
UNDERSTANDING SUBSTANCE USE DISORDER (SUD) TREATMENT NEEDS USING ASSESSMENT DATA: FINAL REPORT
John Richardson, PhD, Alex Cowell, PhD, Eric Villeneuve, MPH, Jesse Hinde, PhD, Kristine Rae Olmstead, MSPH, and Sarita Karon, PhD
RTI International
February 2020
Printer Friendly Version in PDF Format (43 PDF pages)
ABSTRACT
To identify and address gaps in substance use disorder (SUD) treatment capacity, state and federal policymakers need information on the need and demand for different SUD levels of care. Although there exists some information on SUD treatment capacity by level of care, there is no national database of information on the treatment needs of individuals by level of care. This project explored the feasibility of gathering and utilizing patient placement and other needs assessment data to identify and address unmet patient needs by levels of care. We conducted an environmental scan of existing literature, and held discussions with subject matter experts (SMEs) and with state stakeholders from California, Florida, Maryland, Massachusetts, Missouri, New York, Pennsylvania, and Virginia.
We found substantial variability in whether states required a needs assessment or standardized set of intake questions. Even states that used the same placement criteria had different approaches to how they applied the criteria. With regard to the availability of placement criteria data, we found three multi-state data sources, but they are limited in scope and accessibility. Few states analyze their data to assess treatment gaps.
This report was prepared under contract #HHSP233201600021I between HHS's ASPE/DALTCP and RTI International. For additional information about this subject, you can visit the DALTCP home page at https://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-… or contact the ASPE Project Officer at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201; Judith.Dey@hhs.gov.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This report was completed and submitted on August 22, 2019, and updated on December 16, 2019.
TABLE OF CONTENTS
1. BACKGROUND
2.1. Environmental Scan
2.2. Discussions
3. FINDINGS
3.1. How are the Needs Assessments Administered and What is the Context in Which They are Administered?
3.2. How could Data from Recorded Assessments be Obtained for Analysis?
3.3. How have States and Organizations Analyzed the Data?
3.4. What Other Analyses could be Conducted with the Data?
APPENDICES
- APPENDIX A: Search Terms Used for the Environmental Scan
- APPENDIX B: Subject Matter Experts and Reasons for Selection
- APPENDIX C: Subject Matter Expert Discussion Guide
- APPENDIX D: State Discussion Guide
- APPENDIX E: History and Evidence Regarding Placement Assessments
- APPENDIX F: Pathways into Substance Use Disorder Treatment
LIST OF EXHIBITS
- EXHIBIT 1: Selection Criteria for State Discussions
- EXHIBIT 2: Frequency of Re-assessments and Reviews within Residential Care, by State
- EXHIBIT 3: Number of Counties in California Using or Planning to Use Different ASAM-based Tools for Initial Assessment, Full Assessment, and Re-assessment
- EXHIBIT 4: Total Number of GAIN Sites by State in the U.S. Since 1993
- EXHIBIT 5: Reasons for Difference between Indicated Level of Care and Placement Decision
- EXHIBIT 6: Accessibility of Office-based Opioid Treatment Programs in Virginia
- EXHIBIT 7: Types of Analyses State Stakeholders Expressed as Being Useful
- EXHIBIT B-1: SMEs, Their Affiliation, and the Reason for Selecting Them to Participate in this Study
ABSTRACT
To identify and address gaps in substance use disorder (SUD) treatment capacity, state and federal policymakers need information on the need and demand for different SUD levels of care. Although there exists some information on SUD treatment capacity by level of care, there is no national database of information on the treatment needs of individuals by level of care.
This project explored the feasibility of gathering and utilizing patient placement and other needs assessment data to identify and address unmet patient needs by levels of care. We conducted an environmental scan of existing literature, and held discussions with subject matter experts and with state stakeholders from California, Florida, Maryland, Massachusetts, Missouri, New York, Pennsylvania, and Virginia.
