Policy and Research and the National Institute of Mental Health. With respect to persons with schizophrenia who are at high risk for discontinuation of treatment or for repeated crises, the PORT team concluded that:
"Randomized trials have demonstrated consistently the effectiveness of these programs [ACT and ACM] in reducing inpatient use among such high-risk patients. Several studies also support improvements in clinical and social outcomes. These studies suggest that both ACT and ACM are superior to conventional case management for high-risk cases ( Schizophrenia Bulletin, 1998)."
States should consider this recommendation in their plans for comprehensive approaches to community-based mental health services. Programs based on ACT principles can be supported under existing Medicaid policies, and a number of States currently include ACT services as a component of their mental health service package. Consumer participation in program design and the development of operational policies is especially key in the successful implementation of ACT programs.
Consumer Directed Care
Advance directives are becoming an increasingly important tool for consumers of mental health services to articulate their decisions about treatment, and to guide treatment when they can not make these decisions themselves. Current Medicaid rules (42CFR 431.20, 434.20, and 489.100) require that States develop and provide current information about State laws that deal with advance directives. We urge all State Medicaid programs to work with their State mental health authorities to ensure appropriate attention to mental health issues in their advance directives policies, and to consider how these policies are operationalized in Medicaid program services.
Pharmacy
Finally, I would like to underscore that Federal statutory requirements noted in my February 12, 1998 letter about new medications for schizophrenia apply to services that States carry out via contract. When there are prior authorization requirements for prescription medicines, including the new generation of drugs for schizophrenia, prescription requests must be responded to in 24 hours. In emergency situations, there must be provisions for dispensing at least a 72 hour supply of the requested drug.
I appreciate your attention to these important mental health updates. If you have questions or would like further information, please contact Peggy Clark (410-786-5321). If you are interested in finding out more about ACT programs, the mental health authority in your state would be a good resource. Additionally, consultation and technical assistance are available from the Center for Mental Health Services, Substance Abuse and Mental Health Services Administration (Michael English, 301-443-3606).
Sincerely,
/s/
Sally K. Richardson
Director
cc: All HCFA Regional Administrators
All HCFA Associate Regional Administrators for Medicaid and State Operations
Lee Partridge, American Public Health Services Association
Robert Glover, National Association of State Mental Health Program Directors
Joy Wilson, National Conference of State Legislatures
Matt Salo, National Governors' Association
APPENDIX B: Georgia Rehabilitative Services State Plan Amendment
Georgia Medicaid State Plan Amendment:
Community Mental Health Rehabilitative Services (excluding EPSDT services)
(Effective: July 1, 2001)
13.d.1 -Community Mental Health Rehabilitative Services
"The covered Community Mental Health Rehabilitative Services will be available to all Medicaid eligibles with mental illness and substance abuse disorders and who are medically determined to need rehabilitative services. These services must be recommended by a physician or other practitioner of the healing arts within the scope of his/her practice under state law and furnished by or under the direction of a physician, or other practitioners operating within the scope the of applicable state law, to promote the maximum reduction of symptoms and/or restoration of a recipient to his/her best possible functional level."
The services are defined as follows:
Diagnostic/Functional Assessment. Individuals access this service when it has been determined through an initial screening that the person has mental health or substance abuse needs. The Diagnostic/Functional Assessment is required within the initial 45 days of service with ongoing assessments/services provided as needed. This process includes an initial face-to-face screening, additional face-to-face contacts with the consumer and collateral contacts with family members and other treatment providers to determine the consumer's problems and strengths, to develop a differential diagnosis, to identify the disability (ies), to determine the functional level, to determine natural supports and to develop or review an individualized service plan. This service includes developing outcomes, developing social and medical histories, identifying a consumer's symptoms, strengths and needs, conducting a comprehensive clinical evaluation and developing an individualized services plan. Information gathered during the Diagnostic/functional Assessment is used by the physician or the licensed practitioner within the scope of his/her practice to authorize or recommend rehabilitative services. The Diagnostic/Functional Assessment is used to provide and direct rehabilitative services for individuals in need of mental health and/or substance abuse services. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL), and/or State certification. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
Clinic-Based Crisis Management. This service provides a face-to-face assessment and intervention to individuals in an active state of crisis. Services must be provided in a clinical setting. An immediate response is initiated and a thorough assessment of risk, mental status, and medical stability is conducted. Interventions are initiated to de-escalate the crisis. Intervention consists of rapid response to evaluate and screen the presenting situation, assistance in immediate crisis resolution and ultimately ensuring the Consumer's transition to alternate services at the appropriate level. Crisis management services are available 24 hours a day, 7 days a week. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for on Quality Children and Families, Inc. (COA), Council Leadership (CQL), and/or State certification. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
Out-of-Clinic Crisis Management. This service provides assessment to individuals in an active state of crisis and can occur in a variety of settings including the consumer's home, local emergency departments, or other community settings. Immediate response is provided to conduct a thorough assessment of risk, mental status, and medical stability, and immediate crisis resolution and de-escalation if necessary. The presenting crisis situation is such that it is medically necessary to deliver the services in the consumer's home or natural environment setting in that the consumer does not have the resources, or state of mind to present at the clinic for crisis services. Each out-of-clinic crisis provider is required to offer face-to-face crisis management services 24 hours a day, 7 days a week. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL),and/or State certification. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
