
U.S. Department of Health and Human Services
Using MSIS Data to Analyze Mental Health Service Use and Expenditures for Medicaid Beneficiaries with Mental Illness in New Jersey in 1999
Henry Ireys and Ann Cherlow
Mathematica Policy Research, Inc.
January 2004
This report was prepared under contract #HHS-100-97-0013 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and Mathematica Policy Research, Inc. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/daltcp/home.htm or contact the ASPE Project Officer, John Drabek, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. His e-mail address is: jdrabek@osaspe.dhhs.gov.
ACKNOWLEDGMENTS
Several colleagues at the Office of the Assistant Secretary for Planning and Evaluation (ASPE) and at Mathematica Policy Research (MPR) assisted in the development of this report. At ASPE, Cille Kennedy played a major role in the conceptualization of the service categories that we used for our analyses and supported the work with consistent and much-appreciated enthusiasm. John Drabek and Hunter McKay helped in the early stages of the project and provided valuable comments on our approach to the data analysis. At MPR, Myles Maxfield read several drafts of the report and suggested changes that substantially improved the final version. Heather Hesketh helped organize the data specifications and gathered the information we needed to plan and refine our analyses. Deo Bencio conducted the analyses and remained available to help understand the output and its implications. Sharon Clark prepared the manuscript with her usual competence and grace. We thank all of our colleagues for their assistance.
TABLE OF CONTENTS
A. Purpose of Study
B. Overview of Report
II. METHODS
A. Selecting Data from New Jersey
B. Identifying Beneficiaries with Mental Illness
C. Categorizing Mental Health Services
D. Procedures for Calculating Expenditures
III. BENEFICIARIES WITH MENTAL ILLNESS: CHARACTERISTICS AND OVERALL SERVICE EXPENDITURES
A. Number of Beneficiaries with Mental Illness and Overall Costs of Care
B. Characteristics of Beneficiaries with Mental Illness
A. Percent of Beneficiaries Using Selected Types of Services
B. Inpatient Services for Two Age Groups by Gender
C. Service Expenditures
V. CHARACTERISTICS OF HIGH-COST BENEFICIARIES
VI. LESSONS LEARNED, POLICY IMPLICATIONS, AND POTENTIAL NEXT STEPS
A. Patterns of Service Use and Expenditures
B. Next Steps
C. Utility of MSIS Data
APPENDICES
Appendix A: Detailed Data Tables (separate PDF file)
Appendix B: Definitions of Terms in Data Tables (separate PDF file)
Appendix C: Procedures for Identifying Individuals with Mental Illness; Definition of Inpatient Stays; Procedures for Distinguishing Clinical vs. Supportive Services; Pharmaceutical Groups Used to Define Psychiatric Medications (separate PDF file)
Appendix D: Specific Drugs Identified as Psychiatric Medications (separate PDF file)
Appendix E: File Layout (separate PDF file)
LIST OF FIGURES/TABLES
TABLE II.1: Proportions of Sample Found by Identification Methods
TABLE III.1: Medicaid Beneficiaries with Mental Illness in New Jersey: Population Size and Annual Medicaid Expenditures for All Services and For Mental Health Services, 1999
TABLE III.2: Medicaid Beneficiaries with Mental Illness as Percent of All Beneficiaries and Annual Expenditures for Services as Percent of All Expenditures, New Jersey, 1999
TABLE III.3: Characteristics of All Medicaid Beneficiaries and Medicaid Beneficiaries with Mental Illness, New Jersey, 1999
TABLE IV.1: Percent of Medicaid Beneficiaries with Mental Illness Using Selected Mental Health Services By Demographic Characteristics and Program Status, New Jersey, 1999
TABLE IV.2: Medicaid Beneficiaries in Two Age Groups Who Received Inpatient Services, New Jersey, 1999
TABLE IV.3: Female and Male Medicaid Beneficiaries in Two Age Groups Who Received Inpatient Services, New Jersey, 1999
TABLE IV.4: Expenditures for Medicaid Services for All Beneficiaries with Mental Illness and Beneficiaries with Mental Illness Who Used Selected Mental Health Services, by Demographic Characteristics and Eligibility Status, New Jersey, 1999
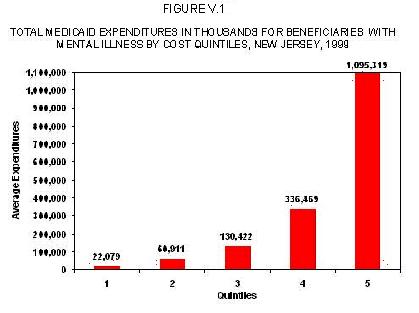
FIGURE V.1: Total Medicaid Expenditures in Thousands for Beneficiaries with Mental Illness by Cost Quintiles, New Jersey, 1999
TABLE V.1: Characteristics of Beneficiaries with Mental Illness in the Highest Cost Quintile, New Jersey, 1999
TABLE V.2: Expenditures for Medicaid Services for Beneficiaries with Mental Illness in the Highest Cost Quintile by Demographic Characteristics and Eligibility Status, New Jersey, 1999
I. STUDY PURPOSE
A. Purpose of Study
Many Medicaid beneficiaries with chronic mental illness have serious difficulty finding services that will assist them to live in communities and participate in the full range of social activities. Recent national policy reports (GAO 2003; New Freedom Commission on Mental Health 2003) and judicial decisions (U.S. Supreme Court 1999) underscore the critical need to improve the mental health service system, and policymakers, program administrators, and advocacy groups are working to develop effective community-based alternatives to placement in psychiatric hospitals or residential facilities (see, for example, Bazelon 2001). A major obstacle impeding these efforts is the lack of adequate information on what medical and mental health services these individuals use and how much Medicaid spends for their care. Without a better foundation of knowledge, state Medicaid agencies are reluctant to expand services or develop new initiatives for individuals with chronic mental illness, particularly when state governments are facing financial shortfalls.
The Office of the Assistant Secretary for Planning and Evaluation (ASPE) in the Department of Health and Human Services (HHS) plays an important role in establishing national policies for Medicaid and assisting state Medicaid agencies to address emerging policy issues effectively. As part of its mission, ASPE identifies opportunities to develop new sources of information and conduct studies that will be useful to state Medicaid staff and other key stakeholders. The study described in this report was designed to determine whether the Medicaid Statistical Information System (MSIS) files could be used to generate policy-relevant information on the use and costs of Medicaid services for beneficiaries with mental illness.1
MSIS files provide substantial individual-level information on the services that beneficiaries use, the costs of these services, and demographic and program eligibility characteristics of beneficiaries. The study described in this report is one of the first to use MSIS files to examine services for Medicaid beneficiaries with mental illness and it demonstrates how data in these files can be used to address policy issues affecting these individuals. Specifically, in this study we aim to (1) describe Medicaid services used by beneficiaries with mental illness in one state and (2) assess the feasibility of using MSIS data for analyses of mental health services. If MSIS files are found to be useful for this purpose, OASPE or other agencies could consider further analyses of MSIS data to investigate patterns in the use and cost of mental health services.2
B. Overview of Report
In the following chapter (Chapter II), we describe the methods we used for this study. Chapter III includes an overview of our findings on service use and costs for beneficiaries with mental illness compared with services for other Medicaid beneficiaries. The fourth chapter provides information on characteristics of the population with mental illness and the services they use. In Chapter V we examine characteristics of the high-cost subgroup and in the final chapter of the report (Chapter VI), we summarize our findings and suggest next steps. Specifically, we address the lessons learned regarding (1) patterns of service use and expenditures for beneficiaries with mental illness and (2) the utility of MSIS data.
