
October 2020
Printer Friendly Version in PDF Format (45 PDF pages)
ABSTRACT
Both long-stay nursing facilities and short stay post-acute skilled nursing facilities rely on the labor of 1.2 million health care personnel and support workers. Direct care workers such as licensed practical nurses, certified nursing assistants (CNAs), and personal care aides, typically provide most of the hands-on care in nursing homes, including assistance with bathing, dressing, and eating. Recruiting and retaining quality direct care staff has long been a challenge in nursing homes, and these problems have only been amplified by the pandemic. The purpose of this project was to study the impact of the COVID-19 pandemic on nursing homes with respect to these long-standing workforce challenges and to identify new federal, state, and facility-level policies and practices that have been implemented to address these challenges.
We found that nursing homes have grappled with how to retain adequate staffing while rapidly making operational changes to ensure the safety of workers and residents. At the same time, direct care workers are balancing concerns about their own safety, the well-being of the residents they care for, and their financial stability during the pandemic. The pandemic imposed greater demands on nursing home staff, such as new infection-prevention and control measures like screening, testing, and cohorting instituted to minimize transmission and contain the spread of the virus.
To maintain adequate staffing levels, federal and state government agencies, as well as nursing homes, altered their standard policies and practices to mitigate the impact of COVID-19 on the nursing home workforce. Licensing, credentialing, and training requirements were relaxed by federal and state agencies to facilitate the entry of new direct care staff into nursing homes and other health care facilities responding to increased needs. Human resources policies were revised by nursing homes to support workers who may be personally and financially impacted by COVID-19. Wages were increasing by nursing homes, state and local governments through hazard pay or weekly stipends; augmented non-wage benefits such as childcare, housing, transportation assistance, and food supports; and/or provided mental health support to help nursing home staff cope with the anxiety, grief, and fatigue they experience on the job as a result of COVID-19. Several federal initiatives were also designed to address the workforce challenges including: (1) an additional $5 billion in funding through the CARES Act to address critical needs in nursing homes; (2) rapid point-of-care diagnostic testing devices that will be distributed to nursing homes to enhance efforts to keep the virus from entering and spreading throughout nursing homes; and (3) onsite education and support to nursing homes experiencing outbreaks to help reduce transmission of COVID-19 spread among residents and staff.
This report was prepared under contract #HHSP233201500035I between HHS's ASPE/BHDAP and Mathematica. For additional information about this subject, you can visit the BHDAP home page at https://aspe.hhs.gov/bhdap or contact the ASPE Project Officers, at HHS/ASPE/BHDAP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C., 20201; Marie.Squillace@hhs.gov, Helen.Lamont@hhs.gov, Iara.Oliveira@hhs.gov, Judith.Dey@hhs.gov.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This report was completed and submitted on September 24, 2020.
TABLE OF CONTENTS
I. INTRODUCTION
- Background
II. KEY FINDINGS
- What Types of Workforce Challenges are Nursing Homes Facing during the COVID-19 Pandemic?
- What New Policies and Practices have been Implemented to Address Challenges related to the Direct Care Workforce and Nursing Home Operations?
- What Types of Infection-Control Challenges are Nursing Homes Facing during the COVID-19 Pandemic?
- What New Policies and Practices have been Implemented by Federal and State Governments to Address Challenges related to Infection-Prevention and Control, and Nursing Home Operations?
III. CONCLUSION
- Stakeholder Interviews
- Systematic Policy Review
- Gaps and Limitations
LIST OF EXHIBITS
- EXHIBIT 1: Distribution of Types of Nursing Employees in Nursing Homes, 2016
- EXHIBIT 2: Timeline of Federal Actions Taken to Respond to COVID-19 affecting the Nursing Home Industry
- EXHIBIT 3: Average Number of COVID-19 Cases per 1,000 Nursing Home Residents as of July 2020
- EXHIBIT 4: Workforce Challenges in Nursing Homes Stemming from COVID-19 and Strategies Implemented to Mitigate Challenges
- EXHIBIT 5: Stakeholders that Participated in a Semi-Structured Interview
ACRONYMS
The following acronyms are mentioned in this report.
| ASPE | HHS Office of the Assistant Secretary for Planning and Evaluation |
|---|---|
| ASPR | HHS Office of the Assistant Secretary for Preparedness and Response |
| CARES Act | Coronavirus Aid, Relief, and Economic Security Act |
| CDC | HHS Centers for Disease Control and Prevention |
| CHIP | Children's Health Insurance Program |
| CMS | HHS Centers for Medicare & Medicaid Services |
| CNA | Certified Nursing Assistant |
| COVID-19 | Coronavirus Disease 2019 |
| CPRSAA | Coronavirus Preparedness and Response Supplemental Appropriations Act |
| DHS | U.S. Department of Homeland Security |
| DPA | Defense Production Act |
| eNLC | Enhanced Nursing Licensure Compact |
| FDA | HHS Food and Drug Administration |
| FEMA | Federal Emergency Management Agency |
| FMLA | Family and Medical Leave Act |
| HHS | U.S. Department of Health and Human Services |
| LPN | Licensed Practical Nurse |
| NHRA | Nursing Home Reform Act |
| PPE | Personal Protective Equipment |
| PPP | Paycheck Protection Program |
| PTO | Paid Time Off |
| QIO | Quality Improvement Organization |
| RN | Registered Nurse |
| SNF | Skilled Nursing Facility |
| UV | Ultraviolet |
I. INTRODUCTION
A. Background
1. Nursing Home Workforce
Approximately 3.9 million Americans receive care in nursing homes each year.[1] Older adults and people with disabilities receive nursing home care either for a short stay in a skilled nursing facility (SNF) intended for those who require a higher intensity of skilled care (rehabilitation after surgery, physical therapy following stroke, wound treatment after surgery), or for a long stay in a nursing facility, for those who need less intensive, long-term care services, including custodial care, and who can no longer have their care needs met at home. Medicare covers care and services up to 100 days in SNFs, and Medicaid finances most of the long-term care services provided in nursing facilities for those who cannot afford the cost. More than 90 percent of nursing homes participate in both Medicare and Medicaid, and the less intensive long-term care services usually makes up the majority of the facility's business.[2] According to the Centers for Disease Control and Prevention (CDC), there are approximately 15,600 nursing homes in the United States with 1.7 million licensed beds, occupied by 1.4 million patients.[3]
| EXHIBIT 1. Distribution of Types of Nursing Employees in Nursing Homes, 2016 |
|---|
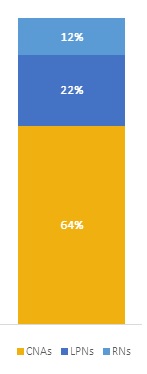 |
| SOURCE: Centers for Disease Control and Prevention. Available at: https://www.cdc.gov/nchs/fastats/nursing-home-care.htm. |
Both long-stay nursing facilities and short stay post-acute SNFs rely on the labor of 1.2 million health care personnel and support workers.[3] In recent years, the industry has faced critical challenges in both recruiting and retaining these direct care workers. While many people join the field with a desire to provide compassionate, hands-on care for residents, physical and emotional demands and low wages drive high rates of turnover among direct care workers. The onset of the COVID-19 pandemic has intensified workforce shortages to crisis conditions, putting the safety and well-being of both vulnerable residents and nursing home staff at risk.
Direct care workers such as licensed practical nurses (LPNs), certified nursing assistants (CNAs), and personal care aides, typically provide most of the hands-on care in nursing homes, including assistance with bathing, dressing, and eating.[4] Registered nurses (RNs) oversee the activities of the nursing staff and each patient's overall health and medical histories. Depending on their place of employment and patient population, RNs may also provide direct hands-on care. Nursing homes employ a broad mix of staff, including administrators, housekeeping staff, dietary staff, personal care aides, and licensed independent medical providers. In 2016, CNAs comprised 64 percent of employee full-time equivalents in nursing homes, followed by LPNs (22 percent) and RNs (12 percent).[5]
The CNA workforce is overwhelmingly female (90 percent), and about 54 percent of workers are minorities: 36 percent identify as Black, 11 percent as Hispanic/Latino, 5 percent as Asian/Pacific Islander, and 3 percent as another race or ethnicity. Thirty-one percent of CNAs have a child under the age of 18 at home; and 15 percent of CNAs have a child under the age of 5 at home. The nursing home industry also employs a large proportion of immigrant workers; 21 percent of CNA workers in nursing homes were born outside of the United States.[6, 7, 8, 9]
Amplified by the COVID-19, recruiting and retaining quality direct care staff has long been a challenge in nursing homes. Among CNAs, who provide 80-90 percent of hands-on care, the median annual turnover rate is 51.5 percent.[10] CNAs do physically demanding work, receive limited training, care for many residents per shift, receive low wages and few benefits, and have limited prospects in terms of advancing in their careers. Annual turnover rates among LPNs and RNs in nursing homes are also high, at 36.4 percent and 50 percent respectively.[10] While most direct care staff entered the field because they derive satisfaction from caring for older adults,[11] many are dissatisfied with their jobs; results from a 2004 national survey of CNAs in nursing homes found that 45 percent of CNAs are 'somewhat' or 'very likely' to leave their jobs within the year.[12]
Low wages are an underlying cause of staff shortages, both before and during the COVID-19 pandemic.[13] On average, according to the May 2019 Bureau of Labor Statistics, nursing assistants (including CNAs) earn $14.77 per hour, and nursing assistants who work in nursing facilities earn $14.25 per hour.[14] LPNs in nursing homes earn an average of $23.93 per hour, which is on par with the industry average, while RNs in nursing homes earn $33.53 per hour, 11 percent less than the industry average ($37.24 per hour).[15, 16]
While these wages have increased marginally in the last decade, they have not kept pace with inflation. Data show that a significant share of CNAs access some form of public assistance, such as Medicaid (21 percent) and food and nutrition assistance (22 percent).[6] Additionally, 31 percent of CNAs lack affordable housing.[6] CNAs often work in multiple long-term care facilities to supplement their earnings. Because of the physical demands of the job, CNAs are three times more likely to be injured on the job than the typical United States worker.[17] When staff are injured on-the-job because of repetitive lifting, overexertion, or a patient-inflicted injury, 63 percent of them will not receive paid leave.[17]
| Key Facts |
|---|
SOURCE: See https://www.cdc.gov/nchs/data/series/sr_03/sr03_43-508.pdf. |
As a result of these challenging working conditions, most nursing homes (75 percent) do not have enough staff to provide the 4.1 hours of daily nursing care per resident that is recommended by experts.[18] A 2019 report from the National Center for Health Statistics found that nursing homes, on average, were able to provide 3.8 hours of direct nursing care (RNs [0.54 hours per day], LPNs [0.85 hours per day] and Aides [2.41 hours per day]) to each resident per day in 2016, before the COVID-19 pandemic.[5] The staffing model for providing nursing care to residents, based on the Nursing Home Reform Act (NHRA) passed in 1987, has not been adjusted in more than 30 years to account for the increased acuity of residents now served by nursing and long-term care facilities.[19] The NHRA establishes minimum staffing standards of an LPN on duty 24 hours a day, a RN on duty 8 hours a day, 7 days a week, and a RN director of nursing for each facility.[20] The Act does not specify staffing requirements for CNAs, who provide the majority of hands-on care; CNA staffing requirements are determined by each state.[21]