We found substantial variability in whether states required a needs assessment or standardized set of intake questions. Even states that used the same placement criteria had different approaches to how they applied the criteria. With regard to the availability of placement criteria data, we found three multi-state data sources, but they are limited in scope or accessibility. Few states analyze their data to assess treatment gaps.
ACRONYMS
The following acronyms are mentioned in this report and/or appendices.
| ARTS | Addiction Recovery Treatment Services |
|---|---|
| ASAM | American Society for Addiction Medicine |
| ASI | Addiction Severity Index |
| ASI-Lite | Addiction Severity Index - Lite |
| CSB | Community Service Board |
| DHHS | New Hampshire Department of Health and Human Services |
| DMAS | Virginia Department of Medical Assistance Services |
| EHR | Electronic Health Record |
| GAIN | Global Appraisal of Individual Needs |
| GPRA | Government Performance and Results Act |
| ISAP | UCLA Integrated Substance Abuse Programs |
| LA | Los Angeles |
| LOCADTR | Level of Care for Alcohol and Drug Treatment Referral tool |
| MCO | Managed Care Organization |
| NASADAD | National Association of State Alcohol and Drug Abuse Directors |
| OhioMHAS | Ohio Department of Mental Health and Addiction Services |
| PhD | Doctor of Philosophy |
| SAMHSA | Substance Abuse and Mental Health Services Administration |
| SBIRT | Screening, Brief Intervention, and Referral to Treatment |
| SME | Subject Matter Expert |
| SUD | Substance Use Disorder |
| TAP | Treatment Assignment Protocol |
| UCLA | University of California Los Angeles |
| WITS | Web Infrastructure Treatment System |
EXECUTIVE SUMMARY
The opioid crisis has highlighted inadequate capacity for substance use disorder (SUD) treatment (Jones, et al., 2015; Andrilla, et al., 2019). To address this treatment gap, state and federal policymakers need information on the intensity of treatment needs among those seeking care and the types of SUD services available. Many states and organizations have categorized SUD services into levels of care (e.g., outpatient, residential) and use intake and patient placement assessments--or more generally needs assessments--to determine the appropriate level of care and services. Although there exists some information on capacity by level of care, there is no national database of information on the treatment needs of individuals by level of care. This project explored the feasibility of gathering and utilizing needs assessment data to identify and address unmet patient needs by levels of care. We conducted an environmental scan of existing literature and discussions with both subject matter experts and state stakeholders from California, Florida, Maryland, Massachusetts, Missouri, New York, Pennsylvania, and Virginia. The major themes and findings are presented under four main research questions:
-
How are the needs assessments administered and what is the context in which they are administered?
-
We found substantial variability in whether states required a needs assessment and standardized set of intake questions. Even though six of eight states in our study used the American Society for Addiction Medicine (ASAM) Patient Placement Criteria (or ASAM Criteria), these states had different approaches to requiring semi-structured or unstructured assessment tools.
-
Results of some assessments may also be biased in that they may reflect more the location of the provider offering the initial assessment than the patient's need for a level of care independent of the location of first contact.
-
If data are recorded, the information is often siloed across states, payers and providers in one of three general areas: third-party databases specific to certain standardized assessment tools; electronic health records; and prior authorization records typically gathered by managed care organizations (MCOs).
-
-
How could data from recorded assessments be obtained for analysis?
-
There is no database that spans all states. We identified three databases that could be used to examine need by level of care across more than one state: the Global Appraisal of Individual Needs (GAIN) database; the ASAM Continuum repository; and the Web Infrastructure Treatment System (WITS), a web-based medical record system.
-
Only the GAIN data can readily be obtained through a research application process. States and organizations need to approve research access for the ASAM Continuum and WITS and some states have been unwilling to share the data due to privacy concerns.
-
-
How have states and organizations analyzed the data?
-
California is the only state in our study that has analyzed and published findings from their needs assessment data like the proportion of individuals seeking treatment by levels of care and the frequency of and reasons why patients receive a different level of care than what was recommended to them.