Information for the analyses presented in Chapters III-V was drawn from the detailed data tables in Appendix A, which were produced in accordance with specifications developed in consultation with staff at the OASPE. These tables contain more information than could be presented in the text of this report. We selected key findings to include in the text that we believe would be of broad interest and would illustrate the feasibility of using MSIS data to provide policy relevant information. In addition to Appendix A, we include the following appendices:
Appendix B: Definitions of Terms in the Tables
Appendix C: Procedures for Identifying Individuals with Mental Illness, Definition of Inpatient Stays, Procedures for Distinguishing Clinical vs Supportive Services, and Pharmaceutical Groups Used to Define Psychiatric Medications
Appendix D: Specific Drugs Identified as Psychiatric Medications
Appendix E: File Layout
II. METHODS
Our first step for this study was to select an appropriate state in which to examine patterns of mental health service use and associated expenditures.3 After this decision was made, we then (1) identified beneficiaries with mental illness, (2) sorted mental health services into selected categories, and (3) calculated expenditures for the services used. In this chapter, we discuss our approach to each of these steps.
A. Selecting Data from New Jersey
After examining MSIS data from numerous states, we selected files from New Jersey for three reasons. First, New Jersey data were being analyzed for a concurrent study and therefore we could conduct our analyses efficiently. Second, New Jersey had low rates of beneficiary enrollment in Medicaid behavioral managed care in 1999, and therefore claims data on service use were available for the large majority of beneficiaries. (As states began enrolling beneficiaries into managed care programs, claims data became increasingly incomplete because managed care organizations usually were not required to submit specific claims or encounter data to the state Medicaid agency.) Finally, New Jerseys a large population of Medicaid beneficiaries allowed for statistically robust analyses. We used MSIS data from calendar year 1999 because these were the most complete data available at the start of the study (September 2001).
B. Identifying Beneficiaries with Mental Illness
We elected to focus on beneficiaries with mental illness (including those who also have any other co-occurring mental disorder) because this study was designed to assess the feasibility of using MSIS data to examine services for a targeted group of beneficiaries rather than to conduct a comprehensive assessment of cost and service use for all individuals with any mental disorder. Therefore, we distinguished beneficiaries with mental illness from beneficiaries who have other mental disorders, including substance abuse (SA) problems, mental retardation or developmental disabilities (MR/DD), or organic brain disorders (OBD). Of course, many individuals with mental illness also have co-occurring SA, MR/DD, and/or OBD, and we included these individuals in our analyses. If MSIS data are found to be useful for describing service use and costs for beneficiaries with mental illness, future studies can analyze cost and use data for groups of beneficiaries with other mental disorders as the targeted group of individuals.
Beneficiaries with mental illness are defined as individuals who had (1) a psychiatric diagnosis (using specific ICD-9-CM codes) on any claim in calendar year 1999 or (2) any claim for a selected mental health service. The ICD-9-CM codes and the mental health services used to select individuals with mental illness are in Appendix C.4
Most individuals whom we identified as having a mental illness were identified by either diagnosis alone, or diagnosis in conjunction with service codes (Table II.1). Only 5 percent of individuals identified were found based exclusively on services.
| TABLE II.1. Proportions of Sample Found by Identification Methods | |
| Identified by: | Percent of Identified Individuals |
| Diagnosis Only | 71% |
| Service Only | 5% |
| Diagnosis and Service | 23% |
Some services provided to individuals who have mental illness are not strictly mental health services although they often are provided to this population for therapeutic purposes. For example, occupational therapy is not usually considered a mental health service but many individuals with serious mental illness who are in day treatment or residential settings engage in occupational therapy as part of their treatment. Although we did not use certain types of services to identify beneficiaries with a mental illness, these services were designated as mental health services for the purposes of calculating expenditures. Consequently, we expected to find (and did find) that beneficiaries who did not have mental illness nonetheless had expenditures for mental health services. For example, some beneficiaries who do not have a mental illness will be given occupational therapy as treatment for other conditions. In future work, we will need to develop methods for distinguishing when a particular service such as occupational therapy should be considered as a mental health service, and when it should not be so considered.
Our approach may miss counting individuals who in fact have mental illness but are not diagnosed as such because the physicians they visit may be treating medical problems and because they do not use mental health services. Furthermore, individuals with mental illness in certain groups of beneficiaries are disproportionately likely to be missed. For example, in the group of aged beneficiaries who also have Medicare, individuals with mental illness may be missed because Medicare covers most of their services and, as a result, their residual Medicaid claims do not include qualifying codes.
Finally, as part of our feasibility assessment, we also considered using psychiatric medication codes to identify individuals as having a mental illness. However, after conducting a preliminary examination of the potential codes that could be used for this purpose, we elected not to use this identification strategy because many psychiatric medications also are used to treat certain types of physical symptoms (e.g., seizures) in individuals who do not have mental illness. We concluded that the use of psychiatric medication codes would yield high numbers of false positives, and therefore would be an unreliable indicator of the target population.
C. Categorizing Mental Health Services
We classified mental health services into three primary categories: psychiatric inpatient services, community mental health services, and psychiatric prescription drugs. Within the category of inpatient services, we made further distinctions between services provided in long-term psychiatric institutions, acute psychiatric inpatient facilities (for example, psychiatric units of a general hospital), and other psychiatric residential facilities (for example, certain types of group homes).
Community mental health services were classified into two categories suggested by OASPE staff: individual clinical services, such as evaluation, diagnostic, and treatment services provided to individual beneficiaries in community settings or private offices; and all other therapeutic services, including family or group counseling and certain types of psychiatric case management services. Additional details regarding service classifications are in Appendix C.
D. Procedures for Calculating Expenditures
We used the amounts Medicaid paid on claims, as taken from MSIS, in calculating Medicaid expenditures. These expenditures include both payments for fee-for-service claims and payments for capitation premiums (e.g., to HMOs).
In all cases, we created fully adjusted payments, meaning that we combined original claims with subsequent additions or subtractions and resubmissions so that we were left with the final amount actually paid for each service. The expenditure data from MSIS do not allow association of some Medicaid expenses with individual beneficiaries; these missing expenditures include administrative expenses of the Medicaid program, disproportionate share hospital payments, and other provider-level payments.
We calculated two types of Medicaid expenditures for services that beneficiaries received in 1999: expenditures for all services and expenditures for mental health services. The list of mental health services that we included in these calculations is in Appendix C. For most analyses, we calculated mean expenditures for each beneficiary. For selected analyses, we calculated expenditures based on person-years of enrollment, thereby accounting for the transient nature of Medicaid enrollment in some eligibility groups.
III. BENEFICIARIES WITH MENTAL ILLNESS: CHARACTERISTICS AND OVERALL SERVICE EXPENDITURES
In order to enhance existing mental health policies or plan new initiatives for individuals in Medicaid, policymakers and program administrators need reliable information on the number and characteristics of beneficiaries with mental illness. We used the 1999 MSIS eligibility and claims files for New Jersey to identify (1) beneficiaries with mental illness, (2) their demographic characteristics and program status, and (3) expenditures for the services they used. Key findings include the following:
- In 1999, 11.5 percent of all Medicaid beneficiaries in New Jersey had a mental illness (including those with mental illness only and mental illness with SA, MR/DD, or OBD as a co-occurring disorder).
- Beneficiaries with mental illness (including those with mental illness and co-occurring mental disorders) accounted for 30.1 percent of Medicaid expenditures.
- Beneficiaries with mental illness had annual Medicaid expenditures for all services that were 2.5 times greater than beneficiaries in general.
- Compared with beneficiaries in general, the group of beneficiaries with mental illness includes proportionally more males, fewer children, more whites, fewer Hispanics, and more individuals who are receiving SSI disability payments and who are dually enrolled in Medicaid and Medicare.
Detailed findings are presented in the two parts of this chapter: (1) Number of beneficiaries with mental illness and co-occurring mental disorders and the overall expenditures for the services they used and (2) characteristics of beneficiaries with mental illness compared with beneficiaries in general.
A. Number of Beneficiaries with Mental Illness and Overall Costs of Care
A total of 868,106 individuals were Medicaid beneficiaries in New Jersey in 1999. Of these, were 99,976 (11.5 percent) had mental illness, including those with co-occurring mental disorders (Table III.1 and Table III.2). This group accounted for 30.1 percent of the costs of all Medicaid expenditures. Other key findings shown in the tables include the following:
- A total of $1.1 billion dollars were spent on mental health services for beneficiaries with mental illness in New Jersey in 1999.
