
This is one of two reports examining the use of Medicaid to cover services for individuals experiencing chronic homelessness, particularly in Permanent Supportive Housing (PSH). It provides a “how-to” guide on the various ways that Medicaid can cover such services, including the Medicaid authorities and new options provided under the Affordable Care Act.
Acknowledgments
The Office of the Assistant Secretary for Planning and Evaluation, within the U.S. Department of Health and Human Services (HHS), acknowledges with gratitude the assistance of the HHS Centers for Medicare and Medicaid Services, the HHS Substance Abuse and Mental Health Services Administration, the HHS Health Resources and Services Administration, the U.S. Department of Housing and Urban Development, and the Interagency Council on Homelessness in completing this Primer. At Abt Associates, Dr. Jill Khadduri and Dr. Meryl Finkel provided thoughtful review throughout the project. We also acknowledge the late Gary Smith, the principal author of the 2007 Centers for Medicare and Medicaid Services document, A Primer on How to Use Medicaid to Assist Persons Who are Homeless to Access Medical, Behavioral Health, and Support Services.
Acronyms
The following acronyms are mentioned in this report.
| ACO | Accountable Care Organization |
|---|---|
| ACT | Assertive Community Treatment |
| AHAR | Annual Homeless Assessment Report |
| AIDS | Acquired Immune Deficiency Syndrome |
| CHCS | Center for Health Care Strategies |
| CHIP | Children's Health Insurance Program |
| CMCS | CMS Center for Medicaid and CHIP Services |
| CMS | HHS Centers for Medicare and Medicaid Services |
| COPD | Chronic Obstructive Pulmonary Disease |
| CSPECH | Community Support Program for People Experiencing Chronic Homelessness |
| DRA | Deficit Reduction Act |
| DSM-IV-TR | Diagnostic and Statistical Manual, IV version, text revision |
| FPL | Federal Poverty Level |
| FQHC | Federally Qualified Health Center |
| FY | Fiscal Year |
| GAF | Global Assessment of Functioning |
| HCBS | Home and Community-Based Services |
| HCH | Health Care for the Homeless |
| HHO | Heartland Health Outreach |
| HHS | U.S. Department of Health and Human Services |
| HIV | Human Immunodeficiency Virus |
| HRSA | HHS Health Resources and Services Administration |
| HUD | U.S. Department of Housing and Urban Development |
| IMD | Institution for Mental Disease |
| LOCUS | Level of Care Utilization System |
| LTSS | Long-Term Services and Supports |
| OB/GYN | Obstetrics and Gynecology |
| PIT | Point in Time |
| POC | Plan of Care |
| PPS | Prospective Payment System |
| PSH | Permanent Supportive Housing |
| SAMHSA | HHS Substance Abuse and Mental Health Services Administration |
| SMDL | State Medicaid Directors Letter |
| SMI | Serious Mental Illness |
| SNAP | Supplemental Nutrition Assistance Program |
| SOAR | SSI/SSDI Outreach, Access, and Recovery |
| SPA | State Plan Amendment |
| SSDI | Social Security Disability Insurance |
| SSI | Supplemental Security Income |
| TCM | Targeted Case Management |
1. Introduction
Ample evidence documents the potential for people with complex health and behavioral health conditions who have been homeless to achieve housing stability, pursue recovery, manage chronic health conditions, and stay out of hospitals, if they receive appropriate health care, other services and supports, and care coordination. On January 1, 2014, in states that have chosen to expand Medicaid eligibility under the Affordable Care Act, nearly all chronically homeless people who lacked health insurance became eligible for Medicaid. Even in states that have not expanded their Medicaid programs, Medicaid still offers eligible beneficiaries experiencing homelessness critical health and supportive services. This Primer offers state Medicaid officials and other interested parties strategies for using Medicaid to meet the needs of this very vulnerable population--some strategies that have succeeded in the past and some that are emerging under provisions of the Affordable Care Act.
1.1. Innovative Strategies
In recent years, innovative practitioners and state Medicaid offices have developed strategies for incorporating Medicaid benefits into the structures of services and supports that help keep formerly homeless people healthy and stably housed.1 Implementation of the Affordable Care Act provides opportunities for states to expand Medicaid eligibility and enrollment for people who are or were experiencing chronic homelessness. The Act also expands the mechanisms that states can use to provide a package of benefits that is effective in meeting this population's needs, improving health outcomes while contributing to the goals of controlling health costs and ending chronic homelessness.
Building on the experiences of innovators and the opportunities available through the Affordable Care Act, this Primer describes opportunities for states to use Medicaid to support the health and behavioral health services needed by people experiencing chronic homelessness or living in permanent supportive housing (PSH). It offers practical building blocks for change, including Medicaid's legislative authorities, specific provisions in state Medicaid plans, benefit design, payment mechanisms, contract provisions, and implementation strategies that states could replicate or adapt. Where available, it provides links to web-based resources such as plan documents and Centers for Medicare and Medicaid Services (CMS) informational bulletins.
1.2. Primary Audience for this Primer
The Primer's primary audience is State Medicaid Directors, other senior state Medicaid staff, and policy experts focused on ending chronic homelessness and using Medicaid to finance health care and behavioral health services to achieve that end. It assumes some knowledge of Medicaid policies and practices as they have operated in the past and strives to augment this knowledge with examples of innovative practices that states and providers have developed within traditional frameworks to meet the needs of people experiencing chronic homelessness. In addition, it describes new opportunities available under the Affordable Care Act for states to shape benefits in ways that maximize impacts on people with histories of chronic homelessness who are new to Medicaid. For each approach, this Primer describes the authorities under which Medicaid is able to provide funding support for these benefits, the specific services it provides, the providers who may deliver the services, the settings in which the services may be delivered, and the eligibility criteria required for Medicaid beneficiaries to receive the services.
1.3. Characteristics of People Experiencing Chronic Homelessness
The U.S. Department of Housing and Urban Development (HUD) defines someone as chronically homeless if he or she is homeless now, has one or more disabling conditions and has been homeless continuously for a year or more or has had four or more homeless episodes in the previous three years.2 This definition applied only to single adults through 2009, when the Homeless Emergency Assistance and Rapid Transition to Housing Act extended it to include families with a parent who meets the same criteria.3
Many people experiencing chronic homelessness have been on the streets or in shelters for years. They often have complex physical, mental, and substance use conditions that can only be ameliorated if they have a safe, stable, and secure living environment. Their homelessness may exacerbate health difficulties, making it increasingly unlikely that they can get back into housing on their own. Many people who experience chronic homelessness are not effectively engaged in treatment or ongoing care for their chronic health conditions, mental health or substance use disorders. They may be distrustful of treatment systems or mainstream health care providers, and they may find it difficult to access care or participate in treatment programs because they are focused on meeting other priorities such as finding food or shelter.
Further, many people who experience chronic homelessness make frequent and avoidable use of emergency rooms and inpatient hospital treatment.4 This use of expensive crisis public services has been a major motivator for developing PSH, which has been shown to help tenants reduce inappropriate use of services. The supportive services offered in PSH can help tenants access more appropriate primary care and treatment, learn or restore coping and independent living skills that have been impaired by disability, and avoid actions or resolve problems that could cause them to lose their housing again and return to homelessness and previous expensive patterns of crisis health service use.
From a Medicaid point of view, a key distinction within the chronically homeless population and those now living in PSH is whether or not a person has serious mental illnesses (SMI).5 Many Medicaid state plans make a wide array of mental health services available to people who qualify to receive these services by reason of SMI, while offering a less-intensive set of behavioral health services to those who do not. Most people with SMI who are or have been chronically homeless also have co-occurring substance use disorders and/or chronic medical conditions.6
Among chronically homeless people who do not have a SMI, disabling health conditions often include chronic conditions such as hypertension or heart disease, substance use disorders, mobility impairments, cognitive impairments including traumatic brain injury, developmental disabilities, and mental health disorders such as depression, anxiety, or trauma that do not meet the criteria for SMI.
Individuals experiencing chronic homelessness are getting older. Researchers have identified a cohort of people now in their late 50s who face the highest risk of continuing homelessness.7 In 2012, approximately 29 percent of individuals who stayed in homeless shelters or transitional housing programs were over age 50.8 In Los Angeles, more than one in three people experiencing chronic homelessness in 2011 (34 percent) was age 55 or older.9 As a result, the rates of age-related chronic health conditions and risks of mortality are increasing for this group. People experiencing homelessness who are age 65 or older are usually eligible for both Medicare and Medicaid.
1.4. Why Focus on People Experiencing Chronic Homelessness?
People experiencing chronic homelessness often need a broad array of health and behavioral health services to help them succeed in housing and to achieve individual health outcomes. For many, Medicaid did not figure largely as a source of financial support for these services because, until January 1, 2014, many of these people were not eligible for Medicaid. Most are single adults between the ages of 18 and 64; unless they had qualified for SSI on the basis of disability, most would not have met the criteria that would have placed them in an eligible category, with the consequence that most Medicaid providers would not have developed experience in meeting their needs.
Because most people experiencing chronic homelessness are new to Medicaid, as well as to Medicaid managed care plans and many Medicaid providers, this Primer has been developed to describe the opportunities available for delivering the most effective service approaches. It offers information to state Medicaid officials and service providers working with people experiencing chronic homelessness that is designed to help them adopt the most innovative and successful strategies currently in the field for helping this population improve its health conditions, reduce costly and avoidable hospitalizations and emergency room visits, and leave homelessness.
The remainder of this introductory chapter sets the scene for the Medicaid-related strategies described later in the Primer. It briefly describes the population of interest--people who have experienced chronic homelessness--including the complexities of their health and behavioral health conditions. It notes a growing body of evidence that PSH may save Medicaid money, as the services available through this housing model help homeless users of expensive crisis care reduce such use after becoming stably housed.
1.5. Medicaid Not Expected to Pay for Housing
Housing is a key component of all strategies for ending chronic homelessness. Statutory provisions prohibit Medicaid from paying for housing itself; none of the approaches described in this Primer expect it to do so. What Medicaid can do is finance many of the health and behavioral health elements of the supportive services without which people often fail to get or remain in housing.
1.6. The Rest of This Primer
Chapter 2 covers Medicaid eligibility issues for anyone applying for Medicaid, including the changes in the Affordable Care Act. It also describes strategies for reaching, engaging, and enrolling very low-income and homeless people that have evolved in states that opted for early-expansion after 2010 and developed by providers working with people experiencing chronic homelessness. Chapter 3 describes PSH, the approach that shows the strongest evidence for effectively ending homelessness for those who have been homeless the longest. It describes the housing and its tenants, and gives a general overview of the services that help tenants remain stably housed and healthy.
Chapter 4 describes the Medicaid authorities available to states to accommodate the needs of people experiencing chronic homelessness. These include benefits covered through longstanding strategies, options, and waivers, including Medicaid-financed care provided by Federally Qualified Health Centers (FQHCs)/Health Care for the Homeless (HCH) programs, under options for providing behavioral health care (rehabilitative services and targeted case management [TCM]), through state plan amendments (SPAs) for home and community-based services (HCBS), and other options. It also describes new possibilities under the Affordable Care Act such as Alternative Benefit Plans and new optional Medicaid health home benefits.
Chapter 5 describes the ways that service delivery for Medicaid-covered services can be organized and how providers can be reimbursed for care delivered to people experiencing chronic homelessness and those living in PSH, including new approaches being developed in communities that were part of the study underlying this Primer. It covers services through FQHCs, Medicaid rehabilitative services and other services available under optional Medicaid state plan benefits and waivers, and services needed to coordinate and integrate care across medical, behavioral health, and housing needs. It also considers integration strategies and related issues as a matter of concern for promoting the efficiency and effectiveness of a state's Medicaid program for people with complex health needs.
Chapter 6 describes the criteria of medical necessity that apply to the array of services that might potentially benefit people experiencing chronic homelessness or living in PSH. Chapter 7 reviews payment mechanisms and structures for payment reform. Chapter 8 concludes with a summary of the changes at the state and provider levels that can contribute to supporting people with histories of chronic homelessness.
In addition to describing the innovations themselves, this Primer identifies lessons learned and some of the challenges being encountered as states strive to offer appropriate care to those who have experienced chronic homelessness. Examples, which come from the six states involved in the study underlying this Primer, are works in progress. Strategies continue to evolve as states develop strategies to accommodate a major system such as Medicaid to the needs of a new and highly vulnerable population.
Many state Medicaid offices have been very focused on major tasks related to the Affordable Care Act, preparing for eligibility expansion and enrolling large numbers of people into new forms of coverage beginning in 2014. These administrative demands may have limited their capacity to also focus on small numbers of high-cost and extremely vulnerable beneficiaries, including those who are homeless. This Primer describes significant opportunities for structuring Medicaid elements to increase Medicaid's applicability to people who have been chronically homeless, which states may choose to address in coming years.
2. Medicaid Eligibility and Enrollment
Medicaid programs are partnerships between each state and the Federal Government, with each paying part of the cost. Some states involve counties in the partnership as well, with counties paying all or part of the nonfederal share for some Medicaid-covered services. Each state must develop a Medicaid state plan that describes the populations eligible for the program and the benefits its program will provide, and must have this plan approved by CMS.
Though every Medicaid state plan is different, federal law and CMS regulations prescribe a core set of benefits that each state must provide.10 States may decide to cover additional optional services and may limit eligibility for some of these additional services to specific groups of people.11 Medicaid state plan provisions specify many program details, including provider qualifications, definitions of covered services, target populations, and payment mechanisms for covered benefits. The innovations described in this and later chapters have focused on using, and if needed modifying and expanding, these elements of Medicaid state plans to increase access to and coordination of services for people who are or have been experiencing chronic homelessness. States must obtain CMS approval for optional services and other program details through SPAs.
Federal law also allows states to seek waivers of certain Medicaid rules and regulations. Several kinds of waivers are authorized under federal law.12 The primary waiver that some states have used to expand eligibility is the Section 1115 Research and Demonstration waiver. States may apply for a waiver under this authority to obtain program flexibility to test new approaches to financing and delivering Medicaid. In the years since passage of the Affordable Care Act in 2010, some states have expanded Medicaid eligibility with an 1115 waiver for people who otherwise were not eligible before passage of the Affordable Care Act. Some states have also obtained waivers under various provisions of Section 1915 to expand services for specific groups of beneficiaries or to give themselves flexibility to use proceeds from money-saving practices to cover services not specifically included in their Medicaid state plans. Waivers that include provisions to expand coverage also often include other provisions to implement changes in Medicaid payment and delivery systems through managed care.
2.1. Eligibility for Medicaid
Within the framework of federal law, states establish policies regarding Medicaid eligibility.13 Federal law requires states to cover certain population groups and allows them to cover others. In general, Medicaid covers low-income mothers and children, elderly people, and people with disabilities, although specific income and other requirements vary by state. Parents, children, and pregnant women are commonly known as the Covered Families and Children population; elderly and disabled individuals are known as the Aged, Blind, and Disabled population. Disability status is often linked to the determination used by the U.S. Social Security Administration for SSI or Social Security Disability Insurance (SSDI).14
Before 2014, adults who were not elderly, disabled, pregnant, or parents of young children were not eligible for Medicaid in most states, regardless of their income. Some states used Medicaid 1115 waivers to expand coverage to some groups of children or adults who were otherwise not eligible for Medicaid, as part of research and demonstration projects that, in addition to whatever health benefits might accrue to participants, are required to show "budget neutrality" to the federal Medicaid program.
Among people experiencing chronic homelessness, nearly all are single adults living in households without children.15 Until recently, most were not eligible for Medicaid unless they first established eligibility for SSI.16 With implementation of the Affordable Care Act's provisions for expanded eligibility based on income on January 1, 2014, 25 states and the District of Columbia expanded eligibility for Medicaid in ways that significantly increase the number of people experiencing homelessness who are eligible for Medicaid benefits. Over time additional states are likely to do the same.
HUD's definition of chronic homelessness includes the criterion of one or more disabilities. Many people who are or have been chronically homeless have disabilities that would qualify them for SSI. The rest have a variety of health and behavioral health conditions, including substance use disorders that are not defined as disabilities for purposes of SSI or Medicaid eligibility.
The Affordable Care Act expands eligibility for Medicaid in several ways. First, the law as it was enacted required states to expand eligibility to people with incomes below 133 percent of the FPL starting in 2014.17 It provides federal funding for 100 percent of the costs of Medicaid benefits for this newly eligible population between 2014 and 2016, phasing down to 90 percent in 2020 and beyond.18 Before January 2014, the law allowed states to expand eligibility based on income, with the state and Federal Government sharing costs for Medicaid benefits at the regular matching rate until the end of 2013, without the "budget neutrality" required with an 1115 waiver. In June 2012, a U.S. Supreme Court decision had the effect of making the expansion of Medicaid eligibility to people with incomes below 133 percent of poverty optional for states.
On January 1, 2014, 25 states and the District of Columbia expanded Medicaid eligibility to adults with incomes below 133 percent of poverty. Six of these states had already done so earlier, for at least some of these adults, by implementing early-expansion of Medicaid eligibility. About 64 percent of homeless people reside in these states,19 where nearly all people experiencing chronic homelessness are expected to be eligible for Medicaid in 2014 if they are United States citizens or eligible permanent residents.
In the states that have not yet moved forward to expand Medicaid eligibility under the Affordable Care Act, people will still need to meet categorical eligibility requirements to enroll in Medicaid. For most people experiencing chronic homelessness, this means they must demonstrate that they have a disability that would also make them eligible for SSI, which is not always easy to do even for people who do have a qualifying disability.
For people with disabilities experiencing chronic homelessness, establishing eligibility for SSI benefits will continue to be important regardless of whether they live in a state that expands Medicaid eligibility. In some states, people who are eligible for Medicaid because they are SSI beneficiaries will have access to a broader range of Medicaid benefits, while those who are eligible under new income-based criteria may be enrolled in Alternative Benefit Plans that may cover a slightly different set of benefits. One advantage of Alternative Benefit Plans for people experiencing chronic homelessness, however, is that they include a requirement for behavioral health parity that could provide more behavioral health services for people under these plans than would be available through traditional Medicaid. Equally important, SSI provides a source of income that can be used to pay for some housing costs and for other basic living expenses.
A small but growing number of people experiencing chronic homelessness are eligible for Medicare in addition to Medicaid. The group of people who are "dual eligible" for both Medicare and Medicaid includes adults age 65 or older who receive Medicare because they are old enough and Medicaid because they have low incomes and few assets and qualify for SSI by reason of age. Many in this group also have one or more disabilities. Some other adults with end-stage renal disease or other disabilities could also be dual eligible, if they meet additional eligibility criteria.
2.1.1. Medicaid Eligibility for People Involved in the Criminal Justice System
Many people released each year from prison or jail do not have health insurance. In states that have expanded Medicaid eligibility under the Affordable Care Act, most of these recent inmates are likely to qualify to enroll in Medicaid because their incomes are very low.
Among people returning to the community from jails and prisons, many have health care needs related to mental illness, substance use disorders, and chronic health conditions. Some of these individuals were experiencing homelessness before they were incarcerated, and they are at very high risk of returning to homelessness when they return to the community. Continuity of care for medical and behavioral health conditions can help to improve health outcomes and reduce rates of reincarceration.20
States can adopt strategies to facilitate Medicaid enrollment and continued eligibility for Medicaid for people involved in the criminal justice system, including those who have experienced chronic homelessness. Under federal law Medicaid cannot pay for health care services provided in correctional settings, but federal law does not require states to terminate Medicaid enrollment during incarceration. Instead, states may suspend a beneficiary's Medicaid enrollment when a person is incarcerated. Suspension allows states to restore Medicaid coverage immediately when the person is released from jail or prison, without the gaps in coverage that occur when enrollment is terminated. At least 12 states have adopted laws or administrative policies to suspend rather than terminate Medicaid enrollment for incarcerated people.
2.2. Enrollment Strategies
Establishing expanded eligibility for Medicaid is only the first step in expanding the population of Medicaid beneficiaries. Many of those newly eligible for Medicaid on the basis of income alone will not know about the opportunity to enroll and will not have experience with health insurance. Early-expansion states and providers working with individuals with very low incomes and those experiencing homelessness have evolved strategies for reaching, engaging, and enrolling the newly eligible population.
Enrolling people experiencing homelessness into Medicaid includes letting them know they are eligible, helping them with the enrollment process, and assuring that they remain enrolled. States that already expanded Medicaid eligibility through early implementation of the Affordable Care Act or provided Medicaid-financed coverage using 1115 waivers have developed or are developing strategies for accomplishing these tasks, which may interest many states that began to expand Medicaid eligibility in 2014.21
In these early implementer states, outreach and enrollment efforts generally started with people who were already receiving health care services from safety-net hospitals and clinics but were not Medicaid beneficiaries. Safety-net agencies have used state or local funding, grants, or other resources to pay for services for low-income people without insurance. This starting place can be effective in reaching people experiencing homelessness when they use hospital or clinic services.
Enrollment strategies employed by early implementation states include the following:
|
|---|
Implementation of the Affordable Care Act significantly simplifies and streamlines the process of determining eligibility for Medicaid enrollment in the states that expanded eligibility based on income. In a letter to state health officials and Medicaid Directors in May 2013, CMS encouraged states to adopt strategies that will facilitate enrollment.22 These include: (1) enrolling any household that receives benefits through the Supplemental Nutrition Assistance Program (SNAP, formerly food stamps), because SNAP income eligibility falls slightly below income eligibility for Medicaid under the Affordable Care Act's eligibility expansion provisions (130 percent vs. 133 percent of the FPL); and (2) for parents of children already enrolled in the Children's Health Insurance Program (CHIP), enrolling the parents based on children's income eligibility. Further, states and the Federal Government are enhancing their ability to verify citizenship, residency, and income status through electronic searches of official records. When these electronic verification systems are fully operational, they should greatly facilitate access to required documentation. Unlike the health insurance marketplaces created under the Affordable Care Act that have specific open enrollment periods, enrollment into Medicaid is always open.
In states that do not expand eligibility for Medicaid, people who experience homelessness will only be eligible for Medicaid if they meet requirements for categorical eligibility through SSI, age, pregnancy, being a parent or a member of another defined eligibility group, in addition to having an income below the limits set by the state for each eligibility category.
2.2.1. Gathering Documents to Establish Eligibility
Under federal law, states must verify some of the information submitted by people who apply for Medicaid, including income, Social Security numbers, citizenship, and immigration status. For other aspects of eligibility, including state residency, age or date of birth, and household composition, states have more flexibility and may choose from the following options:
- Rely on self-attestation without additional verification;
- Rely on self-attestation to make the eligibility determination and verify post-enrollment; or
- Verify data to determine eligibility.
States are establishing data linkages with federal and state data sources to facilitate electronic verification of information provided by Medicaid applicants. A federal data hub contains data from federal agencies such as the Internal Revenue Service, U.S. Social Security Administration, and U.S. Department of Homeland Security. State data sources can provide vital statistics and information about wages, unemployment compensation, and eligibility data for other public programs. If states verify nonfinancial eligibility criteria, they are expected to use electronic data sources to minimize requirements for applicants to submit paper documentation at the time they apply for or renew Medicaid eligibility.
Under federal law, a person must be a United States citizen or a legal resident for at least five years to qualify for enrollment in Medicaid (with some exceptions that provide limited coverage for emergency medical care or coverage funded by the state without federal funds).23 Approximately 30 states have taken up a new option, authorized in the Children's Health Insurance Program Reauthorization Act, to provide Medicaid and CHIP coverage to children and/or pregnant women who are lawfully residing in the United States, including those within their first five years of having certain legal status. The 2005 Deficit Reduction Act (DRA) imposed restrictions on eligibility for federal benefits and established requirements for Medicaid applicants to submit documentation of citizenship or immigration status. In the past it has been difficult for many people experiencing homelessness to meet these documentation requirements because they often do not have a birth certificate or appropriate identification cards. States and counties implementing coverage expansions in recent years have found that significant backlogs were created by the need for people to obtain and submit documentation to meet the DRA requirement.