Crisis Residential Services. This is a structured residential alternative or diversions from psychiatric inpatient hospitalization or inpatient detoxification. Crisis Residential Services are for individuals who are experiencing a period of acute stress that significantly impairs the capacity to cope with normal life circumstances for whom clinic or out-of-clinic services are not effective. The program provides psychiatric and/or substance abuse stabilization services that address the psychiatric, psychological, and behavioral health needs of the individuals. Specific services are: psychiatric evaluation, crisis stabilization and intervention, substance abuse detoxification, medication management and monitoring, individual, group and/or family training and counseling. A physician or a person under the supervision of physician, practicing within the scope of state law, provides crisis residential services. Services must be provided in a facility licensed as an emergency receiving and evaluating facility; however, not in an inpatient hospital or freestanding institute for mental disease (IMD). Services are provided in a facility that is less than 16 beds. This intervention is short-term, with the a length of stay not to exceed 72 hours except in individual circumstances where symptoms continue to Supersedes require this services. The need for additional services will be determined on an individual basis. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL), and State certification. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
Individual Outpatient Services. Individual outpatient services provide face-to-face counseling services for symptom/behavior management of mental health problems and substance abuse treatment. Services are directed toward developing, restoring or enhancing interpersonal and adaptive behaviors and daily living skills. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL), and/or State certification. This service maybe offered in a clinic setting or in the community. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
Family Outpatient Services. Family Outpatient services provide face-to-face counseling services to the eligible individual and their families for symptom/behavior management of mental health problems and substance abuse treatment. Services are directed toward the restoration and enhancement of the interpersonal skills of the individual within the family unit Services are directed towards the identified individual. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL), and/or State certification. This service may be offered in a clinic setting or in the community. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
Group Outpatient Services. Group Outpatient services provide for symptom/behavior management; counseling; development, restoration or enhancement of adaptive behaviors and skills; and enhance mentor maintenance of daily living skills. Services are provided to individuals in a group setting. Services may include assisting individuals in the group with enhancing or developing symptom/behavior management skills, may provide knowledge regarding mental health and substance abuse disorders and prescribed medication (including adherence to medication regimen); may provide specific problem solving skills and coping mechanisms; may provide knowledge of adaptive behaviors and skills; and may provide assistance with interpersonal skills, or community resources and support system access. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL), and/or State certification. This service maybe offered in a clinic setting or in the community. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
Medication Administration. Medication Administration is the giving or administration of an oral or injectable medication. Medication administration includes the assessment of the consumer's physical and behavioral status and a determination to continue the medication or refer the consumer to the physician. A physician or licensed nurse (working within the scope of his/her practice) can administer medication. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL), and/or State certification. This service maybe offered in a clinic setting or in the community. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
Ambulatory Detoxification. This service is the medical management of the physical process of withdrawal from alcohol or other drugs in an outpatient setting. The services focus on the rapid physical stabilization of the consumer and entry into the appropriate level of care of treatment based upon the ASAM (American Society of Addiction Medication) guidelines placement criteria. The severity of the individual's symptoms, level of supports needed, and the physician's authorization for the service will determine the outpatient setting, as well as the amount of nursing and physician supervision necessary during the withdrawal process. The individual may or may not require medication; 24-hour nursing services are not required. However, there is a contingency plan for "after hours" concerns/emergencies. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL), and/or State certification. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
Physician Assessment. A physician's assessment is the provision of specialized medical and/or psychiatric services that will result in improved levels of functioning or maintaining existing levels of functioning. The Physician Assessment provides a more comprehensive assessment of the medical psychiatric treatment needs of the individual. The information provided by the Diagnostic/Functional Assessment is used by the physician as an integral part of the assessment process, which supports diagnostic and treatment decisions. A Physician Assessment will be completed by a medical doctor. The Physician Assessment is performed by providers qualified to perform this function as determined through national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CAW), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL), and/or State certification. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
Nursing Assessment and Care. Nursing Assessment and Care is the face-to-face contact with a consumer to monitor, evaluate, assess, and/or carry out physicians' orders regarding the physical and/or psychological problems of a consumer. It includes providing special nursing assessments to observe, monitor and care for physical, nutritional and psychological problems or crises manifested in the course of the consumers treatment; to assess consumers on medication to determine the need to continue medication and/or for a physician referral; to consult with the consumer's family and/or significant other about medical and nutritional issues; medication education of the consumer and family and training for self administration of medication. The nurse's observations are reported to the physician and assist in overall medication management. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL), and/or State certification. This service maybe offered in a clinic setting or in the community. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