Maintaining adequate staffing levels are also important for staff retention; a recent metanalysis of the literature found that the most important organizational factors that contributed to job satisfaction were facility resources and workload.[22] Because of demographic changes in the United States population, staffing challenges in the long-term care sector are likely to increase in the coming years as the number of older adults needing long-term services and supports grows. Before the pandemic, experts had been projecting that through 2026, more than 260,000 personal care aides, 135,000 RNs, and 113,000 CNAs would be needed annually to fill new or vacant positions.[23]
2. Policy Context
Nursing homes have long grappled with challenges that impact the quality of care, including workforce capacity and infection-prevention and control.[24] Research suggests that these challenges are largely driven by two factors: (a) long-term care financing that is dependent on Medicaid funding, and (b) a gradual increase in recent years in the acuity of nursing home residents.[25, 26] Providers and researchers claim that Medicaid reimbursement rates for nursing home stays often do not offset the cost of care, with nursing homes receiving, on average, $200 per day for a Medicaid patient, compared to about $500 per day for a traditional Medicare patient needing post-acute skilled care.[27] These low reimbursement rates limit revenue for nursing homes, and in turn contribute to low compensation for workers, staffing shortages, and fewer hours of care for residents.[25] Medicaid reimbursement rates are correlated with quality of care: nursing homes that serve a high proportion of Medicaid residents are likely to earn lower ratings on the Federal Government's quality rating system and provide fewer hours of care per resident per day.[28]
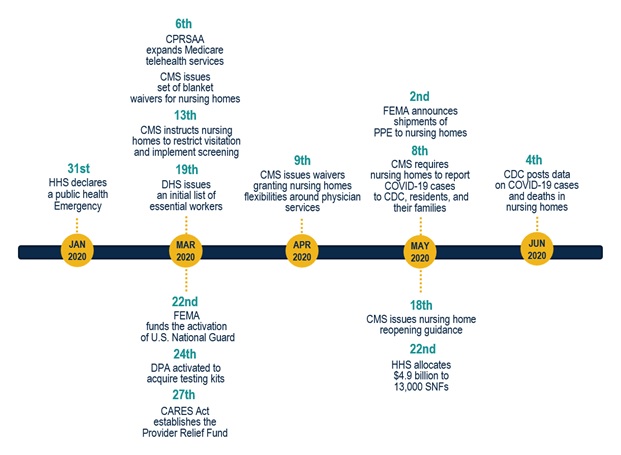
The Federal Government took several steps to provide immediate relief to health care providers on the frontlines of the coronavirus response (Exhibit 2). For example, the CARES Act, signed into law on March 27, 2020, allocated $100 billion to the Provider Relief Fund that is supporting hospitals and other health care providers during the outbreak. The CARES Act first allocated dedicated funding to hospitals on April 24, 2020; SNFs received $4.9 billion in dedicated federal stimulus on May 22, 2020 and the Centers for Medicare & Medicaid Services (CMS) announced the release of an additional $5 billion from the Provider Relief Fund for nursing homes on July 22.[29, 30] Under Sections 1102 and 1106 of the CARES Act, nursing homes were also eligible to receive up to $10 million in potentially forgivable loans through the Small Business Administration's Paycheck Protection Program (PPP) which helped employers affected by COVID-19 to retain staff during the public health emergency; these loans may be fully forgivable if staff and salary levels are maintained.[31, 33]
| EXHIBIT 2. Timeline of Federal Actions Taken to Respond to COVID-19 affecting the Nursing Home Industry |
|---|
 |
3. Nursing Homes and COVID-19
The COVID-19 pandemic has disproportionately affected nursing home residents and staff. In 23 states, deaths related to COVID-19 in long-term care facilities (including, but not limited to, assisted living facilities and nursing homes) accounted for over half of all fatalities stemming from the coronavirus as of the writing of this report.[32] COVID-19 deaths in nursing homes reached 49,871 residents as of September 2, 2020 (25 percent of total deaths nationwide).[34, 35] On average, the number of COVID-19 cases per 1,000 long-term care facility residents is highly variable across states, ranging from about 373 cases in New Jersey to 137 cases in New York to 1 case in Hawaii (data not shown) (Exhibit 3). Several factors may have contributed to the high rate of fatalities in nursing homes, including quick transmission of the virus in congregate care settings, a lack of testing and adequate personal protective equipment (PPE) during the early phase of the outbreak, asymptomatic spread by staff, the vulnerability of older adult residents to succumb to the disease, and the inability of many nursing homes to effectively contain the rapid spread of the virus.[36, 37] Also, recent research indicates that nursing homes with positive COVID-19 cases are more likely to have positive COVID-19 cases in the surrounding community, be located in an urban area, and have a larger facility size.[38] Preliminary research has also found that nursing homes with low nursing staff levels per resident had a higher burden of COVID-19 cases than those nursing homes with higher nursing staff levels.[39]
| EXHIBIT 3. Average Number of COVID-19 Cases per 1,000 Nursing Home Residents as of July 2020 |
|---|
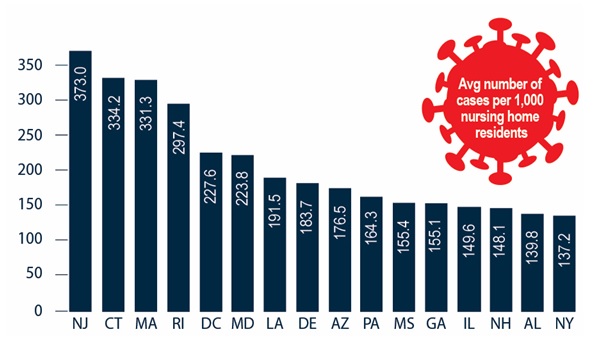 |
| SOURCE: The Nursing Home COVID-19 Public File includes data reported by nursing homes to the CDC's National Healthcare Safety Network system COVID-19 Long-Term Care Facility Module. Accessed on July 17, 2020, available at: https://data.cms.gov/Special-Programs-Initiatives-COVID-19-Nursing-Home/Resident-Average-Cases-per-1-000-Residents/ix9m-ky63. |
Nursing homes are designed for the short-term or long-term care of people who have chronic conditions and disabilities that affect their ability to perform daily activities, including self-care. Early in the pandemic, a lack of understanding related to transmission of COVID-19 tested infection-prevention and control measures in nursing homes. While nursing homes trained staff in infection-prevention and control practices, the surge in infections due to COVID-19 overwhelmed nursing homes which are not well equipped to manage COVID-19 as residents often share rooms and receive direct personal care from staff who support many residents. Many nursing homes also lack dedicated in-room sinks to support care delivery and nearby or in-room storage to ensure that linens and supplies remain sterile. Few, if any, nursing homes have rooms designed for isolation with a negative air flow or at least high-efficiency particulate air filtration equipment on site to allow for respiratory isolation in the event of pathogens such as COVID-19.
Conditions in nursing homes are exacerbated by the impact of the COVID-19 on staff. For example, nursing homes face additional worker shortages when staff get sick, when they must care for children or other relatives, or when they are afraid of being infected at work. Staff are also responsible for complying with new infection-prevention and control protocols to keep themselves and the residents they support safe. At a time when nursing homes need more staff to respond to the pandemic and to implement social distancing measures, they are often unable to maintain--rather than increase--pre-pandemic staffing levels. Two-thirds of facilities that responded to a recent survey by McKnight's Long-Term Care News reported that workers quit or call in sick because of COVID-19.[40] Difficulties procuring PPE has also escalated the crisis, both in terms of infection-control and the willingness of staff to remain in their positions.
4. Motivation for the Research
The Office of Behavioral Health, Disability, and Aging Policy within the U.S. Department of Health and Human Services (HHS), Office of the Assistant Secretary for Planning and Evaluation (ASPE) contracted with Mathematica to research the impact of the COVID-19 pandemic on the nursing home workforce to better understand the challenges faced by nursing homes during the outbreak. This project therefore has two objectives: (1) to gather information about the impact of the COVID-19 pandemic on the nursing home workforce to better understand the challenges faced by nursing homes during the outbreak; and (2) to identify new federal and state policies and practices that have been implemented to address these challenges in nursing homes. To meet these objectives, we sought to address the following broad policy questions through a series of structured stakeholder interviews and a systematic policy review conducted in June 2020:
-
What challenges are nursing homes facing during the COVID-19 pandemic with regard to:
-
PPE, supplies for staff, and infection-control policies and procedures.
-
The ability to maintain sufficient staffing levels and manage turnover.
-
-
What new federal, state, and facility-level assistance, policies, and practices have been implemented to address the challenges in nursing homes as a result of the COVID-19 pandemic and the effectiveness of this assistance.
| Summary of Key Findings |
|---|
|
II. KEY FINDINGS
A. What Types of Workforce Challenges are Nursing Homes Facing during the COVID-19 Pandemic?
The COVID-19 pandemic is imposing unprecedented demands on health care facilities and on nursing homes. Nursing homes have had to quickly respond in order to suppress the threat of the virus, absorb a flood of federal and state guidance, make rapid changes in how care is delivered, and implement new guidelines to safeguard residents and workers. We interviewed nine stakeholders and asked them what pressing workforce issues nursing homes have faced thus far during the COVID-19 pandemic. Five of them reported that COVID-19 escalated pre-existing workforce challenges that affect workers, characterizing the outbreak as "a complete crisis" that is having a "devastating impact on the workforce." In this section, we also present insights gained from the systematic policy review about these workforce challenges and strategies implemented to mitigate the challenges. The challenges are described below and summarized in Exhibit 4.
Stakeholders cited staffing shortages and retention of staff in the nursing home sector as major barriers during the COVID-19 pandemic. Increased staffing shortages and attrition have further strained nursing homes during the pandemic, according to six stakeholders. Early in the pandemic, acute care and critical access hospitals nimbly redeployed nurses, physicians, and equipment to emergency and intensive care units to address a potential surge in admissions caused by COVID-19. In comparison, nursing homes hoped the staff scheduled for each shift would report to work despite the acute illness that residents exhibited and the risk of COVID-19 infection to these staff and their families. As mentioned, low pay and part-time work has prompted some nursing home staff to work more than one job, which increases the risk of COVID-19 transmission across multiple health care facilities.[41] One stakeholder reported that nursing homes in his constituency lost 13-35 percent of their workforce once routine COVID-19 screenings of workers began. According to another stakeholder, one provider in the Midwest reportedly shut down its facility because none of the staff scheduled to work reported for their 7 a.m. shift. In response to low pay, poor working conditions, few or unaffordable health benefits or health insurance,[12] and the high risk of exposure to COVID-19 infection without proper PPE, some nursing home staff are leaving the sector during this critical time when there is an increased demand for their skills and expertise.[42]
| "If you're a low wage worker, and you don't want to risk yourself, your family, or your residents, you're going to make the choice--if you can financially afford it--to not work. Because many nursing homes are struggling with recruitment and retention, it can mean that they sometimes don't have a backup plan when a worker chooses not to go to work." |
The COVID-19 pandemic has imposed even greater demands on nursing home staff. The pandemic and the corresponding infection-prevention and control practices increased demands on nursing home staff, escalating an already critical shortage, according to the six stakeholders. Three stakeholders said that staff responsibilities and the time required to deliver care expanded because of changes in their unit's environment. For example, the additional demands imposed by the COVID-19 response include the following:
-
Additional precautions and training needed to reduce both airborne and contact exposure to the virus, and the need to isolate residents to prevent the infection from spreading created challenges for the workforce in terms of meeting the needs of all residents in a timely fashion. This slowed the pace of routine care provided to residents and interrupted the nursing staff's monitoring of residents at risk of falling, in need of assistance with feeding, and other critical care.
-
The need for staff to help deliver meals to rooms and assist residents individually at mealtimes increased due to the suspension of group dining.
-
The need to move residents to single rooms or for cohorting purposes became more frequent and has increased the demand on staff time.