Many people experiencing homelessness or living in PSH have behavioral health disorders or cognitive impairments that can make it difficult for them to understand and respond to written notices.24 In addition, people experiencing homelessness often find it difficult to get mail. This can impede program efforts to follow up and obtain additional documentation to complete a Medicaid application.
| Targeted outreach and enrollment assistance efforts can help individuals experiencing homelessness to complete the enrollment process. |
|---|
Targeted outreach and enrollment assistance efforts can help individuals experiencing homelessness to complete the enrollment process. If workers use mobile devices with wireless data access, they may be able to take pictures and submit copies of identification cards or other documents needed for verification of eligibility. Enrollment workers also try to complete the process at one time because it can be difficult to contact the individual again if additional information or documentation is required.
Providers of health, behavioral health, and homeless assistance services work to help people obtain missing birth certificates or other identification documents. In many cases the documents needed to establish eligibility for Medicaid are also needed to qualify for some housing assistance programs or for General Relief or other benefits provided by local or state government cash assistance programs. Providers of affordable and supportive housing and case managers working to assist homeless people with housing applications may already have collected some of the needed documents and can help their clients with the process of qualifying for Medicaid.
| Some organizations that provide PSH or operate homeless assistance programs have become certified enrollment assistance entities or application counselors for Medicaid. |
|---|
In some communities, organizations that provide PSH or operate homeless assistance programs have become certified enrollment assistance entities or application counselors for Medicaid, and designated staff members have become qualified as navigators or assistance personnel. These official statuses allow them to provide individualized help with the process of enrolling into Medicaid or subsidized insurance coverage through federal or state insurance marketplaces. In addition, many Health Centers have received federal grants to provide outreach and help their patients with enrollment.25 Health Centers that serve people experiencing homelessness, including those that deliver services in PSH, can be effective partners in facilitating Medicaid enrollment for people who need or already live in PSH. Private foundations have supplemented public investments in some communities, to support such targeted outreach and enrollment efforts. These activities ensure that people experiencing chronic homelessness get enrolled in Medicaid or in coverage that was made available (before 2014) through Medicaid 1115 waivers as a bridge to expanded Medicaid eligibility.
States can also engage officials in the corrections system to facilitate making Medicaid enrollment a key component of discharge planning for people who are leaving jails and prisons, many of whom are likely to be eligible to enroll in Medicaid or federally subsidized health coverage. Employees of state or county corrections departments and others who work with individuals who have been incarcerated may serve as authorized representatives for helping soon to be discharged inmates submit an application for Medicaid coverage.
| In Connecticut, the state accepts a simplified Medicaid application from inmates who are soon to be released. |
|---|
In Connecticut, the state accepts a simplified Medicaid application from inmates who are soon to be released. The applications are approved in an expedited manner and benefits are activated when the Medicaid agency receives notification that the person is being released. State corrections officials recognize that enrollment is only the first step in assuring access to health care and treatment services, and some inmates will need additional help to learn how to make and keep appointments and use available health care services appropriately.
2.2.2. Assuring Continuity of Care
States and communities that have enrolled newly eligible people into Medicaid managed care plans have had to assure continuity of care for people experiencing homelessness. States must notify new enrollees of their options for selecting a health plan and primary care provider or medical home. People experiencing homelessness may fall through the cracks of these notification processes, because they do not receive a notification sent by mail or because they do not understand the need to respond, the implications of the choices they are called upon to make, or that they will be assigned to a provider if they do not respond.
When a state Medicaid office assigns this population to a primary care provider because the people themselves have not made a choice, the assignment is often to a service provider that the beneficiaries have not previously used rather than to the care providers they are accustomed to seeing, if they have in fact had a relationship with a particular provider. Further, the assigned providers often have little capacity to meet complex needs, having no prior experience working with people experiencing homelessness. These experiences suggest that states that have or will be enrolling newly eligible people into Medicaid managed care plans will want to take steps to facilitate continuity of care as people transition from whatever care they were receiving before enrollment to the plans and providers they will use after enrollment.
With appropriate training and information, providers of services in PSH and other providers of health care and behavioral health services for homeless people may be able to work with Medicaid offices and health plans to help people who are newly eligible for Medicaid make choices about the most appropriate plans and providers based on existing relationships and needs. For example, if a clinic or provider offers primary care services that are available on-site in the person's supportive housing building or co-located with behavioral health services that the person is receiving, they can help a person select that provider. Helping people experiencing homelessness understand their options and make informed choices can help them avoid disruptions in care relationships that can occur if such people are auto-assigned to a health plan and health care providers that do not have the capacity to engage and serve this population.
2.2.3. Maintaining Enrollment
Enrolling people in Medicaid is important, but keeping them enrolled is equally critical. Before passage of the Affordable Care Act, Medicaid rules required beneficiaries to reestablish their eligibility, periodically submitting documentation to prove they continued to be eligible for Medicaid enrollment. Some states required redetermination as often as every six months. For people experiencing homelessness and for residents of PSH, the requirement to submit paperwork documenting continued eligibility poses the same issues as initial enrollment--without a reliable mailing address they often do not receive notices or fail to respond before the deadline and they experience difficulty assembling the required documentation. As a result, some providers of innovative coordinated or integrated care initiatives found their clients were being disenrolled from Medicaid in numbers almost equal to the rate of new enrollments.
In response, some agencies created systems designed to keep track of clients' recertification dates and worked with local Medicaid offices to ensure that paperwork was completed and submitted in time to prevent disenrollment.
The Affordable Care Act requires that states provide 12 months of continuous eligibility for Medicaid, rather than the shorter periods that many states had been using. As implementation of the Affordable Care Act proceeds in 2014, states are also expected to reduce or simplify requirements associated with the eligibility redetermination process and rely on electronic verification of income to establish continued eligibility. These changes should significantly reduce the churning in enrollment that was experienced in programs that expanded coverage before 2014. In its May 2013 letter to state Medicaid Directors, CMS included several options that states could adopt to reduce loss of eligibility.26
One action states can take to reduce churning in eligibility and prevent loss of benefits relates to people who enter jails or prisons. As described earlier, some states have adopted policies and procedures to suspend rather than terminate Medicaid eligibility upon incarceration, which facilitates resumption of benefits upon discharge without having to repeat the entire eligibility determination process. As many people experiencing homelessness now lose Medicaid benefits when they enter jail or prison, changing the practice from termination to suspension of benefits facilitates continued enrollment and access to care, and may reduce the risk of returning to homelessness.
2.3. Helping Establish Supplemental Security Income
SSI beneficiaries are categorically eligible for Medicaid--although in some states they still have to go through the Medicaid application process separately after qualifying for SSI. In recent years, the SAMHSA has encouraged states and communities to increase the effectiveness of their efforts to enroll people with qualifying disabilities and levels of functional impairment into SSI through its SSI/SSDI Outreach, Access, and Recovery (SOAR) program.27 In addition, some communities desiring to increase Medicaid eligibility for people experiencing chronic homelessness have independently developed mechanisms for helping people qualify for SSI on the basis of their disabilities.28 The text box gives one example.
| In Chicago, Heartland Health Outreach (HHO) has long maintained a team devoted to helping clients establish eligibility for an array of benefits, including SSI. To document disability, team members have access to HHO's own records and have cooperative relationships with some of the hospitals its clients use that facilitate further documentation. The team has good relationships with a U.S. Social Security Administration office and partners with Health and Disability Advocates for situations that require specialized assistance. Team members have recently become SOAR trainers and offer training and technical assistance to caseworkers in other agencies who have SSI-eligible clients. |
|---|
2.4. Summary
This chapter has reviewed basic guidelines for Medicaid eligibility that apply regardless of a person's housing status. These include the traditional bases for categorical eligibility--belonging to the Covered Families and Children population or the Aged, Blind, and Disabled population. It went on to describe strategies to facilitate enrollment for people experiencing chronic homelessness or living in PSH, and also examined ways to help people qualify for SSI and thus establish categorical eligibility for Medicaid.
3. Permanent Supportive Housing and Services for People Experiencing Chronic Homelessness
This chapter describes PSH, an approach that has been very successful in helping people experiencing chronic homelessness to leave the streets and achieve housing stability. It covers the housing and service configurations most commonly employed for PSH, the types of people who live in PSH, and the services offered to tenants of PSH.
3.1. Permanent Supportive Housing for People Experiencing Chronic Homelessness
PSH is intended to provide affordable housing combined with supportive services for people with disabilities or other significant barriers to housing stability. PSH is decent, safe, affordable, community-based housing, providing tenants with the rights of tenancy through leases and similar arrangements. PSH staff help tenants link to voluntary and flexible supports and services. SAMHSA has recognized PSH as an Evidence-Based Practice for reintegrating into the community people experiencing chronic homelessness and other highly vulnerable individuals with behavioral health disorders who are experiencing or at risk of homelessness or institutional care.29
3.1.1. The Housing
Across the country, PSH has been implemented using a range of models that respond to the needs and preferences of tenants and communities. PSH is intended for people who need both subsidized rent to make housing affordable and access to supportive services to help them retain their housing. It may take any of the forms of housing described below.
Creating PSH units may involve renovating units, constructing new housing, setting aside apartments within buildings, or leasing individual apartments in locations that may be scattered throughout an area. The housing component of supportive housing takes three primary forms:
- Single-Site Housing, in which the tenants receiving support services live in units in the same apartment building or a group of buildings that offer affordable housing.
- Scattered-Site Housing, in which tenants live in apartments throughout the community, often leased from private owners with rental assistance provided through government subsidies; supportive services may be delivered through home visits or provided at other locations in the community.
- Mixed Housing, in which tenants live in developments, usually affordable housing, that contain a mix of supportive housing tenants and other tenants not part of the supportive housing program; supportive services may be delivered through home visits or provided at other locations in the community.
The various supportive services needed by PSH tenants may be provided at the housing site, through home visits, or at other locations in the community. Supportive services may be delivered by staff of the housing provider or staff of health, mental health, and other providers in the community, as needed and chosen by the tenants.
3.1.2. The People Who Live in PSH
The PSH model may support a range of populations, including families or individuals who have experienced chronic homelessness, people who have been in shelters or living on the streets or in other places not meant for human habitation, individuals transitioning from institutions, or individuals with disabilities.
Over the past two decades, many state and local government agencies that have responsibility for mental health services have collaborated with housing agencies and community providers to create PSH for people with SMI who are experiencing or at risk of homelessness. Because of the sources of funding used for services or housing costs, some of these PSH programs are available only to people with a qualifying diagnosis of SMI. Other PSH programs offer housing that is designated for people experiencing chronic homelessness regardless of the specific type of disabling condition.
In communities across the country, public and private funding agencies and the organizations that create and operate supportive housing programs often collaborate to expand the availability of PSH and to prioritize access to PSH for people who have been homeless the longest. Access may be targeted to those who are most vulnerable and at risk of mortality because of their age or health conditions, or people who have most frequently used expensive crisis services such as detox, emergency rooms, hospital inpatient care, or medical care provided in jails.
3.1.3. Services in PSH
People experiencing chronic homelessness and people who live in PSH may receive care from an array of health and behavioral health care providers of their choice. These services are usually intended to help people achieve several goals:
- Manage chronic medical conditions and preventing avoidable health crises.
- Improve health and wellness through regular preventive and primary care.
- Understand and manage the symptoms of mental illness and develop coping skills.
- Provide assistance with the identification of individual strengths, preferences, hopes, and choices.
- Restore and strengthen interpersonal, functional, and community living skills that have been impaired by behavioral health disorders.
- Motivate changes in risky behaviors and harmful substance use, engage people in treatment for substance use disorders, and support recovery.
- Identify risk factors for relapse and develop relapse prevention plans and strategies.
- Get and keep housing by providing help to find and apply for housing, building skills to negotiate with landlords and get along with neighbors, and problem-solving to support stable living in the community.
- Obtain other benefits and access to community resources.
- Reduce frequent and avoidable hospitalizations, emergency room visits, stays in detox programs, nursing homes, or other crisis or institutional care.
Engagement
The services that help to achieve these goals for people who experience chronic homelessness often begin with engagement and establishing trust. People experiencing chronic homelessness are often socially isolated and they may be distrustful of medical providers and treatment systems. Their thinking and ability to communicate may be impaired by mental illness, substance use disorders, brain injuries, or other factors. As communities work to identify and house the most vulnerable people living on the streets and those who have experienced homelessness the longest, service providers often begin with engagement and assessment while people are still homeless, and their work continues through the process of helping people find and move into housing and then providing ongoing support for housing stability and recovery. Service providers make home visits or deliver care in satellite clinics or other locations that are accessible to people living in PSH, as well as to those who are still living in shelters or on the streets.
| In Washington, DC, a SAMHSA grant to integrate primary and behavioral health care supports outreach efforts by Pathways to Housing and Unity Health Care. These efforts engage some of the most vulnerable people living on the street who have resisted earlier efforts to bring them into housing and care. After the Department of Mental Health's street outreach team identifies a likely candidate, a Pathways staffer and a Unity nurse-practitioner go out to meet and engage the person. The nurse-practitioner is able to do an on-the-spot health and mental health assessment that facilitates the process of enrollment, and the outreach team works to convince the person to accept help, and eventually housing. |
|---|
Need for Multi-Disciplinary Approach
Many people who experience chronic homelessness have co-occurring medical, mental health, and substance use conditions. To address these varied needs, they often receive services delivered by multidisciplinary teams. Teams include clinicians and other team members, and also often include peers who have personal experience with homelessness and recovery. These peers can help the team establish and sustain relationships with clients and prospective clients. Collectively, the team has the expertise to address a range of medical conditions and to provide or support participation in integrated treatment and recovery for mental health and substance use disorders. Teams help to educate clients about their medical and behavioral health conditions so they will better care for themselves by taking medications regularly, improving nutrition, reducing harmful substance use, and participating in activities that promote health and reduce social isolation.
Teams may be created through partnerships among organizations that provide different types of Medicaid-covered services, such as a collaboration involving a Health Center and a provider of rehabilitation services. The Integrated Mobile Health Teams supported by the Los Angeles County Department of Mental Health are examples of this approach, with each team containing primary care clinicians from a Community Health Center and behavioral health staff from mental health providers. The teams have links to housing resources, allowing them to offer participants all of the components of PSH. In other cases a single organization provides both medical and behavioral health care services. The JWCH Center for Community Health in Los Angeles operates in this manner.
Effective Help for People with Substance Use Disorders
For people experiencing chronic homelessness, and particularly for those who have frequent and avoidable hospitalizations and emergency room visits, services to address substance use disorders are critically important. But these services for PSH tenants need to differ in important ways from the treatment programs that are available in many communities. Often people who experience chronic homelessness have difficulty effectively engaging with substance use disorder treatment programs when the programs require complete abstinence.30 Meeting this requirement is usually neither attractive nor possible for many people experiencing chronic homelessness who have long histories of substance use, particularly if they have co-occurring mental health disorders. These barriers make it hard for such programs to achieve lasting results for those who are not ready for treatment and abstinence. New models and approaches are needed, and have been developed within programs serving this population.
An approach known as Housing First has gained acceptance in recent years because it offers housing immediately without requiring people to stop using substances or start taking psychiatric medications. Housing First offers permanent housing as quickly as possible for people with long histories of homelessness, who often have substance use disorders and co-occurring health challenges. Services in the Housing First approach concentrate on helping people keep their housing and avoid returning to homelessness; addressing the ways that substance use might interfere with these goals is a key component of the approach.
The Housing First approach begins with an immediate focus on helping people get housing. Participation in services is strongly encouraged, but neither sobriety nor participation in services is required as a condition of tenancy. This structure makes it more possible for many people with long histories of homelessness to accept the offer of housing. Services are flexible and individualized, and service providers do "whatever it takes" to help the person achieve goals related to housing stability. Service providers work to motivate reductions in harmful substance use and steps toward recovery, instead of requiring people to complete a substance use disorder treatment program first. Service providers may offer help with practical needs (including food, clothing, household supplies) and work to establish a trusting relationship before expecting that a person will engage in treatment or more-intensive case management services. Peer-based recovery services are often offered and may emphasize consumer empowerment and self-direction.
Case Management and Care Coordination
In addition to the services that directly focus on medical and behavioral health conditions, some of the core services that people living in PSH receive are often described as case management. These services usually begin with a focus on helping people achieve and maintain housing stability. They include coordinating access to medical and behavioral health care services by helping people get to appointments and fill prescriptions; linking people to home health services or to services that provide wheelchairs or other durable medical equipment following a medical procedure or hospitalization; helping people obtain benefits; building skills for independent living; helping to problem-solve relationships with landlords and neighbors; and connecting people to community resources.
For many people experiencing chronic homelessness or living in PSH, Medicaid can pay for some of these services, and a growing number of states and service providers are working to deliver Medicaid services in ways that are accessible and effective. With more people becoming Medicaid beneficiaries beginning in 2014, states are strengthening their health care delivery systems, developing ways to provide appropriate Medicaid benefits for beneficiaries' medical and behavioral health care needs. As states make these changes, there will be greater opportunities to deliver Medicaid-covered health care and behavioral health services for people experiencing chronic homelessness and those living in PSH.
3.1.4. PSH Compared to Residential Treatment and Institutions for Mental Disease
For purposes of understanding what services Medicaid may be able to support for people who have experienced chronic homelessness who are now living in PSH, it is important to understand the differences between PSH and two other arrangements--residential treatment programs and Institutions for Mental Disease (IMDs).
The primary purpose of PSH is housing to end a person's homelessness. Tenants have leases in their own names or other arrangements assuring the same tenancy rights as any other person with a lease. Tenancy in housing continues according to the terms of one's lease, not on the basis of participation in services. In contrast, clients of residential treatment programs have no tenancy rights, and continue in residence only as long as they participate in treatment.
PSH differs from a residential treatment program in another important way--the tenants' ability to choose the types of care and support they will receive, and from whom. Tenants who live in PSH may choose to participate in various forms of health care and treatment services for which they are eligible, and they may choose whether to receive services from providers who are connected to their housing or from other qualified Medicaid service providers in the community. In contrast, clients of residential treatment programs are there primarily for the treatment, not the housing, which is expected to be temporary until participation in the treatment program ends. Refusal to participate in treatment usually results in termination from the program, including the end of the client's residency in the program.
PSH also differs from IMDs in other important ways, and thus is not subject to some important restrictions in the Medicaid rules that apply to those institutions. The discussion of Medicaid reimbursement for services in PSH often raises questions about the Medicaid payment exclusion for IMDs. Medicaid payment does not extend to services provided to individuals who reside in an IMD, except for services furnished pursuant to the state plan benefit ("inpatient psychiatric services for individuals under 21") or pursuant to an exclusion for individuals age 65 or older who reside in institutions that are IMDs. Medicaid defines an IMD as "a hospital, nursing facility, or other institution of more than 16 beds that is primarily engaged in providing diagnosis, treatment, or care of persons with mental diseases, including medical attention, nursing care, and related services. Regulations also indicate than an institution is an IMD if its "overall character" is that of a facility established and maintained primarily for the care and treatment of individuals with mental diseases.31
Unlike institutions, including IMDs, PSH offers housing in community settings, facilitating engagement and integration into the broader community. Regardless of whether PSH units are apartments scattered throughout the community or in apartment buildings dedicated to providing PSH for people with disabilities who have been homeless, PSH offers person-centered, community-based support, generally meeting the criteria CMS has established to define a home and community-based setting in which some Medicaid services may be provided. The supportive services available to persons with mental disorders who live in PSH may include diagnosis or treatment of medical or behavioral health conditions, but the primary purpose of services in PSH is helping tenants to achieve and maintain stability in housing, not treatment of their mental disease. As already noted, continued tenancy in the housing is not contingent upon participation in supportive services offered by the PSH program or other providers who work with PSH tenants.32
3.2. Summary
PSH is permanent housing; tenants have leases that give them the same rights to live in their apartment as any other person with a lease, for as long as they like. The housing units themselves may be apartments scattered throughout the community, in buildings where all units are dedicated to PSH, or in affordable housing developments that set aside a percentage of all units as PSH. PSH tenants have been homeless, often for long or repeated periods of time, and have one or more disabilities, often accompanied by acute and chronic medical conditions. PSH offers its tenants important supports to help them achieve stability and maintain their tenancy, including engagement, case management and care coordination, a multi-disciplinary approach, holistic integration of services for mental health and addictive disorders, attention to physical health concerns, and approaches that promote the skills needed for living in the community.
4. Medicaid Authorities and Options, Providers and Settings
Federal law defines the types of services that can be covered in states' Medicaid programs, including those services that state Medicaid programs must cover (mandatory services), and those that a state may cover (optional services) in its Medicaid state plan.33 This chapter reviews the statutory authorities under which states may include as covered Medicaid benefits the services needed by people with health and behavioral health needs, including those experiencing chronic homelessness or living in PSH. It describes the legal auspices for the most commonly used approaches through which states can cover these activities, including services provided by FQHCs, those available using Medicaid optional services such as Rehabilitative Services, TCM, and Health Homes, and through HCBS. It also examines the qualifications specified in state Medicaid programs for the types of providers that Medicaid will reimburse, and the settings in which services that qualify for reimbursement can be delivered. Chapter 5 continues discussion of Medicaid benefits to assist people experiencing chronic homelessness or living in PSH with details on the specific services that states may choose to include under the authorities described in this chapter.
4.1. Overview of Authorities and Options
States take several different approaches to using Medicaid benefits to cover the medical and behavioral health services most frequently used by people experiencing chronic homelessness. These include the services that connect homeless people to housing opportunities and the services and supports that people receive to promote recovery and stability and address their ongoing health care needs after they move into housing.
The authorities that states may consider using to cover services for people experiencing chronic homelessness through their Medicaid program are listed below:
- State plan benefits and services: Services delivered by FQHCs,34 and optional state plan benefits such as Rehabilitative services,35 TCM services,36 Health homes,37 and Home and community-based state plan services.38
- HCBS Waiver Programs.39
- Other types of Medicaid waiver programs that may be approved by CMS.40
Services provided under these authorities may be delivered by qualified staff through a variety of structures and use a variety of payment mechanisms, including fee-for-service and managed care. Payment mechanisms are described in Chapter 7. Within the framework of federal laws, regulations, and policies established by CMS, states have significant latitude to define the types and qualifications of providers that may participate in their Medicaid programs as well as where care may be delivered. State professional practice acts are state laws and regulations that define the scope of practice for a particular provider type. These requirements, as well as licensing requirements and professional standards, apply to providers regardless of whether they are paid by Medicaid or other sources of funding.
4.2. Federally Qualified Health Centers
Health Centers, which include HCH programs, generally receive federal grants from the HHS Health Resources and Services Administration (HRSA) to provide comprehensive primary care and preventive services to low-income people in underserved communities. These Health Centers generally also receive Medicaid and Medicare reimbursements as FQHCs.41 States are required to provide FQHC services in the Medicaid program. FQHCs provide primary and preventive health care to individuals who are homeless and others. In addition, FQHCs are qualified to furnish mental health and substance use disorder services.