-
The remaining states plans to examine needs assessments and outcomes by level of care, but they have not executed those plans because of recent changes to their assessment and data collection approaches.
-
-
What other analyses could be conducted with the data?
-
States could map out the recorded needs by level of care and compare them to mapped out resources by level of care.
-
State stakeholders also mentioned that they want to examine timeliness of entering different levels of care, transitions between levels of care, and outcomes related to different levels of care.
-
Our findings highlight that needs assessment data could be a rich source of information, but they are currently an untapped resource for most states. Variation across states in needs assessments and privacy concerns pose challenges to the development of multi-state databases. Despite these challenges, we have identified three data sources in this report that could be used to assess the distribution of SUD needs by level of care. A fourth data source--which we did not assess but could also be useful--is health insurance companies that have MCOs across multiple states. Future research should also examine the feasibility of using MCO data for assessing level of SUD need.
In order to achieve a national perspective of needs by level of care, a new data collection tool may need to be established. One approach would be to develop a free online short assessment tool that results in a provisional level of care recommendation. This could be offered in conjunction with a level of care treatment locator tool and could support individuals attempting to locate needed treatment as well as agencies attempting to gather information nationally about the need across different levels of care.
1. BACKGROUND
To reduce the impact of substance use disorders (SUD) on communities, it is important that people have access to care, and that the type and intensity of that care--or level of care--is appropriate. Studies have found that people who received an appropriate level of care according to pre-established placement criteria or needs assessments had reduced no-show rates (Angarita, et al., 2007), improved retention in treatment (Stallvik, Gastfriend, & Nordahl, 2015), fewer hospital bed-days in the following year (Sharon, et al., 2003), and better substance use outcomes (Magura, et al., 2003; Stallvik, Gastfriend, & Nordahl, 2015) than those who received a lower level of care than what was recommended using the criteria.
Overmatching, or placement in a higher level of care than recommended, has been shown to be associated with increased no-show rates (Magura, et al., 2003) or no improvement in outcome(Angarita, et al., 2007). Even if overmatching does not result in poorer outcomes, it is likely an inefficient use of resources and may crowd out access to higher levels of care that typically have no excess capacity. Depending on the level of care, overmatching may also be contrary to the Olmstead decision[1] that favors the placement of people in less restrictive settings.
People may receive a different level of care than what is recommended for many reasons, such as personal preference or a lack of available providers of the recommended level of care. The opioid crisis has brought concerns about unmet need into sharp focus, as the need for treatment has increased and the capacity to address that need has not been sufficient (Jones, et al., 2015; Andrilla, et al., 2019).
To address treatment gaps across the spectrum of levels of care, policymakers can influence treatment capacity through policy levers, such as regulatory and funding mechanisms, but they need an understanding of the type and quantity of care needed to effectively applythese levers. An impactful response to a shortage of outpatient prescribers of medication assisted treatment, for example, will require different funding streams and regulatory mechanisms than would be needed to address a shortage of residential services. Many states and organizations have tried to categorize types of SUD services into levels of care that require different amounts of resources and regulatory oversight. Thus, data to address the treatment gap should detail the gap at these multiple levels of care, from early SUD interventions to intensive inpatient services.
Data at the appropriate level of detail are available on treatment capacity. For example, the National Survey on Substance Abuse Treatment Services provides treatment capacity data (SAMHSA, n.d.). This survey covers all known public and private drug and alcohol abuse treatment centers in the country and is the primary source of data for Substance Abuse and Mental Health Services Administration's (SAMHSA's) Inventory of Behavioral Health Services. The survey specifically asks facilities about the SUD levels of care offered, and its data can be usedto map capacity and accessibility by level of care and geographic region.
There is, however, no national data source that provides information on the distribution of need for treatment by level of care. Although the National Survey on Drug Use and Health is the leading source of surveillance data on SUD, including need and unmet need for treatment, it does not provide detail on the intersection between need and level of care. Thus, while the survey does provide significant insight into broad gaps in treatment--for example, in 2017, fewer than 20% of people assessed as needing SUD treatment in the United States actually received it (SAMHSA, 2018)--it does not indicate how this proportion varies by levels of care.