- Mean costs of care for Medicaid services overall and for mental health services were higher for beneficiaries who had mental illness than for the beneficiaries in general. Beneficiaries with mental illness had annual costs of care for all services that were 2.5 times more than beneficiaries in general ($16,540 vs $6,504).
- Slightly more than 8 percent of all Medicaid beneficiaries had only a mental illness and no other co-occurring mental disorder, and this subgroup accounted for about 15.6 percent of the costs for all Medicaid services and 21.6 percent of the costs for Medicaid mental health services.
- Different co-occurring mental disorders have different implications for costs of care. For example, the co-occurring disorder that has the greatest impact on costs of care is MR/DD. Only 1.5 percent of all Medicaid beneficiaries have mental illness and MR/DD, but these individuals account for 17.5 percent of the costs of mental health services.
| TABLE III.1. Medicaid Beneficiaries with Mental Illness in New Jersey: Population Size and Annual Medicaid Expenditures for All Services and For Mental Health Services, 1999 | |||||
| Number | Annual Expenditures | ||||
| All Services | Mental Health Services Only | ||||
| Total(in $1,000s) | Mean | Total(in $1,000s) | Mean | ||
| All Medicaid Beneficiaries | 868,106 | $5,358,079 | $6,504 | $2,270,448 | $2,721 |
| Beneficiaries with: | |||||
| Mental Illness and Any Co-occurring SA, MR/DD, or OBD | 99,976 | $1,645,200 | $16,540 | $1,120,905 | $11,202 |
| - Mental Illness Only | 70,659 | $833,569 | $11,694 | $490,968 | $6,747 |
| - Mental Illness and SA | 8,109 | $155,197 | $18,860 | $105,175 | $12,550 |
| - Mental Illness and MR/DD | 12,778 | $449,917 | $35,512 | $394,121 | $31,107 |
| - Mental Illness and OBD | 10,162 | $273,293 | $26,618 | $181,026 | $17,459 |
| Any Mental, SA, MR/DD, or OBD | 126,989 | $2,585,498 | $20,459 | $1,812,785 | $14,259 |
| SA only, MR/DD only, and OBD only | 27,013 | $940,298 | $35,860 | $691,880 | $26,272 |
| SOURCE: New Jersey MSIS Files, 1999. NOTE: SA is Substance Abuse; MR/DD is Mental Retardation/Developmental Disabilities; OBD is Organic Brain Disorder. Expenditures are adjusted for person-years. | |||||
As Table III.1 shows, individuals with any mental disorder--including mental illness, substance abuse, mental retardation/developmental disorders, or organic disorders--constitute 14.6 percent of the population and account for 79.8 percent of the expenditures for mental health services. The remaining 20 percent of expenditures for mental health services result from either (1) individuals who are not identified as having a mental disorder but who in fact do and are using mental health services or psychiatric medications that were not used for identification purposes (see Chapter II) or (2) individuals who do not have a mental disorder but who are using psychiatric medications for selected conditions (such as epilepsy).
Additional information on annual and mean costs of care for major groups of beneficiaries can be found in Appendix A.
B. Characteristics of Beneficiaries with Mental Illness
We found important differences in demographic characteristics and eligibility status of beneficiaries with mental illness compared with beneficiaries in general (Table III.2). Demographic differences include the following:
- Males comprise a somewhat greater percentage of the group of beneficiaries with mental illness compared with beneficiaries in general (44.5 vs. 39.3 percent).
- Beneficiaries with mental illness tend to be older than beneficiaries in general; for example, slightly more than half of all beneficiaries (51.9 percent) are under 18 years of age but less than a third (31.7 percent) of beneficiaries with mental illness are in this age group.
- The racial composition of the group of beneficiaries with mental illness is somewhat different compared with beneficiaries overall. For example, there are proportionally more Whites and fewer Hispanics in the group of beneficiaries with mental illness.
We also found major differences in eligibility status between beneficiaries in general and beneficiaries with mental illness:
- Overall, 11.3 percent of all Medicaid beneficiaries in New Jersey in 1999 were receiving SSI payments; in contrast, 36.0 percent of beneficiaries with mental illness were receiving these payments.
- Children comprised 54.2 percent of all Medicaid beneficiaries in New Jersey in 1999 (13.5 percent were AFDC children and 40.7 percent were other children) but only 25.7 percent of beneficiaries with mental illness were children.
- 18.6 percent of all beneficiaries and 23.7 of beneficiaries with mental illness were dually enrolled in Medicare.
| TABLE III.2. Medicaid Beneficiaries with Mental Illness as Percent of All Beneficiaries and Annual Expenditures for Services As Percent of All Expenditures, New Jersey, 1999 | |||
| Percent of Beneficiaries | Percent of Expenditures | ||
| All Services | Mental Health Services | ||
| All Medicaid Beneficiaries | 100.0 | 100.0 | 100.0 |
| Beneficiaries with: | |||
| Mental Illness and Any Co-occurring SA, MR/DD, or OBD | 11.5 | 30.1 | 49.4 |
| Mental Illness Only | 8.1 | 15.6 | 21.6 |
| Mental Illness and SA | 0.9 | 2.9 | 4.6 |
| Mental Illness and MR/DD | 1.5 | 8.4 | 17.4 |
| Mental Illness and OBD | 1.2 | 5.1 | 8.0 |
| Any Mental, SA, MR/DD, or OBD | 14.6 | 48.3 | 79.8 |
| SA only, MR/DD only, and OBD only | 3.1 | 17.5 | 30.5 |
| SOURCE: New Jersey MSIS Files, 1999. NOTE: SA is Substance Abuse; MR/DD is Mental Retardation/Developmental Disabilities; OBD is Organic Brain Disorder. Expenditures are adjusted for person-years. | |||
The descriptive data in Table III.3 illustrate in a general way the differences between all Medicaid beneficiaries in New Jersey in 1999 and those with mental illness. Further analyses or drill downs could be used to identify more precisely the subgroups that are at greatest risk of having mental health problems. For example, gender and race cross tabulations (see Appendix A) provide further insight into the beneficiaries who are most likely to have mental illness. Other cross-tabulations (for example, race by program eligibility) could provide program administrators with additional information useful for developing targeted mental health services.
| TABLE III.3. Characteristics of All Medicaid Beneficiaries and Medicaid Beneficiaries with Mental Illness, New Jersey, 1999 | ||||
| All Beneficiaries | Beneficiaries with Mental Illness | |||
| Number | Percent | Number | Percent | |
| Total | 868,106 | 100.0 | 99,976 | 100.0 |
| Gender | ||||
| - Females | 526,760 | 60.7 | 55,490 | 55.5 |
| - Males | 341,346 | 39.3 | 44,486 | 44.5 |
| Age | ||||
| - 0-17 | 450,268 | 51.9 | 31,696 | 31.7 |
| - 18-21 | 47,855 | 5.5 | 3,994 | 4.0 |
| - 22-29 | 64,414 | 7.4 | 6,801 | 6.8 |
| - 30-39 | 67,855 | 7.8 | 15,302 | 15.3 |
| - 40-44 | 26,912 | 3.1 | 8,699 | 8.7 |
| - 45-49 | 19,586 | 2.4 | 6,793 | 6.8 |
| - 50-59 | 33,352 | 3.8 | 9,753 | 9.8 |
| - 60-64 | 16,156 | 1.9 | 3,475 | 3.5 |
| - 65+ | 141,706 | 16.3 | 13,463 | 13.5 |
| Race | ||||
| - White | 261,212 | 30.1 | 44,646 | 44.7 |
| - Black | 299,904 | 24.5 | 29,440 | 29.4 |
| - Hispanic | 194,266 | 22.4 | 13,364 | 13.4 |
| - Other | 112,724 | 13.0 | 12,526 | 12.5 |
| Program Eligibility | ||||
| - SSI Aged | 50,158 | 5.8 | 4,796 | 4.8 |
| - Other Aged | 91,548 | 10.5 | 8,667 | 8.7 |
| - SSI Disabled | 97,855 | 11.3 | 35,968 | 36.0 |
| - Other Disabled | 27,221 | 3.1 | 6,776 | 6.8 |
| - AFDC Adults | 39,759 | 4.6 | 4,962 | 5.0 |
| - Other Adults | 91,092 | 10.5 | 13,090 | 13.1 |
| - AFDC Children | 116,943 | 13.5 | 7,614 | 7.6 |
| - Other Children | 353,528 | 40.7 | 18,103 | 18.1 |
| Dual Status | ||||
| - Aged, Full Medicaid | 100,403 | 11.6 | 11,271 | 11.3 |
| - Disabled, Full Medicaid | 35,200 | 4.1 | 12,090 | 12.1 |
| - Aged & Disabled, Lim. Medicaid | 24,873 | 2.9 | 270 | 0.3 |
| - Disabled Non-Duals | 86,761 | 10.0 | 31,147 | 31.2 |
| - Non-Duals | 620,869 | 71.5 | 45,198 | 45.2 |
| SOURCE: New Jersey MSIS Files, 1999. NOTE: Aged groups include beneficiaries who are 65 years old or older. Aged & Disabled with Limited Medicaid are beneficiaries for whom Medicaid pays Medicare premiums only. | ||||
IV. USE AND COSTS OF SERVICES
In addition to knowing the characteristics and eligibility status of beneficiaries with mental illness, program administrators and policy makers would benefit from understanding what services were used by these beneficiaries and how much these services cost. MSIS data files include extensive information on services and expenditures, and can be used to identify the dollars spent on specific services for specific subgroups of individuals within the group of beneficiaries with mental illness. In this chapter, we first examine the percent of beneficiaries with mental illness that use selected types of services. We then drill down somewhat further and examine service use for males and females in two age groups. In the chapters final section, we present findings on expenditures for services by age, gender, racial, and program eligibility subgroups.