The majority of Health Center patients have incomes below the FPL. Before 2014, about 40 percent of Health Center patients were Medicaid beneficiaries but more than one-third of them were uninsured. Many uninsured patients served by Health Centers before 2014 became eligible for Medicaid or federally subsidized insurance coverage beginning in 2014.42
HCH programs receive 8.7 percent of total federal funding for Health Centers. The more than 200 HCH programs include grantees operating in all 50 states, the District of Columbia, and Puerto Rico. Some programs are operated by Health Centers that also receive federal funding to serve a general, medically underserved population in a defined service area, while some programs receive federal grant funding to target services to a specific designated population, such as homeless people. In 2012, programs nationwide served over 835,000 patients, of whom approximately 90 percent had incomes at or below the FPL.43
HCH programs funded under Section 330(h) of the Public Health Service Act provide services to people experiencing homelessness, and may continue to provide services for up to 12 months after a formerly homeless person moves into housing. The definition of homelessness used by HHS for purposes of eligibility for HCH services is broader than HUD's definition of homelessness, and includes people who are staying in hotels or doubled up with other households, in addition to people living on the streets, in shelters, and in transitional housing programs. Language included in the FY 2012 Appropriations Act allows HCH grantees flexibility to consider residents of PSH or other housing programs that are targeted toward homeless populations as "homeless" for purposes of continued eligibility for services.44
4.2.1. FQHC Services
FQHCs provide preventive and primary care health services, as required by their federal grant funding. These include, at a minimum, services provided by physicians, physician assistants, nurse-practitioners, certified nurse-midwives, and clinical psychologists or clinical social workers and services and supplies furnished incident to these practitioners' services. FQHCs must also offer "any other ambulatory services" that are included in the state's Medicaid state plan, so additional services such as dental services may also be offered. FQHCs are required to provide health care to all individuals regardless of their ability to pay and are required to be located in geographic areas that have few health care providers. Qualifying Health Centers are reimbursed by Medicaid for care included in their state's Medicaid FQHC benefit that they provide to patients who are Medicaid beneficiaries.
In addition to health services provided by physicians and physician extenders, Health Centers must provide in their package of required primary health services referrals to providers of "other health-related services, including substance use disorder and mental health services." This referral requirement is a minimum; many Health Centers directly provide behavioral health services, including services delivered by psychiatrists, licensed clinical social workers, and other clinicians and paraprofessional staff. Health Centers are also required to provide services that Medicaid is not required to reimburse, including preventive dental services, case management, and services that enable patients to access health services such as transportation and translation.
Health Care for the Homeless Programs
HCH programs have some additional requirements. In addition to basic primary and preventive health services, they must also offer the following:
- Substance abuse treatment, which is often offered through partnerships with other programs, but some HCH programs and other Health Centers offer some of these services directly.
- Case management services.
- Services that enable people to use other Health Center services (e.g., outreach, transportation, and translation services).
- Patient education regarding the availability and proper use of health services.
Mental health services are not a required component of HCH services under federal program rules, but most programs deliver mental health services directly or through partnerships with other providers, and all are expected to make referrals to specialty services including those for mental health care. The text box below shows how one HCH Program, in Skid Row Los Angeles, organizes itself to provide integrated services to the area's many homeless people and people living in PSH.
| JWCH, an FQHC, operates the Center for Community Health in the heart of Skid Row in Los Angeles. The Center is designed to support the delivery of integrated services including medical, mental health, substance abuse, clinical pharmacy, dental, and other services and supports. The building is designed to support interdisciplinary teams working in "pods," so that a primary care provider can walk a client over to a mental health provider for assessment on the same day, and team members can consult with one another. Each team (i.e., each pod) is responsible for a group of patients and uses weekly case conferencing to coordinate care for those with the most intensive needs. In addition to care provided in the JWCH clinic, the program sees patients in clinics located in PSH buildings. |
|---|
When HCH programs provide covered services to Medicaid enrollees, the programs are required to bill Medicaid for reimbursement, but before 2014 most patients were uninsured so the programs could not bill Medicaid for their care. In 2012, over 61 percent of HCH adult patients in the United States did not have any public or private health insurance, and 29 percent were covered by Medicaid.45 In the states that chose to implement the expansion of Medicaid eligibility in 2014 under the provisions of the Affordable Care Act, most patients became eligible for Medicaid coverage based on their low incomes.
Health Centers and HCH programs provide services linked to housing through one or more of the following models:
- Delivering on-site services through home visits or satellite clinics located in or near PSH buildings.
- Operating a clinic that is easily accessible by PSH residents and designed to meet their needs.
- Partnering with a mental/behavioral health service provider to conduct outreach to vulnerable homeless people and deliver integrated care to people experiencing homelessness and residents of scattered-site PSH, creating a multi-disciplinary team of primary and behavioral health care providers.
- Engaging "frequent users" of emergency room care and people experiencing homelessness who are being discharged from hospitals and linking them to permanent housing.
4.2.2. FQHC Providers
Medicaid reimburses qualifying Health Centers and HCH programs for visits with specific types of clinicians, based on a per-visit rate.46 Qualifying providers include:
- physicians, including primary care providers and specialists such as psychiatrists;
- mid-level practitioners, including physicians' assistants and nurse-practitioners; and
- licensed clinical social workers and clinical psychologists.
In addition to Medicaid reimbursement, most FQHCs receive federal grant funding administered by HRSA's Bureau of Primary Care. These grants are authorized by Section 330 of the Public Health Service Act.47 Health Centers must obtain HRSA approval for the scope of Section 330 grant-related projects; the "scope of project" specifies the services, sites, providers, target population(s), and service areas for which federal grant funds have been approved.
4.2.3. FQHC Service Settings
A Health Center's scope of project for HRSA also defines the service sites and services that qualify for Medicaid and Medicare reimbursement, based on the established payment methodology for FQHCs. For FQHCs, a service site is any location where a Health Center grantee provides primary and preventive care services to a defined service area or target population, either directly or through a subrecipient or established arrangement. Particularly for vulnerable populations, including people who are experiencing homelessness and those who are living in PSH, FQHC services may be delivered "outside the four walls" of the Health Center. Service sites may be permanent, seasonal, or intermittent, or delivered by a mobile van, as appropriate to meet the needs of the target population. A service site may provide comprehensive primary care services or may provide a single service such as oral or mental health services.
- Permanent sites are open year-round on a regularly scheduled, full-time or part-time basis. There is no minimum number of hours that services must be available at a site. Some Health Centers and HCH programs operate permanent sites located in or adjacent to PSH, and these sites may operate on a full-time or part-time basis.
- Seasonal sites operate for only part of the year, and are designed to meet the needs of patients who may be mobile and working or living in a location for only part of the year.
- Intermittent sites provide direct primary care services but operate for a short period of time at locations that change frequently to meet the needs of mobile populations, including migrant workers or people experiencing homelessness. For example, potential locations for intermittent sites include shelters, soup kitchens, and encampments.
- A fully equipped mobile van is considered a service site if it is staffed by Health Center clinicians and is providing direct primary medical care or oral health services at various locations.
- Health Centers also often provide activities within their scope of project that are delivered at locations that do not meet the definition of a service site because they are mobile or are conducted on an irregular schedule and offer a limited set of services drawn from the full complement of services defined by the scope of project. Locations may include places where clinicians and project staff go from time to time to seek out, engage, and serve people who are covered under the scope of project and eligible to receive services but who are unlikely to access services at a Health Center, at least at first. These locations, which are outside of the walls of an established site, could include settings in which clinicians engage and provide services to people who are experiencing homelessness or tenants of PSH. Specifying an exhaustive list of such activities and locations as part of a Health Center's scope of project is impractical; a more functional approach is to include general categories of locations and the activities likely to be offered there as part of the approved scope of project.48
4.3. Medicaid State Plan Optional Behavioral Health Benefits--Rehabilitative Services and Targeted Case Management
States can use Medicaid state plan optional benefits to cover most of the Medicaid-reimbursed services delivered in or closely connected to PSH tenants. Most often these are Medicaid's Rehabilitative Services option, but services covered under the TCM option are used as well. This section briefly describes these optional Medicaid benefits that a state could include in its Medicaid state plan and use to cover some of the services for people living in PSH, as well as other people with disabilities who need them.
For people living in PSH, the Medicaid optional benefits most likely to be used to cover the care they receive are those their state defines as mental health or behavioral health services. A SAMHSA publication, Medicaid Handbook: Interface with Behavioral Health Services, contains more detailed information regarding Medicaid coverage for behavioral health services, complementing the information provided in this Primer.49 In addition, a December 2012 Information Bulletin from the CMS Center for Medicaid and CHIP Services provides information regarding services and good practices for individuals with behavioral health disorders.50 The Medicaid Handbook and the CMS guidance may be useful resources for states considering potential uses or changes in Medicaid optional benefits for behavioral health services.
In some states mental health services or behavioral health services are managed through a carve-out arrangement in which the state Medicaid agency may delegate some program administration duties, and potentially some financial responsibility for providing the funds to match federal funding, to another state agency or to counties. Some states have contracted with managed care plans, which are responsible for managing a broad range of mental health or behavioral health services, including many of the services covered by Medicaid, for a defined population. In some states the managed care plans are responsible for Medicaid-covered specialty mental health services for the group of people who are enrolled in Medicaid and also meet additional criteria related to SMI. In other states the plans are responsible for behavioral health services for a more broadly defined group of people who may have a range of behavioral health care needs that could be more or less severe, temporary or long term. The scope of services covered through these types of managed care arrangements are specified in agreements between the state and the plans.
4.3.1. Services Under Behavioral Health Optional Benefits
For people who have experienced chronic homelessness, the mental health or behavioral health services that are offered when they live in PSH often include a combination of services that may be covered as Medicaid benefits under the Rehabilitative Services option or TCM.
Rehabilitative Services Option
Medicaid's rehabilitative services option allows states to cover a fairly broad range of recovery-oriented mental health and substance use disorder services to individuals in the community. Coverage for rehabilitative services is authorized by §1905(a)(13) of the Social Security Act, and is defined at 42 CFR 440.130(d) as:
any medical or remedial services recommended by a physician or other licensed practitioner of the healing arts, within the scope of his practice under state law, for maximum reduction of physical or mental disability and restoration of a recipient to his best possible functional level.
To qualify for this option, the service must meet the purposes of "reducing disability and restoring function."51 Examples of specific services that some states cover under this option are described in detail in Chapter 5, Section 5.2.
States can choose to use the rehabilitative services option to furnish behavioral health services (including mental health and/or substance use disorder services) and/or to provide physical health rehabilitative services, such as physical or orthopedic rehabilitation. As of 2013, all 50 states and the District of Columbia covered behavioral health services to some extent under the rehabilitative services option. The majority of Medicaid beneficiaries who receive rehabilitative services are people with mental health disorders.52
The rehabilitative services option can offer states flexibility to cover services delivered in a range of settings, and to provide reimbursement for services delivered by licensed practitioners, paraprofessionals, peers, and teams who meet the practitioner qualifications established by the state, including the state's supervisory requirements and arrangements. Rehabilitative services can be used to help people restore the skills they need to function at home, work, school, and in the community.
TCM
TCM services are defined at 42 CFR 440.169 as "services furnished to assist individuals, eligible under the state plan in gaining access to needed medical, social, educational and other services." States may target the TCM benefit to specific beneficiary groups. Targeted beneficiary groups can be defined by disease or medical condition or by geographic regions, such as a county or a city within a state. Targeted populations, for example, could be individuals with HIV/AIDS, tuberculosis, chronic physical or mental illness, or developmental disabilities. TCM is an optional service that states may elect to cover, for which they must get CMS approval through SPAs.
| Examples of TCM Services |
|---|
| A Comprehensive Assessment: Gathering documentation of clinical assessments or medical records; arranging for clinical assessments; conducting a reassessment to identify a client's ongoing needs for medical, social, educational, and other services; completing a written functional assessment; and assisting in determining the client's eligibility for services. |
| Service Plan Development: Working with a client to develop a service plan based on the client's needs as identified in the assessment. |
| Referral, monitoring and follow-up: Conducting activities to help a client obtain services; assisting with linkages to services such as medical coverage and transportation; coordinating services identified in the service plan, including completion of necessary paperwork, monitoring/evaluating services, and determining whether the services were provided as requested and meet the clients' needs; adjusting services as needed and documenting referrals. |
TCM services include a comprehensive assessment and periodic reassessment; development and periodic revision of a specific care plan; referral and linkage activities; and monitoring and follow-up activities. The services could include assistance in finding housing or linking people with other needed services and supports, but Medicaid TCM services do not include the direct delivery of underlying medical, educational, social, or other services to which an eligible individual has been referred. The text box provides some examples of assistance that may be part of TCM services.
4.3.2. Providers of Behavioral Health Services
In general, state policies determine which individuals, organizations, or facilities are qualified to diagnose and treat mental illness or substance use disorders, within the scope of applicable state laws and professional licenses. Some of the services that may be delivered in PSH, including mobile services that may be delivered through home visits, are likely to be subject to these state laws and requirements. Individuals who are not licensed--including many social workers, case managers, community support paraprofessionals, and peers--deliver many of the services that are provided to people living in PSH, including some of the services that can be reimbursed by Medicaid. States may establish specific requirements that determine who is eligible to deliver covered services, and these requirements may specify the type of training and supervision that these workers must receive for the services they provide to qualify for Medicaid reimbursement.
Some state plan rehabilitative services can be performed by individuals who are not licensed under professional scope of practice laws, including paraprofessionals and peers, as long as they have training and experience consistent with the requirements established by the state and work under the supervision of a licensed mental health professional.
Unlike clinic or outpatient hospital services, for which treatment location is included as part of the service definition, many of the benefits provided under the state plan rehabilitative services benefit can be delivered in a variety of settings, including the consumer's own home or another living arrangement. This makes it possible to deliver and use Medicaid reimbursement to pay for state plan rehabilitative services for people living in PSH or other settings where people experiencing chronic homelessness can be served.
Peer Support Providers
Many Medicaid state plans include peer support providers as a distinct provider type for the delivery of counseling and other support services to Medicaid-eligible adults with mental illnesses and/or substance use disorders. Under Medicaid, peer support providers include self-identified consumers who are in recovery from mental illness and/or substance use disorders. Peer support providers can be effective in engaging and building trust with consumers, motivating change, reducing stigma, facilitating community integration, and serving as role models for the opportunity to live a fulfilling and productive life.
In 2007, CMS provided guidance to states interested in covering peer support services under their Medicaid program.53 The CMS guidance recognizes the value of including peer support services as a component of a comprehensive mental health and substance use service delivery system, and provides more information about requirements for supervision, care coordination, and minimum training criteria.
Medicaid-reimbursed peer support services furnished by peer support specialists may be covered as a service under state plan rehabilitative services or HCBS for people with mental health and/or substance use disorders. Supervision must be provided by a competent mental health professional. Peer support services must be coordinated within the context of an individualized plan of care (POC) that includes specific individualized goals for participants. Peer support providers must complete training and certification as defined by their state to ensure that they have the basic set of competencies needed to support the recovery of others.
Among the new directions in integrating health and behavioral health care (discussed in Chapter 5, Section 5.5) is the use of peer support specialists as part of integrated health teams. Peer support specialists working in this context promote outcomes of integrated health self-management and skills that help people manage situations that might once have caused a crisis leading to hospitalization or other emergency care. The Center for Integrated Health Solutions has developed training for people interested in becoming "whole health and wellness coaches," called Whole Health Action Management. Georgia's Medicaid program includes coverage for whole health and wellness peer support provided by certified peer specialists. At least 29 additional states and the District of Columbia have added certified peer specialists to their Medicaid programs.54
4.3.3. Settings for Medicaid Rehabilitative and TCM Services
Unlike clinic or outpatient hospital services, for which treatment location is included as part of the service definition, many of the benefits provided under the state plan rehabilitative services benefit or TCM services benefit can be delivered in a variety of settings, including the consumer's own home or another living arrangement in the community. This makes it possible to deliver and use Medicaid reimbursement to pay for rehabilitative and TCM services in PSH or other settings where people experiencing chronic homelessness can be served.
Settings for Medicaid Substance Use Disorder Services
A common exception to the flexibility of service delivery locations occurs in some states with respect to services for substance use disorders. Under the rehabilitative services option, states may offer services to address substance use disorders. These services may be offered as an aid in recovering from co-occurring mental illness and substance use or, more rarely, as services for people with a substance use disorder but without a mental illness. These services are critically important to people experiencing chronic homelessness or living in PSH, as a very high percentage of them have problems with alcohol, drugs, or both.
Many states specify that all or most Medicaid-covered services to address substance use disorders must be delivered in clinics or in certain types of facilities that the state certifies as treatment programs. These policies may limit the potential for Medicaid reimbursement for substance use disorder services to people experiencing homelessness or living in PSH that are fully integrated with other health care or mental health services covered by Medicaid, including services delivered by multi-disciplinary teams that are mobile or based in PSH settings.
| States have the authority to allow a wide variety of service locations, including in people's own homes. Federal law and Medicaid program rules do not limit settings for delivering services to address substance use disorders. |
|---|
Some individuals with serious substance use disorders are more comfortable receiving services in their own home or community. Substance use services delivered outside a clinic, in turn, help people experiencing chronic homelessness and PSH tenants in numerous ways. They are designed to reduce health-related risks and other harms related to substance use, to help people get and keep housing, and to increase their motivation to take steps toward recovery, including engagement in treatment and self-help programs. Provisions in Medicaid state plans that restrict service delivery sites for substance use disorder treatment can limit the potential for using Medicaid to finance some of the services that are most often provided to achieve the goals just noted.
Medicaid specifications of service locations are state policy decisions. Federal law and Medicaid program rules generally do not impose limits on the settings in which some types of substance use disorder services can be delivered, including services that could be included as a component of covered rehabilitative services, Health Home, or HCBS. However, state plan rehabilitative services may only be furnished in noninstitutional community-based locations. States could merely describe their covered services and not ascribe a location for their delivery.
4.5. Other Medicaid Waivers
A Medicaid waiver is an agreement between a state and the Federal Government that exempts the state from certain provisions of federal law. Sections 1915 and 1115 of the Social Security Act define specific circumstances under which CMS may approve a state's waiver requests. For example, most Medicaid benefits must be made available on a statewide basis, but a Medicaid waiver can allow a state to waive "statewideness" in order to implement some changes or offer some benefits in only part of a state.
Medicaid waivers under Section 1915 or 1115 allow some states to partner with managed care organizations or health plans to administer some of the benefits covered under their Medicaid state plan. Medicaid 1915(b) waivers allow states to implement managed care plans that may restrict the types of providers that people may use to get Medicaid benefits. A 1915(b)(3) waiver allows a state to use the savings achieved by a managed care delivery system to provide additional services. If a managed care delivery system is able to save money by improving care coordination and integrating services for people with complex health needs, this type of waiver will allow the state to use some of its savings to provide additional services, including services that are not explicitly part of the Medicaid state plan. An example of one state's use of this waiver appears in the text box on this page.
| Michigan used a 1915(b)(3) waiver to implement a managed care delivery system for Medicaid mental health and substance use disorder services, and to obtain approval to use savings for additional waiver services. Community Living Supports are covered among the additional waiver services and supports the state has made available to Medicaid beneficiaries whose needs exceed the benefits available from a Medicaid Health Plan. Community Living Supports are part of the services delivered in PSH for some people with mental illnesses who have experienced chronic homelessness. |
|---|
As described earlier, Medicaid 1915(c) waivers allow states to cover HCBS for people who would otherwise qualify to receive institutional care.
Section 1115 research and demonstration waivers can be used to give states broad flexibility to design and test innovative ways to deliver and pay for Medicaid coverage. At the discretion of the Secretary of HHS, an approved 1115 waiver can give a state the opportunity to implement projects that test policy innovations. States can use an 1115 waiver to obtain approval to use Medicaid funding to pay for the costs of services that would not otherwise qualify for federal match (known as "Costs Not Otherwise Matchable") but which further the goals of the Medicaid program. Before passage of the Affordable Care Act, several states used 1115 waivers to obtain Medicaid funding to expand coverage to people who would not otherwise meet Medicaid's categorical eligibility requirements, including adults without children. The waivers for two of these states are described below.
- California's "Bridge to Reform" 1115 waiver allowed counties to expand coverage through a Low-Income Health Program. By providing federal funding to match county spending for medical care provided to previously uninsured patients, this coverage expansion (before Medicaid eligibility expansion in 2014) freed up some county funds to pay for other services, including services in PSH for people who are experiencing homelessness and receiving care in county hospitals and clinics. The Los Angeles County Department of Health Services is paying for services in PSH and partnering with public housing authorities and other local government agencies to create housing opportunities, with the goal of reducing avoidable hospitalizations and emergency room visits and improving access to more appropriate care to produce better health outcomes for people experiencing chronic homelessness.
- Massachusetts has an 1115 waiver that includes provisions allowing the Massachusetts Behavioral Health Plan (the state's Medicaid behavioral health carve-out) to pay for diversionary services to reduce avoidable hospitalizations. These services are delivered through the Community Support Program for People Experiencing Chronic homelessness (CSPECH; described in more detail in Chapter 5).
4.7. Alternative Benefit Plans
For nonpregnant adults ages 19-64 with incomes at or below 133 percent of the FPL (the adult group) who are newly eligible for Medicaid thanks to the expansion authorized by the Affordable Care Act, the law requires states to offer Alternative Benefit Plans.62
States must select a coverage option from four benchmark options in Section 1937 of the Act:
- The Standard Blue Cross/Blue Shield Preferred Provider Option offered through the Federal Employees Health Benefit program.
- State employee coverage that is offered and generally available to state employees.
- The commercial HMO with the largest insured commercial, nonMedicaid enrollment in the state.
- Secretary-approved coverage, a benefit package the Secretary has determined to provide coverage appropriate to meet the needs of the population.
Alternative Benefit Plans must cover the ten Essential Health Benefits as described in Section 1302(b) of the Affordable Care Act.63 As Secretary-approved coverage, states may choose to offer the existing package of benefits covered in the state's Medicaid state plan (the Medicaid benefits available to other groups of individuals who meet categorical eligibility criteria) to people who are newly eligible as members of the adult group. Alternatively, states may elect to provide an Alternative Benefit Plan that covers a package of benefits that will differ in some ways from full plan Medicaid. In some states, an Alternative Benefit Plan may offer a package of benefits or a provider network that is different from the regular Medicaid program.
Alternative Benefit Plans are subject to the requirements of the Mental Health Parity and Addiction Equity Act of 2008. As a result, these plans may offer a package of benefits to address mental health and substance use disorders that is different, and potentially more generous, than the state's full plan Medicaid.64
States are not restricted to design only one Medicaid Alternative Benefit Plan. Alternative Benefit Plans include the ability for states to tailor plans to meet the needs of specific groups of individuals. For example, if a state wanted to provide different benefit packages to a group of individuals in the new adult group that have a specific chronic condition such as diabetes, or a benefit package that includes more comprehensive LTSS for people with complex and disabling health conditions, the state may do so. The state would still need to cover the rest of the adult group in an Alternative Benefit Plan that meets the minimum requirements described in federal rules.
In states that choose to establish an Alternative Benefit Plan that is different from the regular Medicaid program, enrollment in the Alternative Benefit Plan is voluntary for some groups of people, including some members of the newly eligible adult group. An individual who is medically frail or otherwise considered to have special medical needs must be offered the alternative to participating in an Alternative Benefit Plan by enrolling in the standard approved Medicaid state plan benefit package. Under federal law, individuals with disabling mental disorders, chronic substance use disorders, or serious and complex medical conditions are included among those who are considered to be medically frail.
4.8. Summary
This chapter has focused on ways that states can use various Medicaid authorities to include as covered Medicaid benefits the services needed by people with complex and interacting health and behavioral health needs, including those experiencing chronic homelessness or living in PSH. It described the legal auspices for the most commonly used approaches through which states can cover services needed by this population, as well as requirements for providers and settings. In addition to services provided by FQHCs, the authorities include the Medicaid state plan options of Rehabilitative and TCM services, and HCBS, either in the state plan or in a waiver program. States are slowly beginning to exercise the additional options available under the Affordable Care Act to establish one or more Health Homes to provide care coordination and integration to targeted populations with complex needs. The Health Home option seems especially promising as a way to provide the care coordination and service integration that proves so valuable for very vulnerable populations.
States may find it advantageous to re-examine their provisions for the settings in which particular types of care may be delivered and who is authorized to deliver them. Innovative models of care focus on serving people in the community or in their own homes rather than in clinic or treatment settings--a model of service delivery particularly suited to people experiencing chronic homelessness or living in PSH. Accommodating Medicaid state plans to this mode of service delivery for primary care, mental health care, and services to address substance use disorders would go a long way toward the goal of providing the integrated care that is most likely to achieve the best outcomes for this population. Movement is also occurring in the direction of reimbursing care delivered by properly certified and supervised peer support personnel. Peer support staff often have the greatest success in building trust and helping clients move toward full participation in treatment activities that lead to recovery.