Data from the clinical intake process at SUD treatment facilities is a potential untapped source for examining needs among those seeking SUD treatment. During the intake process several assessments may be done. A placement assessment is typically done to determine the appropriate level of care for an individual (e.g., outpatient or residential). A more general term for the different assessments performed is "needs assessments," which includes the intake and placement assessments. The needs assessments may follow a standardized, structured approach resulting in information that is stored centrally within a large electronic database. Most state-funded facilities also must record the results of these needs assessments and share them with the proper authorities to demonstrate medical necessity and receive prior authorization for certain levels of SUD care.
Existing knowledge on the potential for such data is out-of-date. In 2006, the National Association of State Alcohol and Drug Abuse Directors published a report that described the landscape of patient placement criteria used by different state substance abuse agencies (Kolsky, 2006). Since the publication of the report, the criteria may have changed and data availability may have evolved.
The 2006 report does, however, provideuseful information on what kinds of criteria may be used in practice, which in turn would influence the availability and comparability of data on need for treatment by level of care. At the time of the report, 43 states required the use of needs assessments with standard patient placement criteria and 29 specifically required the use of the American Society for Addiction Medicine (ASAM) Criteria. These criteria guide the provider in assessing six broad dimensions of the patient's life and his or her need and readiness for treatment. Other criteria and assessments used by states included the Addiction Severity Index (ASI) and various state-specific criteria like the Pennsylvania Client Placement Criteria, or New York's Level of Care for Alcohol and Drug Treatment Referral (LOCADTR) tool.
| ASAM's Six Dimensions |
|---|
|
Recent growth in the use of centralized electronic health records (EHRs) and adoption of standardized criteria by treatment providers suggest that multi-state data on the distribution of need for treatment may be available. To our knowledge, no recent study has examined how states require the use of different treatment needs or placement assessments; how the data from the assessments are used, stored, and accessed; or the degree to which the data can be used to understand the distribution of treatment needs.
The objective of this project was to determine the feasibility of gathering and using data within and across states to assess the distribution of SUD treatment needs by level of care. The following research questions guided the data collection efforts of this project and are presented in the results of this report:
-
How are the needs assessments (i.e., intake and placement assessments) administered and what is the context in which they are administered?
-
How could data from recorded assessments be obtained for analysis?
-
How have states and organizations analyzed the data?
-
What other analyses could be conducted with the data?
2. DATA AND METHODS
As background for the four research questions, we conducted an environmental scan of the literature and policy documents to describe the needs assessments used by states and organizations. The results of the scan then informed semi-structured stakeholder discussions that provided the bulk of the data for the findings related to the research questions. There were two sets of discussions: discussions with subject matter experts (SMEs) and discussion with state stakeholders.
2.1. Environmental scan
For the environmental scan, we developed a list of search terms based on the initial study questions (see Appendix A for a list of general search terms used). We then applied these terms to Google and Bing search engines, databases of published articles (e.g., PubMed), and specific websites that were relevant to the study (e.g., the ASAM website), and we systematically documented the results. The materials we examined included presentations, reports, peer reviewed manuscripts, and website content. Rather than naively applying terms to search engines, we used a snowball approach to identify related documents that were linked or included as citations in reports.
2.2. Discussions
For the discussions, we drafted a preliminary core list of SMEs and state stakeholders. We cascaded the discussions so that information from discussions with the core group helped us identify other SMEs and refine the list of state stakeholders. In total, we conducted discussion with nine SMEs (see Appendix B for a list) and stakeholders in eight separate states.
Each discussion lasted between 30 minutes and 1 hour; two or more RTI staff (at least one lead discussant and a note-taker) facilitated the discussions. Discussions were semi-structured, where the lead discussant used a prepared discussion guide listing topics and possible questions (see Appendix C for the SME guide and Appendix D for the state stakeholder guide). We tailored each discussion guide to fit with the background and experience of the stakeholder. Discussions were recorded--with discussant agreement--and we used the recording to check the accuracy of notes.