A. Percent of Beneficiaries Using Selected Types of Services
To illustrate patterns of service use, we present information related to three types of mental health services: inpatient, outpatient, and psychopharmacological services. Overall, of the 99,976 beneficiaries with mental illness in New Jersey in 1999, 13.5 percent used inpatient mental health services, 36.8 percent used outpatient mental health services, and 53.2 percent were given psychiatric medications (Table IV.1). These data underscore the frequency of psychiatric treatment that is based on medication only.
We found that a slightly higher percent of females compared with males were inpatients (14.1 percent vs 12.7 percent) and were given psychiatric medications (55.2 percent vs 50.7 percent). The pattern was reversed for outpatient services, where proportionally fewer females used these services compared with males (31.0 percent vs 44.0 percent). Overall, adult males are far less likely than adult females to be covered by Medicaid unless they are disabled; hence, it is possible that a larger proportion of male beneficiaries are eligible because of serious mental illness that leads to hospitalizations. Additional analyses and possibly fieldwork to gather more qualitative data would be needed to identify other reasons behind these results.
We found substantial differences across age groups (Table III.1). For example, children are far less likely to use inpatient services than adults and somewhat more likely to use outpatient services. The percent of each age group that use psychiatric medications increases consistently with age, from 23.3 percent for children to 83.4 for beneficiaries aged 60-64.
| TABLE IV.1. Percent of Medicaid Beneficiaries with Mental Illness Using Selected Mental Health Services by Demographic Characteristics and Program Status, New Jersey, 1999 | ||||
| Number of Beneficiaries | Percent Using | |||
| Inpatient Mental Health Services | Outpatient Mental Health Services | Medicaid-Covered Medications | ||
| Total | 99,976 | 13.5 | 36.8 | 53.2 |
| Gender | ||||
| - Females | 55,490 | 14.1 | 31.0 | 55.2 |
| - Males | 44,486 | 12.7 | 44.0 | 50.7 |
| Age | ||||
| - 0-17 | 31,696 | 7.5 | 46.7 | 23.3 |
| - 18-21 | 3,994 | 16.9 | 39.3 | 35.4 |
| - 22-29 | 6,801 | 16.2 | 38.8 | 49.4 |
| - 30-39 | 15,302 | 16.1 | 44.1 | 57.7 |
| - 40-44 | 8,699 | 16.4 | 40.6 | 69.0 |
| - 45-49 | 6,793 | 15.9 | 37.7 | 74.0 |
| - 50-59 | 9,753 | 15.7 | 27.4 | 80.4 |
| - 60-64 | 3,475 | 15.5 | 17.7 | 83.4 |
| - 65+ | 13,463 | 17.1 | 12.3 | 77.4 |
| Race | ||||
| - White | 44,646 | 15.4 | 34.8 | 63.1 |
| - Black | 29,440 | 13.3 | 44.7 | 41.8 |
| - Hispanic | 13,364 | 7.8 | 33.6 | 29.3 |
| - Other | 12,526 | 13.3 | 28.6 | 70.2 |
| Program Eligibility | ||||
| - SSI Aged | 4,796 | 18.8 | 8.9 | 84.7 |
| - Other Aged | 8,667 | 16.2 | 14.1 | 73.4 |
| - SSI Disabled | 35,968 | 16.6 | 33.7 | 72.8 |
| - Other Disabled | 6,776 | 19.4 | 25.5 | 82.3 |
| - AFDC Adults | 4,962 | 8.0 | 41.7 | 14.2 |
| - Other Adults | 13,090 | 9.7 | 65.8 | 44.7 |
| - AFDC Children | 7,614 | 4.2 | 43.2 | 6.0 |
| - Other Children | 18,103 | 10.4 | 40.4 | 22.1 |
| Dual Status | ||||
| - Aged, Full Medicaid | 11,271 | 18.0 | 11.3 | 78.7 |
| - Disabled, Full Medicaid | 12,090 | 20.7 | 26.3 | 87.3 |
| - Aged & Disabled, Lim. Medicaid | 270 | 3.3 | 63.3 | 35.2 |
| - Disabled Non-Duals | 31,147 | 15.8 | 34.2 | 69.6 |
| - Non-Duals | 45,198 | 8.9 | 47.5 | 26.5 |
| SOURCE: New Jersey MSIS Files, 1999. NOTE: Aged groups include beneficiaries who are 65 years old or older. Aged & Disabled with Limited Medicaid are beneficiaries for whom Medicaid pays Medicare premiums only. | ||||
Patterns of service use differ by race. For example, a smaller percentage of Hispanic beneficiaries use inpatient services (7.8 percent) and receive psychiatric medications (29.3 percent) compared with other racial groups and a larger percentage of Black beneficiaries use outpatient services (44.7 percent).
Service utilization patterns also vary by program eligibility group (Table IV.1). Proportionally more beneficiaries with mental illness who are aged or disabled received inpatient services and psychiatric medications compared to other eligibility categories, and were less likely to have received outpatient mental health services. We found a similar pattern in groups based on dual status, where proportionally more of the aged and disabled duals who had full Medicaid coverage received inpatient care and psychiatric medications and proportionally fewer received outpatient services compared with the non-duals. This finding reflects two familiar patterns of coverage: (1) Medicare pays before Medicaid for Medicare-covered services (such as outpatient psychiatric services) and (2) Medicare does not cover most pharmaceuticals and hence Medicaid covers the major share of prescription drug costs for the dually enrolled.
B. Inpatient Services for Two Age Groups by Gender
To illustrate how MSIS data can be used to identify different service use patterns for different subgroups of beneficiaries with mental illness, we examined inpatient care data for two age groups (Table IV.2). A total of 31,696 beneficiaries aged 0 to 17 had mental illness in New Jersey in 1999 and, of these, 2,364 (7.5 percent) received some inpatient services. In contrast, a total of 15,302 beneficiaries aged 30 to 39 had mental illness and, of these, 2,460 (16.1 percent) received some inpatient services. This information, coupled with additional data found in Appendix A, suggests that older groups of Medicaid beneficiaries include proportionally more individuals who require inpatient psychiatric care compared to younger groups.
New Jersey covers the costs of psychiatric institutional care provided to Medicaid-enrolled children but, like all states, it does not cover such costs for adults.5Table IV.2 reflects these different policies for children and adults. Of the 2,364 children who received inpatient care:
- 326 (13.8 percent) were in institutions for mental disorders for 30 days or less and 786 (33.3 percent) were in these settings for more than 30 days;
- 1,211 (51.2 percent) received services in acute inpatient settings for 30 days or less and 274 received services in these settings for more than 30 days; and
- Less than one percent were in other types of inpatient settings.