When considering the options and authorities that may be used to cover services available to people who experience homelessness or live in PSH, it is important to keep in mind two basic requirements of the Medicaid program--freedom of choice and comparability. In general, Medicaid requires that beneficiaries have free choice of providers for benefits covered under the Medicaid program. This means that people living in PSH can opt to receive services from a qualified provider of their own choosing, whether that service provider is affiliated with the housing program or not. One possible exception is when states implement managed care arrangements, for which they often obtain Medicaid waivers that limit plan members' free choice of providers to those that are affiliated with the beneficiaries' managed care plan.
Also in general, Medicaid services covered in a state plan must be comparable for all beneficiaries, meaning that benefits available to one group of individuals may not be less in amount, duration, or scope than the benefits available to other individuals who meet similar medical necessity criteria.65 This means that Medicaid services cannot be limited to persons who are living in PSH, if these services are not also available to other Medicaid beneficiaries who need them, as determined by the medical necessity criteria established by the state for these services. There are some exceptions to Medicaid's comparability requirements, and some optional benefits (such as TCM or health home services) or waiver services may be targeted to specific groups of beneficiaries, with CMS approval. Chapter 6 provides more information about the criteria states may use to specify who is eligible to receive some Medicaid services.
5. Defining Medicaid Benefits and Services
This chapter describes the many services that Medicaid can cover to address the health and behavioral health care needs of people experiencing chronic homelessness and those living in PSH. These Medicaid-reimbursed health care and supportive services help people with disabling health conditions, including those who have experienced chronic homelessness, to recover and to live in community settings. Many states use Medicaid benefits to provide health care and some of the supportive services that help vulnerable people get and keep housing. With housing and supports, this population is able to avoid or change very costly patterns of service utilization, including frequent and avoidable emergency room visits, hospitalizations, and stays in nursing homes, detox facilities, or other types of inpatient or institutional care.
Because Medicaid is implemented through partnerships between states and the Federal Government, every state's Medicaid program is different. Within the definitions and guidelines provided by federal law and CMS, states have substantial flexibility in determining which optional Medicaid services to cover, and in defining Medicaid-covered services in state Medicaid plans and programs. This flexibility results in much variability among states in the approaches they have taken to defining the covered services that are available to people who experience homelessness or live in PSH. This chapter takes a closer look at some of the Medicaid benefits and services that some states have defined in ways that make it possible to cover some of the services provided in PSH or in other settings for people experiencing chronic homelessness, assuming those beneficiaries meet applicable criteria for medical necessity or service eligibility. Benefits and services potentially covered include FQHC services, rehabilitative services, case management services, and HCBS. The chapter stresses the importance of including in covered activities the supports that provide the "glue" that holds it all together for clients with complex needs--collateral contacts, case consultation, and multi-disciplinary team conferencing and interactions.
5.1. Federally Qualified Health Center Services
Health Centers and HCH programs often provide services that can be linked to housing assistance for people who experience chronic homelessness. Some organizations operate Health Centers that receive Medicaid reimbursement as FQHCs and also develop and operate affordable housing and PSH, using other sources of funding to pay for housing costs. Other FQHCs establish collaborative partnerships with housing providers, or help their clients obtain housing assistance administered by public housing authorities or other agencies. FQHCs deliver services to PSH tenants through one or more of the following models:
- Deliver on-site services through home visits to PSH tenants or satellite clinics located in PSH buildings.
- Operate a clinic that is easily accessible by PSH residents and designed to meet their needs.
- Partner with a mental/behavioral health service provider to create a mobile, multi-disciplinary team of primary and behavioral health care providers that conducts outreach to vulnerable people and delivers integrated care to people experiencing homelessness and residents of scattered-site PSH.
- Engage "frequent users" of emergency room care and people experiencing homelessness who are being discharged from hospitals and link them to permanent housing through partnerships with housing providers.
Health Centers may use multiple financing mechanisms to develop the capacity to offer a range of services to people with complex needs, including federal grant funding from HRSA, as well as Medicaid payments for services that can be reimbursed through the FQHC mechanism (described in Chapter 7) and obtaining certification to provide mental health or substance abuse treatment services in programs that may be reimbursed separately through state or county contracts, managed care plans, or separate Medicaid payments for covered behavioral health services.
5.3. Case Management
Services provided in PSH are often described as "case management," but Medicaid has its own set of requirements if the state seeks federal reimbursement for TCM state plan services. TCM services are separate from the rehabilitative services benefit. TCM services assist individuals in gaining access to needed medical, social, educational, and other services. A state that intends to target a certain population, such as persons who are experiencing homelessness, must meet all of the applicable TCM requirements including the service definition, requirements regarding the qualifications of the providers, and case records.68 TCM services do not include services that are an integral and inseparable part of another covered Medicaid service or activities that constitute the direct delivery of underlying medical, educational, social, or other services to which an individual has been referred.
TCM includes:
|
|---|
TCM services begin with a "comprehensive assessment" of individual needs to determine the need for any medical, social, educational, and other services. This can include taking the client history and gathering information from other sources such as family members, medical providers, social workers, and others who are qualified to form a complete assessment of the individual. A comprehensive assessment could include information about the following:
- Mental health symptoms and needs as presented in a diagnostic assessment;
- Use of drugs and alcohol;
- Vocational and educational functioning;
- Social functioning, including the use of leisure time;
- Interpersonal functioning, including relationships;
- Self-care and independent living;
- Medical and dental health;
- Financial assistance needs;
- Housing and transportation needs;
- Current living conditions; and
- Other needs and problems.
The next step is to "develop a specific care plan" that is based on the information collected through the assessment. The plan specifies goals and actions to address the medical, social, educational, and other services needed by the individual.
"Referral and linkage" activities may include the following:
- Providing referrals to appropriate housing.
- Communicating with a landlord on behalf of a client.
- Monitoring service delivery through inter-agency consultation and communication, coordination, and referrals.
- Helping clients understand the requirements of programs or services in which they are participating (including a housing program or other community resources) and monitoring a client's progress.
- Assisting a client in making linkages to get needed services.
- Coordinating with other agencies to obtain services for clients.
- Coordinating with discharge planners to facilitate linkages to needed services for a person who is leaving a residential program or hospital.
- Assisting a client to obtain health coverage for medical services.
- Helping a person with linkages to transportation or child care needed to facilitate getting to medical appointments or gaining access to other needed services.
"Monitoring and follow-up activities" may include making contact with the individual, family members, and service providers to ensure that the care plan is implemented and adequately addresses the individual's needs. Related activities may include the following:
- Regularly reviewing the written functional assessment.
- Participating in case conferences to coordinate linkages to services.
- Communicating routinely with the individual or other relevant people about the status of the individual or progress in achieving the goals of the service plan.
- Conducting planning, assessment, record keeping, and documentation associated with service coordination.
- Developing goals, service plans, written service agreements, and routine case supervisory activities, including receiving clinical supervision.
| Case Management Arrangements |
|---|
|
Case management services may also be offered as part of the care coordination functions of Medicaid managed care, or provided as part of the package of services offered by a health home, or as part of a package of HCBS provided through benefits established under Section 1915(i) of the Social Security Act or using a 1915(c) HCBS waiver. These are discussed later in this chapter and in Chapter 7.
5.4. Collateral Contacts, Team Conferences, and Case Consultation
It often happens that a client's case manager or care coordinator must spend time in collateral contacts--talking with a client's primary or behavioral health caregivers, arranging or following up on appointments, conferring with other providers working with the same client, communicating with potential or current landlords, or making other connections on behalf of the client but without the client being present. These activities are essential if case managers are to fulfill their core function for clients with complex health needs, including those living in PSH. For Medicaid beneficiaries with interacting health and behavioral health conditions, care by a multi-disciplinary team is increasingly acknowledged to be an approach of choice that includes team meetings and case conferences as efficient means of communicating about clients and making ongoing care decisions.69 In many states, Medicaid state plans do not include these activities as covered services, but they could do so, and some do.
When they define the services that are components of a broader service such as rehabilitative services, ACT, or TCM, states may include collateral contacts, team conferences, and case consultation when the client is not present, since these collateral contacts or consultations are for the direct benefit of the Medicaid-eligible individual. For example, TCM services include contacts with ineligible individuals who are directly related to identifying an eligible individual's needs and care for the purpose of helping the eligible individual access services; identifying needs and supports to assist the eligible individual in obtaining services; providing case managers with useful feedback, and alerting case managers to changes in the eligible individual's needs. Collateral contacts are particularly important for the population experiencing chronic homelessness, for whom case managers must make ongoing arrangements.
In addition, case conferences are an essential component of team models of care because they provide an opportunity for team members to share information about a client's needs and functioning, and to collaborate in determining how to provide support most effectively to achieve each client's goals.
Including collateral contacts, case conferencing, and team models of care as components of covered services will help to facilitate and provide reimbursement for the work of service providers who are seeking to integrate and coordinate care, help clients access benefits and community resources, and help clients get and keep housing in the community. They have proven to be especially helpful for clients coming from chronic homelessness and those living in PSH, whose histories of erratic and uncoordinated, but expensive, care have not improved their health outcomes and have left them alienated from many systems of care.
5.7. Integrating Primary Care and Behavioral Health Services
A growing number of states and health care providers are involved in efforts to integrate the delivery of primary care and behavioral health services. Efforts to support the integration of primary care and behavioral health services are gaining momentum across the country. In some states, planning or implementation is underway to use new approaches to Medicaid financing to facilitate the integration and coordination of care by using Medicaid Health Home benefits or by organizing networks of health care and behavioral health providers into Accountable Care Organizations (ACOs) or other organized delivery systems. People who have experienced chronic homelessness, including those now living in PSH and those still living on the streets, can benefit greatly from the integrative approaches being developed by health homes as well as other innovative care coordination strategies. Many have the health and behavioral health conditions commonly found among people who have the highest utilization rates for expensive emergency room or hospital care. Experience has shown that inappropriate use of these facilities can be substantially reduced with appropriate models of care coupled with housing.71
In many states, providers are using existing benefits that cover primary care and behavioral health services to work toward service integration. Medicaid financing may be used most frequently for integrated care when services are delivered through partnerships that involve two or more organizations, usually community behavioral health service providers and Health Centers that receive Medicaid financing as FQHCs. In some cases a single organization may operate as both an FQHC and a behavioral health service provider, but these services may function as separate programs within the same organization. For Medicaid financing to support integrated care, it is important that definitions of covered services include activities related to contacts among team members through case conferences or other direct communications to coordinate care for shared clients, as described in Chapter 4. Health home services, which are optional Medicaid benefits described in Section 4.6 of this Primer, can also facilitate the coordination or integration of primary care and behavioral health services.
Integrated care is particularly important to improve health outcomes for people with mental and substance use disorders. For people experiencing chronic homelessness--who often have co-occurring chronic medical conditions, mental health, and substance use disorders, as well as unmet needs for primary and preventive health care--integrated care can be particularly important. When communities and PSH providers work to prioritize access to housing for the most vulnerable people who are experiencing chronic homelessness, primary care and behavioral health services are often integrated in PSH.
5.7.1. Challenges to Integrated Care
State policies that define Medicaid benefits are not always aligned with emerging models of integrated care. States adopt Medicaid program rules and requirements that determine which services or procedures may be provided by individuals, programs, and organizations with specific types of credentials or certification. In most states these definitions of covered services and other requirements related to Medicaid primary care, mental health, and substance use disorder services were developed separately, and these requirements often did not anticipate or provide for integration in the delivery of services by a multi-disciplinary team or through a partnership involving more than one provider coordinating care for the same group of consumers. The lack of consistency in these requirements can create barriers to the delivery of integrated care.
In some states, Medicaid managed care plans are responsible for managing Medicaid benefits for some behavioral health services as well as primary care and other medical care. In other states, Medicaid benefits for primary care, mental health, and substance use disorder services are defined and administered separately, and may be delivered through separate managed care plans or provider networks. Provisions in the contracts between the state and managed care plans may require or help to incentivize collaboration and formal agreements to facilitate coordinated or integrated care, particularly for Medicaid beneficiaries with disabilities or chronic health conditions and co-occurring behavioral health disorders. The example below describes a recent innovative approach to service integration for people experiencing chronic homelessness in Los Angeles County. The approach integrates housing as well as medical and behavioral health services.
To facilitate progress toward integrated care within the Medicaid system, SAMHSA and HRSA, the latter of which administers federally funded community Health Centers, created and support the Center for Integrated Health Solutions to promote the development of integrated primary and behavioral health services.72 The Center promotes integrated care from several perspectives, including integrating primary care into behavioral health settings, integrating behavioral health into primary care settings, examining the promise of health homes under the Affordable Care Act to promote integrated care, and focusing on the needs of specific populations. The ability of providers to be reimbursed for the coordinative aspects of delivering integrated care is a primary concern. The Center provides tools and resources to help states structure integrated care in ways that support Medicaid reimbursement for integrated care, including worksheets that have been developed for each state.73 Each Interim Center for Integrated Health Solutions Billing and Financial Worksheet has been reviewed by the specific state's Medicaid office. With continuing changes in health care financing, states continually review and update their Medicaid state plans and programs. The Center also offers a variety of trainings, one of which is discussed below in relation to peer support specialists.
| Integrated Mobile Health Teams: Housing, Medical, and Behavioral Health Services |
|---|
| The Los Angeles County Department of Mental Health has funded five Integrated Mobile Health Teams using funds provided by California's Mental Health Services Act. Each multi-disciplinary team includes staff from 1-2 community-based mental health service providers and a Community Health Center. Staff work as one integrated team to provide mental health, physical health, and substance abuse services. The partner agencies are working to establish one set of administrative and operational policies and procedures and use an integrated medical record/chart to ensure integrated and coordinated services for people served by each team. Each partner agency obtains Medicaid reimbursement separately for covered services, including FQHC services provided by the Community Health Center and specialty mental health services covered under the rehabilitation option and TCM. The Integrated Mobile Health Team program model is designed to serve people with SMI who also have other vulnerabilities, including age, years of homelessness, co-occurring substance abuse and/or other physical health conditions that require ongoing primary care (such as diabetes, hypertension, cardiovascular disease, asthma or other respiratory illnesses, obesity, cancer, arthritis, and chronic pain). The teams use a vulnerability scale to identify and serve the most vulnerable individuals among those people experiencing homelessness who have a SMI. The team may engage identified individuals through outreach to the streets, encampments, and other locations where many people experiencing homelessness congregate. The team tries to find and engage people with a high level of vulnerability who have not been well-connected to mental health services. Integrated Mobile Health Team services are intended to increase immediate access to housing by using a housing first approach that incorporates harm reduction, motivational interviewing, and access to housing without requirements for treatment, sobriety, or "housing readiness." Each team partners with a PSH developer(s) to dedicate housing units to clients served by the team. With the exception of some administrative activities or medical procedures that require a clinic setting, all team services are delivered in the field, including engaging people experiencing homelessness on the streets and making home visits to people in PSH. |
5.8. Home and Community-Based Services
Medicaid HCBS are most often covered through a 1915(c) waiver or increasingly through optional state plan services authorized by Section 1915(i) of the Social Security Act. Other options include covering personal care through the Medicaid state plan or through a 1915(k) state plan option. HCBS benefits can be used to cover some of the services that connect people with disabilities to housing and provide ongoing support for housing stability and community integration. These services may include the following:74
- Case management/service coordination;
- Homemaker/home health aide;
- Personal care;
- Health-related services, including skilled and unskilled nursing services to address chronic conditions and functional impairments;
- Habilitation;
- Psychosocial rehabilitation services;
- Social supports to participate in community activities;
- Family and caregiver supports, including training and education and respite care;75
- Adaptive services for accessibility, including home modifications such as wheelchair ramps; and
- Other services, including housing locator services.
In January 2014, CMS published a Final Rule regarding Medicaid HCBS.76 The Final Rule specifies that service planning for participants in Medicaid HCBS programs must be developed through a person-centered planning process that addresses health and long-term services and support needs in a manner that reflects individual preferences and goals, including those related to community participation, employment, health care and wellness, and education. The rule describes minimum requirements for person-centered plans developed through this process, which must include an independent assessment of the individual's functioning and needs for services and supports to achieve personally defined outcomes in the most integrated community setting.
Some psychosocial rehabilitation services may be included as HCBS benefits, or covered under Medicaid's rehabilitative services option. Covering these services as HCBS benefits may provide more flexibility for using Medicaid to cover psychosocial services that help people function in community housing, regardless of whether functional impairments are related to mental illness, substance use disorder, or other health conditions. Because HCBS benefits may include habilitation, as well as rehabilitation, these benefits may provide opportunities to deliver services and supports that help people develop new skills for community living, as well as helping to restore skills that have been lost as a result of a disabling health or behavioral health conditions.
For people transitioning to the community from institutional settings, CMS permits coverage for one-time transition expenses under HCBS waiver programs. Community transition services are nonrecurring set-up expenses necessary to enable a person to establish a basic household and do not constitute room and board.77 These expenses may include security deposits; essential household furnishings; set-up fees or deposits for utilities; services necessary for health such as pest eradication, moving expenses, home accessibility adaptations; and activities to assess need, arrange for, and procure necessary resources. Community transition services are furnished only to the extent that they are reasonable and necessary as determined through the person-centered planning process and clearly identified in the service plan.
5.8.1. Supporting Housing Stability with HCBS
A priority need for people experiencing chronic homelessness is access to housing, while the priority for people living in PSH is being able to maintain housing stability. For this to happen, the primary care, mental health care, and substance use treatment that are central to recovery work best if integrated with housing-related services. Provisions to accomplish this integration are built into the community psychiatric support and treatment services offered to participants in Louisiana's PSH Program under the state's 1915(i) SPA78 and include the following:
- Providing restoration, rehabilitation, and support to develop skills to locate, rent, and keep a home; for landlord/tenant negotiations; for selecting a roommate, and for understanding renter's rights and responsibilities.
- Assisting the individual to develop daily living skills specific to managing their own home, including managing their money and medications and using community resources and other self-care requirements.
Louisiana also sought and received approval for amendments to their HCBS waivers to incorporate similar services for any PSH Program clients receiving these services. Medicaid waivers allow states to establish caps for the number of participants who may receive waiver services, and also allow states to waive some requirements related to offering comparable services to all people with similar needs who are enrolled in Medicaid in the state. This allows Louisiana to link eligibility for these services to people who live in a housing unit that is part of the state's PSH program. Wording for this waiver is shown in box below.
| EXHIBIT 5.1. Possible Service Definitions for Two New Housing Services Provided under 1915(c) Waiver |
|---|
| 1. Housing Stabilization Services |
| 2.Housing Transition or Crisis Intervention Services |
Service Definition (Scope): Housing Stabilization Services enables waiver participants to maintain their own housing as set forth in the participant's approved POC. Services must be provided in the home or a community setting. The service includes the following components:
|
| Specify Applicable (if any) Limits on the Amount, Frequency, or Duration of this Service: This service is only available upon referral from the Support Coordinator. This service is not duplicative of other waiver services including support coordination. This service is only available to persons who are residing in a State of Louisiana PSH unit. No more than 72 units of Housing Stabilization Services can be used per year without written approval from the Support Coordinator. No more than 165 units of Housing Transition or Crisis Intervention and Housing Stabilization Services can be used per year without written approval from the Support Coordinator. |
Service Definition (Scope): Housing Transition or Crisis Intervention Services enable participants who are transitioning into a PSH unit, including those transitioning from institutions, to secure their own housing or provide assistance at any time the participant's housing is placed at risk (e.g., eviction, loss of roommate or income). The service includes the following components:
|
| Specify Applicable (if any) Limits on the Amount, Frequency, or Duration of this Service: This service is only available upon referral from the Support Coordinator. This service is not duplicative of other waiver services including support coordination. This service is only available to persons who are residing in a State of Louisiana PSH unit or who are linked for the State of Louisiana PSH selection process. No more than 93 units of Housing Transition or Crisis Intervention can be used per year without written approval from the Support Coordinator. No more than 165 units of Housing Transition or Crisis Intervention and Housing Stabilization Services can be used per year without written approval from the Support Coordinator. |
5.9. Summary
This chapter has described specific service models in detail, including examples from case study sites. These include FQHC services, rehabilitation-oriented services, ACT and similar models, case management, housing support services and strong links with housing programs, and diversionary services.
In adapting their Medicaid programs to cover the services that people experiencing chronic homelessness or living in PSH need, it is important for states to attend carefully to the requirements of Medicaid state plan services and other Medicaid programs. It is particularly important that definitions of medical necessity focus on symptoms, functional impairments, and other indicators of need rather than simply on diagnostic categories. New ways of thinking about vulnerability and medical necessity are evolving and incorporating them into state programs can provide greater flexibility to accommodate the needs of people with complex, interacting health and behavioral health conditions that often do not fit neatly into simple diagnostic categories. We turn to these issues in the next chapter.
6. Medical Necessity Criteria: WHO Can Receive Specific Services?
Chapter 4 described the various statutory authorities under which states could incorporate services important for people experiencing chronic homelessness or living in PSH into their Medicaid programs. It also discussed the provider qualifications and settings in which services may qualify for Medicaid reimbursement. Chapter 5 then examined some specific services and service models included in at least some state Medicaid programs that are being used to serve this population. This chapter examines which Medicaid beneficiaries are eligible to receive the specific services that may be covered by Medicaid, with a focus on the services of most use to people experiencing chronic homelessness or living in PSH. It does so by looking at the medical necessity criteria that a Medicaid beneficiary would have to meet to be eligible for some of the most effective specific services.
In addition to the federal and state policies that determine who is eligible to enroll in Medicaid, states set additional eligibility criteria to determine who, among all of the people who are enrolled in Medicaid, is eligible to receive specific services such as HCBS, health home services, or rehabilitative services. States may consider diagnoses and other health and functional criteria to define medical necessity for these services, and they may use a number of different terms to refer to medical necessity. These terms include level of care criteria or service criteria. Medical necessity criteria are designed to ensure that people with legitimate needs have access to services that are likely to be effective, economical, and appropriate to the illness, injury or type of disability for which the service is being performed.
6.1. Medical Necessity Criteria: Implications for People Living in Permanent Supportive Housing
State policies regarding medical necessity criteria have important implications for people experiencing homelessness and for PSH service providers because these policies determine who qualifies to receive specific Medicaid-reimbursed services. Some people who experience chronic homelessness are likely to have the specific health conditions, diagnoses, and other characteristics that make them eligible to receive some of the services that Medicaid covers, including services that can be delivered in a range of home or community settings outside of clinics or treatment facilities. On the other hand, other people who experience homelessness may not meet the criteria associated with eligibility for these types of services.
6.1.1. Medical Necessity for Rehabilitative Services
In many states, medical necessity for rehabilitative services delivered in PSH or other community settings is limited to people with SMI, particularly for service approaches such as community support or ACT that offer an intensive or moderately intensive level of support.
State plans, and policies that states often incorporate into Medicaid provider manuals or similar guidance, may include specific diagnostic and additional criteria related to service need, or they may simply set forth service descriptions available under the rubric of rehabilitative services. When they include specific criteria, diagnosis and functional impairment are often included.
- The diagnosis criterion, when it is specified, is most often one of the following diagnoses, which may also be accompanied by a co-occurring diagnosis of substance use disorder or developmental disability:
- Schizophrenia;
- Other psychotic diagnosis;
- Bipolar disorder;
- Major depressive disorder.
Some states use medical necessity criteria that include a broader range of mental health disorders. States may use criteria that include additional diagnoses as well as consideration of severity of symptoms or needs, including co-occurring substance use disorders or other health conditions.
- Service need or functional level criteria often take into consideration some or all of the following factors, and admission and continued eligibility criteria for some intensive services are likely to require some combination (often more than three) of the factors:
- Recent and/or multiple psychiatric hospitalizations, emergency room visits, or interactions with law enforcement for emergency services due to mental illness or substance use.
- Inability to participate or remain engaged or respond to less-intensive community-based services.