Psychiatric Intensive Day Treatment. Intensive Day Treatment provides for the stabilization of psychiatric impairments with time limited, intensive, clinical service by a multi-disciplinary team in a clinic or facility-based setting. This service includes medication administration. Candidates for these services have adequate natural/community support systems and do have behavioral health issues, which are imminently dangerous. This level of care for each consumer should include services available at least 20 hours per week and must be ordered by the physician. The maximum allowed to bill in one day is 5 hours and does not include any residential, room or board supports. Weekend services may be necessary to meet the needs of consumers requiring crisis stabilization or other services. Services include physician and nursing services available on a daily basis. Mandatory services include medical services, family contact, group counseling, nursing services, medical management and continuing care planning. Available services include family counseling, individual counseling, and education/training as it pertains to the alleviation of identified behavioral health problems. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL), and/or State certification. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
Psychosocial Rehabilitation. A therapeutic rehabilitative social skill building service for individuals to gain the necessary social and communication skills necessary to allow them to remain in or return to naturally occurring community programs. Services include: skill building activities that focus on the development of problem-solving techniques, social skills and medication management, and recreational activities that improve self-esteem. These services are offered in group settings. This service is provided as a step-down from intensive day treatment. Services must be provided in a clinic or other facility-based setting. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL), and/or State certification. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
Psychosocial Day Support. This service focuses on training designed to assist the consumer in the acquisition, retention or improvement of self-help, socialization and adaptive skills, which takes place in a facility-based environment with adequate staff support. These services provide less costly step-down service as an alternative to psychosocial rehabilitation. Individuals appropriate for these services do not meet the admission criteria for intensive day treatment or psychosocial rehabilitation. Providing a lower level of intensity this structured program assists consumers to attain his/her maximum functional level and is coordinated with other services on the Individualized Service Plan (ISP).Day Supports maybe used to reinforce skills or knowledge in more intensive level services. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Council on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL), State certification. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
Substance Abuse Intensive Outpatient Services. This service is a time limited treatment service for persons who require structure and support to achieve and sustain recovery. The following types of services are included in the intensive outpatient program: didactic presentations on addiction and recovery, individual and group counseling; family counseling (as it relates to the consumer's substance abuse treatment issue), regular urine drug screening; and community and social support system strategies. Services must be provided in a clinical setting. Family counseling as provided within these services must be consistent with requirements outlined in Family Outpatient services. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL), and/or State certification. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
Residential Rehabilitative Supports. Residential Rehabilitative Supports are rehabilitative services for the treatment of mental health or substance abuse problem specifically provided to individuals in a 24 hour supervised residential setting. The specific treatment services that are covered include: daily living skills training (personal hygiene skills, performance of household tasks, utilization of public transportation), behavior management training and intervention, counseling or therapy. Services are delivered to individuals according to their specific needs. Individual and group activities and programming shall consist of services to restore and develop skills in functional areas which interfere with consumer's ability to live in the community, to live independently, or regain or maintain competitive employment, to develop or maintain social relationships or to independently participate in social, interpersonal or community activities. Rehabilitative services will be provided in a certified or licensed residential setting. This service does not include inpatient hospital or care in an Institute for Mental Diseases. Services are provided in a facility that is less than 16 beds. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL), and/or State certification. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
Assertive Community Treatment (ACT). ACT is an intensive mental health service for consumers discharged from a hospital after multiple or extended stays, or who are difficult to engage in treatment. Intensive, integrated rehabilitative, crisis, treatment and community support services provided by an interdisciplinary staff team and available 24-hours/ seven days a week and be ordered by the physician. Services offered by the ACT team must be documented in an Individual Service Plan (ISP) and must include (in addition to those provided by other systems): medication administration and monitoring; self medication; crisis assessment and intervention; symptom assessment, management and individual supportive therapy; substance abuse training and counseling; psychosocial rehabilitation and skill development; personal, social and interpersonal skill training; consultation, and psycho-educational support for individuals and their families. This service is community-based. The team must include a psychiatrist and/or registered nurse, a Mental Health Professional (MHP) (SAP), or Substance Abuse Professional and/or a Peer/family Support Specialists. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL), and/or State certification. Providers are required to meet all applicable licensure and certification requirements, hold to a current license and adhere to scope of practice definitions of licensure boards.