In contrast, no adult received care in institutions for mental disorders. Virtually all of the adults aged 30 to 39 who received inpatient care in 1999 were hospitalized in acute inpatient facilities and most of these individuals had short stays. Of these 2,460 beneficiaries:
- 2,132 (86.7 percent) were in acute inpatient facilities for 30 days or less and 263 (10.7 percent) were in for more than 30 days; and
- About 3 percent were in other types of inpatient settings.
Further analyses reveal differences in the use of inpatient services for females and males in the two age groups (Table IV.3). In the younger age group, of those children who receive inpatient care, proportionally more are males (61.3 percent, compared with 38.7 percent of females). Furthermore, boys comprise a greater percentage of the children with long stays. Of all children who stay in institutions for mental disorders for longer than 30 days, 65.8 percent are boys and of all children who stay in acute care facilities for longer than 30 days, 63.1 percent are boys.
In the older age group, of those individuals who receive inpatient care, proportionally more are females (56.6 percent compared with 43.4 percent). Of these adults who stay in acute care facilities for longer than 30 days, about half are women and half are men.
Overall our analyses of inpatient service use suggest that:
- The extent of inpatient care increases proportionally as age increases; i.e., a greater percentage of older age groups are likely to receive inpatient services.
- About two-thirds of children who receive inpatient services are hospitalized in acute inpatient facilities (for example, the psychiatric unit of a childrens hospital) and slightly less than one-half are inpatients in institutions for mental disorders, where many of them stay longer than a month.
- Within the childhood group, boys are disproportionately represented in the group that stays for more than a month in all types of psychiatric inpatient facilities.
- Medicaid does not pay for inpatient services to adults with mental illness, except when adults are hospitalized in acute care facilities, where stays are likely to be less than 30 days.
These analyses illustrate how MSIS data can be used to establish initial benchmarks against which to assess subsequent program changes or as an aid in defining specific measurable targets or objectives for policy initiatives. For example, if a state were to expand or strengthen home and community-based mental health services for children, including hospital diversion and or intensive family support programs, the effect of these initiatives on service use could be measured over time using MSIS data.
| TABLE IV.2. Medicaid Beneficiaries in Two Age Groups Who Received Inpatient Services, New Jersey, 1999 | ||||||||||||||
| Beneficiaries with Mental Illness | Beneficiaries Receiving Inpatient Services In | |||||||||||||
| Any Inpatient Setting | Institutions for Mental Disorders | Acute Care Facilities | Other Inpatient Settings | |||||||||||
| 30 Days or Less | More Than 30 Days | 30 Days or Less | More Than 30 Days | 30 Days or Less | More Than 30 Days | |||||||||
| Age | Number | Number | Number | Percent | Number | Percent | Number | Percent | Number | Percent | Number | Percent | Number | Percent |
| 0-17 | 31,696 | 2,364 | 326 | 13.8 | 786 | 33.3 | 1,211 | 51.2 | 274 | 11.6 | 13 | 0.6 | 0 | -- |
| 30-39 | 15,302 | 2,460 | 0 | -- | 0 | -- | 2,132 | 86.7 | 263 | 10.7 | 74 | 3.0 | 3 | 0.1 |
| SOURCE: New Jersey MSIS Files, 1999. NOTE: Percent columns refer to percentages of beneficiaries in any inpatient setting. Percents add to more than 100 because some beneficiaries received services in more than one type of setting during the year. | ||||||||||||||
| TABLE IV.3. Female and Male Medicaid Beneficiaries in Two Age Groups Who Received Inpatient Services, New Jersey, 1999 | ||||||||||||||
| Beneficiaries Receiving Inpatient Services In | ||||||||||||||
| Any Inpatient Setting | Institutions for Mental Disorders | Acute Care Facilities | Other Inpatient Settings | |||||||||||
| 30 Days or Less | More Than 30 Days | 30 Days or Less | More Than 30 Days | 30 Days or Less | More Than 30 Days | |||||||||
| Number | Percent | Number | Percent | Number | Percent | Number | Percent | Number | Percent | Number | Percent | Number | Percent | |
| 0-17 | 2,364 | 100.0 | 326 | 100.0 | 786 | 100.0 | 1,211 | 100.0 | 274 | 100.0 | 13 | 100.0 | 0 | -- |
| - Females | 914 | 38.7 | 146 | 44.8 | 269 | 34.2 | 504 | 41.6 | 101 | 36.9 | 4 | 30.8 | 0 | -- |
| - Males | 1,450 | 61.3 | 180 | 55.2 | 517 | 65.8 | 707 | 58.4 | 173 | 63.1 | 9 | 69.2 | 0 | -- |
| 30-39 | 2,460 | 100.0 | 0 | -- | 0 | -- | 2,123 | 100.0 | 263 | 100.0 | 74 | 100.0 | 3 | 100.0 |
| - Females | 1,392 | 56.6 | 0 | -- | 0 | -- | 1,230 | 57.7 | 135 | 51.0 | 32 | 43.2 | 1 | 33.3 |
| - Males | 1,068 | 43.4 | 0 | -- | 0 | -- | 902 | 42.3 | 129 | 49.0 | 42 | 56.4 | 2 | 66.7 |
| SOURCE: New Jersey MSIS Files, 1999. NOTE: Aged groups include beneficiaries who are 65 years old or older. Aged& Disabled with Limited Medicaid are beneficiaries for whom Medicaid pays Medicare premiums only. | ||||||||||||||
C. Service Expenditures
Total expenditures for all Medicaid services used by Medicaid beneficiaries with mental illness in New Jersey in 1999 were $1.5 billion, with an average of $15,243 (Table IV.4). The data on total expenditures provides a somewhat different picture compared with the data on mean expenditures. Overall, total expenditures for females are higher than for males ($859,316,000 versus $664,553,000) but average expenditures are quite similar ($15,486 versus $14,939). The amount of total expenditures on health services provided to children with mental health conditions ($263,563,000) is quite high relative to the other age groups, but the average expenditure is quite low ($8,316). Total expenditures for white beneficiaries were more than twice the total expenditures for black beneficiaries, but the average expenditure was 50 percent higher. Similar differences are evident for the different eligibility groups and for the dual groups.
Table IV.4 also shows mean expenditures for all Medicaid services provided in 1999 to individuals with mental illness who used selected types of mental health services. The mean Medicaid expenditure was $26,940 for beneficiaries with mental illness who used inpatient services, $17,907 for beneficiaries who used outpatient services, and $20,374 for those who were prescribed psychiatric medications.
Mean expenditures for all Medicaid services were quite similar for female and male beneficiaries who had mental illness and who used outpatient mental health services and received psychiatric medications. However, males who used inpatient mental health services had somewhat higher mean Medicaid expenditures compared with females ($29,930 versus $24,749), possibly because of slightly longer lengths of stay in some age groups.
Substantially different cost patterns are evident across the age groups and across service types (Table IV.4). For example, mean Medicaid expenditures:
- Increase consistently with age for those who use outpatient mental health services, from $10,033 for children to $24,752 for beneficiaries over 65.
- Are high for children who use inpatient mental health services ($37,765), decrease for adults in their twenties who use inpatient services ($20,354), and increase again for the elderly who use inpatient services ($29,215).