- Inability to meet basic survival needs, chronically homeless, homeless, or at imminent risk of becoming homeless.
- Evidence of co-occurring mental illness and substance use disorder.
- Suicide attempt or suicidal ideation.
- History of violence due to untreated mental illness or substance use disorder.
- Lack of support systems.
- History of inadequate follow-through with treatment plan, resulting in psychiatric or medical instability.
- Documented inability to sustain involvement in needed services, or evidence that a comprehensive integrated program of medical and psychosocial rehabilitation services are needed to support improved functioning at the least-restrictive level of care.
- Evidence of harm to others, or significant psychotic symptomology such as command hallucinations to harm others.
| LOCUS |
|---|
The LOCUS assesses seven domains, using five-point scales for which a higher score indicates greater need for assistance. The seven domains are listed below:
The assessor rates a person on each domain, and then adds up the scores to get a global score. States that use rating scales vary in the number of levels of care they define and how they match LOCUS or GAF scores to those levels. Levels may be called "tiers," "levels," or simply associate a global LOCUS score or range of scores with particular services. |
As part of the determination of service need, states may require use of a rating scale such as the Global Assessment of Functioning (GAF) Scale or Level of Care Utilization System (LOCUS) (see box above).79 Some states specify certain scores on these instruments as qualifying for different types of service interventions, but these scores are virtually always only one piece of evidence among others considered in the determination of service need. For instance, the District of Columbia requires a global LOCUS score of 20 to qualify for community support services and a score of 24 or higher to qualify for ACT, along with other criteria. In Minnesota, the LOCUS score is converted to a level of care recommendation.
6.1.2. Medical Necessity for Behavioral Health Services: Broadening the Definition
Some people who experience chronic homelessness have mental health conditions such as depression, anxiety, or trauma, and they also have co-occurring substance use disorders or cognitive impairments resulting from brain injuries. Yet the conditions they have may not be considered to be SMI and therefore will not meet the medical necessity criteria adopted by states for mental health services. These individuals may have significant impairments that interfere with their ability to get and keep housing, avoid crises, and manage chronic health conditions, but they do not qualify to receive rehabilitative services or other mental health services covered by Medicaid in some states, or they may be eligible to receive only a more limited set of benefits such as mental health assessment or crisis intervention.
To accommodate the realities of multiple co-occurring chronic conditions that are common among people experiencing chronic homelessness, some states use broader medical necessity criteria for eligibility for some services than the specific diagnoses that are recognized as SMI. For example, in Massachusetts the services provided by the Community Support Program to End Chronic Homelessness are covered under a Medicaid waiver as "diversionary services" and available to people enrolled in the Medicaid program (MassHealth) who have mental health and/or substance use conditions or are at increased medical risk, and experiencing chronic homelessness. The services are designed to respond to the needs of people at high risk of hospital admission. Clinical criteria to establish medical necessity for the Massachusetts program appear in the box below.
| Massachusetts: Clinical Criteria to Establish Medical Necessity for Diversionary Services |
|---|
|
6.1.3. Eligibility for HCBS 1915(i) State Plan and 1915(c) Waiver Services
States define eligibility for Medicaid HCBS so they can target these services to people who are, or might otherwise be, receiving care in nursing homes or other institutional settings, or to people who need HCBS so they can live independently in community settings.
As described earlier in this chapter, Section 1915(c) waivers are used to provide HCBS to individuals who meet the criteria for an institutional level of care. To qualify to receive services under a HCBS waiver, a person must be disabled and qualify to receive care in a nursing home or other institutional setting. Growing numbers of people experiencing chronic homelessness are older adults with health conditions that put them at risk for needing nursing home care if they are unable to get support and move into more appropriate housing. In addition, nonelderly people with disabilities who experience chronic homelessness may be discharged from hospitals to nursing homes because they do not have a place to live and are unable to care for themselves following a health crisis. If such individuals also have access to affordable housing, HCBS may be an appropriate way to ensure that they make the transition to community living successfully. While people experiencing chronic homelessness have not been a significant part of the population receiving HCBS covered under waivers in many states, it is likely that some of these individuals qualify to receive these services.
HCBS 1915(i) state plan services can be provided to people with disabilities who do not need institutional care. This makes these services potentially available to people with a broader range of disabling conditions and levels of functioning. A state must establish needs-based criteria for determining an individual's eligibility for 1915(i) HCBS, and must develop an independent assessment process that determines the necessary level of services and supports to be provided to each individual. The independent assessment cannot be provided by the same organization that delivers the HCBS.
In the design and implementation of eligibility criteria for a HCBS waiver and state plan services covered under Sections 1915(c) and 1915(i), states should consider issues related to the continued eligibility of participants to receive the services they need to live successfully in integrated community settings such as PSH. For many people who have experienced chronic homelessness, their health and functioning will improve after they move into stable housing and receive appropriate health care and supports. As they recover they may no longer qualify to receive institutional care, and as a result they no longer qualify for the 1915(c) HCBS. Continuity of care can be facilitated if the PSH providers delivering support to the individual are qualified to deliver both HCBS 1915(c) waiver and 1915(i) state plan services. As determined by an independent assessment and the individually identified goals and preferences reflected in the person-centered POC, less-intensive ongoing services and supports could be made available through 1915(i) for people who no longer qualify to receive the HCBS waiver.
6.1.4. Eligibility for Health Home Services
Section 2703 of the Affordable Care Act allows states to elect to provide optional health home benefits under the state's Medicaid plan. The health home provision authorized by the Affordable Care Act provides an opportunity to build a person-centered system of interdisciplinary care to improve outcomes for beneficiaries with chronic health conditions, while also providing value to state Medicaid programs.
Medicaid health home benefits can be made available to Medicaid beneficiaries with:
- two or more chronic conditions;
- one chronic condition and who are at risk for a second; or
- a serious and persistent mental health condition.
All people served with Medicaid health home benefits must meet the minimum criteria described above, which are set by federal law.
As part of a SPA to add these benefits, states may designate particular chronic conditions and eligibility criteria. For example a state might target these services to people with higher numbers or severity of chronic health conditions, or higher costs that might be associated with frequent and avoidable use of hospital emergency and inpatient care. In defining the population eligible for health home services, a state might choose to use eligibility criteria that incorporate the chronic conditions that are often found among people experiencing chronic homelessness. These include mental health and substance use disorders, diabetes, asthma, and heart disease. In addition, states may request CMS approval to base eligibility on additional or different chronic conditions, including conditions that occur at high rates among people experiencing homelessness. These might include Hepatitis C, liver disease, and HIV/AIDS. A state might also request CMS approval to incorporate measures of vulnerability or chronic homelessness into criteria used to determine the severity of chronic health conditions.
Eligibility for health home services cannot be limited based on other factors such as age, use of a specific delivery system, or category of aid. States may not exclude people who are eligible for both Medicaid and Medicare (dual eligible beneficiaries).
Section 1945(f) of the Affordable Care Act requires states that implement Medicaid health home programs to track avoidable hospital readmissions. States are also expected to track emergency room visits and skilled nursing facility admissions. A substantial body of evidence shows that for people experiencing chronic homelessness, PSH is associated with reductions in hospital admissions and emergency room visits.80 There is also some evidence that PSH is associated with reductions in admissions to skilled nursing facilities for people with chronic health conditions who are experiencing homelessness.81 States that establish Medicaid health home programs using eligibility criteria that include people experiencing chronic homelessness, and link these services to housing opportunities, may be able to achieve significant reductions in avoidable hospital readmissions.
6.1.5. Targeting Services to Frequent Users of Crisis Health Services to Decrease Costs and Improve Outcomes
Innovative health care providers and their partners have developed promising approaches that target new models of care delivery to Medicaid beneficiaries with complex health issues and a history of frequent encounters with health care services in hospitals and institutional settings--sometimes called super-utilizers.82 A disproportionate share of all health care spending is used to provide care for a relatively small group of patients, with just 5 percent of Medicaid beneficiaries accounting for 54 percent of total Medicaid expenditures, and 1 percent of Medicaid beneficiaries accounting for 25 percent of total Medicaid expenditures. Most of these high-cost Medicaid beneficiaries have multiple chronic health conditions, often including co-occurring mental health and/or substance use disorders, and some are experiencing homelessness.83
Some states are designing or considering health home benefits to provide more cost-effective, coordinated care for these frequent users, potentially targeting health home benefits to the highest-cost beneficiaries with the most severe conditions or the greatest number of chronic or mental health conditions.84 States could also structure payment methodologies to incentivize health homes to deliver more-intensive care management services to the most complex patients who have the greatest need. These approaches are likely to include some of the most vulnerable people who are experiencing chronic homelessness.
6.1.6. Accommodating Changes in Service Needs and Eligibility as People Recover
States often define medical necessity or service eligibility criteria for continued eligibility for some types of services, as well as the initial admission criteria. Criteria for continued eligibility will be different from criteria for admission to services, allowing people whose health and functioning is improving to remain eligible to receive services and supports they need to maintain stability and continue in their recovery.
As people who live in PSH recover and as their functioning improves, they may no longer have symptoms or impairments that meet medical necessity criteria for continued eligibility for services they needed when they were experiencing homelessness or when they first moved into housing. In developing strategies to finance services for people living in PSH, providers and funders need to anticipate that the needs of tenants may change over time, and some tenants may no longer have a medical necessity for some of the Medicaid-covered services that can be delivered in a PSH setting. This can create challenges for some people living in PSH, particularly if they have established trusting relationships with service providers and have come to rely on the availability of supports that help them maintain stability, manage chronic and disabling health conditions, and anticipate and respond quickly to relapse.
States may use more than one Medicaid benefit package to provide the range of services that help people with disabilities who have experienced homelessness live successfully in the community. Doing so would make it easier to ensure continuity of care to beneficiaries whose health conditions and functioning change over time. If the services that support community living include varying levels of intensity, available through several elements of a state's Medicaid program that all provide benefits for people with complex health needs, a person could potentially shift seamlessly from coverage under one benefit package to services available under a different one as needs change over time. To ensure maximum continuity of care it is also important that the same provider or team of providers is able to deliver the new level of supports. To make this possible, it is advisable that the providers available to this population include health professionals who meet the qualifications established by the state and set forth in the Medicaid state plan or waiver program.
Because the nature of mental illness may include worsening of symptoms and functioning from time to time as well as the types of improvements just discussed, it is important that Medicaid structures facilitate periodic changes in care levels to increase as well as decrease the intensity of care. The ability to modify individual care plans as needed is also an important factor in successful supports for people with complex health conditions who experience chronic homelessness. When an individual first accepts care and works with program staff to develop an individual treatment plan, he or she may not reveal, or may not be ready to work on, some aspects of recovery and may not be willing to have them included in the treatment plan. Providers need to have the flexibility to add components to an existing plan or modify components that are already there and know that they will be able to receive Medicaid reimbursement for the additions and modifications as long as the need for them is appropriately documented.
6.2. Considerations for State Policymakers and Their Partners--New Ways to Think About Vulnerability and Medical Necessity
Unintended consequences may arise when states include specific types of disabilities or diagnoses in the definition of medical necessity for rehabilitative services or other optional Medicaid benefits that cover the services that can be delivered in PSH. One of these consequences may be to create incentives for housing providers to establish tenant selection criteria that incorporate specific types of disability, to ensure that the person qualifies to receive services that are covered by Medicaid so the PSH service provider can be reimbursed for the services delivered to the person living in PSH.
To facilitate the use of Medicaid reimbursement for services that can be delivered in PSH to vulnerable people who are experiencing chronic homelessness, states should align Medicaid reimbursement for services with the rules that govern housing assistance. This applies for states considering adapting medical necessity criteria for these services that focus on symptoms, functional impairments, and indicators of need that can be assessed consistently, regardless of the specific diagnoses or conditions that contribute to the symptoms or impairments. Taking this approach, a state could choose to provide Medicaid-covered rehabilitative services to a person who has cognitive impairments and difficulties with interpersonal and community coping skills that result from a brain injury, trauma, and a co-occurring serious substance use disorder, regardless of whether the person also has a diagnosis included in the definition of SMI.
| Focus medical necessity criteria on symptoms, functional impairments, and indicators of need rather than on diagnoses. |
|---|
In a growing number of communities, providers of health care, housing, and homeless assistance services are working together to prioritize access to PSH for the most vulnerable people experiencing chronic homelessness, including people living on the streets who are at greatest risk for mortality or those who most frequently use high-cost health care services in hospitals and institutional settings. Some of these vulnerable adults are people with a mental illness serious enough to qualify them to receive rehabilitative services. However, some people who experience chronic homelessness need similar services because they have complex, co-occurring health and behavioral health conditions that can result in avoidable hospitalizations or other crisis and institutional care. But because they do not have a SMI, they have not been able to access the intensive, face-to-face case management and interventions being used in models of care that Medicaid reimburses as rehabilitative services if state policies make these services available only for people with SMI.
A further consideration is the need of many people experiencing chronic homelessness to learn new skills as part of adjusting to living stably in housing in the community. In Medicaid terminology learning new skills--ones the person has never known how to do--is designated "habilitative" to distinguish it from rehabilitation, or relearning things that were once within the person's skill set but have been lost.85 Habilitative services are not covered under Medicaid's rehabilitative services option. However, if a state includes habilitation as part of its service definitions approved by CMS under these authorities, it may be part of services delivered under a HCBS waiver (1915(c)) or 1915(i) SPA, or as part of health home services or some other types of benefits. Innovative care coordination models often include helping clients learn new skills in addition to their attention to health and behavioral health care, as they promote the development of interpersonal and community coping skills and habits that prevent crises that might otherwise lead to hospitalizations, institutional care, or the loss of housing in the community. This chapter has described how some states are incorporating care coordination models for this population without SMI into their Medicaid programs. Other states could make similar changes, following or adapting these examples to their own situations to achieve the same effects.
6.3. Summary
This chapter has examined the medical necessity criteria established by states that determine which Medicaid beneficiaries may receive specific services that have proven to be most efficacious in addressing the health and behavioral health needs of people experiencing chronic homelessness or living in PSH. It reviewed medical necessity criteria for behavioral health services covered under Medicaid's rehabilitative services option, HCBS under waivers or SPAs, and the opportunities now available through health homes. Exhibit 6.1 summarizes this discussion.
The chapter then described: (1) new ways to think about medical necessity--beyond diagnosis--and how these new ways of thinking may be used to serve the most vulnerable beneficiaries; (2) the value of targeting services to the most vulnerable, and ways that states' Medicaid programs could accomplish this goal; and (3) the desirability of smoothing transitions for people whose conditions change in such a way as to alter their eligibility for the specific level of care they have been receiving. States have the opportunity to shape their Medicaid state plan to increase the number of people who are or have been experiencing chronic homelessness for whom the answers to Exhibit 6.1's questions are "yes." Focusing on these themes could help states tailor the services in their Medicaid programs to maximally benefit people experiencing chronic homelessness or living in PSH, with the added benefit that others with complex interacting health and behavioral health conditions would also benefit.
| EXHIBIT 6.1. Eligibility for Different Medicaid Services | ||||
|---|---|---|---|---|
| Step 1: Are you eligible for Medicaid? |  | NO | No Medicaid services | |
 | | |||
| YES, categorically (SSI, children, pregnant women, certain family members) | YES, income-eligible in states that expand Medicaid eligibility | |||
| | |||
| Eligible for full Medicaid state plan | Eligible for Alternative Benefit Plan (which may be the same as full Medicaid state plan) | |||
| Step 2: Do you meet medical necessity criteria for specific services that work for PSH tenants?[Medical necessity criteria for specific services vary by state.] | | NO | Still eligible for other Medicaid services | |
| | |||
| YES, by having a SMI | YES, by having a disability/condition that meets medical necessity criteria specified in your state's Medicaid plan for 1 or more specific services (e.g., HCBS, health homes) | |||
| | |||
| Eligible to receive rehabilitative and/or other behavioral health services under several Medicaid options, if included in your state's plan | Eligible to receive specific services (e.g., health home services) | |||
| Step 3: Do you receive this care from a qualified Medicaid provider? | | NO | Medicaid will not cover the cost of this care | |
| ||||
| YES, Medicaid will cover the cost of covered services for which you meet medical necessity criteria | ||||
7. Medicaid Payment Mechanisms and Innovative Service Delivery Structures
This chapter begins with a review of the basic fee-for-service payment mechanisms and payments for FQHCs that have been used most frequently to provide Medicaid reimbursement for services to people living in PSH. Next, the chapter focuses on Medicaid managed care. While new payment mechanisms are being developed, these three mechanisms will likely be the ones used for years to come to pay for the most services for the greatest number of PSH tenants and people currently experiencing chronic homelessness. Thus it is important to understand how these payment mechanisms work for the PSH-eligible population and how states can use them to respond to this population's needs.
The last half of this chapter focuses on emerging models of payment reform that are tied to changes in health and behavioral health care delivery systems and approaches to care coordination. These include health homes, "super-utilizer" programs, ACOs, and other mechanisms to pay for care coordination. Some of these innovative approaches offer potential for achieving better health outcomes as well as cost savings associated with PSH residents with long histories of homelessness who have complex health care needs. The Federal Government considers several of these alternatives so important for saving Medicaid dollars that the Affordable Care Act includes incentives to states that adopt them.
7.1. Medicaid Fee-For-Service Payment Mechanisms
Until recently, most people with disabilities who were enrolled in Medicaid, including people experiencing homelessness and those who became tenants of PSH, have received health care and behavioral health services reimbursed through fee-for-service arrangements. As many states expand Medicaid managed care structures and explore payment reform and health care delivery system changes, some of these fee-for-service arrangements are changing, but many providers of health care and behavioral health services are likely to continue to receive fee-for-service payments for Medicaid-covered services. Financing for the Medicaid-covered services that can be delivered in PSH has most frequently been provided through the fee-for-service payment mechanism.
Under fee-for-service, qualified Medicaid providers are paid for each covered service such as an office visit, test, or procedure according to rates set by the state. States may develop their payment rates based on: (1) the costs of providing the service; (2) a review of what commercial payers pay in the private market; or (3) a percentage of what Medicare pays for equivalent services.86 The service provided must correspond to the description of covered services under the Medicaid state plan, and the service must be delivered by a qualified Medicaid provider.
7.1.1. Fee-For-Service Payment Arrangements
If they are Medicaid beneficiaries, people experiencing homelessness or living in PSH often receive covered services for medical conditions in the same way as any other beneficiary does, from clinics, doctors, and other qualified providers. These health care providers may receive payment from the Medicaid program on a fee-for-service basis, with rates that are established for specified procedures or types of encounters. Alternatively, health care providers may be compensated through other payment arrangements, such as capitation, if beneficiaries are enrolled in Medicaid managed care plans.87
Many people who are or have been chronically homeless receive Medicaid-covered behavioral health services, such as rehabilitative services or HCBS (described in Chapter 5), including services that are connected to PSH and services they may receive from other providers in the community. These services are often reimbursed with fee-for-service payment. In many states, in order to qualify for payment for some behavioral health services, Medicaid providers must have contracts with public behavioral health departments. Reimbursement for HCBS or behavioral health services is often based on a unit of service, with the covered services and activities and the units of service defined by the state. Units of service may be defined and counted by the minute or quarter hour (15-minute) increment. For some types of services, a unit of service may be a day.
PSH service providers often perform a range of activities, and Medicaid reimbursement is available only for the activities that fit definitions of covered benefits. For mobile services that are delivered in a person's home or in other settings where providers deliver care to homeless people, reasonable travel time for the service provider may be included in the definition of a covered service or unit of service and compensated through fee-for-service payments.
States have the authority to define covered services as including both face-to-face and collateral contacts made by service providers for the direct benefit of an eligible person. For example, depending upon the definition of a covered service, fee-for-service reimbursement may be available for the time a service provider spends obtaining information such as the results of medical examinations or procedures on behalf of a client, or talking with a client's family member or other responsible person (such as a housing provider) to offer advice about how to assist the client. For these types of activities, fee-for-service payment may be available for the units of service delivered (e.g., the amount of time staff perform these activities) regardless of whether the client is present or the contact is face-to-face.
From the perspective of service providers, fee-for-service payment mechanisms offer some advantages when delivering care to people with high levels of need. In general, under fee-for-service, a provider can deliver more covered services to people who need more frequent, intensive interventions during times of crisis, or initially when people are getting engaged in care and stabilized in housing, and be reimbursed for all the care delivered that is justified by medical necessity. With fee-for-service payment, as people recover and need less frequent or intensive services, costs to the Medicaid program are likely to be lower because these individuals need and receive fewer units of service, and resources can be used to pay for services to other people.
There are also some challenges associated with fee-for-service payment. These include administrative burdens associated with providing documentation to back up claims for each covered service delivered or billing for each procedure performed. States have often set up separate systems that include separate groups of providers and separate fee-for-service payment mechanisms for Medicaid-covered services to address medical, mental health, and substance use disorders--and this can make it very difficult for a provider or team to deliver integrated care when they have to use multiple fee-for-service payment mechanisms and those mechanisms are not aligned.
As described in Chapter 5, states could define covered services in ways that provide substantial flexibility for including the supports needed by people with behavioral health disorders or multiple chronic health conditions, including co-occurring mental health and substance use conditions. These conditions may be highly variable over time and in relation to each other, with one requiring a lot of attention at one time and another requiring more care at another time. Providers must be able to work very flexibly with clients to address their issues in an integrated way if they are to achieve the highest level of success.
However, current definitions in many Medicaid state plans may not include some of the activities performed by service providers that have a good track record of achieving better outcomes, including impacting positively on a participant's health, helping to motivate healthy behavior changes, and contributing to more appropriate and less unnecessary use of more expensive services that the Medicaid state plan does cover. Revising current Medicaid state plan definitions of covered services could go far toward enabling providers to serve their PSH tenants and others experiencing homelessness or having complex health care needs more efficiently and effectively, rather than leaving providers without reimbursement for the time associated with those interventions or activities that comprise an integral part of their approach.
States and local mental health authorities can help with efforts to use available Medicaid benefits to pay for some of these services if they provide service agency staff with training tailored to the needs of direct service providers who work in PSH or other home and community settings. It can be very helpful to give workers and service provider organizations clear guidance about how to appropriately document and claim fee-for-service payment for the covered services they deliver. Provider handbooks and training could also reduce the misunderstandings, disputes, and disallowances that can otherwise result if service providers submit claims for time spent on activities that are not included as covered benefits.
When providing payments on a fee-for-service basis, a state may control costs by limiting the maximum number of units of service a beneficiary may receive each month, or require prior authorization for more frequent and intensive services that may be justified on the basis of that person's level of functioning. States may accommodate varying levels of need for these services by setting higher limits on units of service for people with more severe or complex health and behavioral health conditions or other disabilities. For example, states may limit the amount of services that a beneficiary can receive, and then allow providers to request additional services if medical necessity can be justified.
7.1.2. Payment Mechanisms--Daily or Monthly Rates Under Fee-For-Service
A variation on minute-by-minute fee-for-service billing is a daily or monthly rate. Usually, daily or monthly rates under fee-for-service are used to pay for covered services for people with chronic conditions, particularly when a mix of services are delivered over a period of time to achieve goals established in an individualized service plan. Examples of daily or monthly rates for the general Medicaid population would include nursing home daily rates or hospice daily rates. Examples of the services that may be provided to PSH residents and reimbursed with daily or monthly rates include community support services, ACT, and some HCBS under 1915(c) waivers (see Chapter 6 for descriptions).
The daily or monthly rate must be based upon the costs of services that are defined as covered benefits under a state's Medicaid plan or waiver, just as only covered benefits qualify for payment when using billing by the minute or other unit of service, but the provider is spared the work of keeping track of time and activities minute-by-minute. Rates may be established based on time studies that determine the costs associated with the usual or average amount of a covered service that is medically necessary to achieve the desired outcomes and delivered to a qualifying client each day or month. Time studies are usually repeated once a year, often for a month, during which time minute-by-minute tracking is required to verify or adjust the rate.