-
The required screening of staff and visitors, such as contractors and vendors, for COVID-19 symptoms has pulled nurses away from their routine duties. This issue will persist as some states and the Federal Government require routine testing of staff on site, and RNs may likely administer the tests to staff.[43]
-
There has been an increase in the time that dedicated staff spend on facilitating both telehealth visits with providers and telephone and outdoor visits with family. For example, residents with dementia and those with limited mobility or impaired vision require support to use tablets so that they can participate in telehealth visits and remain connected to their families.
New workforce challenges that have emerged during the pandemic stem from a lack of critical resources. New workforce challenges that nursing homes are confronting during the pandemic are varied, according to the stakeholders we interviewed, but they all stem from the lack of critical resources. Six stakeholders reported that access to PPE for the direct care workforce is a major issue, as many staff reportedly did not receive adequate amounts of PPE nor were paid well enough to match the risk level to which they were now exposed. One of these stakeholders noted that inadequate testing for staff and residents led many staff to leave their jobs as a result. Three stakeholders said that closing schools and a lack of childcare coverage prompted many staff to stay home to care for their children. One stakeholder characterized the lack of daycare as having a "profound impact on the workforce," increasing staff shortages especially because grandparents cannot care for children now that they are vulnerable to COVID-19 infection.
| EXHIBIT 4. Workforce Challenges in Nursing Homes Stemming from COVID-19 and Strategies Implemented to Mitigate Challenges | ||
|---|---|---|
| Challenges Identified by Stakeholders | Strategies Implemented to Mitigate Challenge | Summary of Insights and Recommendations from June 2020 Stakeholder Interviews to Further Address Challenges |
| Inadequate workforce capacity | ||
| Staff shortages (6 stakeholders) |
|
|
| Retention of staff (5 stakeholders) |
|
|
| Increased demands on nursing home staff (3 stakeholders) |
|
|
| Lack of critical resources | ||
| Fear of exposing family members to virus (2 stakeholders) |
|
|
| Inadequate availability of PPE (6 stakeholders) |
|
|
| Difficulties accessing and paying for testing (4 stakeholders) |
|
|
| Lack of access to childcare (3 stakeholders) |
|
|
| Infection-prevention control | ||
| Inadequate infection-prevention training (3 stakeholders) |
|
|
| Lack of non-punitive sick leave policies (2 stakeholders) |
|
|
NOTE: Semi-structured interviews with 9 stakeholders conducted between June 6, 2020, and June 24, 2020, and systematic review of state and federal policies conducted through June 21.
|
||
B. What New Policies and Practices have been implemented to Address Challenges related to the Direct Care Workforce and Nursing Home Operations?
The COVID-19 pandemic is an emergency on a scale and of a nature that has proven difficult for nursing homes to tackle. Many nursing homes found themselves inadequately staffed, financed, and equipped to address the pandemic within their facilities. This section describes several strategies that nursing homes--along with federal and state governments--have adopted to mitigate the impact of COVID-19 on direct care workers and to maintain adequate staffing levels.
1. Policies and Practices for Mitigating Staffing Shortages
Six of the nine stakeholders interviewed for this study cited staffing shortages as the primary challenge that nursing homes faced even before the COVID-19 pandemic; three stakeholders drew contrasts between the ability of nursing homes and the ability of hospitals to attract and retain staff. According to one stakeholder, one of his organization's members reported that two RNs left their positions in nursing homes to work in hospitals because they were offered a substantially higher salary plus a $20,000 signing bonus. Nursing homes and policymakers are adopting several policies and practices to mitigate the impact of COVID-19 on staff in an attempt to maintain adequate staffing levels. Most common among those strategies are: (a) developing new recruitment infrastructures; (b) altering licensing and credentialing policies; and (c) deploying non-traditional staff for surge support.
a. Recruitment and Hiring Infrastructure
To facilitate recruitment and hiring during the COVID-19 pandemic, some states expanded the infrastructure that connects health care professionals to open positions in nursing homes. States such as Louisiana, Massachusetts, North Carolina, West Virginia, and Virginia accelerated recruitment by developing online portals designed to connect volunteers and unemployed medical professionals with nursing homes in need of personnel.[44] For example, the Louisiana Department of Health launched Louisiana Health Work Connect, a website to which health care professionals can submit resumes and nursing homes can post staffing needs.[45] The Department of Health uses information posted to the site to match nursing homes with candidates that meet their staffing needs. MassHealth, the state Medicaid program in Massachusetts, developed a similar portal and further incentivized applicants by providing a $1,000 signing bonus to those who secure a position through the site.[46] Other states, such as Virginia and West Virginia, are using portals and databases to recruit, deploy, and track volunteers willing to provide medical surge support during the emergency.[44]
b. Licensing and Credentialing Policies
Attracting new staff during the pandemic was sometimes hindered by rigorous licensing, credentialing, and training standards by the state and federal governments. To diminish these obstacles, federal and state agencies and trade associations relaxed licensing, credentialing, and training requirements to create greater flexibility for existing staff and to facilitate the quick entry of new personnel. For example, CMS waived policies requiring CNAs to meet the 75-hour training and certification requirement within 4 months of employment, and CMS reduced the training requirements for paid feeding assistants from 8 hours to 1 hour.[47] National credentialing organizations also altered standards. The American Healthcare Association, for instance, offered a "temporary nurse aide" training, which at least eight states are accepting as sufficient preparation for new nurse aides or for existing staff who are transitioning to different direct care roles to meet new demands.[48]
Stakeholders interviewed expressed mixed feelings about CMS waivers relaxing licensing, credentialing, and training requirements. Three stakeholders said that the waivers are helpful policies in some respects, but two others expressed concerns about the sustainability of "under-trained workers performing important, skilled functions" as the crisis stretches on for months. In contrast, one stakeholder conveyed that the waivers allowed nursing homes to adopt an "all hands on deck" approach in which staff could be quickly redeployed to fill under-staffed positions. However, this stakeholder also stated that waiving training requirements for staff without nursing home experience could pose a significant safety risk to residents and impede the work of experienced nursing home staff.
Several states have developed strategies to improve staff capacity in nursing homes. Florida, Indiana, Kansas, and Wisconsin relaxed training requirements for CNAs, nursing aides, and feeding assistants to increase the pool of potential employees.[44] Arizona extended license renewal deadlines to avoid lapses, allow for the immediate reactivation of recently lapsed licenses, and issue provisional licenses to job applicants who met all requirements for a health care position but had not yet taken a certification examination.[49] One stakeholder said that licensing, credentialing, and training standards did not change in many states, regardless of federal blanket CMS waivers. The stakeholder posited that state legislatures must often enact new policies to make federal modifications effective, and many legislatures neglected to take up such legislation.
Several states that experienced a surge of COVID-19 cases early on were not part of the Enhanced Nursing Licensure Compact (eNLC), legislation which allows licensed nurses to practice across state lines by aligning licensure standards in eNLC participant states. These states--including California, Connecticut, Massachusetts, and New York--removed restrictions on out-of-state health care workers.[50] Three stakeholders cited improved interstate compacts as a policy that may improve nursing home staffing. One stakeholder noted that in almost all crisis situations, states scramble to allow health care workers to practice across state borders. The stakeholder also proposed that a standing set of executive orders should exist to quickly facilitate cross-border practicing. This stakeholder also noted that the waivers are often applicable only to nurses, but nursing homes could greatly benefit from similar waivers for CNAs and other direct care staff.
c. Non-traditional Staff for Surge Support
Altering state licensing, credentialing, and training policies also enabled nursing homes to use non-traditional staff for surge support and to address critical staffing shortages. For example, California and South Carolina allowed emergency medical technicians to function as nurses' aides.[47] Similarly, waivers in New Jersey allowed registered medical technicians and certified home health aides to function as certified CNAs.[51]
In states and localities where staffing shortages were persistent, nursing homes leaned heavily on National Guard units for key support functions. For example, in Alabama and New Mexico, National Guard teams were deployed to help nursing home staff disinfect facilities in which some residents had COVID-19.[52] National Guard teams also distributed PPE, trained nursing home staff in how to use PPE properly, administered COVID-19 tests to staff and residents, and supported care for residents in nursing homes hard hit by the outbreak.[53]
In some states, the timing at which National Guard units were mobilized may have prevented them from making the greatest impact in helping to slow and stop transmission of the virus in nursing homes. One stakeholder reported that staffing support from National Guard units would have been more helpful if they were mobilized earlier in the crisis; the stakeholder's facilities in Massachusetts were first offered staffing support from the National Guard staff in early May, after the initial surge of the pandemic.
2. Policies and Practices Employed by States and Nursing Homes for Retaining Staff
Retaining nursing staff has been a critical aspect of addressing staff shortages but doing so became increasingly difficult during the first peak of the pandemic. Federal, state, and local governments, as well as nursing homes, employed policies and practices designed to keep staff on the job; these often took the form of: (a) increased wages; (b) augmented non-wage benefits such as childcare; (c) housing; (d) transportation assistance; (e) food supports; and (f) crisis resources. Adequate access to PPE and paid sick leave are also critical to staff retention; more information on these topics can be found in Section C on infection-prevention and control policies and practices.
a. Increased Wages
Some states have provided direct or indirect financial support to nursing home staff by increasing wages to boost retention during the COVID-19 pandemic. For example, Michigan provided a $2 per hour hazard pay increase for direct care workers; the increase was appropriated from the federal relief fund and applied from April through June 2020.[54] Other states provided funds directly to nursing home staff through stipends. For example, New Hampshire's Long-Term Care Workforce Stabilization Program provided full-time, direct care workers with $300 per week stipends (or $150 per week for part-time workers) in addition to regular pay, through July 31, 2020.[55] Other states, such as Connecticut, Maine, and Massachusetts temporarily enhanced Medicaid reimbursement rates to provide bonuses or extra overtime compensation.[56] A National Investment Center for Seniors Housing and Care survey of 105 senior housing and SNF executives found that many nursing homes are raising wages on an hourly basis in the same way that Michigan is doing.[57] However, the increases which are often limited in their duration can take many forms, including shift differentials, incentive pay, stipends, and bonuses. One stakeholder reported that facilities with COVID-19 units have often made payment differentials more robust during the pandemic.
b. Childcare
For nursing home staff with children at home, the closing of schools to reduce the spread of COVID-19 left the staff patching together a system of childcare with extraordinarily limited resources. Recognizing that school closures may prevent frontline workers from reporting for work, many states are providing childcare support for essential workers, including nursing home staff. Some states, such as Minnesota, Oregon, and Washington, ordered public schools to provide emergency childcare for health care workers.[58, 59, 60, 61] Other states are providing childcare stipends to frontline workers, although the utility of the stipends was limited during the early phase of the pandemic when childcare centers were closed to limit exposure. Connecticut, for example, offers full-time frontline workers $200 per child each week (a maximum of $500 per family) through its Frontline Workers Childcare Program,[62] and Colorado is issuing essential workers a 100 percent tuition credit for use at licensed childcare facilities.[63] New York City opened "regional enrichment centers" for children of parents in essential positions.[64]
Some nursing homes attempted to fill the gap in childcare by providing direct support to employees. For example, a number of nursing homes and senior care facilities included a childcare stipend in their employee benefit programs in light of COVID-19. Other facilities, such as Garden Spot Village in New Holland, Pennsylvania, are providing on-site childcare for their workers.[65]
One stakeholder noted that state and local efforts to secure childcare for nursing home staff is essential. The stakeholder made the point that many nursing home staff do not have paid leave or childcare while schools are closed, creating a situation in which they must choose between caring for their children and earning a wage. The same stakeholder also commended nursing homes that are providing on-site childcare but noted that licensing for daycare has made implementation challenging, contributing to the already heavy burden on the workforce and providers.