The environmental scan and SME discussions helped refine the criteria for which states would be included in the state stakeholder discussions (Exhibit 1). The sample of states was createdto represent variation across these criteria. For example, one requirement for a state to receive Section 1115 Medicaid Demonstration Waiver to expand coverage of SUD services[2] is that the state mandate the use of evidence-based placement criteria. Thus, the sample includes a mixture of states that did and did not have a SUD 1115 Medicaid Demonstration. Other state selection criteria included the degree to which electronic data could be potentially used, whether intake processes were centralized, and the availability of evaluation reports documenting evaluation findings for SUD 1115 Medicaid Demonstrations.
| EXHIBIT 1. Selection Criteria for State Discussions | ||||||||
|---|---|---|---|---|---|---|---|---|
| Selection Criteria | Targeted States for Discussions | |||||||
| CA | FL | MA | MD | MO | NY | PA | VA | |
| Collecting data systematically through the ASAM Continuum | X[a] | X | X[a] | |||||
| Using the ASAM Criteria | X | X | X | X | X[b] | X | ||
| Using other needs assessments | X | X | ||||||
| Has a centralized electronic reporting system for behavioral health (e.g., WITS) | X | X | X | X | X | X | ||
| Has a centralized intake process or phone line for SUD services | X | X | X | X | X | X | ||
| Has a SUD 1115 demonstration | X | X | X | X | X | |||
| Has generated evaluation reports regarding their SUD 1115 demonstration | X | X | ||||||
NOTE:
| ||||||||
Typically, we conducted one discussion per state with one or more stakeholders at a time. However, for two states (California and Massachusetts) we held multiple discussions. For Californiawe had three discussions: one with Los Angeles (LA) County, which is using the ASAM Continuum; a second with the evaluator of the state SUD 1115 demonstration; and a third with a member of the Department of Health Care Services who oversees ASAM assessments across the state. For Massachusettswe had two discussions with stakeholders with different perspectives: one with Medicaid staff and the other with public health staff.
We systematically synthesized by research question the information from the environmental scan and discussions. For the synthesis, we first reviewed the notes from each discussion and summarized them in a report to ASPE on a continuing basis. We purposively incorporated some of the findingsfrom these preliminary summaries into the dialogue notes for later discussions with other stakeholders. In this way, the summaries were adaptive rather than naive. For this report, we then re-reviewed notes summaries, identified common themes across stakeholders, and documented evidence under each of these themes.
3. FINDINGS
Of the eight states for which we held stakeholder discussions, all but one require the use of evidence-based criteria as part of a needs assessment. There was variation across states, and frequently within states, in how the data were obtained, and definitions of level of care vary by state as well. There are three main sources of centrally held assessment data that could be exploredfor further analyses (see Section 3.2). Other alternatives include working with separate entities such as states and managed care organizations (MCOs) to obtain data. All stakeholders raised the need to appropriately address significant institutional concerns to protect privacy when accessing data.
Although data may be available, in only a few instances had any of the states in which we held discussions performed analyses of need by level of care. California is perhaps the lead example of a state using its own data to address this topic. State stakeholders seem most interested in analyses of transitions between level of care, timeliness in entering into a level of care, and the relationship between level of care and outcomes. By comparing the needs assessment data by level of care to measures of capacity by level of care, states and organizations can better plan for treatment capacity and assess network adequacy.
3.1. How are the Needs Assessments Administered and Whatis the Context in Which They are Administered?
The evidence suggests that nearly all states in our sample required a specific systematic needs assessment to determine appropriate services and level of care. Most, but not all, assessments were modeled on the ASAM Criteria. One state--Missouri--avoided the concept of level of care and deliberately chose to tailor treatment planning to individual needs. Of those states that required a specific approach, some only required the use of criteria or guidelines that allow the provider flexibility in what to ask and how to assess needs (e.g., the ASAM Criteria), whereas others require the use of a structured and standardized assessment tool (e.g., the ASAM Continuum, which is software that integrates with electronic medical records and includes a set of prescribed questions for following the ASAM Criteria). Some states have tried to improve standardization of assessment procedures through training, but there is also variability across states and organizations in how providers are trained.