Community Support Services. Community support services consist of mental health and substance abuse rehabilitative, services and supports necessary to assist the person in achieving rehabilitative and recovery goals. This service is often a step-down from Assertive Community Treatment, Intensive Family Intervention and Residential Rehabilitative Supports. The service activities of Community Support consist of a variety of interventions: identification and intervention to address barriers that impede the development of skills necessary for independent functioning in the community; participation in the development of the consumer's Individualized Service Plan (ISP), and one-on-one interventions with the consumer to develop interpersonal and community coping skills, including adaptation to home, school and work environments; symptom monitoring and self management of symptoms. The focus of the interventions include, minimizing the negative effects of psychiatric symptoms which interfere with the consumer's daily living, financial management, and personal development; developing strategies and supportive interventions for avoiding out-of-home placements for adults and children; assisting consumers to increase social support skills that ameliorate life stresses resulting from the consumer's disability and coordinating rehabilitative services in the ISP. An individual or a team can provide community Support Services. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL), and/or State certification. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
Peer Support. This service provides structured, scheduled activities that promote socialization, recovery, self-advocacy, development of natural supports, and maintenance of community living skills, under the direct supervision of a mental health professional. Consumers actively participate in decision-making and program operation. Services are directed toward achievement of the specific goals defined by the individual and specified in the Individual Service Plan (ISP), and provided under the direct supervision of a Mental Health Professional. The interpersonal interactions and activities within the program are directed, supervised, guided and facilitated by the Mental Health Professional (MHP) in such a way to create the therapeutic community or milieu effect required to achieve individual treatment goals within a controlled environment. This concept is similar to the manner in group therapy sessions in which the staff leader or therapeutic community setting utilizes the interactions of the group members to achieve the desired individual therapy goals. Provider qualifications to provide these services are ensured by provider compliance with requirements and standards of the national accreditation Joint Commission on Accreditation for Healthcare Organizations (JCAHO), Commission on Accreditation for Rehabilitation Facilities (CARF), Council on Accreditation of Services for Children and Families, Inc. (COA), Council on Quality Leadership (CQL), and/or State certification. This service maybe offered in a clinic setting or in the community. Providers are required to meet all applicable licensure and certification requirements, hold a current license and adhere to scope of practice definitions of licensure boards.
APPENDIX C: Profiles of States that Operate Managed Mental Health Service Delivery Systems under 1915(b) and 1115 Health Care Demonstration Waiver Programs
| Profiles of 1915(b) Waiver Programs for Persons with Mental Illness | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| State | In operation since | 1915(b) Authority | Service Area | Beneficiaries Served | Services | Contractor Type | |||
| b(1) | b(2) | b(3) | b(4) | ||||||
| California (Medical Specialty Mental Health Services Consolidation) (Selective contracting only; not a capitated managed care program) (Operated by California Department of Mental Health through an interagency agreement with the Department of Health Services, the state Medicaid agency). |
1995 | X | Statewide except San Mateo and Solano Counties (San Mateo and Solano Counties are served under other waiver programs) | All beneficiary groups (adults and children) |
|
County mental health plan | |||
| Colorado (Medicaid Mental Health Capitation and Managed Care Program) (Operated by state mental health agency through an interagency agreement with the state Medicaid agency). |
1995 | X | X | X | Statewide (since 1998) | All Medicaid beneficiaries (children and adults) |
|
Mental Health Assessment and Services Agencies (community mental health centers, consortia of centers and/or partnership of one or more centers and private behavioral health organization) | |
| Florida (Previously the "Prepaid Mental Health Plan"; now combined with the Medicaid Managed Care Waiver) |
1996 | X | X | Prepaid Mental Health Providers operate in two regions. | All major eligibility groups (adults and children) except dual eligible, medicaly needy, nursing home/ ICF/MR residents and certain others |
|
Partnership between community mental health providers and private managed care company | ||
| Iowa (Iowa Plan for Behavioral Health) (Replaced separate mental health and substance abuse managed care plans |