| "The shutdown of schools and other businesses had a profound impact on the workforce due to lack of daycare. With the elderly being more at risk, grandparents couldn't care for them either. So, we lost a lot of the workforce." |
c. Housing
Essential workers, including CNAs and other health care workers, may be afraid to go home at the end of their workday because of the risk of exposing their family members to COVID-19. In response, cities and states partnered with hotel chains, rental companies, and universities to provide temporary housing for essential workers, including nursing home staff. The partnerships allowed frontline staff at risk of COVID-19 exposure to reduce the likelihood of transmitting the virus to their families. New York City, for instance, developed a program that enabled health care workers to stay free of charge at hotels near their places of work. The city also offered free Airbnb and hotel rooms to workers who tested positive for COVID-19 and were unable to self-isolate at home.[66] Similarly, the California Healthcare Workers Program provided hotel rooms to health care workers who were exposed to, or tested positive for, COVID-19.[67] Rhode Island worked with universities to provide single-occupancy dorm rooms to frontline workers.[68] New Orleans, among other cities, partnered with Airbnb to house medical workers.[69]
d. Transportation Assistance
With many cities limiting public transportation schedules to adjust for the drop in ridership during the COVID-19 pandemic, some nursing home staff were having trouble commuting to and from work. Some metropolitan regions, such as Minneapolis-Saint Paul, are offering solutions to this transportation problem.[70] The twin cities' Metropolitan Council is providing door-to-door transportation for frontline health care workers by using city vehicles, and Wisconsin's government recommended that nursing homes provide workers with access to free ride services or rental vehicles.[71]
e. Food Supports
A survey by McKnight's Long-Term Care News in late March asked nearly 500 long-term care facility managers what strategies they are using to "keep the staff's spirits up." McKnight found that food is the most popular strategy for boosting staff morale. Many facilities, for example, have been giving staff daily meals, occasional food deliveries, groceries, and/or snacks as an incentive to stay on the job.[72] Another survey of 105 executives in senior housing and SNFs conducted from April 13, 2020 to April 19, 2020, by the National Investment Center for Seniors Housing and Care found that approximately one-third of senior housing and SNF operators have been supporting staff by providing to-go meals for them and their families.[57]
f. Crisis Resources
The COVID-19 pandemic has imposed anxiety, grief, and fatigue on nursing home staff, as increased responsibilities and care for severely ill residents--many of whom do not recover--takes an emotional toll. State and federal agencies have developed guidance for health care providers, including nursing home managers, to foster mental wellness during the pandemic, including links to crisis resources and tips for coping with stressful situations at the individual and facility level. The CDC published guidance on identifying and coping with stress for frontline health care providers.[73] The guidance also included a directory of help lines and mental health providers. Similarly, the HHS Office of the Assistant Secretary for Preparedness and Response (ASPR) released a guide for health care leaders on how to "Mitigate Absenteeism by Protecting Healthcare Workers' Psychological Health and Well-being during the COVID-19 Pandemic," which provides actionable strategies for reducing stress and burnout among health care workers.[74] The CDC and ASPR also combined resources with the National Emerging Special Pathogens Training and Education Center to develop and host the webinar "Resilience and Care of the Caregiver."[75] The webinar provided health care leaders with tools to build staff resilience, provide peer support during the pandemic, and make behavioral health referrals.
| "Although frontline nursing home staff are accustomed to advanced illness and caring for people as they approach the end of life, the number of people who were very ill and required end-of-life care was difficult. Staff knew what to do, but the mental toll was impactful." |
State toolkits addressing best practices during COVID-19, such as Minnesota's Long-Term Care Toolkit, often include sections with advice on safeguarding the mental well-being of staff during the pandemic.[76] Some states went beyond providing guidance and implemented new mental health wellness programs for health care providers. For example, Maryland launched a COVID-19 Crisis Support Program, which provided mental health support to employees of Maryland's nursing homes.[77] The program's services included individual counseling, self-care webinars, management consultation related to improving the staff's well-being, group support for teams, and debriefings after traumatic incidents. Other states established mental health hotlines. For instance, Ohio's COVID CareLine is an emotional support phone service that is available to health care professionals and the general public.[78]
C. What Types of Infection-Control Challenges are Nursing Homes Facing during the COVID-19 Pandemic?
The potential for the quick transmission of COVID-19 in nursing homes underscores the risks to the safety of staff and residents and the importance of applying strong infection-prevention practices when delivering care. The stakeholders shared their perspectives on infection-prevention and control during the pandemic and cited several challenges including: (1) the lack of a unified testing strategy; and (2) workforce safety, including access to PPE.
Lack of a unified testing strategy has hindered efforts to contain the outbreak. The lack of a unified testing strategy, test kits, and an approach to covering the cost of testing left all nine of the stakeholders dismayed and reportedly created confusion across the long-term care continuum about how, who, and when to test. One stakeholder conveyed that CDC guidelines allowed for two separate testing strategies, either a symptom-based strategy or a testing-based strategy.[80] As the symptom-based strategy often allowed a health care worker to return to work sooner than the testing strategy--which required obtaining two negative tests more than 24 hours apart--some facilities chose to use this strategy rather than test staff. Moreover, although these testing strategies were recommended by the CDC, they were not mandated nor paired with funding. Three stakeholders stressed the importance of providing financial coverage for the testing rather than passing the costs on to providers and staff. One stakeholder explained that a state issued a mandate requiring all nursing home and long-term care staff to be tested every 2 weeks. The state planned to distribute kits to the nursing homes, but it did not provide the means to cover the cost of either administering the test or being tested; some nursing homes plan to pass the cost for receiving a test on to staff. In addition, the state did not make any provisions for testing nursing home residents. By contrast, CMS guidance for reopening nursing homes recommends weekly testing for staff and baseline testing for all residents.[79, 82]
In other states, testing is left up to individual facilities. According to another stakeholder, if staff who tested positive for the virus wish to return to work, the person has to test negative twice according to early CDC guidance. Because of the backlog at laboratories, staff had to wait up to 10 or more days before returning to work. However, if these absences were determined on the basis symptoms, and a test had not been administered, staff could return to work after 7 days as long as they were symptom free. Since a positive test result may lead to longer absences because of a laboratory backlog and re-testing, a perceived increase in absences and, in some instances, lower pay and no sick leave for workers made some nursing homes reluctant to provide tests and some staff reluctant to be tested. The stakeholders reported that in some instances, staff opted to stay home for a few days if they developed COVID-like symptoms. The CDC recommended that isolation should continue for 10 days from the onset of symptoms; this recommendation and the stakeholders' comments suggest that there is a need to amplify CDC guidance.[81]
Workforce safety remains an area of concern. The pandemic introduced infection-prevention and control-management activities that are straining supply chains and nursing home administration. In May 2020, the CDC released options for managing PPE when providers and facilities encounter a surge in patient volume and the need to conserve PPE. The CDC applied a surge capacity framework to PPE conservation and suggested three new strata for guiding PPE use: (1) conventional capacity; (2) contingency capacity; and (3) crisis capacity.[83]
The limited supply of PPE and the CDC's suggested strategies for conserving PPE based on patient census created tensions between suppliers, providers, and workers. Prices for PPE soared at the start of the pandemic, with prices increasing by over 1,000 percent by April 7, 2020.[84] Six stakeholders reported that some facilities ran out of PPE during the pandemic. One stakeholder described situations in which staff were not provided with the necessary PPE, or they were instructed to reuse their masks for several weeks. In one nursing home, an employee filed a complaint with the Occupational Safety and Health Administration and the American Health Care Association because PPE was not available. After the complaint, the nursing home reportedly held a staff meeting to discuss PPE, informing staff that additional complaints would make PPE less available. Furthermore, staff reported that management accompanies them when agencies and advocacy groups visit the site. In these instances, the staff reported that they "have everything they need" out of fear of retaliation for reporting shortages of PPE. According to this stakeholder, nursing homes continue to operate and ration PPE as if they are in a crisis mode, and this far into the pandemic, nursing homes ought to be operating in a conservation mode.
| "There has been evidence that nursing home staff are not washing their hands as often as they should...if they're not washing their hands, it's because they have 27 residents [to care for at a time]. You have to make a decision - do you want them to stop and wash their hands before they run and catch your mother from falling off the toilet? These are the decisions CNAs have to make." |
In contrast, another stakeholder explained that providers reported that the availability of PPE has improved, although many continued to encounter challenges in procuring gowns and N95 masks. Supplies continue to be reused, and most nursing homes are not yet implementing conventional practices. This stakeholder believed that some nursing homes may be answering questions about PPE availability based on the CDC-defined conservation methods as opposed to conventional methods. This stakeholder explained that most providers they spoke with are at conservation levels but do not want to reveal this status for fear of being identified in an infection-control survey as having a deficiency and then face fines and liability issues. Although four stakeholders said that the availability of PPE has reportedly improved somewhat since the outbreak, it remained an issue at the time the interviews were conducted. Compounding the threat to worker safety is the confusion among some providers about consistently applying conservation and conventional PPE management guidance from the CDC.
One stakeholder spoke from experience with successful infection-control training in which an infection-prevention team monitored every shift and provided immediate feedback to staff on how to detect and correct issues. The stakeholder explained that this approach gave staff the knowledge they needed and some comfort with what they were being asked to do when caring for residents. However, the staff's uncertainty about COVID-19, not knowing which residents have the virus, and whether there is asymptomatic transmission, reportedly continued to present challenges.
D. What New Policies and Practices have been implemented by Federal and State Governments to Address Challenges Related to Infection-Prevention and Control, and Nursing Home Operations?
During the outbreak, federal and state governments implemented several policies and practices designed to prevent and control COVID-19 infections among nursing home staff and residents. These policies include increasing access to PPE, creating non-punitive leave policies, and regularly monitoring staff for illness.
1. Access to PPE
Both federal and state governments helped nursing homes obtain additional PPE supplies by distributing PPE to facilities in critical need. Federal Emergency Management Agency (FEMA) coordinated two shipments of 7-day supplies of PPE (including masks, gloves, eye protection, and gowns) to approximately 15,400 nursing homes.[85] The shipments were spread out over 2 months and were intended to supplement other supply efforts by state agencies and provider organizations. The first shipment went to metropolitan COVID-19 hotspots such as Boston, Chicago, New York City, northern New Jersey, and the District of Columbia. Smaller metropolitan, urban, and rural areas received shipments later during the outbreak. Nursing homes have publicly expressed concerns about the quality and adequacy of the PPE provided through these shipments, noting sub-standard or expired PPE.[86] Two stakeholders also stated that some materials from the Federal Government were either not well coordinated or not of overall good quality.