3.1.1. How do States and Organizations Define SUD Levels of Care?
The SMEs said that the varied definitions of services and levels of care across states pose a major challenge to gathering needs assessment data for understanding the distribution of need by level of care nationally. As a result, multi-state analyses by level of care may need to focus on general categories of care (e.g., residential vs. outpatient) rather than specific subcategories (e.g., different levels of residential) that may have more nuanced definitions which vary by state.
ASAM has established the most widely used framework for defining SUD levels of care (see Appendix E for more information on the history and development of placement assessments). This framework specifies five main levels of care and several sublevels based on the amount and intensity of medical supervision offered with each treatment (ASAM, 2019a). To more clearly define and establish these levels of care in practice, ASAM is working with the Commission on Accreditation of Rehabilitation Facilities to establish a certification and accreditation program for residential levels of care 3.1, 3.5, and 3.7 (ASAM, 2019b). This program will allow for more uniformity and quality assurance among certified residential facilities.
| ASAM Levels of Care |
|---|
| 0.5 - Early Intervention 1 - Outpatient Services 2 - Intensive Outpatient / Partial Hospitalization Services 2.1 - Intensive Outpatient Services 3 - Residential / Inpatient Services 3.1 - Clinically Managed Low-intensity Residential Services 4 - Medically Managed Intensive Inpatient Services |
In contrast to the standardization that ASAM is trying to establish across states, Missouri's approach to publicly-funded SUD treatment is to avoid the use of levels of care categories altogether and focus on whatever blend of services the patient needs that are available locally. Part of the reason for this approach is that not all levels of care are available throughout the state, so state stakeholders are trying to help providers think about how to optimally use the resources that are locally available to achieve the best patient outcomes. This approach has allowed for some home-grown levels of care. State stakeholders also shared that it has been liberating for the providers to focus less on a prescribed checkbox approach in assessments or categories of treatment, and to focus more on the therapeutic alliance and individualized treatment plan for each client.
3.1.2. What are the Key Features of Intake and Re-assessment Processes?
There are several pathways to treatment that may involve primary care referral, criminal justice referral, telephone access lines, central intake centers, and a patient's personal investigations and preferences (see Appendix F for a more detailed description). Some of these pathways, such as telephone access lines, are more likely than others to involve a pre-assessment or screener prior to the initial intake process. These pre-assessments can influence where the individual shows up to receive a full intake and placement assessment. There is also the possibility of gathering and using standardized pre-assessment data that result in a provisional level of care. Among the states for which we held stakeholder discussions, California is the only one gathering some information on the screener results from their access lines.
When an individual shows up at a clinic, an initial interview and assessment are conducted. This initial interview must fulfill clinical and regulatory requirements. It can be a very long process and may need to fulfill some or all of the following purposes:
-
Determine the appropriate level of care for the individual (this is especially done if the facility offers multiple levels of care, or if the placement assessment is required by the funder).
-
Determine whether the payer's medical necessity criteria are met and the prior authorization is received for the certain level of care the client is seeking.
-
Gather information for treatment planning.
-
Gather additional information required from public funding, like the performance data required in the Government Performance and Results Act (GPRA) measurement tool.
-
Establish rapport with the patient.
This intake process may use a structured biopsychosocial needs assessment tool or may be an unstructured or semi-structured conversation with the patient. In some situations, the ASAM Criteria are the entire focus of the interview; in other situations, a separate biopsychosocial assessment is the focus and a placement assessment is just one of the outcomes. In New York, providers may use whatever biopsychosocial assessment they prefer, and then, after the intake interview is complete, they are required to fill out a placement assessment from the information that was gathered.