Daily or monthly rates can be structured to provide more continuity of care than minute-by-minute or procedure-by-procedure billing, particularly if the definition of the covered service that is being billed on a daily or monthly basis is designed to address co-occurring behavioral health disorders or chronic health conditions with a range of activities that restore and support the skills needed for community living, facilitate illness self-management, and coordinate access to appropriate health services and other community resources. For people who are or have been chronically homeless, if service definitions include the supports needed to help them obtain housing and then remain stably housed, daily or monthly rates may allow service providers to focus on doing "whatever it takes" to achieve this goal, while reducing the administrative burden of documenting activities by the minute or quarter-hour.
Daily or monthly rates relieve providers of the administrative burden associated with detailed documentation for activities, but do not in and of themselves promote greater care coordination or an integrated approach to mental health and substance use disorders and other health conditions. Some states have adopted definitions of covered services that do incorporate care coordination, and monthly rates are paid for some of these services.88
- Under Massachusetts's Section 1115 waiver, the Massachusetts Behavioral Health Partnership, the state's Medicaid behavioral health carve-out, has established monthly rates for community support services for people with a qualifying mental illness or substance use disorder. Covered services include providing service coordination and linkage, and assisting with obtaining benefits, housing, and health care.
- Minnesota counties and managed care plans have established monthly rates to pay for TCM services for people with mental illness. These benefits are often used to provide case management services that help Medicaid beneficiaries experiencing chronic homelessness to move into PSH and get connected to other needed services.
Financial incentives for providers operating under daily or monthly rates may be somewhat more oriented toward promoting better health outcomes compared with those that receive payment for visits or procedures under fee-for-service arrangements, particularly if states establish contract provisions that provide incentives for improving health outcomes or shared savings for demonstrated reductions in avoidable hospitalizations or utilization of other high-cost services.
7.1.3. Payment Mechanisms for Community Health Centers that Operate as FQHCs
Before 2014, many of the patients served by Health Centers, including HCH and other programs, were not eligible for or enrolled in Medicaid. In 2012, only 28 percent of HCH patients and about 40 percent of all Health Center patients were enrolled in Medicaid.89 That situation has now changed in states that have expanded Medicaid eligibility, so Medicaid reimbursement policies have become increasingly relevant to these Health Centers.
For patients who are Medicaid beneficiaries, Health Centers typically receive Medicaid reimbursement as FQHCs. Generally, Medicaid payments are provided to these Health Centers on a per-visit basis, using a prospective payment system (PPS). While specifics vary by state, in general an FQHC receives a per-visit payment each time an eligible patient has a face-to-face encounter with a specified type of health care provider, including a physician (primary care or psychiatrist), mid-level (nurse-practitioner or physician's assistant), licensed clinical social worker, or clinical psychologist.90
The FQHC payment methodology for Medicaid beneficiaries is designed to ensure that the costs of treating Medicaid patients are not shifted to federal grant funding that is meant to pay for care to people who are uninsured and for services that are not covered by insurance payments.
For several reasons, FQHC Medicaid rates for clinic sites or programs that serve large numbers of people experiencing chronic homelessness and PSH tenants are often higher than rates paid at sites that serve mostly other types of patients. People experiencing chronic homelessness and those who live in PSH often have multiple chronic medical and behavioral health conditions that must be treated or monitored during each visit. In addition to having high levels of vulnerability and complexity, they may be distrustful of health care providers and challenging to engage in needed health care services because of past experiences or because of the symptoms of mental illness, trauma, brain injuries, or substance use disorders. For these patients, visits with Health Center clinicians often require more time, and these clinicians therefore may see fewer patients in a day, than those who deliver care in clinics that primarily serve people with less complex needs.
In addition, Health Centers often use multi-disciplinary teams that include community health workers, social workers, case managers, and other front-line workers or "care extenders" to engage hard-to-reach people in health care services, make sure they get to appointments with clinicians, and provide health education, coaching and encouragement for patients to follow through on the recommendations of their health care providers.
Some innovative programs operated by Health Centers rely on specialized funding in addition to their HRSA grants and Medicaid reimbursement to cover some of the costs for implementing team-based models of integrated care, including state and federal grants, contracts with states or local governments, philanthropic support, and other funding sources. Some of these other sources of funding are time-limited, and funders often expect Health Centers to sustain and expand effective program models using Medicaid reimbursement. States may consider these costs, including personnel costs for unlicensed members of multi-disciplinary teams that deliver health care and behavioral health services to high-need patients, when establishing FQHC prospective payment rates or adjusting rates in conjunction with changes in the scope of services provided by a Health Center. The text box below illustrates the approach and funding mix of Boston's HCH Program.
| Using Multiple Funding Sources in a Health Care for the Homeless Program |
|---|
Most Boston HCH Program clients have multiple chronic health conditions, including medical and behavioral health disorders. Treatment and supportive services are delivered by multi-disciplinary teams that include physicians, physician assistants, nurse-practitioners, nurses, case managers, and behavioral health practitioners. Team members work collaboratively to deliver care to homeless people on the streets, at McInnis House medical respite, in outpatient primary care, in behavioral health and dental clinics in several locations, in shelters, and in housing. Continuity of caregiving relationships is maintained across settings for the same people. The program integrates primary care, behavioral health care, dental care, vision, pharmacy, and case management services, as well as linkage to a range of nonmedical supports. To cover the range of services it offers, the Boston HCH Program uses Medicaid reimbursement in addition to several other funding sources, which include the following:
|
As many states are relying on Medicaid managed care to provide health care for a growing number of beneficiaries, most Health Centers have become part of these managed care plans' provider networks to assure that they will receive payment to care for clients who are health plan members. In many cases, the health plans make payments to the Health Centers as a fixed amount of funding per-member per-month for health plan members who have selected or been assigned to the Health Center for purposes of receiving primary care. This amount will be similar to the monthly rates the plan pays to any provider. Usually this practice results in payments from the health plan to Health Centers that are lower than the Medicaid reimbursement they would get based on payments at the FQHC rate for billable encounters based on the PPS. States are required by federal law to give FQHCs additional "wraparound" Medicaid payments based on the gap between the health plans' per-member per-month payments and the revenues they would otherwise have received using the FQHC PPS payment methodology (based on the number of visits with a center's licensed health care providers, as described above). However, FQHCs often have to wait a year or more to complete the cost reconciliation process and receive this wraparound payment, which comes to them directly from the state Medicaid program.
7.1.4. Looking Beyond Fee-For-Service and Payment Based on Encounters
Increasingly, health policy experts agree that fee-for-service payment rewards volume but not value. If health care providers deliver more covered services, under a fee-for-service payment structure they receive more income. But fee-for-service does not provide strong incentives for health care providers to reduce avoidable service utilization, either by preventing health crises or by delivering interventions that reduce the need for more costly covered services. Fee-for-service payment mechanisms do not reward health care providers for keeping people healthy and improving health outcomes.
Further, it is not easy to obtain reimbursement for care coordination and integration under fee-for-service. With fee-for-service payment mechanisms, each provider of covered services gets reimbursed separately for activities and interventions that often could be much more effective if they were coordinated. When hospitals, specialists, primary care providers, and behavioral health services providers receive fee-for-service payments separately, they face little incentive to coordinate with one another or to facilitate transitions in care across settings to achieve the best results for shared patients, or to reduce avoidable hospitalizations and readmissions.
7.2. Medicaid Managed Care Payment Mechanisms
In recent years states have moved away from using fee-for-service payment for many of the health care services covered by Medicaid, relying instead on Medicaid managed care approaches to organizing payment and delivery of medical and/or behavioral health services for growing numbers of Medicaid beneficiaries.
In a managed care delivery system, people get most or all of their Medicaid services through an organization under contract with the state. States may adopt one or more of three different managed care arrangements:91
- Managed care organizations;
- Limited benefit plans;
- Primary care case management programs.
Medicaid managed care organizations, also often referred to as health plans, are responsible for delivering a defined set of Medicaid benefits to a group of people who are enrolled as plan members. The health plans receive capitated financing with a fixed amount of reimbursement per-member per-month to pay for covered benefits and other expenses for administration and care coordination. The plans then contract with health care providers under arrangements that are intended to deliver covered services while also reducing costs and increasing the quality of care.
Limited benefit plans allow states to "carve-out" certain services for which the state contracts with specialized health plans that have established provider networks to deliver Medicaid-covered dental care, mental health or substance use treatment, transportation, and other services.
With Medicaid-financed primary care case management arrangements, states make payments to primary care providers for care coordination services in addition to reimbursing the costs of health care services, usually on a fee-for-service basis. Primary care providers receive a small monthly fee per patient to deliver case management services that include coordinating referrals for specialty care and other health services.92
The first two of these arrangements have been and are likely to continue to be most relevant to Medicaid financing for services delivered to people experiencing chronic homelessness and those who live in PSH. In addition, some states are developing enhanced primary care case management programs and using these to serve high-cost Medicaid beneficiaries with complex needs and/or patterns of avoidable use of inpatient and crisis services as well as the family and children beneficiaries who have been the more usual recipients of primary care case management. As these programs evolve, there may be opportunities for states to tailor the programs to address the needs of people who are homeless or living in PSH.
7.2.1. How Medicaid Managed Care Is Evolving
Medicaid managed care arrangements are evolving rapidly in most states and are increasingly important when considering how Medicaid services are provided to people experiencing chronic homelessness or living in PSH. In 2013, almost 50 million Medicaid beneficiaries received benefits through some form of managed care, either on a voluntary or mandatory basis.93 Until recent years, though, the Medicaid beneficiaries with the most complex health care needs and who have the greatest cost of care--seniors and people with disabilities--have remained in fee-for-service.
In many states, Medicaid managed care began with a focus on enrolling children and families. A growing number of states now allow people with disabilities to enroll in managed care plans, and some states require that most seniors and people with disabilities do so. Many states are also using managed care plans to provide coverage to people who became newly eligible for Medicaid in 2014 under the terms of the Affordable Care Act.
Some states have separate managed care arrangements for medical care and behavioral health care services, "carving out" the latter and administering them under specialized limited benefit plans. When medical and behavioral health services are administered by different managed care organizations, the plans often use different provider networks and separate payment systems. Under these circumstances, states may require managed care plans that are responsible for medical care to coordinate care with other Medicaid services that are financed or delivered separately, particularly for seniors and people with disabilities. In other states, the health plans are responsible for mental health benefits and other behavioral health services as well as medical care. Even when the same managed care plan is responsible for both medical care and behavioral health services, many health plans subcontract responsibility for managing behavioral health services to a specialty managed care organization. Finally, some states make the health plans responsible for LTSS, including nursing home services and HCBS, while other states administer LTSS separately and may pay for them on a fee-for-service basis.
States' decisions about the scope of services covered through managed care plans will have implications for opportunities to coordinate care across providers and settings as well as for opportunities to achieve and reinvest savings. For example, some of the services in PSH that are defined as specialty mental health services produce savings by reducing costs for medical hospitalizations and emergency room visits. If the same managed care plan is responsible for both mental health and medical costs, the plan will be able to realize savings attributable to mental health services, and potentially reinvest those savings to expand effective service interventions linked to housing for plan members who experience homelessness. If health plans are also responsible for costs of long-term care, they may be able to recognize and reinvest savings associated with interventions that reduce nursing home stays and use more of their resources to expand the availability of care management, community support, and a range of HCBS that can reduce the need for care in nursing homes. If these benefits are covered through separate managed care plans, however, states will need to look for ways to align incentives for the plans to deliver services that contribute to reducing overall Medicaid costs and improving outcomes for beneficiaries.
Medicaid managed care organizations must comply with extensive federal requirements to assure that members get appropriate care. Health plans must ensure quality and provide reasonable and timely access to an adequate network of providers and they must establish procedures for handling appeals and grievances. Because of these requirements, managed care plans may improve the availability of care for some beneficiaries who have found it difficult to access the care they need in fee-for-service Medicaid programs.
In most cases, when Medicaid beneficiaries are required to enroll in managed care plans, they have a choice between at least two plans, and the right to change managed care plans periodically. Medicaid managed care implementation is often accomplished under a waiver of some Medicaid rules, including a waiver of "freedom of choice" requirements.94 When people are enrolled in managed care plans, instead of accessing care from any qualified Medicaid provider willing to serve them, they must also select or be assigned to a primary care provider or medical home. These waiver provisions allow health plans to contract with a limited set of providers and to establish rules and procedures that govern where members may receive services that the plan will reimburse.
For reasons noted in Chapter 2, beneficiaries often do not choose a plan and provider for themselves but instead find themselves auto-assigned to a plan and a primary care provider based on limited information about individual needs or existing relationships with care providers. When Medicaid beneficiaries are auto-assigned to a provider, they can select a different primary care provider in the plan's network, but often health plans will not make these changes until the next month after a request is made. States and health plans need to ensure that procedures are in place for quickly making changes in provider assignment and for facilitating access to the most appropriate care providers for people who are homeless, supportive housing tenants, and people with behavioral health disorders. If they receive accurate and timely information and cooperation from the Medicaid program and the health plans, PSH case managers and homeless assistance programs and behavioral health service providers can help people navigate the process of selecting health plans and primary care providers, and requesting changes when needed.
Many states have used Medicaid managed care arrangements to incentivize improved performance, care quality, and better health outcomes through setting expectations, requiring appropriate measurement, and monitoring performance. These requirements are particularly important for adults with chronic health conditions and people with disabilities, for whom the challenge of care coordination is substantially greater than it is for young families.
For example, performance measures that require health plans to reduce hospital readmissions may create incentives for the plans to identify patients who are homeless and at high risk for complications and readmission if they are not connected to housing and appropriate supports at the time of hospital discharge. Partnerships with medical respite programs and PSH and attention to the needs of people experiencing homelessness and PSH tenants during care transitions can help health plans achieve performance goals related to reducing hospital readmissions and improving health outcomes.
As growing numbers of people with disabilities, including PSH tenants and people experiencing chronic homelessness, enroll in Medicaid managed care, health plans need to expand their provider networks to include Medicaid providers who have experience with homeless people and high-risk, hard-to-reach populations. In addition to providers of medical and behavioral health services, health plans can benefit from collaborations with organizations that have experience serving people experiencing homelessness or living in PSH. These service providers are often working to help facilitate access to health care and coordinate care for people who are chronically homeless and for PSH tenants; they are seeking to understand how managed care plans work for the people they serve. These providers can be valuable partners in helping plans effectively manage care for this group of beneficiaries.
Managed care arrangements can offer promise for people with more complex health care needs, including those who are or have been chronically homeless, because one expectation for their performance is care coordination. But existing systems for care coordination in many health plans were developed to meet the needs of relatively healthy children and parents. These systems will probably need to be modified to meet the needs of people with more complex health conditions and service needs. Many Medicaid managed care plans rely on telephone contacts to coordinate care for their members, but as CMS notes, for people who are the most frequent users of emergency and inpatient care, "Telephonic case management alone has had limited success, perhaps because people may be difficult to reach by phone and require more-intensive, in-person interventions to build trust and provide needed supports."95
Some states and managed care plans are working to develop and implement newer approaches to providing these more-intensive face-to-face interventions through a variety of models. States have the option to require or encourage plans to provide or contract for intensive, in-person care management services for their most high-need members, including those who have experienced chronic homelessness.
Capitation, which provides a fixed per-member per-month payment to health plans for all covered services, offers strong incentives for plans to control costs by reducing avoidable hospitalizations, emergency department visits, and stays in skilled nursing facilities. Evidence shows that the "whatever it takes" approach to services that has been developed in housing first programs for people who have been chronically homeless produces significant reductions in the utilization and costs of these expensive crisis services. Case managers, nurses, and other staff in these programs take the time needed to establish trusting relationships and offer assistance with basic needs for homeless people who may at first be reluctant to stop drinking or take medications for mental health disorders. They use motivational interviewing and other practices to encourage people to take steps toward changes that support housing stability and enhance well-being and connections to appropriate health care. While capitated financing could potentially offer health plans the flexibility and the incentives to pay for some of these services, based on evidence that they will reduce unnecessary use of crisis services, states may need to expand their service definitions or seek approval from CMS to allow health plans to use Medicaid financing to pay for services that are not specifically defined as covered benefits in their Medicaid state plan.
As part of 1115 demonstration waiver requests, states may request CMS approval to use Medicaid to pay for "costs not otherwise matchable." As part of 1115 or 1915(b) waiver requests, states may request CMS approval to use savings achieved through the implementation of managed care to pay for additional services.
- In Michigan a 1915(b) waiver is used to allow the state to cover Community Living Supports and Services. These services assist individuals with the skills and supports they need to live in the community.
- In Massachusetts, the CSPECH provides nonclinical support services for adults experiencing chronic homelessness. The intent is to help people access and sustain permanent housing and avoid unnecessary hospitalizations. CSPECH operates under a Medicaid 1115 waiver that authorizes Massachusetts to use Medicaid to pay for medically necessary "diversionary services" as alternatives to inpatient services.
7.3. Payment Reform: Emerging Structures for Improving Health Outcomes and Reducing Costs
Increasingly, states are working to develop more efficient and effective systems of care. The Affordable Care Act included many provisions to give these efforts a substantial push forward. This section examines several approaches that state Medicaid officials could consider as ways to meet the needs of people who are now experiencing chronic homelessness or living in PSH. These efforts are all works in progress; they face many challenges and are in the process of developing a range of approaches to meet them. Their experiences offer state Medicaid officials a look at practices they might adapt and what aspects of their Medicaid programs they could use or modify to do so.
State Medicaid officials, innovative health care providers, and health policy experts are working to design and implement new models of payment that provide financial incentives for coordinating and integrating care, containing costs, and improving quality and health outcomes. Some of these new payment models can provide opportunities to make changes in the health care delivery system that will improve care and lower health care costs for people with the greatest health and social needs, including those with multiple chronic health conditions and co-occurring behavioral health disorders who have experienced chronic homelessness. Emerging approaches to payment and delivery system reform may include new ways to provide care for PSH tenants including ways to pay for some of the services in PSH.
The reality of Medicaid funding is that just 5 percent of Medicaid beneficiaries account for about 50 percent of Medicaid spending.96 Further analysis indicates that about 60 percent of these high-cost beneficiaries (i.e., 3 percent of all beneficiaries) have mental health and substance use disorders that occur along with chronic physical illnesses.97 This combination of co-occurring medical and behavioral health disorders contributes to high use of costly health services (see Exhibit 7.1, reproduced from the CHCS publication cited in footnote 97).
| EXHIBIT 7.1. Impact of Behavioral Health Co-morbidities on Per Capita Hospitalization among Medicaid-Only Beneficiaries with Disabilities |
|---|
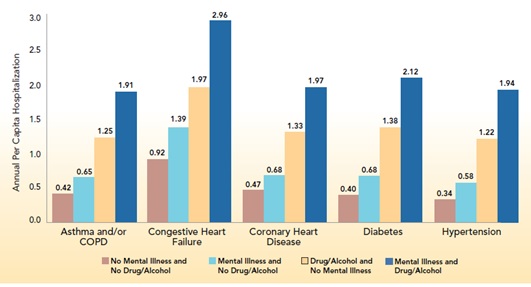 |
Because a large share of Medicaid spending is associated with care for seniors and people who have disabilities or multiple chronic health conditions and co-occurring behavioral health disorders, states are increasingly seeking ways to improve their ability to manage care for these groups of beneficiaries in ways that produce better health outcomes while also reducing expensive and unnecessary service use. Some of these strategies include efforts to coordinate or integrate care for medical, mental health, and substance use conditions.
By definition, people experiencing chronic homelessness have disabilities and they often have co-occurring and interacting chronic medical and behavioral health conditions. Many communities are prioritizing the most vulnerable chronically homeless people and those who have been the most frequent users of hospital emergency rooms and inpatient care for access to PSH. This means that initiatives that focus on high-cost, high-need Medicaid beneficiaries with complex health conditions are likely to include people who are experiencing chronic homelessness as well as those who are now living in PSH. This situation creates opportunities to incorporate services that are delivered in or linked to PSH as a component of emerging payment and delivery system reforms in some states.
Anticipating that the growth in health care costs can be contained by a significant restructuring of the system to incentivize performance/health outcomes and encourage a greater focus on prevention, primary care, and care coordination, the Affordable Care Act enabled several new structures for integrated care management and payment, including health homes and ACOs, along with a focus on "super-utilizers." These new delivery system and payment models incorporate options for financing more integrated care delivery and care coordination, which are seen as vital to two major system goals--improving health outcomes and controlling costs. CMS offers states substantial encouragement to participate in these efforts to become more efficient and effective.98
The strategies described in this section are all geared to working with a highly targeted subset of the Medicaid population--those who need more hands-on care and coordination than other beneficiaries because of multiple health and behavioral conditions, social needs, high levels of vulnerability, and often a history of high costs for avoidable hospitalizations and emergency room visits. Goals for these strategies include the following:
- Integrating care across physical health, mental health, and substance use treatment (often also pharmacy and sometimes dental), or at least across mental health and substance use.
- Identifying and targeting the people who have the highest levels of avoidable costly care.
- Paying attention to social determinants of health--poverty, housing, the lack of social supports--and developing working relationships with community agencies that can help alleviate them (e.g., housing, social services).
- Making maximum use of available data, improving data adequacy, developing shared data systems, using data for targeting, monitoring, and evaluation.
- Using payment mechanisms that cover the costs of care integration and coordination such as team meetings and face-to-face care management.
- Using payment mechanisms that facilitate flexibility in care delivery--moving toward capitation, payment per-episode-of-care, or payment for a defined bundle of services.
- Developing effective ways to adjust payments on the basis of patient risk/complexity/level of care needed, both across patients (some people needing more-intensive care than others) and within patients over time as level of functioning changes.
- Developing appropriate incentives--pay for performance, opportunities to reinvest a share of savings.
7.3.1. Super-Utilizer Programs
In a growing number of states, specialized programs are being developed to focus on improving care and reducing costs for a small subgroup of "super-utilizers." These are Medicaid beneficiaries for whom health care costs are extraordinarily high and "impactable," meaning that some costs could be reduced or avoided with more effective interventions. Patients in this group often have multiple emergency department visits and/or preventable hospital admissions for multiple poorly controlled chronic medical conditions, co-occurring behavioral health disorders, and social barriers, including homelessness.
In its informational bulletin of July 24, 2013, CMS states "Programs that target 'super-utilizers'--beneficiaries with complex, unaddressed health issues and a history of frequent encounters with health care providers--demonstrate early promise of realizing [the potential to improve care, improve health, and reduce costs] for Medicaid populations." Super-utilizer programs may work in close partnership with primary care providers, enhancing their capacity to care for people who are super-utilizers and provide alternative intensive services, or they may transfer these patients from primary care arrangements to a specialized care setting or team.
Super-utilizer programs often embed case managers or outreach workers in primary care settings, where they work closely with medical providers to assure appropriate care. Alternatively, they may be housed in community organizations that work with high-utilizers who receive care from multiple primary care providers. The care managers provide added support to high-utilizers while also helping to build primary care providers' capacities to meet the needs of this part of their patient population. Finally, some programs create interdisciplinary care teams that have a geographic focus, accepting referrals from and working with primary care providers in the region. These teams may be based in Community Health Centers, home health agencies, or other community-based organizations.
Benefits of Super-Utilizer Programs
A review of pioneering programs for super-utilizers identified key lessons learned and promising practices:99
- High-utilizer programs can make substantial reductions in hospital admissions, hospital days, emergency department visits, and total costs of care.
- For homeless or precariously housed people, providing permanent housing with case management appears to be the most powerful way to reduce costly health care utilization.
- Many programs have a home visit component, and they engage in frequent, in-person outreach to clients to build trust, establish relationships, and provide needed supports.
- Most programs perform a careful initial assessment, develop a care plan, and incorporate regular follow-up by the care management team.
- There is no standard composition of care management teams. Most programs create interdisciplinary care teams that include a nurse and a social worker. It is helpful if teams also work with a psychiatrist and pharmacist. Nonprofessional personnel such as navigators or health coaches can assist professional team members.