Several states set up their own supply programs to facilitate access to adequate PPE. For example, the Massachusetts Department of Public Health and the Massachusetts Emergency Management Agency distributed up to 7 days' worth of supplies to facilities with less than 5 days of PPE in stock, and Washington State implemented a centralized program for emergency restocking of nursing homes.[87] Other states connected nursing homes to PPE providers, such as South Carolina's COVID-19 Emergency Supply Collaborative or North Dakota's PPE Portal, which connects groups in need to individuals and organizations with available PPE. Texas created the Supply Chain Strike Force to increase the supply of PPE by acquiring supplies and initiating new production.[44]
To conserve supplies, nursing homes are testing new strategies to disinfect PPE, made possible by the Food and Drug Administration's (FDA's) Emergency Use Authorization. The authorization allows health care workers to use decontaminated N95 masks. As of the writing of this report, the practice was in use in 35 states and the District of Columbia. For example, nursing homes managed by Haven Health Group and Pioneer Health Group in Arizona used ultraviolet (UV) machines to disinfect PPE supplies and employees' personal items.[44]
2. Non-punitive Employee Leave Policies
The CDC recommends that health care facilities "implement sick leave policies that are non-punitive, flexible, and consistent with public health policies" so that workers feel comfortable to stay home if they are ill and prevent further spread of COVID-19 or other contagious illnesses.[88] Many state governments provided similar recommendations when crafting guidance to nursing homes. For example, Texas encouraged facilities to review and revise sick leave policies that penalize staff by diminishing their wages or benefits.[89] Connecticut backed this recommendation with financial incentives; its Department of Social Services Coronavirus Relief Fund requires nursing homes to provide paid sick leave to staff in order to qualify for a grant.[90] Some nursing homes responded to the CDC's recommendations and augmented paid sick leave policies. For example, the Avamere Family of Companies, in negotiations with a labor union, implemented several sick leave policies designed to support ill employees and reduce the transmission of COVID-19.[92]
Many nursing homes, however, still have penalizing sick leave policies (policies that penalize staff by diminishing there wages or benefits), even if direct care workers have contracted COVID-19 or are experiencing symptoms. The Federal Families First Coronavirus Response Act, signed into law on March 18, 2020, provides an allowance for employers of health care providers to exclude some employees from the expansion of Family and Medical Leave Act (FMLA). The expansion of this act provides job security and enables eligible workers to take leave under the FMLA. Nursing staff who work part-time or who have low earnings may not qualify for or can afford using the FMLA as the expansion intended. As a result, a national survey of nursing home staff fielded from May 20, 2020, through June 7, 2020, found that 72 percent of staff reported that their employers are not providing paid sick leave if they are required to self-quarantine for 2 weeks because a suspected COVID-19 infection.[91]
Other human resource policies designed to keep healthy workers on the job may also incentivize ill staff to continue working. One interviewed stakeholder said that some nursing homes are providing attendance bonuses to staff who do not call in sick. Some of these nursing homes do not offer paid time off (PTO) to ill staff. The policies, therefore, work together to encourage nursing home staff to work while they are sick.
3. Monitoring Staff for Illness
CMS, the CDC, and the states have issued guidance to nursing homes on how to monitor the health of staff and under what conditions staff who have symptoms or who tested positive for COVID-19 can return to work. The CDC guidance as well as state guidance emphasizes that health care workers should be screened for fever and respiratory symptoms at the beginning of every shift[93] Los Angeles County recommends monitoring twice daily, and Texas recommends that facilities ask staff to self-monitor on days when they are not working.[89, 94]
In addition to regular monitoring, the CDC recommends that nursing homes develop and execute plans for testing health care providers for COVID-19. The CDC also recommends that all CNAs and other ancillary staff receive a baseline COVID-19 test, with re-testing continuing each week. The weekly testing recommendation may be adjusted based on the prevalence of the virus. In addition, any nursing home employee who provides care to residents and who has symptoms of COVID-19 should be tested immediately and then sent home. If a case is confirmed, the CDC recommends that the facility test all providers and continue testing every 3-7 days until 14 days pass without a positive result. These recommendations can be altered if a facility has limited testing capacity.[88]
| "A lot of [staff] who have left nursing homes because of COVID may not come back. There's going to be a greater shortage going forward. [COVID-19] has uncovered a terrible issue that's been there for decades. People in long-term care have been advocating for decades to try to get things changed...but people in nursing homes can't go to Capitol Hill." |
Several states have also developed their own testing requirements for nursing home staff. Arizona, Illinois, New York, Pennsylvania, Texas, and Wisconsin require all nursing home staff to receive a baseline test to determine their current COVID-19 status, with New York requiring all personnel to be tested twice per week thereafter.[44] States such as New Mexico, Vermont, and West Virginia, mandated baseline testing at any facility with a reported case.
Overall, state guidance on return-to-work policies refers to the recommendations established and updated by the CDC. However, some states were delayed in revising their policies to adhere to updated CDC guidance. For example, the CDC updated their guidance to restrict asymptomatic staff with confirmed COVID-19 from returning to work until 10 days after illness onset, rather than 7 days, on April 13, 2020; the New Jersey Department of Health updated the guidance from 7 to 10 days on May 15, 2020.[95, 96]
III. CONCLUSION
The COVID-19 pandemic imposed immense challenges on the nursing home workforce, compounding pre-existing difficulties with hiring and retaining nursing staff. Stakeholders interviewed for this study cited staffing shortages as the primary challenge that nursing homes faced before and during the COVID-19 pandemic. During the early phase of the outbreak, nursing homes grappled with how to retain adequate staffing while rapidly making operational changes to ensure the safety of workers and residents. In turn, direct care workers need to balance concerns about their own safety, the well-being of the residents they care for, and their financial stability during the pandemic.
To maintain adequate staffing levels, federal and state government agencies, as well as nursing homes, altered their standard policies and practices to mitigate the impact of COVID-19 on the nursing home workforce. Several states took an active role in strengthening the sector's recruitment infrastructure to quickly engage volunteers and hire health care professionals during the pandemic. Federal and state agencies and trade associations also relaxed licensing, credentialing, and training requirements to facilitate the entry of new direct care staff into nursing homes and other health care facilities responding to increased needs. Federal relief programs, such as the PPP, also provided short-term financial assistance to many small businesses, including nursing homes, to help maintain staffing levels. Further, some nursing homes revised their human resources policies to support workers who may be personally and financially impacted by COVID-19.
The nursing home workforce also confronted new challenges during the pandemic that stem from a lack of critical resources, such as childcare coverage, which escalated critical shortages of staff. To retain nursing staff, nursing homes and state and local governments employed several strategies to support staff to stay on the job. These strategies often took the form of increasing nursing home staff wages through hazard pay or weekly stipends; augmenting non-wage benefits such as childcare, housing, transportation assistance, and food supports; and providing mental health support to help nursing home staff cope with the anxiety, grief, and fatigue they experience on the job as a result of COVID-19.
The pandemic imposed greater demands on nursing home staff, such as new infection-prevention and control measures like screening, testing, and cohorting instituted to minimize transmission and contain the spread of the virus. Interviewed stakeholders reported that early in the pandemic, the lack of a cohesive testing strategy and funding to cover the cost of testing for COVID-19 created confusion about how, who, and when to test. Also, the limited supply of PPE reportedly resulted in some nursing home staff having to reuse their supplies which may have threatened the safety of both workers and residents.
Although many nursing homes operated under resource constraints early in the pandemic, several federal initiatives designed to strengthen nursing homes' capacity to respond to COVID-19 have been implemented or announced since the completion of this study. These initiatives, summarized in the Addendum, include: (1) an additional $5 billion in funding through the CARES Act to address critical needs in nursing homes; (2) rapid point-of-care diagnostic testing devices that will be distributed to nursing homes to enhance efforts to keep the virus from entering and spreading throughout nursing homes; and (3) on-site education and support to nursing homes experiencing outbreaks to help reduce transmission of COVID-19 spread among residents and staff. This multi-prong approach announced on July 22, 2020, promises to equip the nursing home workforce with enhanced resources to more fully respond to the outbreak.
Based on these developments and findings from this study, we have identified several opportunities for future research. These include examining how nursing homes have taken advantage of federal initiatives implemented in response to COVID-19; assessing which resources have directly impacted the capacity of the nursing home workforce; understanding which interventions have had the greatest impact on how nursing homes have responded to COVID-19; and understanding any long-lasting effects of the pandemic on the nursing home workforce including the prolonged physical and emotional toll, burnout, and fatigue. Additional work in this area can help improve the nursing home workforce, improve resident care, and ensure adequate protections are in place for future emergencies.
NOTE: The systematic policy review that informed this report was completed in late June 2020 as the pandemic was ongoing. Federal, state, and facility policy are likely to evolve over time, impacts of the pandemic and these policies will undoubtedly change, and many temporary policies will come to an end. Since the completion of this policy review, as of September 2020, federal and state governments and nursing facilities have continued to implement new policies and initiatives in response to the challenges the COVID-19 pandemic continues to impose on a disproportionate number of nursing homes in the United States. Relevant federal policies instituted since the policy review for this study concluded, from July 2020 through the publication of this report, are summarized in the Addendum.
APPENDIX
A. Stakeholder Interviews
1. Process for Identifying, Engaging, and Interviewing Stakeholders
We interviewed nine stakeholders for this study; many were leaders of national associations who shared the perspectives of their constituent members, which included nursing homes, direct care staff, and special needs plans. To recruit stakeholders for this study, we compiled a list of leaders in the long-term industry to invite to participate in an interview. With ASPE project staff input, we engaged ten leaders who have deep insight into the workforce challenges affecting nursing homes during the COVID-19 pandemic. We attempted to establish contact via email and telephone. After stakeholders expressed interest in participating in the study, we arranged the interviews and provided the topics that would be covered during the discussion. Nine stakeholders ultimately agreed to participate in a semi-structured interview (Exhibit 5). Interviews were conducted via telephone during June 2020. Seven of these interviews were recorded for note-taking purposes. The ASPE project staff requested we share the recordings and notes (when recordings were not available) with ASPE staff working on this project.
| EXHIBIT 5. Stakeholders that Participated in a Semi-Structured Interview | |
|---|---|
| Stakeholders' Organizations | Perspective |
| American Health Care Association and National Center for Assisted Living | National association representing for-profit and non-profit nursing homes |
| Genesis Healthcare | Nursing home provider |
| Johns Hopkins School of Nursing, Center for Innovative Care in Aging | Academic research center |
| Justice in Aging | Advocacy organization |
| LeadingAge | Professional association representing long-term care service providers |
| National Association for Health Care Assistants | National association representing direct care staff |
| Paraprofessional Healthcare Institute | National association representing direct care staff |
| Service Employees International Union | Labor union representing direct care staff and other workers |
| SNP Alliance | National association for special needs plans |
2. Approach to Developing the Data Collection Tools
In collaboration with ASPE project staff, we developed two interview guides, one for stakeholders representing the perspective of nursing home providers and one representing the perspective of national leaders within the direct care workforce and nursing home industries. The interview guides covered the following topics:
-
Background on stakeholder's role and organization.
-
Nursing home workforce.
-
Infection-prevention and control practices in nursing home settings.
-
New federal or state policies and practices that have been implemented to address workforce challenges in nursing homes.
These guides included interview questions and prompts to facilitate a free-flowing conversation and uncover rich insight into the types of workforce challenges nursing home staff have been confronting during the COVID-19 pandemic. The guides were designed to increase both the overall yield and the quality of information generated from a research interview. For example, we used plain language when designing the guides to require minimal interpretation for stakeholders participating in an interview. For the direct care providers, we asked the stakeholder to provide relevant information about the facility's capacity, case mix, and population before the interview. After each interview, the task lead conducted a high-level review of transcribed notes to identify missing and inconsistent data. All data (including recording and transcript notes) were stored on a secure server, accessible only to relevant project staff. We identified follow-up questions in collaboration with ASPE project staff and sent these via email to participating stakeholders to fill gaps in understanding.
3. Analysis Methods
We employed standard qualitative methods to develop insight into the effects of the COVID-19 emergency and the recovery response. This analysis was based on data gathered through the interviews that involved five steps:
-
We first transcribed all interviews within 24 hours after completion of each interview.
-
Second, we developed an analytic framework to organize the data for analysis. We constructed this framework by using an Excel workbook to capture information generated from the interviews as well as respondent-level (that is, nursing home industry representative, direct care provider, advocacy organization, etc.) characteristics for stakeholders who participated in an interview. Including these characteristics in the analytic file allowed us to identify themes across respondent types and to inform our interpretation of the data.
-
Third, two research staff independently entered qualitative data from the interviews into this Excel workbook.