- Are lower for children who use psychiatric medications ($15,526), increase somewhat for young adults who use psychiatric medications ($18,596) for the 20-29 year old group) and stay at that level through adulthood, and then increase again for beneficiaries over 65 who use psychiatric medications ($25,567).
| TABLE IV.4. Expenditures for Medicaid Services for all Beneficiaries with Mental Illness and Beneficiaries with Mental Illness Who Used Selected Mental Health Services, by Demographic Characteristics and Eligibility Status, New Jersey, 1999 | |||||
| Expenditures for All Health Services by Beneficiaries with Mental Illness | Mean Expenditures for All Health Services by Beneficiaries with Mental Illness Who Used | ||||
| Total Expenditures(in 1,000s) | Mean Expenditures | Inpatient Mental Health Services | Outpatient Mental Health Services | Psychiatric Medications | |
| Total | $1,523,870 | $15,243 | $26,940 | $17,907 | $20,374 |
| Gender | |||||
| - Females | $859,316 | $15,486 | $24,794 | $17,658 | $20,418 |
| - Males | $664,553 | $14,939 | $29,930 | $18,126 | $20,314 |
| Age | |||||
| - 0-17 | $263,563 | $8,316 | $37,765 | $10,033 | $15,536 |
| - 18-21 | $42,918 | $10,746 | $28,158 | $11,940 | $17,390 |
| - 22-29 | $91,811 | $13,500 | $20,354 | $21,921 | $18,596 |
| - 30-39 | $243,559 | $15,917 | $20,460 | $21,462 | $20,025 |
| - 40-44 | $151,787 | $17,449 | $22,701 | $23,455 | $19,766 |
| - 45-49 | $130,074 | $19,148 | $24,656 | $26,577 | $20,485 |
| - 50-59 | $191,492 | $19,634 | $26,458 | $29,334 | $19,994 |
| - 60-64 | $70,798 | $20,374 | $28,408 | $30,447 | $20,742 |
| - 65+ | $337,867 | $25,096 | $29,215 | $24,752 | $25,567 |
| Race | |||||
| - White | $876,118 | $19,624 | $27,708 | $24,246 | $23,192 |
| - Black | $385,191 | $13,084 | $27,551 | $13,619 | $20,459 |
| - Hispanic | $92,263 | $6,904 | $22,164 | $8,249 | $11,989 |
| - Other | $170,297 | $13,596 | $25,337 | $18,213 | $14,969 |
| Program Eligibility | |||||
| - SSI Aged | $89,791 | $18,722 | $25,366 | $19,798 | $18,946 |
| - Other Aged | $248,076 | $28,623 | $31,698 | $26,492 | $29,800 |
| - SSI Disabled | $522,172 | $14,518 | $24,100 | $17,504 | $16,139 |
| - Other Disabled | $142,717 | $21,062 | $22,529 | $16,608 | $21,456 |
| - AFDC Adults | $26,398 | $5,320 | $11,890 | $6,662 | $6,951 |
| - Other Adults | $308,549 | $23,571 | $27,579 | $31,701 | $32,811 |
| - AFDC Children | $32,242 | $4,235 | $14,824 | $5,594 | $5,700 |
| - Other Children | $153,925 | $8,503 | $41,046 | $9,794 | $18,899 |
| Dual Status | |||||
| - Aged, Full Medicaid | $294,523 | $26,131 | $28,539 | $25,174 | $26,319 |
| - Disabled, Full Medicaid | $189,415 | $15,667 | $16,630 | $16,567 | $15,927 |
| - Aged & Disabled, Lim. Medicaid | $2,736 | $10,135 | $13,298 | $11,147 | $10,034 |
| - Disabled Non-Duals | $487,511 | $15,652 | $27,811 | $17,730 | $17,780 |
| - Non-Duals | $549,684 | $12,162 | $31,508 | $17,816 | $24,661 |
| SOURCE: New Jersey MSIS Files, 1999. NOTE: Aged groups include beneficiaries who are 65 years old or older. Aged & Disabled with Limited Medicaid are beneficiaries for whom Medicaid pays Medicare premiums only. | |||||
Mean Medicaid expenditures for all racial groups who use inpatient services are similar, but there are wide variations in mean Medicaid expenditures for users of outpatient mental health services and psychiatric medications across racial groups. Mean expenditures for Hispanic beneficiaries, however, are consistently less than mean expenditures for white or black beneficiaries.
In general, beneficiaries in the other aged and other adults groups have higher mean Medicaid expenditures compared with beneficiaries in the other eligibility groups. Variation also is evident across groups of beneficiaries with and without Medicare.
V. CHARACTERISTICS OF HIGH-COST BENEFICIARIES
In general, a small proportion of the population of individuals enrolled in health plans account for a large proportion of the expenditures. Program administrators and policy makers are naturally interested in identifying the individuals who are likely to use many services (i.e., the high-cost beneficiaries) because of the possible fiscal benefits that can ensue from efforts, such as care coordination, that aim to track and reduce their expenditures.
To examine characteristics of the high-cost beneficiaries with mental illness in New Jersey in 1999, we first divided the population of beneficiaries with mental illness into five groups, each with an equal number of individuals, where the first group included all those with the smallest total Medicaid expenditures and the last group included all those with the highest total Medicaid expenditures. Figure V.1 presents the total expenditures for each quintile and shows that the total expenditures for the fifth quintile ($1.1 billion) is 3.3 times more than the total expenditures for the fourth quintile ($336 million) and 49.6 times more than the total expenditures for the lowest quintile ($22,079).
| TABLE V.1. Characteristics of Beneficiaries with Mental Illness in the Highest Cost Quintile, New Jersey, 1999 | ||||
| Beneficiaries with Mental Illness | Beneficiaries with Mental Illness in the Highest Cost Quintile | |||
| Number | Percent | Number | Percent | |
| Total | 99,976 | 100.0 | 19,995 | 100.0 |
| Gender | ||||
| - Females | 55,490 | 55.5 | 11,655 | 58.3 |
| - Males | 44,486 | 44.5 | 8,340 | 41.7 |
| Age | ||||
| - 0-17 | 31,696 | 31.7 | 2,292 | 11.5 |
| - 18-21 | 3,994 | 4.0 | 446 | 2.2 |
| - 22-29 | 6,801 | 6.8 | 1,060 | 5.3 |
| - 30-39 | 15,302 | 15.3 | 2,805 | 14.0 |
| - 40-44 | 8,699 | 8.7 | 1,791 | 9.0 |
| - 45-49 | 6,793 | 6.8 | 1,569 | 7.8 |
| - 50-59 | 9,753 | 9.8 | 2,363 | 11.8 |
| - 60-64 | 3,475 | 3.5 | 975 | 4.9 |
| - 65+ | 13,463 | 13.5 | 6,694 | 33.5 |
| Race | ||||
| - White | 44,646 | 44.7 | 12,734 | 63.7 |
| - Black | 29,440 | 29.4 | 4,561 | 22.8 |
| - Hispanic | 13,526 | 12.5 | 1,956 | 9.8 |
| - Other | 12,526 | 12.5 | 1,956 | 9.8 |
| Program Eligibility | ||||
| - SSI Aged | 4,796 | 4.8 | 1,195 | 6.0 |
| - Other Aged | 8,667 | 8.7 | 5,499 | 27.5 |
| - SSI Disabled | 35,968 | 36.0 | 5,432 | 27.2 |
| - Other Disabled | 6,776 | 6.8 | 1,681 | 8.4 |
| - AFDC Adults | 4,962 | 5.0 | 114 | 0.6 |
| - Other Adults | 13,090 | 13.1 | 4,456 | 22.3 |
| - AFDC Children | 7,614 | 7.6 | 118 | 0.6 |
| - Other Children | 18,103 | 18.1 | 1,500 | 7.5 |
| Dual Status | ||||
| - Aged, Full Medicaid | 11,271 | 11.3 | 5,988 | 29.9 |
| - Disabled, Full Medicaid | 12,090 | 12.1 | 1,967 | 9.8 |
| - Aged & Disabled, Lim. Medicaid | 270 | 0.3 | 15 | 0.1 |
| - Disabled Non-Duals | 31,147 | 31.2 | 5,325 | 26.6 |
| - Non-Duals | 45,198 | 45.2 | 6,700 | 33.5 |
| SOURCE: New Jersey MSIS Files, 1999. NOTE: Aged groups include beneficiaries who are 65 years old or older. Aged & Disabled with Limited Medicaid are beneficiaries for whom Medicaid pays Medicare premiums only. | ||||
Characteristics of the group of beneficiaries in the highest cost quintile (i.e., the fifth quintile) are different from the characteristics of all beneficiaries with mental illness (Table V.1). Specifically, compared with the group of beneficiaries with mental illness overall, the highest cost quintile subgroup has:
- Slightly more females,
- Substantially more individuals in the older age groups,
- Substantially more white beneficiaries,
- Fewer individuals from the child-related eligibility groups and more individuals from the aged eligibility groups,
- Substantially more aged individuals with Medicare.