- Programs tend to have a coaching philosophy. They attempt to teach patients to better self-manage their health and social problems, and to navigate health and social services systems.
- Coaching patients to understand their medications and to become more medication adherent is an essential feature of all programs.
For people experiencing chronic homelessness or living in PSH, a big advantage of super-utilizer programs is that the programs often integrate or coordinate treatment for mental illness and substance use disorders with primary care and other medical care, and also collaborate with community-based agencies to address social determinants of health including stable housing and social supports. While the programs do not use Medicaid to pay the cost of housing itself, they recognize the importance of stable housing for reaching the goal of improved health outcomes and reduced use of avoidable services, and work to help clients find and keep housing. These programs may deliver, partner with, or supplement the services component of a supportive housing program for people experiencing homelessness who are frequent users of hospital care.
Payment Mechanisms for Super-Utilizer Programs
States have used a variety of Medicaid payment mechanisms to cover the costs of super-utilizer programs, including the costs of care management. These include: (1) a fixed per-member per-month primary care case management or other care coordination fee to fund care managers; (2) multi-payer case management payments involving Medicaid, Medicare, and commercial insurers for privately insured individuals; (3) a single per-episode-of-care payment that covers all costs associated with a particular episode of care; (4) a risk-based per-member per-month capitation payment to a managed care health plan; and (5) shared savings arrangements with care teams if program clients incur lower-than-expected costs for total care over a fixed time period. These payment mechanisms may be tiered or adjusted based on the complexity of an individual's medical, psychosocial, and behavioral health conditions.
Some approaches to payments for super-utilizer programs cover the cost of coordination but not the cost of covered health care services, for which providers may be reimbursed through existing fee-for-service or managed care payment arrangements. Other approaches to payment include the cost of health care services in addition to the cost of coordination. Examples of each payment mechanism and what it covers are included in the CMS July 24, 2013, bulletin.100
Financing for super-utilizer programs often incorporate benefits covered under Medicaid state plans, including Medicaid optional benefits such as health homes or TCM, and FQHC payment mechanisms. States may also use payment mechanisms included in Medicaid 1115 waivers or federally-funded demonstration programs such as the Multi-Payer Advanced Primary Care Practice Demonstration and FQHC Advanced Primary Care Practice Demonstration. Several states implementing super-utilizer programs are doing so in part with grant funding from CMS's Center for Medicare and Medicaid Innovation. In addition to public funding, many pioneering super-utilizer programs also receive grants and technical support from philanthropy.
In addition to the various ways that state Medicaid offices pay for the care provided by super-utilizer programs, federal Medicaid funding is available at a 90 percent match rate for a variety of activities related to data system design, development, and implementation costs. High-quality data is essential for super-utilizer programs--for targeting, ongoing care management, monitoring, and evaluation--so the opportunity to have federal funding to cover most of the up-front costs of a good data system is an added value to state Medicaid programs. Participants at a super-utilizer summit convened by CHCS in 2013 emphasized the importance of good data at every point along the path of program development, starting with an assessment of whether a state needs such a program, determining whom it would serve, developing and operating targeting strategies, contributing to care decisions, monitoring the program, and evaluating its impact.101
7.3.2. ACOs and Integrated Care Models
ACOs are networks of physicians, hospitals, and other providers that work collaboratively to improve the quality of health care services and reduce costs for a defined patient population. ACOs have financial incentives for coordinating care, containing costs, and improving quality across multiple sites of patient care. This makes ACOs and ACO-like integrated care models particularly promising as a strategy for integrating care for Medicaid beneficiaries who have multiple chronic conditions and face social barriers to health, including people experiencing chronic homelessness and many of the people who are living in PSH.
ACOs and similar integrated care models emphasize person-centered, continuous and comprehensive care. The CMS Center for Medicaid and CHIP Services released two letters to state Medicaid directors in 2012, providing guidance regarding Medicaid integrated care models, including ACOs and ACO-like models for payment and service delivery reform.102
CMS has been working to support the development of ACOs since before the passage of the Affordable Care Act, offering multiple approaches to shared savings and incentive structures with the goal of promoting more coordinated and appropriate care for Medicare and Medicaid beneficiaries. Most of the action in the first few years focused on Medicare, but increasing attention is being paid to developing integrated care models that are similar to ACOs for seniors and disabled adults within Medicaid, as well as for people who are beneficiaries of both programs (dual eligibles).103
ACOs for Medicaid beneficiaries are still works in progress and will be so for years to come, in part because there is no specific current statutory authority for ACOs within the Medicaid program. ACOs or similar integrated care models for Medicaid beneficiaries are being implemented by states using a mix of financing mechanisms that include fee-for-service, managed care, and primary care case management. Increasingly states are working to implement ACOs or similar models within a managed care environment, working to define and align responsibilities and financing incentives between managed care health plans and ACOs.104
CMS allows states considerable flexibility in structuring payment mechanisms for ACO or ACO-like models. While policy development is still under way at the federal level, CMS is working with states to move from volume-based fee-for-service reimbursement to integrated care models with financial incentives to improve beneficiary health outcomes. States may offer care coordination payments, reimbursement through per-member per-month arrangements, and/or financial incentives through shared savings arrangements or incentive payments for providers who demonstrate improved performance on quality and cost measures.105 Some state proposals for integrated care models may require a combination of state plan and waiver authority.106
In addition, CMS offers an extensive array of technical assistance to states and others seeking to form ACOs, along with the opportunity to obtain innovation grants and financial help with the data system development work that is required for an ACO to operate effectively.
States that are working to implement ACOs or ACO-like integrated care models for Medicaid beneficiaries may take different approaches with varying levels of integration across physical health, behavioral health, public health, and community services. The models that will be of most relevance to people experiencing chronic homelessness or living in PSH will be those that opt for maximum integration across all of these domains, as all are relevant to the needs of this population.
As observed by CHCS, some state Medicaid programs have adopted care coordination models that are similar to ACOs, and these models generally fall into one of three types.107 The first is a provider-driven model, with providers establishing integrated delivery systems or collaborative networks that assume some level of financial risk and responsibility for coordinating care and achieving client outcomes, including identifying and managing care for high-cost patients.
The second type is driven by managed care health plans that are actively engaged with health care providers in forming an ACO. Health plans assume a greater role in supporting data systems and building provider capacity for care management. The managed care organizations involved retain the financial risk of their capitation structures, but may develop new payment models for their contracted providers, who partner with the managed care organization to improve client outcomes.
Hybrid models incorporate elements of managed care health plan-led and provider-led ACOs. This approach builds upon the strengths of health plans, which have strong capacity for managing data and claims, and providers, who have the capacity to implement targeted care management and support as well as linkages to community partners to better manage care for patients with complex needs.
Another third type of ACO is the regional or community partnership. In this model, community organizations join together to develop care teams that manage the care a client receives and work to improve health outcomes while avoiding unnecessary care. These partnerships go well beyond the more usual interdisciplinary team approach, in that they create a formal organizational entity that receives payments and shares in savings. However, the state or managed care organizations may retain the financial risk if the total cost of care needed exceeds the level of payment provided to the ACO.
7.4. Summary
This chapter has reviewed traditional Medicaid payment mechanisms along with some of the new approaches being developed to accommodate new models of care. These newer models are of particular interest because it has often been difficult for agencies serving PSH tenants and people experiencing homelessness to cover the range of services needed by these populations through traditional fee-for-service payment structures. Some of the challenge of doing so stems from the variety of services included or left out of Medicaid state plans that are important for people experiencing homelessness or living in PSH, but some of the difficulty arises due to the fee-for-service mechanism itself. Other approaches include daily or monthly rates under fee-for-service, payment by episode, and payment through FQHCs and managed care organizations. The most recent approaches involve paying for care coordination and integration as an overlay on direct services, through health homes, care coordination entities, and some programs for super-utilizers. Another emerging approach for financing and delivering care for Medicaid beneficiaries is through ACOs. These latter approaches are particularly promising for populations with complex and interacting health and behavioral health conditions, for whom integrated care can make the difference in stabilizing living situations and improving health outcomes.
8. Putting the Pieces Together
As this Primer has frequently noted, people experiencing chronic homelessness and those who have spent years living on the streets and in shelters before moving into PSH often have complex co-occurring health conditions. These include chronic medical conditions as well as mental health and/or substance use disorders. Some have cognitive impairments that result from brain injuries, substance use, or other health conditions, and many have experienced trauma and toxic levels of stress that have had significant long-term health consequences. Their circumstances call for mechanisms that coordinate and integrate care for physical, mental, and substance use conditions and incorporate links to housing and coordination with staff that can provide the supports that help people maintain that housing.
Many Medicaid beneficiaries who have not had the misfortune to be homeless also experience this complex pattern of health conditions and would benefit from similar coordinating and integrating mechanisms. Attention to housing circumstances as part of the package is not misplaced for this larger group of beneficiaries with complex conditions, as their housing circumstances could change in ways that would put their health and health care at risk. Some beneficiaries could leave institutional care in nursing facilities or IMDs once they are able to access supportive housing in the community; others could lose a caregiver or no longer be able to maintain independent living. Care coordination and service integration will have the greatest impact if it includes a commitment to assure housing stability with supports as needed to maintain and improve health conditions.
The approaches described earlier in this Primer are primarily mechanisms for coordinating and integrating care for physical, mental, and substance use conditions. Development of these mechanisms has been spurred by the increasingly widespread recognition that, for people with complex needs, such integration is needed. Integrated care helps lead to better health outcomes, better care experiences for patients or clients, and care that is more cost-effective. The current state of the issue can be summed up as follows:
- Many useful approaches are being pioneered; using Medicaid to serve people experiencing chronic homelessness and PSH tenants is complicated, but it can be done.
- Medicaid will not cover everything, but it can support various services needed by PSH tenants.
- Many types of Medicaid providers--managed care organizations, FQHCs, behavioral health providers, and ACOs--are playing important roles.
- Conditions are ripe for improving care coordination and services integration, but achieving these goals will take the work of many parties. Some communities are already seeing the benefits from Medicaid expansion, both from Medicaid covering individuals who are homeless and from local resources being freed up to fund PSH programs.
8.1. Making Changes, From Small Steps to Comprehensive Redesign
People experiencing chronic homelessness or living in PSH are part of the larger group of Medicaid beneficiaries with the most complex co-occurring health conditions. They are the most vulnerable to negative outcomes and most likely to incur avoidable costs for crisis services if they receive inadequate and uncoordinated care. People with histories of chronic homelessness have added difficulties with building trust and engaging in services, and the added need for a strong focus on housing acquisition and stability. In thinking about changes to a state's Medicaid program to facilitate delivery of appropriate services to this group, it would be important to plan for the needs of the larger group of people with chronic and disabling health conditions and co-occurring behavioral health disorders, with special attention to housing and engagement for those who are or have been chronically homeless. With appropriate modifications to Medicaid state plans, Medicaid could cover the costs of many of the services needed for this group of beneficiaries. In turn, effective integrated services linked to housing for people who have experienced chronic homelessness could help to achieve savings to the Medicaid program by reducing avoidable hospitalizations and facilitating more appropriate use of other Medicaid-covered services.
For the group of people who are or have been chronically homeless, positive outcomes have been demonstrated by approaches that link medical care, behavioral health care, and supports to housing stability. These approaches focus on engaging and building trust with the most vulnerable people to help them get and keep housing and receive the care they need to manage their health needs. Effective program models incorporate recognition of housing as a social determinant of health. Efforts within Medicaid programs to align benefits, eligibility requirements, qualified service delivery personnel, service delivery sites, and payment mechanisms would promote integration by making it easier for providers to be paid for serving this population and removing current obstacles to integrated care. Risk adjustment and other incentives may be needed to make it feasible for health plans and provider networks to focus on the most high-cost, high-need individuals, for whom there are the greatest opportunities for achieving savings and improving outcomes.
To help state Medicaid officials working toward a more aligned system and greater integration, the Center for Integrated Health Solutions, co-funded by SAMHSA and HRSA, identified a set of promising approaches to integrating physical and behavioral health care that range from small steps to major system change.108 The Kaiser Commission on Medicaid and the Uninsured has released an issue brief based on that report, highlighting five promising approaches ranging from those that are relatively simple to adapt to more ambitious levels of system redesign.109 Most of these approaches are being used in one or more case study sites, as reported earlier in this Primer.
The five approaches described in the Kaiser Commission brief that are currently being modeled in Medicaid case studies aimed at better integrating physical and behavioral health care, are described below:
- Universal Screening. Integrated care begins with screening patients for conditions in addition to the ones they present for. A number of evidence-based tools are available for primary care providers to use to easily screen for behavioral health disorders. Routine screening for common medical conditions among adults with behavioral health conditions can be accomplished by providing behavioral health practitioners with basic equipment like a scale, a blood pressure cuff, and a stethoscope, along with training in how to use them. Early identification of conditions helps to prevent or mitigate their progression.
- Navigators. Even when individuals get screened for other conditions and referred for care, obtaining the recommended services can be challenging. Some state programs or managed care plans are deploying a new cadre of "navigators," who may be nurses, social workers, or trained paraprofessionals, to help beneficiaries navigate the health care system. Navigators' functions can range from simply helping individuals to seek care, to interacting with their health care providers on their behalf, to improving home and community-based support for their clients. Navigators also foster patient engagement.
- Co-Location. Geographic distance between physical and behavioral health provider settings can itself be a significant barrier to coordinated care. Some Health Centers and community behavioral health service providers are leaders in the "co-location" of physical and behavioral health care. Medicaid's system of prospective, cost-based payment for Health Centers supports this model because the costs of licensed behavioral health practitioners can be included in the calculation of Health Centers' prospective rates.
- Health Homes. A growing number of states are using the Medicaid "health home" option, established by the Affordable Care Act, to advance the integration of physical and behavioral health care for Medicaid beneficiaries with SMI. Health home services, which are eligible for a 90 percent federal match for two years (100 percent for those who enrolled under the expansion of Medicaid eligibility), include comprehensive care management, transitional care, referral to community and social services, and other services to foster integrated care for people with complex conditions and needs. Community mental health centers are one natural choice to be designated health home providers for Medicaid beneficiaries with SMI.
- System-Level Integration of Care. System-level integration of services and fiscal accountability underpins truly person-centered, holistic care and represents the most advanced model on the integration continuum. A fully integrated system for Medicaid beneficiaries is one that directly provides and is at financial risk for the entire complement of acute physical and behavioral health services covered by Medicaid.
8.2. The Focus of State Change Efforts
As more people who have experienced chronic homelessness get enrolled in Medicaid, states, health plans, and Medicaid providers will continue to learn more about their needs, and about opportunities to improve the quality of care and health outcomes for them while also managing costs. States that have expanded Medicaid eligibility will now have in their Medicaid program many newly eligible Medicaid beneficiaries who have experienced homelessness and have health care needs that are complicated by substance use disorders and other challenges related to mental health, trauma, isolation, and social service needs.
States and health plans are likely to learn a great deal about the types of services and supports that can help people engage in appropriate health care services, manage chronic health conditions, and reduce risky behaviors to achieve better health outcomes and avoid unnecessary hospitalizations. As they do so, they may want to consider making changes to the benefits and services included in their Medicaid programs, or request federal approval for waivers to develop and implement new approaches to health care that include coverage for diversionary services and tenancy supports. These approaches can achieve better outcomes while also controlling costs.
Often the benefits that states provide through their Medicaid programs are fragmented, in part because benefits have been added or modified by different administrators and stakeholders over a period of decades. This may result in different payment mechanisms for each piece of the package of services and supports needed by people who have experienced chronic homelessness, or gaps in Medicaid reimbursement for some of the services that are needed by this population and delivered in PSH. Many states have established separate benefits and program rules for Medicaid-covered medical care and treatment for mental health and substance use disorders. Often there are separate delivery systems and administrative structures associated with these Medicaid-covered services. To make innovative practices work within the Medicaid framework, states will need to examine, and likely modify, service definitions, medical necessity criteria, and specifications of which people can deliver which services and in which settings to make the services Medicaid-reimbursable.
Fragmentation of benefit design, program rules, financial responsibility, and delivery systems create challenges to delivering integrated, person-centered care for people with complex, co-occurring disorders, including people who have experienced chronic homelessness. State policymakers and Medicaid program officials recognize these challenges. Some are working on innovative approaches to support pilot programs or performance requirements that create more opportunities and incentives for health care providers and delivery systems to establish coordination mechanisms.
For example, states may require Medicaid managed care plans that are responsible for medical care to establish written agreements with counties or managed care plans that are responsible for Medicaid-covered mental health and substance use disorder services. These agreements can facilitate information sharing among the health plans and providers that work with the same Medicaid beneficiaries. This information sharing can be an important starting point for better care. For example, health care providers who prescribe medications or help a patient manage chronic medical conditions can make better clinical decisions if they know about other medications prescribed by a mental health provider.
States could require closer collaboration in the development of plans to provide care to people who receive services in separate systems. For now at least, these arrangements often focus on facilitating referrals, providing authorization for care and reimbursement, and limited information sharing among providers. These arrangements do not usually include mechanisms to support the integration of ongoing care by a multi-disciplinary team of providers working together to serve the same people. As states consider new approaches to care coordination, often in collaboration with Medicaid managed care health plans, there will be more opportunities to align and adapt benefits and payment mechanisms to support innovative approaches that integrate care at the service delivery level through teams or partnerships.
In some states, financial responsibility for the nonfederal share of Medicaid program costs is divided among different government agencies or between states and local governments, and the cost-sharing arrangements are different for medical care, mental health services, services for substance use disorders, and other Medicaid benefits. This can create incentives for cost-shifting, and it can make it difficult to align the incentives of government agencies to achieve overall savings in Medicaid program costs. For example, Medicaid-reimbursed mental health or behavioral health services delivered in PSH are likely to achieve savings in medical costs by reducing avoidable hospitalizations and emergency room visits. However, those impacts may not appear in the same budget that includes costs for the services in PSH. State leadership is often required to support the analysis of overall costs and savings to the Medicaid program and other public systems, and to use this analysis to inform policy decisions.
8.3. The Need for Flexible Funding and the Role of Local Public and Private Funders
Additional flexible funding is essential to achieve better results for both Medicaid beneficiaries and state Medicaid programs. Medicaid reimbursement can pay for many of the services needed by people with disabilities experiencing chronic homelessness or living in PSH, as well as services that help people experiencing chronic homelessness access housing assistance. But Medicaid will not be able to cover all the activities needed to truly stabilize this population's health conditions and housing situations. To engage some very vulnerable people, including those who have significant untreated mental health or substance use disorders who may be reluctant to seek the care they need, and to support stabilization, it is critically important to have funding that is flexible enough to allow programs truly to do "whatever it takes." Such funding may come from states, local governments, foundations, and other sources. In addition to Medicaid reimbursement for covered services, other support from public and private funders helps to pay for many of the services and supports without which people cannot get and keep housing.
As states take on the many administrative tasks related to Medicaid eligibility expansion, expanded partnerships with Medicaid managed care plans, and the design and implementation of new types of Medicaid benefits, support from private funders can support the planning, data analysis, and stakeholder engagement that contribute to innovation. In some states, foundations have provided funding to match or leverage state funding commitments that qualify for matching federal funds through the Medicaid program. In other cases, foundation funding has supported data analysis and planning for a state's Medicaid waiver proposal and the design and implementation of new covered benefits.
8.4. Changes at the Provider Level
For their clients and patients to benefit from these evolving innovations, health care providers and the provider organizations that work with people experiencing chronic homelessness or living in PSH will have to make parallel changes. Those that are not already Medicaid providers will have to become qualified themselves, or partner with agencies that are already Medicaid providers, to deliver and bill for covered services. Several aspects of their current operations may need significant investment to build infrastructure and organizational capacity, including staffing, administrative systems, and ability to produce electronic health records and exchange them securely with other providers serving their clients.
Service providers must make substantial investments in staff credentialing, training, and development; leadership development; and management to make the shift to Medicaid reimbursement if programs have relied on grant funding, fee-for-service, or other forms of Medicaid payment. They will have to implement electronic health records and data management systems that can serve their own purposes and also interact with systems operating at other providers and with Medicaid systems. They will also have to prepare administratively to participate in new Medicaid financing arrangements while simultaneously sustaining programs that rely on existing payment mechanisms. Finally, many will find that they can better serve their clients if they establish partnerships or implement new practice models to deliver more effective and integrated care. Some states and health care providers have received substantial support from foundations to supplement public investments by state and local governments and federal grants to make the investments needed to prepare for the future.
8.5. Conclusion--Making It Happen
If the promise of new and emerging approaches to integrated and cost-effective care for people experiencing chronic homelessness and PSH tenants is to be realized, many aspects of Medicaid state plans will have to be brought into alignment. Service definitions will need to be updated to assure that they can accommodate evidence-based practices and emerging, more integrated models of care, particularly for people who have co-occurring behavioral health and chronic health conditions or other medical needs. The administrative silos in which physical health care, mental health care, and substance use disorder treatment currently reside in many states will have to be breached so service providers can treat people holistically, request payment, and report performance through streamlined and coordinated mechanisms.
Gaps in covered services (e.g., outreach and engagement, collateral contacts, and services that explicitly focus on helping people get and keep housing as a social determinant of health and a driver of health care utilization and costs) will have to be closed to the extent possible under Medicaid, and alternative funding mechanisms identified if possible to fill those gaps. Given the enormous pressures currently facing state Medicaid agencies working to implement changes consistent with Affordable Care Act requirements, in the short term it may not be easy for them to make the time to focus on the needs of the relatively small population of PSH tenants and people still experiencing homelessness who could benefit from PSH.
Although the population of people experiencing chronic homelessness or living in PSH is a very small part of the total Medicaid-eligible population, it is no simple matter to design programs within Medicaid that meet its needs. For this reason, it makes sense to work with other constituencies who need services delivered in their homes and communities to develop care structures that work across a wider range of populations.
In the context of preparing to meet the 2014 requirements of the Affordable Care Act and other major pressures for change, it is remarkable that so many states and health care providers have made it a priority to work on using Medicaid to improve care for people experiencing homelessness, and to find ways to better integrate care and connect housing and services to better serve a small number of the most vulnerable people, including those with the most complex needs. It is not surprising that in some cases this work has moved more slowly and that progress has been more uneven than some might have hoped.
As attention focused on the activities that were most critical to preparing for 2014, stakeholders involved in Medicaid were often reminded that this has been an important deadline for some major activities, but it is not the finish line. While the enrollment of millions of Americans into Medicaid or subsidized insurance coverage began in October 2013 for coverage starting in 2014, the work of ensuring that coverage and care delivery systems work well for the most vulnerable people, including those experiencing homelessness or living in PSH, will require sustained attention in the coming years. This reality makes 2014 a beginning for the next phase of work to achieve the goals of health reform.
Notes
- Examples in this Primer are based on a three-year study conducted by Abt Associates Inc. for the Office of the Assistant Secretary of Planning and Evaluation, U.S. Department of Health and Human Services (HHS), which observed developments in six states and communities: California/Los Angeles, Connecticut, the District of Columbia, Illinois/Chicago, Louisiana/New Orleans, and Minnesota/Hennepin County. Details of the examples presented here may be found in: M.R. Burt, C. Wilkins, and D. Mauch, 2011, Medicaid and Permanent Supportive Housing for Chronically Homeless Individuals: Literature Synthesis and Environmental Scan. M.R. Burt, and C. Wilkins, 2012, Health, Housing, and Service Supports for Three Groups of People Experiencing Chronic Homelessness. C. Wilkins, M.R. Burt, and D. Mauch, 2012, Medicaid Financing for Services in Supportive Housing for Chronically Homeless People: Current Practices and Opportunities. M.R. Burt and C. Wilkins, 2012, Establishing Eligibility for SSI for Chronically Homeless People. C. Wilkins and M.R. Burt, 2012, Public Housing Agencies and Permanent Supportive Housing for Chronically Homeless People. M.R. Burt, C. Wilkins, and G. Locke, 2014, Medicaid and Permanent Supportive Housing for Individuals Experiencing Chronic Homelessness: Emerging Practices from the Field. All are listed at the end of this report and available at http://aspe.hhs.gov/daltcp/reports.htm.