-
Fourth, we analyzed the data in the workbook to identify emerging themes that addressed our research questions, factoring in stakeholder characteristics such as whether they were an advocate who was somewhat removed from care delivery or a direct care provider who offered deeper insight into what nursing home (that is, nursing home industry representative, direct care provider, advocacy organization, etc.) staff were experiencing on the frontlines of the pandemic. Two research staff independently identified key themes that emerged from the data and met to reach consensus and resolve any disagreements. This process ensured that the themes identified were consistent and opened opportunities for novel interpretations of the data.
-
Fifth, we analyzed the qualitative data to quantify emerging themes that addressed the project research questions.
B. Systematic Policy Review
The objective of our systematic policy review was to document federal, state, and local laws, regulations, policies, waivers, and practices designed to help nursing homes during and after the COVID-19 pandemic, with attention focused specifically on nursing workforce challenges.
We started this work by developing a set of search terms to identify relevant media coverage, industry reports, grey literature, and policy guidance released by federal, state, and local government agencies. We developed these search terms in consultation with ASPE project staff and a Mathematica library specialist, who also provided advice on the most effective search strategy.
After solidifying the terms, our library specialist used Nexis, the Harvard Kennedy School Think Tank Directory, and a custom Google search to obtain publicly available material related to nursing home staff/workforce capacity, nursing home working conditions, COVID-19 prevention and treatment for nursing home residents/patients, nursing home payment and delivery system changes, and special liability protections for nursing homes during the pandemic. The search was conducted from June 8, 2020, to June 19, 2020, and we limited it to publicly available information from February 1, 2020 to June 19, 2020. Federal policies instituted after the completion of the systematic policy review are summarized in the Addendum to this report.
The library specialist sorted extant material by relevance. Three analysts then identified sources and information most pertinent to the research objective. For each policy topic, the analysts reviewed 10-15 of the most germane and reliable sources and summarized their findings. To the extent possible, the analysts also gave priority to sources that addressed the potential impact or effectiveness of new policies, including policy changes that were more sweeping and practices that were scalable across different state long-term care systems. The analysts also reviewed policy guidance that had already been compiled, such as the Toolkit on State Actions to Mitigate COVID-19 Prevalence in Nursing Homes released by CMS in addition to documents of interest provided by ASPE project staff.
After reviewing these sources, the analysts reviewed material compiled internally by Mathematica's Medicaid and CHIP (Children's Health Insurance Program) Business Information and Solutions team that is tracking the impacts of COVID-19 on the Medicaid and CHIP programs for the Center for Medicaid & CHIP Services at CMS. The material included a comprehensive list of changes to state Medicaid waivers, Medicaid state plan amendments, and state policies and procedures in response to COVID-19.
Once the analysts completed the literature review and developed policy summaries, the content was reviewed by our quality assurance reviewer and our clinical advisor, Dr. Carol Irvin and Mr. Llew Brown, who are subject matter experts in long-term care policy and in clinical care quality, respectively. Dr. Irvin and Mr. Brown provided constructive feedback on the level of detail in each summary, on the clarity of the content, and made suggestions for adding material that could provide a more complete understanding of a given policy.
C. Gaps and limitations
The systematic policy review that informed this report was completed in late June 2020 during an ongoing pandemic. Some of the findings will have undoubtedly changed, and many temporary policies may be, or will be, coming to an end. This systematic review was also informed by a limited set of stakeholders, including representatives from national associations, nursing providers, professional associations, and advocacy organizations. Since the completion of this review, federal and state governments, and nursing facilities have continued to implement new initiatives in response to the challenges the COVID-19 pandemic continues to impose on a disproportionate number of nursing homes in the United States.
-
Our findings are not broadly generalizable due to a small number of stakeholders. Our research draws heavily on the insight gained from the nine stakeholders who volunteered to participate in the study. Given the small number of stakeholders, the qualitative findings on the challenges facing the nursing home workforce during the COVID-19 pandemic are not generalizable or representative of the experiences of health care workers and administrators across the nursing home industry.
-
Our stakeholder interviews do not include the perspectives of direct care workers, state Medicaid agency staff who oversee the delivery of long-term care, or state Medicaid managed care plans that administer some services in nursing home settings. The stakeholders interviewed for this study included advocates, leaders of professional associations for health care workers and the people they serve, research organizations, and leaders of one large long-term care provider. These stakeholders offered different perspectives on the challenges facing the nursing home workforce and on how nursing homes have responded to the COVID-19 pandemic. Stakeholders' views on new policies and practices that were implemented to address challenges related to the workforce, nursing home operations, and infection-prevention and control are highly idiosyncratic, as they represent their organizations' mission as well as different vantage points of the long-term care continuum.
-
There are gaps in publicly available information on private payers, managed care organizations, and private nursing homes. Although we worked with a Mathematica library specialist to develop a Google Custom Search, a Nexis search, and a search of the Harvard Kennedy School Think Tank Directory to draw upon different sources of gray literature, we were unable to uncover certain insights about nursing home operations. For example, our search returned no material about policies and programs funded by private payers or managed care organizations. In addition, we obtained little publicly available information about private nursing home operations, guidance, or practices. This limitation may reflect a gap between the results of the state and federal policy review and what is occurring "on the ground" in nursing homes.
-
Health care policies and practices related to COVID-19 and the nursing home industry are rapidly changing in response to emerging challenges. In our review, we gave priority to policies, regulations, and practices disseminated most recently. To stay abreast of new developments, we also attended most daily 20-minute webinars convened by the Rapid Response Network for Nursing Homes. However, the systematic policy review included sources identified through June 19, 2020. As a result, more recent policies, programs, regulations, guidance, and news reports are not reflected in this report. In the Addendum, we have summarized relevant federal policies instituted since the policy review concluded, from July 2020 through the publication of this report.
-
Results of the systematic review of state and federal policies were limited to those from three databases: Google Custom Search, Nexis, and the Harvard Kennedy School Think Tank Directory. Mathematica Library Services staff advised our team that these three databases were most likely to produce grey literature and media articles related to our search domains. Other databases may also have produced helpful material, but the time frame for this project limited our ability to investigate other sources.
ADDENDUM
Mathematica completed the systematic policy review in late June 2020 that informed this report. Since the completion of this policy review, the Federal Government has instituted new initiatives to respond to the challenges the COVID-19 pandemic is imposing on nursing home staff and residents, including policies that impact the nursing home workforce. Below, we summarize relevant federal policies instituted since the policy review concluded, from July 2020 through the publication of this report.
-
July 10, 2020: CMS announced an initiative to provide additional resources to nursing homes through Quality Improvement Organizations (QIOs). QIOs will work with nursing home providers to improve their quality of care to beneficiaries, prioritizing nursing homes in hotspot areas, small and rural nursing homes, and those with known infection-control issues. QIOs will also provide training and education opportunities to all nursing homes.[97]
-
July 14, 2020: HHS announced a plan to procure and deliver rapid point-of-care diagnostic test instruments and tests to nursing homes to increase capacity for COVID-19 testing. Distribution of these testing instruments will be prioritized in hotspot geographic areas and is intended to supplement nursing homes' current testing capacity.[98] Distribution is scheduled to begin the week of July 20 and will continue over the course of 14 weeks.[99]
-
July 22, 2020: CMS announced that nursing homes in states with a 5 percent positivity rate or greater will be required to test all nursing home staff each week. This new staff testing requirement is intended to identify asymptomatic staff.[30] The interim final rule enforcing this requirement, along with specific guidance on testing and penalties, is released on August 26.[100]
CMS also announced the deployment of federal Task Force Strike teams, composed of clinicians and officials from CMS, CDC, and the HHS Office of the Assistant Secretary for Health. These strike teams will provide on-site assistance to nursing homes experiencing outbreaks on infection-prevention, detecting COVID-19 cases, preventing viral transmission, and managing staff. The goal of these teams is to both implement immediate actions in nursing homes to reduce the spread of COVID-19 among residents, as well as inform the federal, state, and local response.[30]
-
August 7, 2020: HHS announced that $5 billion from the Provider Relief Fund will be allocated to nursing homes and long-term care facilities to support testing, staffing, and PPE needs beginning in mid-August. Payment will be linked to facility performance--taking into account the prevalence of the virus in the nursing home's community--in order to drive quality improvement and hold facilities accountable. Distributions began in mid-August.[101]
-
August 25, 2020: CMS launched a scenario-based training program for frontline nursing home staff and management. The "CMS Targeted COVID-19 Training for Frontline Nursing Home Staff and Management" teaches staff and management best practices they can implement to address COVID-19, based on lessons learned from nursing homes and the federal Task Force Strike teams. Modules for frontline nursing home staff include hand hygiene and PPE; screening and surveillance; cleaning the nursing home; cohorting; and caring for residents with dementia in a pandemic.[102]
-
September 16, 2020: CMS receives the Independent Coronavirus Commission for Safety and Quality in Nursing Homes Commission final report. CMS had tasked MITRE, the operator of the CMS Alliance to Modernize Healthcare (Health FFRDC), with convening a commission of experts to address safety and quality in nursing homes in relation to the public health emergency. The main purpose of the Commission was to gather information from the early days of the pandemic and provide CMS with recommendations to improve infection-prevention and control efforts, safety procedures, and quality of life of residents in nursing home. The report lists 27 recommendations in the areas of workforce, testing and screening, equipment and PPE, cohorting, visitation, communication, technical assistance, and nursing home data. Specifically on workforce, the report recommendations included mobilizing resources to support a fatigued nursing home workforce and assess minimum care standards; providing guidance for nursing home workforce to safely continue to work in multiple nursing homes while following infection-prevention and control practices; supporting 24/7 RN staffing resources at nursing homes in the event of a positive COVID-19 cases; requiring nursing homes to employ infection preventionist(s) with educator capabilities; improving interest in the CNA profession through various recruitment efforts; issuing guidance for on-the-job CNA training, testing, and certification, and creating a national CNA registry; overhauling the workforce in partnership with federal, state, and local authorities, as well as other public, private, and academic partners; professionalizing infection-prevention positions in nursing homes; and convening a Long-Term Care Workforce Commission to assess, advise on, and provide independent oversight for modernization of the workforce ecosystem. Additional recommendations in other categories, but related to workforce, include: developing and executing a national strategy for testing and rapid turnaround of results; providing specific guidance on the use, decontamination, and reuse of PPE, and guidance on training to all clinical and non-clinical facility staff on the correct use of PPE and equipment; updating cohorting guidance to address resident and staff psychological safety and well-being with infection-prevention and control; updating reimbursement policy to address differences in nursing home resources, including staffing resources; providing resources to help nursing home staff assess and improve the mental health and psychosocial well-being of residents during and after the pandemic; and increasing specificity and expanding guidance on communications between nursing home staff, residents, and families.[103]
ENDNOTES
-
American Health Care Association. "Skilled Nursing Care Centers." Available at: https://www.ahcancal.org/research_data/Documents/FastFacts_SNCCs.pdf.
-
Medicare Payment Advisory Commission. Available at: http://www.medpac.gov/docs/default-source/reports/mar20_medpac_ch8_sec.pdf.
-
Centers for Disease Control and Prevention. Available at: https://www.cdc.gov/nchs/fastats/nursing-home-care.htm.
-
CNAs have federally mandated training requirements, while LPN licensure is regulated by state boards of nursing. Both CNAs and LPNs are authorized to assist with the delivery of medical care under the direction of a RN. Personal care aides assist residents in performing the activities of daily living, but do not support the delivery of health care. Training for personal care aides is not federally mandated, though some states and employers may require completion of a training program. (Also see Endnote 5.)
-
National Center for Health Statistics. "Long-term Care Providers and Services Users in the United States, 2015-2016." Available at: https://www.cdc.gov/nchs/data/series/sr_03/sr03_43-508.pdf.