Medicaid expenditures for the 19,995 individuals in the highest quintile of beneficiaries with mental illness total to more than $1 billion (Table V.2). As this table shows, patterns of total and mean expenditures vary substantially across subgroups. For example, Medicaid expenditures for the 6,694 individuals in the over-65 age group totaled $274 million, with an average of $40,932. In contrast, expenditures for the 2,292 individuals in the childhood group totaled $132 million, with an average of $57,592.
The information in Table V.2 could be used to select an appropriate group for a care management intervention. For example, of the 19,995 beneficiaries in the highest quintile, 1,681 were in the Other Disabled group. Average Medicaid expenditures for these beneficiaries were $63,058, which is well above the mean for the total group of beneficiaries in the highest cost quintile ($51,492), suggesting that these individuals are probably receiving multiple health services and possibly multiple or frequent psychiatric medications. It would be of considerable interest to determine whether a focused service coordination program directed specifically at the Other Disabled group could improve their overall care and potentially reduce costs. A five percent reduction in total expenditures for this group alone would save New Jerseys program over $5 million (1,691 multiplied by $3,153). Even after accounting for the cost of operating the service coordination program, New Jersey would be saving a substantial sum.
Developing a feasible care coordination program necessarily would depend on many factors other than cost. However, analysis of MSIS data can provide a method for identifying target groups who might benefit from special programs and for developing initial financial objectives for these programs.
| TABLE V.2. Expenditures for Medicaid Services for Beneficiaries with Mental Illness in the Highest Cost Quintile by Demographic Characteristics and Eligibility Status, New Jersey, 1999 | |||
| Number of Beneficiaries and Expenditures for All Health Services | |||
| Beneficiaries | Total Dollars(in millions) | Mean Dollars | |
| Total | 19,995 | $1,016 | $50,813 |
| Gender | |||
| - Females | 11,655 | $576 | $49,421 |
| - Males | 8,340 | $441 | $52,878 |
| Age | |||
| - 0-17 | 2,292 | $132 | $57,592 |
| - 18-21 | 446 | $26 | $58,296 |
| - 22-29 | 1,060 | $57 | $53,774 |
| - 30-39 | 2,805 | $157 | $55,971 |
| - 40-44 | 1,791 | $100 | $55,835 |
| - 45-49 | 1,569 | $89 | $56,724 |
| - 50-59 | 2,363 | $132 | $55,861 |
| - 60-64 | 975 | $50 | $51,282 |
| - 65+ | 6,694 | $274 | $40,932 |
| Race | |||
| - White | 12,734 | $646 | $50,730 |
| - Black | 4,561 | $236 | $51,743 |
| - Hispanic | 744 | $37 | $49,731 |
| - Other | 1,956 | $98 | $50,102 |
| Program Eligibility | |||
| - SSI Aged | 1,195 | $58 | $48,536 |
| - Other Aged | 5,499 | $215 | $39,098 |
| - SSI Disabled | 5,432 | $294 | $54,124 |
| - Other Disabled | 1,681 | $106 | $63,058 |
| - AFDC Adults | 114 | $4 | $35,088 |
| - Other Adults | 4,456 | $242 | $54,309 |
| - AFDC Children | 118 | $5 | $42,373 |
| - Other Children | 1,500 | $92 | $61,333 |
| Dual Status | |||
| - Aged, Full Medicaid | 5,988 | $243 | $40,581 |
| - Disabled, Full Medicaid | 1,967 | $115 | $58,465 |
| - Aged & Disabled, Lim. Medicaid | 15 | $1 | $66,667 |
| - Disabled Non-Duals | 5,325 | $294 | $55,211 |
| - Non-Duals | 6,700 | $363 | $54,179 |
| SOURCE: New Jersey MSIS Files, 1999. NOTE: Aged groups include beneficiaries who are 65 years old or older. Aged & Disabled with Limited Medicaid are beneficiaries for whom Medicaid pays Medicare premiums only. | |||
VI. LESSONS LEARNED, POLICY IMPLICATIONS, AND POTENTIAL NEXT STEPS
MSIS data provide valuable opportunities to examine service use and expenditures for Medicaid beneficiaries with mental illness. This study examined MSIS data from one state to illustrate how such data can be used to address important policy issues. Our analyses provide two sets of findings. The first pertains to our policy results on service use and expenditures. The second involves the methodological results on the strengths and weaknesses of using MSIS data. In this chapter, we first summarize our findings on patterns of service use and cost and then suggest potential next steps for the application of MSIS data to the study of service use by Medicaid beneficiaries with mental illness. The final section of the chapter describes our findings regarding the utility of MSIS data.
A. Patterns of Service Use and Expenditures
Our analyses provided substantial information on the services used by Medicaid beneficiaries with mental illness in New Jersey in 1999. Our findings include the following:
- Overall, of the 99,976 beneficiaries with mental illness in New Jersey in 1999, 13.5 percent used inpatient mental health services, 36.8 percent used outpatient mental health services, and 53.2 percent were given psychiatric medications.
- A slightly higher percent of females compared with males were inpatients (14.1 percent vs 12.7 percent) and were given psychiatric medications (55.2 percent vs 50.7 percent), but the pattern was reversed for outpatient services, where proportionally fewer females used these services compared with males (31.0 percent vs 44.0 percent).
- There are substantial differences across age groups in service use; children are far less likely to use inpatient services than adults and somewhat more likely to use outpatient services.
- Patterns of service use also differ by race; fewer Hispanic beneficiaries use inpatient services and receive psychiatric medications compared to other racial groups and a larger percentage of Black beneficiaries use outpatient services.
- Service patterns vary by program eligibility group and dual status; proportionally more beneficiaries with mental illness who are aged or disabled and who had Medicare received inpatient services and psychiatric medications compared with other program categories.
To illustrate how MSIS data can be used to identify different service use patterns for different subgroups of beneficiaries with mental illness, we examined inpatient care data first for two age groups and then for males and females in each of these age groups. Key findings from this analysis include:
- A total of 31,696 beneficiaries aged 0 to 17 had mental illness in New Jersey in 1999 and, of these, 7.5 percent received some inpatient services; in contrast, a total of 15,302 beneficiaries aged 30 to 39 had mental illness and, of these, 16.1 percent received some inpatient services.
- Of the 7,458 children who received inpatient care, 47.1 percent were in institutions for mental disorders and 62.8 percent received services in acute inpatient settings; in contrast, no adult received care in institutions for mental disorders, which means that virtually all (97.4 percent) of the adults aged 30 to 39 who received inpatient care in 1999 were hospitalized in acute inpatient facilities.
- Of all children who received inpatient care, proportionally more are males (61.3 percent, compared with 38.7 percent of females); in the group of beneficiaries aged 30 to 39, of those individuals who received inpatient care, proportionally more were females (56.6 percent, compared with 43.4 percent of males).
Analyses of expenditures indicated the following:
- Total expenditures for all Medicaid services used by Medicaid beneficiaries with mental illness in New Jersey in 1999 were $1.5 billion, with an average of $15,243.
- Overall, total expenditures for females are higher than for males ($859,316 versus $664,553) but average expenditures are quite similar ($15,486 versus $14,939).
- The amount of total expenditures on health services provided to children with mental health conditions ($263,563,000) is quite high relative to the other age groups, but the average expenditure is quite low ($8,316).
- Total expenditures for white beneficiaries were more than twice the total expenditures for black beneficiaries, but the average expenditure was 50 percent higher.
- The mean Medicaid expenditure was $26,940 for beneficiaries with mental illness who used inpatient services, $17,907 for beneficiaries who used outpatient services, and $20,374 for those who were prescribed psychiatric medications.
- Mean Medicaid expenditures increase consistently with the age for those who use outpatient mental health services, from $10,033 for children to $24,752 for beneficiaries over 65.
- Mean Medicaid expenditures are high for children who use inpatient mental health services ($37,765), decrease for adults in their twenties who use inpatient services ($20,354), and increase again for the elderly who use inpatient services ($29,215).