- For purposes of defining chronic homelessness, HUD's definition of a disabling condition is broader than the criteria used to determine eligibility for Supplemental Security Income (SSI), but SSI eligibility criteria apply for purposes of categorical eligibility for Medicaid. HUD's definition of a disabling condition includes people whose disabilities are attributable to substance use disorders, as well as people with other disabling physical or mental health conditions.
- The definition includes individuals who are exiting an institution (including a jail, substance abuse or mental health treatment facility, hospital, or other similar facility) where they resided for fewer than 90 days and who resided in an emergency shelter or place not meant for human habitation immediately before entering that institution. http://portal.hud.gov/hudportal/documents/huddoc?id=pih2013-15.pdf.
- Wilkins, Burt, and Mauch, 2012, Medicaid Financing for Services in Supportive Housing for Chronically Homeless People: Current Practices and Opportunities. C. Caton, C. Wilkins, and J. Anderson, 2007, "People who experience long-term homelessness: Characteristics and interventions". Chapter 4 in D. Dennis, G. Locke, and J. Khadduri (eds.), Toward Understanding Homelessness: The 2007 National Symposium on Homelessness Research. Washington, DC: HHS and HUD, http://aspe.hhs.gov/hsp/homelessness/symposium07/Caton.
- For example, in the 2012 Point In Time (PIT) count of people experiencing homelessness, communities reported that nearly 100,000 people were experiencing chronic homelessness, including 67,247 people who were unsheltered (sleeping on the streets, in encampments, or other places not meant for human habitation). Among people with severe mental illness experiencing homelessness (not all of whom were chronically homeless), 46,550 people were unsheltered. This means that more than 20,000 unsheltered people without a severe mental illness were unsheltered and experiencing chronic homelessness.
- Caton, Wilkins, and Anderson, 2007, "People who experience long-term homelessness: Characteristics and interventions." Burt, Wilkins, and Mauch, 2011, Medicaid and Permanent Supportive Housing for Chronically Homeless Individuals: Literature Synthesis and Environmental Scan. M.R. Burt, 2008, Evaluation of LA's HOPE: Ending Chronic Homelessness through Employment and Housing. Washington, DC: Urban Institute, http://www.urban.org/publications/411631.html.
- D.P. Culhane, S. Metraux, T. Byrne, M. Steno, J. Bainbridge, and National Center on Homelessness among Veterans, "The Age Structure of Contemporary Homelessness: Evidence and Implications for Public Policy," Analyses of Social Issues and Public Policy 13.1 (2013): 1-17, http://works.bepress.com/dennis_culhane/124.
- HUD, 2013, 2012, Annual Homeless Assessment Report (AHAR) Report to Congress, Exhibit 2-9, https://www.onecpd.info/resources/documents/2012AHAR_FinalReport.pdf.
- Los Angeles Homeless Services Authority, 2011, Greater Los Angeles Homeless Count Report, Los Angeles: Los Angeles Homeless Services Authority (page 3).
- Mandatory benefits include inpatient and outpatient hospital services; nursing facility, rural health clinic, FQHC, prenatal and freestanding birth center services; physician, nurse-midwife, and certified pediatric and family nurse-practitioner services; home health, family planning, tobacco cessation, laboratory, X-ray services; and early and periodic screening, diagnostic, and treatment services for children under age 21.
- Optional benefits include clinic services; prescription drugs; rehabilitative services; case management, HCBS as an alternative to institutionalization, physical, occupational, speech, hearing, and language therapy; diagnostic, screening, and a variety of other services that may be approved by CMS.
- For more information see http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Waivers/Waivers.html.
- This section is adapted from information contained in Substance Abuse and Mental Health Services Administration, Medicaid Handbook: Interface with Behavioral Health Services, HHS Publication No. SMA13-4773, Rockville, MD: Substance Abuse and Mental Health Services Administration (SAMHSA), 2013.
- It is important to note that each state establishes an income criterion for Medicaid eligibility in addition to specifying services and other household characteristics. States electing to expand their income criterion for Medicaid eligibility under the Affordable Care Act began accepting households with incomes up to 133 percent of poverty or higher on January 1, 2014, but in the 25 states choosing not to expand income eligibility on January 1, 2014, single adults are still not eligible regardless of income, and families will continue to be eligible only if their household income is, on average, 48 percent of the federal poverty level (FPL) (Kaiser Family Foundation, 2014, Medicaid income limits as of January 2013 for parents and childless adults. http://kff.org/medicaid/fact-sheet/medicaid-eligibility-for-adults-as-of-january-1-2014.
- HUD recently expanded the definition of chronic homelessness to include families, but the vast majority of people experiencing long or repeated episodes of homelessness are unaccompanied adults.
- See Wilkins, Burt, and Mauch, 2012, Medicaid Financing for Services in Supportive Housing for Chronically Homeless People: Current Practices and Opportunities.
- The law allows a standard adjustment that has the effect of increasing this limit to 138 percent of FPL. This is approximately $15,282 for an individual in 2013.
- In addition, the Affordable Care Act expanded Medicaid eligibility for former foster care children through age 25 if they were enrolled in foster care and Medicaid when they turned 18 or aged out of foster care. This provision expands Medicaid coverage for a group of transition-aged youth that is often at risk of homelessness and sometimes served in PSH.
- 2012 AHAR, 2011 data, p. 5, table 3.
- For more information see Medicaid and Financing Health Care for Individuals Involved with the Criminal Justice System, December 2013, http://csgjusticecenter.org/reentry/publications/medicaid-and-financing-health-care-for-individuals-involved-with-the-criminal-justice-system/.
- Burt, Wilkins, and Locke, 2014, Medicaid and Permanent Supportive Housing for Individuals Experiencing Chronic Homelessness: Emerging Practices from the Field.
- SeeCMS State Medicaid Directors Letter (SMDL), SHO #13-003, ACA #26, May 13, 2013, Facilitating Medicaid and CHIP Enrollment in 2014, at http://www.medicaid.gov/Federal-Policy-Guidance/downloads/SHO-13-003.pdf. Other parts of the letter proposing options to maintain enrollment and prevent avoidable gaps in coverage are discussed below.
- For more information about these requirements see http://aspe.hhs.gov/hsp/immigration/restrictions-sum.shtml. For more information about uninsured people who do not qualify for Medicaid because of their unauthorized or recent immigration status see http://www.rwjf.org/content/dam/farm/reports/issue_briefs/2013/rwjf404825.
- Described in detail in Chapter 3.
- For a list of Health Centers that have received federal grant funding for outreach and enrollment assistance see http://www.hrsa.gov/about/news/2013tables/outreachandenrollment/. For more information about the role of Health Centers in providing outreach and enrollment assistance see http://bphc.hrsa.gov/outreachandenrollment/.
- See CMS SMDL, SHO #13-003, ACA #26, May 13, 2013, Facilitating Medicaid and CHIP Enrollment in 2014, at http://www.medicaid.gov/Federal-Policy-Guidance/downloads/SHO-13-003.pdf. Other parts of the letter proposing options to maintain enrollment and prevent avoidable gaps in coverage are discussed below.
- A full description of this program may be found at http://www.prainc.com/soar/.
- See Burt and Wilkins, 2012, Establishing Eligibility for SSI for Chronically Homeless People.
- See SAMHSA's Evidence-Based Practice kit for PSH at http://store.samhsa.gov/product/Permanent-Supportive-Housing-Evidence-Based-Practices-EBP-KIT/SMA10-4510.
- C. Caton, C. Wilkins, and J. Anderson, 2007, "People who xperience long-term homelessness: Characteristics and interventions."
- The IMD payment exclusion is in Section 1905(a) of the Social Security Act (the Act) in paragraph (B) following the list of Medicaid services. The definition of an IMD is in Section 1905(i) of the Act and in 42 CFR 435.1010 of the Code of Federal Regulations. The exclusion for individuals aged 65 and older is in Section 1905(a)(14) of the Act, and 42 CFR 440.140. The exception for individuals under age 21 is in Section 1905(a)(16 of the Act and 42 CFR 440.160. Medicaid guidance can be found at Section 4390 of the State Medicaid Manual.
- Section 4.4 of this Primer provides more details about settings in which Medicaid HCBS may be delivered, including the qualities of a home and community-based setting.
- Section 1905(a) of the Social Security Act (the Act).
- Services delivered by FQHCs are a mandatory state plan benefit at Section 1905(a)(2)(C), respectively, of the Act.
- Section 1905(a)(13) of the Act.
- Section 1905(a)(19) and 1915(g)(1) of the Act.
- Section 1945 of the Act as added by Section 2703 of the Affordable Care Act.
- Section 1915(i) of the Act.
- Section 1915(c) of the Act.
- For example, a waiver under Section 1115 of the Act.
- Under the Social Security Act, three types of organizations are eligible to enroll in Medicaid and Medicare as FQHC. They are: (1) Health Centers that receive grants under Section 330 of the Public Health Service Act; (2) Health Centers that meet all the requirements to receive a Section 330 grant but do not receive such funding; and (3) outpatient facilities associated with tribal organizations and Urban Indian Health Organizations. The first two categories are overseen by HRSA, and in this publication are jointly referred to as "Health Centers." HCH providers are a subset of Health Centers that receive Section 330 grants. This publication does not directly address Native American providers that are enrolled as FQHCs.
- The primary exceptions are people with incomes below the poverty level who live in states that have not expanded Medicaid eligibility. Other exceptions are immigrants with permanent residence but who are still within the five-year period during which they cannot receive public benefits, and people without documentation.
- HRSA 2012 National Homeless Data http://bphc.hrsa.gov/uds/datacenter.aspx?fd=ho&year=2012.
- Letter from James Macrae, Associate Administrator, HRSA Bureau of Primary Care to John Lozier, Executive Director, National Health Care for the Homeless Council, April 13, 2012.
- HRSA 2012 National Data for Homeless: Table 4--Selected Patient Characteristics http://bphc.hrsa.gov/uds/datacenter.aspx?q=tall&year=2012&state=&fd=ho.
- For more detailed information about FQHC payment methodology see Chapter 7 of this Primer and http://downloads.cms.gov/cmsgov/archived-downloads/SMDL/downloads/SHO10004.pdf.
- See http://bphc.hrsa.gov/policiesregulations/legislation/index.html.
- For more information, refer to HRSA Policy Information Notice 2008-01, Defining Scope of Project & Policy for Requesting Changes, http://bphc.hrsa.gov/policiesregulations/policies/pin200801.html.
- Medicaid Handbook: Interface with Behavioral Health Services was published in August 2013. It is available at http://store.samhsa.gov/product/Medicaid-Handbook-Interface-with-Behavioral-Health-Services/SMA13-4773. Some of the information provided in the Medicaid Handbook has been incorporated into this report.
- This Informational Bulletin is available at http://content.govdelivery.com/attachments/USCMS/2012/12/03/file_attachments/178580/CIB-12-03-2012.pdf.
- Medicaid makes an important distinction between rehabilitative services and habilitative services. Services provided through the rehabilitative option must "involve the treatment or remediation of a condition that results in an individual's loss of functioning." Habilitative services are services generally designed to assist individuals in acquiring, retaining, and improving the self-help, socialization, and adaptive skills necessary to reside successfully in home and community-based settings. Habilitative services can be covered by Medicaid through a HCBS waiver or optional HCBS State Plan services. Habilitation is one of the Essential Health Benefits that must be offered when a state adopts an "Alternative Benefit Plan" to provide coverage to people who are newly eligible for Medicaid beginning in 2014. States have some flexibility to determine how to design and implement these benefits and plans, consistent with rules established by the Federal Government. On July 15, 2013, HHS and CMS issued a Final Rule that includes several changes in the Medicaid program, including requirements to ensure that Medicaid benefit packages include Essential Health Benefits and meet certain other minimum standards. This Final Rule can be found at https://www.federalregister.gov/articles/2013/07/15/2013-16271/medicaid-and-childrens-health-insurance-programs-essential-health-benefits-in-alternative-benefit#h-14.
- See http://kaiserfamilyfoundation.files.wordpress.com/2013/01/7682.pdf.
- See http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Benefits/Downloads/Clarifying-Guidance-Support-Policy.pdf.
- CMS has been approving peer support specialists in state plan rehabilitative services for a number of years. For more information, see http://downloads.cms.gov/cmsgov/archived-downloads/SMDL/downloads/SMD081507A.pdf.
- In addition, the Community First Choice 1915(k) Option was established by the Affordable Care Act. This allows states to provide home and community-based attendant services, under a person-centered service plan, to some Medicaid enrollees with disabilities who otherwise qualify for institutional care. Community First Choice provides an enhanced federal matching rate for expenditures related to this option.
- For more information on Medicaid HCBS see: http://aspe.hhs.gov/daltcp/reports/2010/primer10.htm and http://www.medicaid.gov/HCBS.
- A link to the Final Rule, as well as links to several fact sheets and summaries prepared by CMS, are available at http://medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Long-Term-Services-and-Support/Home-and-Community-Based-Services/Home-and-Community-Based-Services.html.
- See SMDL, 10-024, available at http://downloads.cms.gov/cmsgov/archived-downloads/SMDL/downloads/SMD10024.pdf.
CMS guidance offers the following provider definitions:
- A designated provider: May be physician, clinical/group practice, rural health clinic, community health center, community mental health center, home health agency, pediatrician, OB/GYN, other.
- A team of health professionals: May include physician, nurse care coordinator, nutritionist, social worker, behavioral health professional, and can be freestanding, virtual, hospital-based, community mental health centers, etc.
- A health team: Must include medical specialists, nurses, pharmacists, nutritionists, dieticians, social workers, behavioral health providers, chiropractors, licensed complementary and alternative medicine practitioners, and physicians' assistants.
- For more information see http://downloads.cms.gov/cmsgov/archived-downloads/SMDL/downloads/SMD10024.pdf.
- More information about these approved SPAs is available at http://www.medicaid.gov/State-Resource-Center/Medicaid-State-Technical-Assistance/Health-Homes-Technical-Assistance/Approved-Health-Home-State-Plan-Amendments.html.
- A full discussion of Alternative Benefit Plans is beyond the scope of this Primer. For additional guidance about Alternative Benefit Plans, please refer to the CMS SMDL which was issued on November 20, 2012, SMDL #12-003 available at http://www.medicaid.gov/Federal-Policy-Guidance/downloads/SMD-12-003.pdf and additional information about Alternative Benefit Plans is available at http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Benefits/Alternative-Benefit-Plans.html.
- The July 15, 2013 Final Rule regarding Essential Health Benefits and other minimum standards for Medicaid benefit packages can be found at https://www.federalregister.gov/articles/2013/07/15/2013-16271/medicaid-and-childrens-health-insurance-programs-essential-health-benefits-in-alternative-benefit#h-14.
- More information about the application of parity requirements to Medicaid Alternative Benefit Plans is contained in a January 2013 CMS SMDL http://www.medicaid.gov/Federal-Policy-Guidance/downloads/SHO-13-001.pdf.
- This requirement is contained in 42 U.S.C. § 1396a(a)(10)(B).
- More generally Medicaid cannot pay for room and board, services to inmates in public institutions, or services furnished to individuals residing in IMDs. These limitations apply to a wide range of Medicaid services; they are not specific to rehabilitative services.
- For more information about ACT as an evidence-based practice for people experiencing homelessness, see http://usich.gov/usich_resources/solutions/explore/assertive_community_treatment.
- CMS staff can provide additional information and guidance to states regarding requirements that are applicable to TCM services. These case management services must allow individuals free choice of any qualified Medicaid provider, and may not be used to restrict access to other Medicaid services. States may define the target group(s) for TCM services and include a separate SPA when subgroups differ in terms of services, provider qualifications, or payment methodology. Medicaid pays for TCM services only if there are no other liable third parties to pay for such services, except for case management that is included in an individualized education program or individualized family service plan.
- See Section 5.6 for a more extended discussion of integrated care.
- More information about these practices can be found in the U.S. Interagency Council on Homelessness Solutions Database at http://usich.gov/usich_resources/solutions/explore/motivational_interviewing and http://usich.gov/usich_resources/solutions/explore/integrated_treatment_....
- See Burt, Wilkins, and Mauch, 2012, Medicaid and Permanent Supportive Housing for Chronically Homeless Individuals: Literature Synthesis and Environmental Scan, p.6-10.
- See http://www.integration.samhsa.gov.
- These worksheets are available at http://www.integration.samhsa.gov/financing/billing-tools#Billing. It is important to understand that these worksheets provide a PIT and information may change as states change their Medicaid programs.
- For additional information about HCBS, see Understanding Medicaid Home and Community Services: A Primer, http://aspe.hhs.gov/daltcp/reports/2010/primer10.htm.
- For purposes of HCBS, the term respite refers to a service that provides a caregiver, who is often a family member, with temporary, intermittent, and substitute support services for a person with a disability who qualifies for HCBS. This is very different from the use of the term respite to refer to medical respite programs that provide services for people experiencing homelessness.
- A link to the Final Rule as well as links to several fact sheets and summaries prepared by CMS are available at http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Long-Term-Services-and-Supports/Home-and-Community-Based-Services/Home-and-Community-Based-Services.html.
- Federal law prohibits Medicaid payment for room and board, but payment of a security deposit to a landlord is not considered rent.
- These psychosocial rehabilitation services are provided as part of a comprehensive specialized psychiatric program available to all Medicaid-eligible adults with significant functional impairments meeting the need levels in the 1915(i) resulting from an identified mental health or substance use disorder diagnosis.
- W. Sowers, C. George, and K. Thompson, 1999, "Level of care utilization system for psychiatric and addiction services (LOCUS): A preliminary assessment of reliability and validity." Community Mental Health Journal, 35(6):545-63.
- See Burt, Wilkins, and Mauch, 2011, Medicaid and Permanent Supportive Housing for Chronically Homeless Individuals: Literature Synthesis and Environmental Scan.
- See Burt, Wilkins, and Mauch, 2011, Medicaid and Permanent Supportive Housing for Chronicallyu Homeless Individuals: Literature Synthesis and Environmental Scan. A. Basu, R. Kee, D. Buchanan, and L. Sadowski, 2011, "Comparative cost analysis of housing and case management program for chronically ill homeless adults compared to usual care." Health Services Research.
- See Center for Medicaid and CHIP Services (CMCS) Informational Bulletin, July 24, 2013, Targeting Medicaid Super-Utilizers to Decrease Costs and Improve Quality, http://www.medicaid.gov/federal-policy-guidance/downloads/CIB-07-24-2013.pdf.
- C. Mann, 2011, Medicaid and CHIP: On the Road to Reform. Presentation to the Alliance for Health Reform/ Kaiser Family Foundation (based on FY 2008 MSIS claims data). See R. Kronick M. Bella, T. Gilmer, and S. Somers, 2007, The Faces of Medicaid II: Recognizing the Care Needs of People with Multiple Chronic Conditions. Center for Health Care Strategies (CHCS), Inc., http://www.chcs.org/usr_doc/Full_Report_Faces_II.PDF.
- For more information, refer to the CMCS Informational Bulletin CIB-07-24-2013; see footnote 31.
- See text at Section 4.3.1 and associated footnote 50, for details on the difference between habilitative and rehabilitative services.
- See http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Delivery-Systems/Fee-for-Service.html.
- Even as states increasingly move to Medicaid managed care payment and delivery systems and may provide payment to the managed care plans on a capitated (per-member per-month) basis, the managed care plans often pay some service providers on a fee-for-service basis.
- For details on these service and payment arrangements, see Burt, Wilkins, and Locke, 2014, Medicaid and Permanent Supportive Housing for Individuals Experiencing Chronic Homelessness: Emerging Practices from the Field.
- HRSA 2012 Health Center data is available at http://bphc.hrsa.gov/uds/datacenter.aspx and homeless program grantee data is available at http://bphc.hrsa.gov/uds/datacenter.aspx?fd=ho&year=2012.
- For a discussion on how the PPS is developed, see http://downloads.cms.gov/cmsgov/archived-downloads/SMDL/downloads/smd011901d.pdf.
- See http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Deli... and http://kff.org/medicaid/issue-brief/medicaid-and-managed-care-key-data-trends/ for basic information on Medicaid managed care options and enrollment statistics.
- In most cases, the monthly fee paid to primary care providers participating in primary care case management programs is only a few dollars a month. For these programs the expected level of case management or care coordination services is significantly less-intensive than the face-to-face case management and care coordination activities that are part of efforts to facilitate access to housing and appropriate health care services chronically homeless people with complex health needs.
- According to CMS, in 2011 more than 74 percent of all Medicaid beneficiaries in the United States were enrolled in some form of managed care. See http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Data-and-Systems/Downloads/2011-Medicaid-MC-Enrollment-Report.pdf.
- States may implement mandatory enrollment in Medicaid managed care under the authority provided by a 1915(b) waiver or 1115 demonstration waiver, or as a state plan option under Section 1932 of the Social Security Act.
- See http://www.medicaid.gov/federal-policy-guidance/downloads/CIB-07-24-2013.pdf, page 9.
- Kaiser Commission on Medicaid and the Uninsured and Urban Institute estimate based on 2004 MSIS data. Cited in CHCS publication, Clarifying Multi-Morbidity Patterns to Improve Targeting and Delivery of Clinical Services for Medicaid Populations, http://www.chcs.org/usr_doc/clarifying_multimorbidity_patterns.pdf.
- Kronick, Bella, and Gilmer, 2009, The Faces of Medicaid III: Refining the Portrait of People with Multiple Chronic Conditions.
- See http://www.medicaid.gov/federal-policy-guidance/downloads/CIB-07-24-2013.pdf.
- Source: http://www.chcs.org/usr_doc/HighUtilizerReport_102413_Final3.pdf.
- See http://www.medicaid.gov/federal-policy-guidance/downloads/CIB-07-24-2013.pdf.
- See http://www.chcs.org/publications3960/publications_show.htm?doc_id=1261570.
- See SMDL #12-001 available at http://www.medicaid.gov/Federal-Policy-Guidance/downloads/SMD-12-001.pdf and SMDL #12-002 available at http://www.medicaid.gov/Federal-Policy-Guidance/downloads/SMD-12-002.pdf.
- 220 mostly Medicare ACOs were operating as of March 2013, with 3.2 million assigned beneficiaries in 47 states plus the District of Columbia and Puerto Rico. Many are in one or another stage of development but not yet operational. See http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/sharedsavingsprogram/Downloads/All-Starts-MSSP-ACO.pdf. See the extensive materials, including briefs and webinars, accessible through http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ACO/index.html?redirect=/ACO/.
- For more information see The Balancing Act: Integrating Medicaid Accountable Care Organizations into a Managed Care Environment, http://www.chcs.org/usr_doc/ACO111313_Final.pdf.
- T. McGinnis, 2012, Medicaid ACOs: Collaborating toward an improved Health System, http://www.chcs.org/usr_doc/acnews0912McGinnis2.pdf.
- For more information see SMDL #12-002, http://www.medicaid.gov/Federal-Policy-Guidance/downloads/SMD-12-002.pdf.
- Planning for Accountability: Emerging Medicaid ACO Models and Key Issues for States, http://www.chcs.org/publications3960/publications_show.htm?doc_id=1261575#.UnJv9vmsh8E and Accountable Care Organizations in Medicaid: Emerging Practices to Guide Program Design, http://www.chcs.org/usr_doc/Creating_ACOs_in_Medicaid.pdf.
- B. Heath, Jr, Kathy Reynolds, and Pam Wise Romero, 2013, A Standard Framework for Levels of Integrated Healthcare, SAMHSA-HRSA Center for Integrated Health Solutions, http://www.integration.samhsa.gov/resource/standard-framework-for-levels-of-integrated-healthcare.
- Henry J. Kaiser Family Foundation, Integrating Physical and Behavioral Health Care: Promising Medicaid Models, http://kff.org/medicaid/issue-brief/integrating-physical-and-behavioral-health-care-promising-medicaid-models.