-
PHI. "Direct Care Workers in the United States: Key Facts" July 2020. Available at: https://phinational.org/resource/direct-care-workers-in-the-united-states-key-facts/.
-
For CNAs, see: Legal Information Institute. "42 U.S. Code § 1395i-3--Requirements for, and assuring quality of care in, skilled nursing facilities." Available at: https://www.law.cornell.edu/uscode/text/42/1395i-3.
-
For LPNs, see: National Council of State Boards on Nursing. "What You Need to Know About Nursing Licensure and Boards of Nursing." Available at: https://www.ncsbn.org/Nursing_Licensure.pdf.
-
For personal care aides, see: Abby Marquand and Susan A. Chapman. "The National Landscape of Personal Care Aide Training Standards." Available at: https://healthworkforce.ucsf.edu/sites/healthworkforce.ucsf.edu/files/Report-The_National_Landscape_of_Personal_Care_Aide_Training_Standards.pdf.
-
American Health Care Association Staffing Report 2012. Available at: http://publish.ahcatech.org/research_data/staffing/Documents/2012_Staffing_Report.pdf.
-
Darcie M. Brady. "An Exploration of Nursing Assistants' Perceptions About Job Satisfaction." Available at: https://pubmed.ncbi.nlm.nih.gov/27575800/.
-
Office of the Assistant Secretary for Planning and Evaluation. "Understanding Direct Care Workers: A Snapshot of Two of America's Most Important Jobs." Available at: https://aspe.hhs.gov/basic-report/understanding-direct-care-workers-snapshot-two-americas-most-important-jobs-certified-nursing-assistants-and-home-health-aides.
-
PHI. "Raise the Floor." Available at: https://phinational.org/wp-content/uploads/legacy/research-report/phi-raisethefloor-201604012.pdf.
-
Bureau of Labor Statistics. "Nursing Assistants." Available at https://www.bls.gov/oes/current/oes311131.htm#(1) . Accessed June 28, 2020.
-
Bureau of Labor Statistics. "Registered Nurses." Available at: https://www.bls.gov/oes/current/oes291141.htm.
-
Bureau of Labor Statistics. "Licensed Practical and Licensed Vocational Nurses." Available at: https://www.bls.gov/oes/current/oes292061.htm.
-
PHI. "Workplace Injuries and the Direct Care Workforce." Available at: https://phinational.org/wp-content/uploads/2018/04/Workplace-Injuries-and-DCW-PHI-2018.pdf.
-
Charlene Harrington, et al. "The Need for Higher Minimum Staffing Standards in U.S. Nursing Homes." Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4833431/.
-
Kirsten Black et al. "State-Initiated Nursing Home Nurse Staffing Ratios: Annotated Review of the Literature." Available at: https://aspe.hhs.gov/basic-report/state-initiated-nursing-home-nurse-staffing-ratios-annotated-review-literature.
-
Xinzhi Zhang, David C. Grabowski. "Nursing Home Staffing and Quality Under the Nursing Home Reform Act." Available at: https://academic.oup.com/gerontologist/article/44/1/13/586403.
-
Charlene Harrington. "Nursing Home Staffing Standards in State Statutes and Regulations." Available at: https://www.justice.gov/sites/default/files/nursing_home_staffing_standards_in_state_statutes_and_regulations.pdf.
-
Janet E. Squires et al. "Job Satisfaction among Care Aides in Residential Long-Term Care: A Systematic Review of Contributing Factors, Both Individual and Organizational." Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4541006/.
-
Edward Salsberg, Robert Martiniano. "Health Care Jobs Projected To Continue To Grow Far Faster Than Jobs In The General Economy." Available at: https://www.healthaffairs.org/do/10.1377/hblog20180502.984593/full/.
-
Andrea Gruneir and Vincent Mor. "Nursing Home Safety: Current Issues and Barriers to Improvement." Available at: https://www.annualreviews.org/doi/full/10.1146/annurev.publhealth.29.020907.090912.
-
David C. Grabowski. "Testimony Before the United States Senate Committee on Finance. Not Forgotten: Protecting Americans from Abuse and Neglect in Nursing Homes" Available at: https://www.finance.senate.gov/imo/media/doc/Grabowski%20Senate%20Finance%20testimony%20FINAL.pdf.
-
Edith G. Walsh and Joshua M. Wiener. "Hospitalizations of Nursing Home Residents: Background and Options." https://aspe.hhs.gov/basic-report/hospitalizations-nursing-home-residents-background-and-options.
-
Liz Liberman. "Medicaid Reimbursement Rates Draw Attention." Available at: https://www.nic.org/blog/medicaid-reimbursement-rates-draw-attention/.
-
Jordan Rau. "Why Glaring Quality Gaps Among Nursing Homes Are Likely To Grow If Medicaid Is Cut." Available at: https://khn.org/news/why-glaring-quality-gaps-among-nursing-homes-are-likely-to-grow-if-medicaid-is-cut/.
-
Alia Paavola. "CARES Act provider relief fund distribution: A timeline." Available at: https://www.beckershospitalreview.com/finance/cares-act-provider-relief-fund-distribution-a-timeline.html.
-
Centers for Medicare & Medicaid Services. "Trump Administration Announces New Resources to Protect Nursing Home Residents Against COVID-19." Available at: https://www.cms.gov/newsroom/press-releases/trump-administration-announces-new-resources-protect-nursing-home-residents-against-covid-19.
-
Small Business Administration. "Paycheck Protection Program." Available at: https://www.sba.gov/funding-programs/loans/coronavirus-relief-options/paycheck-protection-program.
-
Kaiser Family Foundation. "State Data and Policy Actions to Address Coronavirus." Available at: https://www.kff.org/health-costs/issue-brief/state-data-and-policy-actions-to-address-coronavirus/.
-
According to guidance from the Small Business Administration, at least 75 percent of the PPP loan proceeds shall be used for payroll costs which include compensation to employees with an annual salary less than $100,000 or medical, sick, or personal leave. Information about loan provisions are described in the interim final rule: Available at: Business Loan Program Temporary Changes; Paycheck Protection Program (Small Business Administration), https://www.federalregister.gov/documents/2020/04/15/2020-07672/business-loan-program-temporary-changes-paycheck-protection-program.
-
Centers for Medicare & Medicaid Services. "COVID-19 Nursing Home Data." Available at: https://data.cms.gov/stories/s/COVID-19-Nursing-Home-Data/bkwz-xpvg.
-
World Health Organization. "Coronavirus Disease Situation Report--160." Available at: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200628-covid-19-sitrep-160.pdf?sfvrsn=2fe1c658_2.
-
Centers for Disease Control and Prevention. "Coronavirus Disease 2019: Older Adults." Available at: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/older-adults.html.
-
Janice K. Louie et al. "Lessons from Mass-Testing for COVID-19 in Long Term Care Facilities for the Elderly in San Francisco." Available at: https://pubmed.ncbi.nlm.nih.gov/32687150/.
-
David C. Grabowski et al. "COVID-19 in Nursing Homes: Pragmatic Research Responses to the Crisis." Available at: https://impactcollaboratory.org/special-grand-rounds-covid-19-in-nursing-homes-pragmatic-research-responses-to-the-crisis/.
-
Jose F. Figueroa et al. "Association of Nursing Home Ratings on Health Inspections, Quality of Care, and Nurse Staffing With COVID-19 Cases." Available at: https://jamanetwork.com/journals/jama/fullarticle/2769437.
-
James M. Berklan. "Missing staff, makeshift PPE rampant as COVID-19 hits 34% of nursing homes, new McKnight's survey shows." Available at: https://www.mcknights.com/news/missing-staff-makeshift-ppe-rampant-as-covid-19-hits-34-of-nursing-homes-new-mcknights-survey-shows/.
-
Centers for Disease Control and Prevention. "COVID-19 in a Long-Term Care Facility--King County, Washington, February 27-March 9, 2020." Available at: https://skillednursingnews.com/wp-content/uploads/sites/4/2020/03/mm6912e1-H.pdf.
-
Michael Cantor et al. "Reducing COVID-19 Deaths In Nursing Homes: Call To Action." Available at: https://www.healthaffairs.org/do/10.1377/hblog20200522.474405/full/.
-
Centers for Medicare & Medicaid Services. "Trump Administration Strengthens COVID-19 Surveillance with New Reporting and Testing Requirements for Nursing Homes, Other Providers." Available at: https://www.cms.gov/newsroom/press-releases/trump-administration-strengthens-covid-19-surveillance-new-reporting-and-testing-requirements.
-
Centers for Medicare & Medicaid Services. "Toolkit on State Actions to Mitigate COVID-19 Prevalence in Nursing Homes." Available at: https://www.cms.gov/files/document/covid-toolkit-states-mitigate-covid-19-nursing-homes.pdf.
-
Louisiana Department of Health. "Louisiana Health Work Connect." Available at: https://healthworkconnect.la.gov.
-
MassHealth. "MassHealth Investment to Support Signing Bonuses for Nursing Facility Staff." Available at: https://www.mass.gov/doc/masshealth-investment-to-support-signing-bonuses-for-nursing-facility-staff/download.
-
Centers for Medicare & Medicaid Services. "Long Term Care Facilities (Skilled Nursing Facilities and/or Nursing Facilities): CMS Flexibilities to Fight COVID-19." Available at: https://www.cms.gov/files/document/covid-long-term-care-facilities.pdf.
-
AHCA NCAL ED. "Temporary Nurse Aide." Available at: https://educate.ahcancal.org/training.
-
Office of the Governor Doug Ducey (AZ). "Governor Ducey Issues Executive Order To Expand Licensing Opportunities." Available at: https://azgovernor.gov/governor/news/2020/03/governor-ducey-issues-executive-order-expand-licensing-opportunities.
-
National Council of State Boards of Nursing. "State Response to COVID-19." Available at: https://www.ncsbn.org/State_COVID-19_Response.pdf.
-
New Jersey Hospital Association. "Waiver Tracker." Available at: http://www.njha.com/Coronavirus/Waiver-Tracker.
-
Howard Altman. "Latest Guard update: Over 14,830 troops mobilized for COVID-19 response, more states on Title 32 status." Available at: https://www.militarytimes.com/news/coronavirus/2020/03/30/latest-guard-update-over-14830-troops-mobilized-for-covid-19-response-more-states-on-title-32-status/.
-
Sgt. Amber Mullen. "Ohio National Guard a lifeline for assisted living facility." Available at: https://www.nationalguard.mil/News/Article/2242629/ohio-national-guard-a-lifeline-for-assisted-living-facility/.
-
Office of Governor Gretchen Whitmer. "Governor Whitmer Signs Bill for Supplemental Funding to Support COVID-19 Response." Available at: https://www.michigan.gov/whitmer/0,9309,7-387-90499_90640-533390--,00.html.
-
New Hampshire Employment Security. "Long Term Care Stabilization Program." Available at: https://www.nhes.nh.gov/services/employers/longtermcare.htm.
-
Brendan Flinn. "States Leverage Medicaid to Provide Nursing Homes a Lifeline through COVID-19." Available at: https://www.leadingage.org/regulation/states-leverage-medicaid-provide-nursing-homes-lifeline-through-covid-19.
-
Lana Peck. "Executive Survey Insights: Wave 3, Week Ending April 19, 2020." Available at: https://blog.nic.org/executive-survey-results-for-week-ending-april-19-2020.
-
Mass.gov. "EEC Coronavirus Update for Children & Families." Available at: https://eeclead.force.com/apex/EEC_ChildCareEmergencyParents.
-
State of Minnesota Executive Department. "Emergency Executive Order 20-02." Available at: https://mn.gov/governor/assets/EO%2020-02%20Final_tcm1055-423084%20%281%29_tcm1055-423779.pdf.