- In general, beneficiaries in the other aged and other adults groups have higher mean Medicaid expenditures compared with beneficiaries in the other eligibility groups.
Our analyses of the characteristics of the high-cost beneficiaries with mental illness indicated the following:
- Total expenditures for the highest quintile ($1.1 billion) is 3.3 times more than the total expenditures for the fourth quintile ($336 million) and 49.6 times more than the total expenditures for the lowest quartile ($22,079).
- Compared with all beneficiaries, the highest cost quintile group has slightly more females, substantially more individuals in the older age groups, more white beneficiaries, fewer individuals from the child-related eligibility groups, more individuals from the aged eligibility groups, and substantially more aged individuals with Medicare.
B. Next Steps
This report summarizes only a portion of the data included in the tables in Appendix A because the primary purpose of this study was to assess the feasibility of using MSIS data to examine patterns of service use and expenditures for beneficiaries with mental illness. Therefore, one possible next step could be to address selected questions regarding particular subgroups of beneficiaries or particular services by examining further the data already prepared. For example, it would be possible to develop tables specifically illustrating patterns of service use and cost for gender by age subgroups. These tables could help determine whether male and female beneficiaries of the same age had different patterns of service use.
In addition, using the analytical files from which the tables were generated, analyses similar to the ones presented in this report could be completed for beneficiaries (1) with mental illness and specific co-occurring conditions and (2) with any one of the conditions alone (for example, beneficiaries with only substance abuse). It would be of interest to compare outpatient service use with rates of inpatient service use for subgroups of individuals with mental illness with and without co-occurring conditions. These analyses would assist policy makers and program administrators to identify subgroups within the Medicaid population who are at particularly high risk for using substantial amounts of mental health services.
Finally, we examined data from only one state for only one year. Mental health policy makers, program administrators, and researchers would have considerable interest in examining data from other states over a longer period of time. For example, considerable attention is now being focused on developing community-based services as alternatives to residential care for youth with serious emotional disorders. MSIS files could be used to identify longitudinal patterns in the use of community services in relation to inpatient services for this group of children.
C. Utility of MSIS Data
Our analyses of MSIS data underscore their usefulness for documenting patterns of service use and expenditures for Medicaid beneficiaries with mental illness. Our approach suggests several specific strengths of MSIS data. First, MSIS eligibility and claims files provide information on the demographic characteristics, program eligibility, and dual status of beneficiaries. This information can be used to identify strategically selected subgroups of individuals, such as Hispanic males and females in their twenties, and these different subgroups can be compared in relation to service use or expenditures. The flexibility of these data allow for a large number of subgroup analyses, which can be used to address a wide range of specific policy questions.
A second benefit of MSIS data involves information on services. Just as the individuals in the population can be sorted into policy relevant subgroups, so can different services be grouped into selected categories. In this study, for example, we grouped mental health services into inpatient, community-based, and pharmaceutical service categories. Numerous other combinations of physical and mental health services could be generated, depending on the policy issue.
Third, MSIS data files provide information on both service use and expenditures. Both types of data are useful for policy analyses because together they can clarify the underlying reasons for expenditure patterns. For example, a particular subgroup may have high total expenditures because they use a few services that are extremely costly or because they use many services that are moderately costly. This difference can have different program and policy implications. Our analysis of subgroups within the highest cost quintile further demonstrates how service use and expenditure data can be combined to suggest what groups could be selected for quality-of-care or cost-reduction initiatives.
Although MSIS data offer important opportunities for policy research, they also have critical drawbacks with respect to methods and content. Specifically, preparing MSIS files requires substantial experience with Medicaid data in order to avoid errors in downloading and aggregating data for beneficiary subgroups. In addition, MSIS data provide information only on (1) services used and not services needed by a beneficiary and (2) Medicaid-covered services and not all health-related services. In this respect, they present only a partial picture of health services provided to beneficiaries. Furthermore, they do not include any out-of-pocket payments that beneficiaries make for health services, and hence do not account fully for the cost of all health services that these individuals receive.
Finally, MSIS data can be more or less useful depending on the extent of managed care penetration. For example, some states have large managed care enrollments; data reporting systems that include encounter data for beneficiaries in managed care plans are still poorly developed in most of these states. Hence, analyses of policy issues regarding mental health service use may not be possible in these states.
REFERENCES
Bazelon Center for Mental Health Law. Recovery in the Community: Funding Mental Health Rehabilitative Approaches Under Medicaid. Washington, DC: Bazelon Center for Mental Health Law, November 2001.
Government Accounting Office. Mental Health: Community-Based Care Increases for People with Serious Mental Illness. Washington, DC: December 2000.
Iezzoni, Lisa. "Risk Adjustment for Measuring Health Outcomes, Third Edition." Washington, DC: Academy Health/Health Administration Press. 2003.
New Freedom Commission on Mental Health, Achieving the Promise: Transforming Mental Health Care in America. Final Report. HHS Pub. No. SMA-03-3832. Rockville, MD: 2003.
U.S. Supreme Court, Olmstead v. L.C., 527 U.S. 581, 1999.
NOTES
-
The MSIS files contain administrative and claims data that states submit quarterly to the Centers for Medicaid and Medicare (CMS). These data are submitted in a standardized format and are checked extensively to ensure that they meet explicit standards of quality. If files do not meet standards, they are returned to the state for correction or upgrading. Data are approved for research use only when the standards are met. This report is one of three reports produced for ASPE under the same contract. The other reports are "Using MSIS Data to Analyze Medicaid Coverage of Noninstitutional Long-Term Care in Four States in 1999" and "Using Medicaid Statistical Information System (MSIS) Data for Analysis of Medicaid Managed Care Enrollment." These reports can be obtained by contacting Ann Cherlow at acherlow@mathematica-mpr.com.
-
The information in MSIS files also can be used to assess quality of care by examining whether actual service patterns conform to expected or desired patterns. For example, it would be possible to determine the extent to which beneficiaries who were discharged from inpatient settings received subsequent outpatient services. We did not pursue these types of analyses in this project because our overall goal was to provide descriptive rather than evaluative data.
-
The process of obtaining the original MSIS data files from CMS and preparing them for analysis is described in a companion report, "Feasibility of Using Medicaid Statistical Information System (MSIS) Administrative Data for Policy Research."
-
Although administrative and claims files contain substantial amounts of information, they cannot be used to estimate prevalence of mental illness in the population of Medicaid beneficiaries. Some beneficiaries will not use Medicaid services in any particular year, and hence would not appear in the data files. In addition, some beneficiaries with mental illness may use general medical services for physical health problems and their mental health diagnosis would not be recorded. As a result, they would not be identified as having a mental illness. Finally, Medicaid beneficiaries who are also receiving Medicare (i.e., beneficiaries who are "dually eligible") may receive the bulk of mental health services through Medicare. Their residual Medicaid claims may not include diagnostic or service use information that would identify them as having a mental illness when in fact they do.
- Institutions for Mental Diseases (IMDs) are defined as having more than 16 beds and over half of their patients with mental illness diagnoses. Federal Medicaid law stipulates that patients in IMDs who are between 22 and 64 years of age cannot receive Medicaid coverage for any services.
APPENDICES
Appendix A: Detailed Data Tables [This Appendix is in the Portable Document Format (PDF). You will need a copy of the Acrobat Reader in order to view it.]
Appendix B: Definitions of Terms in Data Tables [This Appendix is in the Portable Document Format (PDF). You will need a copy of the Acrobat Reader in order to view it.]
Appendix C: Procedures for Identifying Individuals with Mental Illness; Definition of Inpatient Stays; Procedures for Distinguishing Clinical vs. Supportive Services; Pharmaceutical Groups Used to Define Psychiatric Medications [This Appendix is in the Portable Document Format (PDF). You will need a copy of the Acrobat Reader in order to view it.]
Appendix D: Specific Drugs Identified as Psychiatric Medications [This Appendix is in the Portable Document Format (PDF). You will need a copy of the Acrobat Reader in order to view it.]
Appendix E: File Layout [This Appendix is in the Portable Document Format (PDF). You will need a copy of the Acrobat Reader in order to view it.]