1999 | X | X | X | Statewide | All major eligibility groups (adults and children) except persons over age 65, dual eligibles, medically needy with a cash spend down and certain others. |
|
Single private behavioral health managed care organization | |
| Michigan (Prepaid specialty mental health and substance abuse services and supports for persons with developmental disabilities) 1915(b)/(c) combination waiver |
1998 | X | X | X | Statewide | All beneficiary groups (adults and children) excluding ICF/MR residents and children enrolled in specialized 1915(c) waiver program |
|
Community mental health services programs (county-based entities that serve MH/DD/SA population) | |
| New Mexico (Salud!) (Salud! operates under a 1915(b) waiver and spans the full range of health services. State plans to breakout behavioral health services into spearate plan in 2005.) |
1997 | X | X | Statewide | All child and adult beneficiary groups, excluding dual eligibles, nursing facility and ICF/MR residents, Native Americans and certain other beneficiaries |
|
Health MCOs that are in turn required to subcontract for behavioral health services through community programs | ||
| North Carolina (Piedmont Cardinal Health Plan) 1915(b)/(c) combination waiver. 1915(c) waiver serves children and adults with developmental disabilities |
Expected state date: April 2005 |
X | Five county region | Children and adults with some exceptions |
|
Local management entity | |||
| Pennsylvania (Health Choices) (MH services are included in Health Choices but carved out) |
1997 | X | X | X | X | Various Pennsylvania counties (about 60% of Medicaid eligible population) | All beneficiary groups except persons in nursing facilities on ICFs/MR |
|
|
| Texas (Northstar) | 1999 | X | X | X | Seven counties in Dallas service area | Most beneficiary groups (children and adults) except for medically needy and institutionalized persons |
|
Single private behavioral health managed care organization | |
| Utah (Prepaid Mental Health Program) |
1991 | X | X | X | Nine of state's 10 mental health service areas (very rural service area excluded) | All types of beneficiaries5 (children and adults) |
|
Nine Community mental health centers | |
| Washington (Integrated Community Mental Health Program) |
1993 | X | X | X | Statewide | All beneficiary groups (children and adults) except dual eligibiles, residents of state owned institutions and certain other groups. |
|
14 Regional Support Networks (county-based entities) | |
| Profiles of 1115 Demonstrations with Managed Care Behavioral Health Carve-Outs | ||||
|---|---|---|---|---|
| State | Scope | Covered Groups | Services | Contractors |
| Arizona (Behavioral Health Services, including mental health and substance abuse services) (Administered by AZ Department of Health Services, Division of Behavioral Health Services) |
All mental health and substance abuse services, including services for individuals with serious mental illnesses and services for "general mental health crisis"). In October 2002, there were 52,000 individuals enrolled for services. | All child and adult eligibility groups except for certain special needs children |
|
Regional Behavioral Health Authorities (8 in total, including 3 tribal RBHAs through intergovernmental agreements) Non-tribal RBHAs are private sector companies or non-profit agencies that serve specified areas |
| Hawaii (Behavioral Health Managed Care Plan -- BMHCP) | This carve-out is part of the Hawaii QUEST 1115 Demonstration. Individuals determined to have a serious mental illness are enrolled in the carve-out on a voluntary basis. BMHCP also serves persons with co-occurring substance-abuse. The carve-out offers a wider array of services than are furnished by standard health care MCOs. | Adult eligibility groups only; children are not included |
|
Private managed care organization/subcontract to private behavioral health organization |
| Massachusetts (Massachusetts Behavioral Health Partnership - MBHP) |
MBHP is part of the Mass Health 1115 Demonstration program. Under Mass Health, individuals may elect to receive services through a comprehensive MCO. Such MCOs are required to furnish mental health services. Alternatively, a person may select PCCM model. Individuals who elect this option are automatically enrolled in MBHP to receive mental health services. SSI beneficiaries are enrolled to PCCM option | All child and adult beneficiaries except dual eligibles, nursing facility residents and persons enrolled in a comprehensive benefits MCO health plan. |
|
Private sector behavioral health managed care organization |
| Oregon Oregon Health Plan (Mental Health/Substance Abuse Full Capitation Program) |
All child and adult eligibility groups with some minor exceptions |
|
10 mental health organizations, either county-operated public entities or regional authority operated entities | |
| Tennessee Tenncare (PIHP Mental Health and Substance Abuse Full Capitation Program) |
Statewide carve-out; no mental health services are furnished by health care MCOs | All child and adult Medicaid eligibility groups plus SCHIP recipients plus expansion populations with some exceptions |
|
Private sector behavioral health managed care organizations |