-
Office of the Governor State of Oregon. "Executive Order Number 20-08." Available at: https://drive.google.com/file/d/1IR5fFOUxLJRDASrvkV-HyZWoi5IHlmXE/view.
-
Washington Office of Superintendent of Public Instruction. "Guidance for Long-term School Closures as of March 23, 2020." Available at: https://www.k12.wa.us/sites/default/files/public/bulletinsmemos/bulletins2020/5_Guidance%20for%20Long-term%20School%20Closures%20as%20of%20March%2023%282%29.pdf.
-
Connecticut Office of Early Childhood. "CTCARES for Frontline Workers Child Care Program." Available at: https://www.ctoec.org/ctcares-for-frontline-workers/.
-
Colorado Children's Campaign. "Colorado Emergency Childcare Collaborative Update." Available at: https://www.coloradokids.org/colorado-emergency-childcare-collaborative-update/.
-
NYC Department of Education. "Regional Enrichment Centers." Available at: https://www.schools.nyc.gov/enrollment/enrollment-help/regional-enrichment-centers.
-
Tim Regan. "Senior Living Providers Adjust Operations, Raise Pay to Meet COVID-19 Staffing Challenges." Available at: https://seniorhousingnews.com/2020/03/30/senior-living-providers-adjust-operations-raise-pay-to-meet-covid-19-staffing-challenges/.
-
Help Now NYC. "COVID-19 Hotel Program." Available at: https://www1.nyc.gov/site/helpnownyc/get-help/covid-19-hotel-program.page.
-
California State Government. "Hotel rooms for California healthcare workers." Available at: https://covid19.ca.gov/hotel-rooms-for-california-healthcare-workers/.
-
Rhode Island Department of Public Health. "Free Housing for Frontline Workers During COVID-19." Available at: https://www.providenceri.gov/wp-content/uploads/2020/05/COVID19_Worker-Housing.pdf.
-
Airbnb. "Providing Accommodations for Frontline Responders in New Orleans." Available at: https://news.airbnb.com/housing-frontline-responders-in-new-orleans/.
-
Metropolitan Council. "Metropolitan Council to Offer Door-To-Door Transport for Essential Health Workers Across the Region." https://metrocouncil.org/News-Events/Transportation/Newsletters/Transportation-for-essential-health-workers.aspx.
-
Wisconsin Department of Health Services. "COVID-19: Long-Term Care Facilities and Services." Available at: https://www.dhs.wisconsin.gov/covid-19/ltc.htm.
-
James M. Berklan. "COVID-19 survey: Nursing homes' top strategies for 'keeping spirits up'." Available at: https://www.mcknights.com/news/covid-19-survey-delivers-nursing-homes-top-strategies-for-keeping-spirits-up/.
-
Centers for Disease Control and Prevention. "Healthcare Personnel and First Responders: How to Cope with Stress and Build Resilience During the COVID-19 Pandemic." Available at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/mental-health-healthcare.html.
-
ASPR TRACIE. "Mitigate Absenteeism by Protecting Healthcare Workers' Psychological Health and Well-being during the COVID-19 Pandemic." Available at: https://files.asprtracie.hhs.gov/documents/strategy-to-mitigate-healthcare-workforce-absenteeism-final.pdf.
-
NETEC. "NETEC COVID-19 Webinar Series (4/6/20): Resilience And Care Of The Caregiver Webinar." Available at: https://repository.netecweb.org/items/show/907.
-
Minnesota Department of Health. "COVID-19 Toolkit: Information for Long-Term Care Facilities." Available at: https://www.health.state.mn.us/diseases/coronavirus/hcp/ltctoolkit.pdf.
-
Maryland Department of Health. "Maryland COVID-19 Crisis Support Program: Free Mental Health for Frontline Workers." Available at: http://www.miemss.org/home/Portals/0/Docs/Executive-Orders/Letter-Maryland-COVID-19-Crisis-Support-Program-20200531.pdf?ver=2020-05-31-172815-783.
-
Ohio Department of Mental Health and Addiction Services. "COVID CareLine." Available at: https://mha.ohio.gov/Health-Professionals/About-Mental-Health-and-Addiction-Treatment/Emergency-Preparedness/Coronavirus/COVID-CareLine.
-
CMS Nursing Home Reopening Recommendations available at: https://www.cms.gov/files/document/qso-20-30-nh.pdf-0. Accessed on July 8, 2020.
-
For symptomatic staff with suspected or confirmed COVID-19, the CDC recommended the following criteria for returning to work at the time this report was written. Symptom-based strategy: exclude staff from work until at least 3 days have passed since recovery from symptoms (both fever and respiratory), and at least 10 days have passed since symptoms first appeared. Test-based strategy: exclude staff from work until fever resolves, improvement in respiratory symptoms, and negative results from two tests (COVID-19 molecular assay for detection of SARS-CoV-2 RNA) collected >24 hours apart. For asymptomatic staff with confirmed COVID-19, the CDC recommended the following criteria for returning to work at the time this report was written. Time-based strategy: 10 days have passed since the first positive COVID-19 test, and no symptoms have developed. Test-based strategy: the staff member is excluded from work until negative results from two tests (COVID-19 molecular assay for detection of SARS-CoV-2 RNA) are collected >24 hours apart.
-
Centers for Disease Control and Prevention. "Duration of Isolation and Precautions for Adults with COVID-19." Available at: https://www.cdc.gov/coronavirus/2019-ncov/community/strategy-discontinue-isolation.html.
-
On July 14, 2020, HHS announced a plan to distribute point-of-care diagnostic test instruments and tests to nursing homes in COVID-19 hotspot geographic areas. On July 22, 2020, CMS announced a plan to begin requiring all nursing homes in states with a 5 percent positivity rate or greater test all nursing home staff each week. These policies were announced after the completion of the stakeholder interviews; therefore, no feedback on these policies was received.
-
Centers for Disease Control and Prevention. "Strategies to Optimize the Supply of PPE and Equipment." Available at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/ppe-strategy/index.html . Accessed June 29, 2020.
-
James M. Berklan. "Analysis: PPE costs increase over 1,000% during COVID-19 crisis." Available at: https://www.mcknights.com/news/analysis-ppe-costs-increase-over-1000-during-covid-19-crisis.
-
Federal Register. "Amendment to Declaration Under the Public Readiness and Emergency Preparedness Act for Medical Countermeasures Against COVID-19." Available at: https://www.fema.gov/news-release/2020/05/02/coronavirus-pandemic-response-ppe-packages-nursing-homes.
-
Andrew Jacobs. "FEMA Sends Faulty Protective Gear to Nursing Homes Battling Virus." Available at: https://www.nytimes.com/2020/07/24/health/coronavirus-nursing-homes-PPE.html.
-
Mass.gov. "Personal Protective Equipment (PPE) During COVID-19." Available at: https://www.mass.gov/info-details/personal-protective-equipment-ppe-during-covid-19#requesting-ppe-.
-
Centers for Disease Control and Prevention. "Preparing for COVID-19 in Nursing Homes." Available at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/long-term-care.html.
-
Texas Health and Human Services. "COVID-19 Response for Nursing Facilities." Available at: https://hhs.texas.gov/sites/default/files/documents/doing-business-with-hhs/provider-portal/long-term-care/nf/covid-response-nursing-facilities.pdf.
-
Connecticut Department of Social Services. "Department of Social Services Coronavirus Relief Fund (CRF) Nursing Home Grants." Available at: https://portal.ct.gov/-/media/Departments-and-Agencies/DSS/Medicaid-Nursing-Home-Reimbursement/FAQ-Document-CRF-Funding-Questions-Update-July-1-2020-REVISED.pdf.
-
SEIU. "SEIU COVID-19 Nursing Home Survey Report, 6/20." Available at: https://seiufacultyforward.wufoo.com/reports/seiu-covid19-nursing-home-survey-report-0620.
-
Avamere's new policy pays employees for shifts missed due to a confirmed case of COVID-19, creates a PTO sharing/donation pool for employees, provides full pay during a staff member's 2-week quarantine due to at-work exposure, and allows employees to carry a negative PTO balance.
-
Centers for Medicare & Medicaid Services. "Guidance for Infection Control and Prevention of Coronavirus Disease 2019 (COVID-19) in Nursing Homes." Available at: https://www.cms.gov/files/document/qso-20-14-nh-revised.pdf.
-
LA County Public Health. "Guidelines for Preventing and Managing COVID-19 in Skilled Nursing Facilities." Available at: http://ph.lacounty.gov/acd/ncorona2019/snf.htm#InfectionPrevention.
-
Centers for Disease Control and Prevention. "Return to Work for Healthcare Personnel with Confirmed or Suspected COVID-19 (April 15, 2020 Archive)." Available at: https://web.archive.org/web/20200417211515/https:/www.cdc.gov/coronavirus/2019-ncov/hcp/return-to-work.html?CDC_AA_refVal=https%25253A%25252F%25252Fwww.cdc.gov%25252Fcoronavirus%25252F2019-ncov%25252Fhealthcare-facilities%25252Fhcp-return-work.html.
-
New Jersey Department of Health. "Protocols for Essential Personnel to Return to Work Following COVID-19 Exposures or Infection." Available at: https://www.nj.gov/health/cd/documents/topics/NCOV/COVID_essential_personnel_return_to_work.pdf.
-
Centers for Medicare & Medicaid Services. "CMS Directs Additional Resources to Nursing Homes in COVID-19 Hotspot Areas." Available at: https://www.cms.gov/newsroom/press-releases/cms-directs-additional-resources-nursing-homes-covid-19-hotspot-areas.
-
U.S. Department of Health and Human Services. "Trump Administration Announces Initiative for More and Faster COVID-19 Testing in Nursing Homes." Available at: https://www.hhs.gov/about/news/2020/07/14/trump-administration-announces-initiative-more-faster-covid-19-testing-nursing-homes.html.
-
Centers for Medicare & Medicaid Services. "Frequently Asked Questions: COVID-19 Testing at Skilled Nursing Facilities/ Nursing Homes." Available at: https://www.cms.gov/files/document/covid-faqs-snf-testing.pdf.
-
Centers for Medicare & Medicaid Services. "Interim Final Rule (IFC), CMS-3401-IFC, Additional Policy and Regulatory Revisions in Response to the COVID-19 Public Health Emergency related to Long-Term Care (LTC) Facility Testing Requirements and Revised COVID19 Focused Survey Tool." Available at: https://www.cms.gov/files/document/qso-20-38-nh.pdf.
-
U.S. Department of Health and Human Services. "HHS Announces Allocations of CARES Act Provider Relief Fund for Nursing Homes." Available at: https://www.hhs.gov/about/news/2020/08/07/hhs-announces-allocations-of-cares-act-provider-relief-fund-for-nursing-homes.html.
-
Centers for Medicare & Medicaid Services. "Trump Administration Launches National Training Program to Strengthen Nursing Home Infection Control Practices." Available at: https://www.cms.gov/newsroom/press-releases/trump-administration-launches-national-training-program-strengthen-nursing-home-infection-control.
-
Coronavirus Commission for Safety and Quality in Nursing Homes https://www.cms.gov/files/document/covid-final-nh-commission-report.pdf.
This report was prepared under contract #HHSP233201500035I between HHS's ASPE/BHDAP and Mathematica. For additional information about this subject, you can visit the BHDAP home page at https://aspe.hhs.gov/bhdap or contact the ASPE Project Officers, at HHS/ASPE/BHDAP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C., 20201; Marie.Squillace@hhs.gov, Helen.Lamont@hhs.gov, Iara.Oliveira@hhs.gov, Judith.Dey@hhs.gov.