There are some differences in this process, depending on the level of care. For outpatient services, providers are typically allowed a few sessions before they must submit any required assessment paperwork. For higher levels of care, the assessment is typically required to be completed upon entry into treatment. This is also reflective of the fact that higher levels of care require prior authorization. SMEs and state stakeholders said that needs assessments, which include placement assessments and other biopsychosocial assessments at intake, are done across all levels of specialized SUD treatment and there is no difference in the level of rigor with which these assessments are done by level of care.
Many of the SMEs and state stakeholders also said that within the intake process, the results of a placement assessment may be biased to represent the level of care the treatment facility offers rather than the level of care a patient really needs. This is evident in the high percentage of agreement between the placement decision and the placement recommendation. In California, there was 89% agreement between the placement decision and recommendation across the state. However, representatives from LA County said that their percentage of agreement was much lower. One suggested reason for this is that LA County uses the ASAM Continuum, which outputs a recommended level of care based on an algorithm rather the clinician's judgment. In a validation study of the ASAM Continuum in Norway, the level of agreement was only 57% (Stallvik, Gastfriend, & Nordahl, 2015). Placement assessments that rely only on a clinician's judgment may allow for more people to be classified as needing the level of care that can be supplied at wherever they show up to receive care. This bias may affect the feasibility of distinguishing between the actual need for SUD treatment by level care and the receipt of different levels of care.
For those with comorbid conditions, there is an additional challenge of determining the right combination of mental health and SUD services. The systems of care for treating mental health and SUD are often separate. One state stakeholder said she was not aware of an instrument that considers levels of care for SUD and mental health, and then helps the provider to develop a recommendation for the level of care that is most appropriate across both systems of care. The ASAM Criteria focus on placement into only SUD levels of care. The Level of Care Utilization System for Psychiatrics and Addiction Services places individuals into six different levels of care based on their psychiatric and SUD needs; however, the final output focuses more on mental health levels of care and does not distinguish between SUD and psychiatric treatment needs (Sowers, George, & Thompson, 1999). More work is needed in this field in order to better integrate SUD and mental health services and deliver the combination of care that would be most beneficial to an individual.
Once an individual is in treatment, the frequency of re-assessment varies substantially by state, payer, and level of care. Exhibit 2 provides an example of this variability across residential services in four states. Re-assessment data would be valuable because they capture the patient's trajectory while in treatment. However, even if this information is gathered, it may be challenging to compare across states due to the differences in re-assessment frequency. There is one consistent point in time when re-assessments are done--that is, when patients transition to a different level of care. States would need linked patient records across different levels of care in order to be able to assess re-assessments at times of transitions between levels of care.
| EXHIBIT 2. Frequency of Re-assessments and Reviews within Residential Care, by State | |||
|---|---|---|---|
| Florida | Maryland | Pennsylvania | Massachusetts |
| Re-assessment every 14 days | Re-assessment every 15 days | Updated recovery plan every 60 days | Concurrent review every 90 days |
3.1.3. What Assessments are Used and Why are They Used?
Almost all state stakeholders spoke of the large variability across and within states in terms of the assessments used. This threatens the feasibility of gathering and analyzing data across multiple states. Six of the states with which we had discussions required the use of the ASAM Criteria, and two had developed their own requirements and guidelines for assessments. Even in the six states that require the use of the ASAM Criteria, there is a lack of consistency across providers' intake and placement assessments. For example, the State of California requires the use of the ASAM Criteria, but each county has developed its own approach for conducting an "ASAM-based" assessment (see Exhibit 3 below). Many counties have developed their own set of standardized questions that relate to the ASAM Six Dimensions, whereas others do not specify which questions should be asked--they simply require that providers conduct an assessment that follows the guidelines in the ASAM Criteria Book. A couple of counties (like LA County) use the only standardized assessment tool sanctioned by ASAM, known as the ASAM Continuum.
| EXHIBIT 3. Number of Counties in California Using or Planning to Use Different ASAM-based Tools for Initial Assessment, Full Assessment, and Re-assessment |
|---|
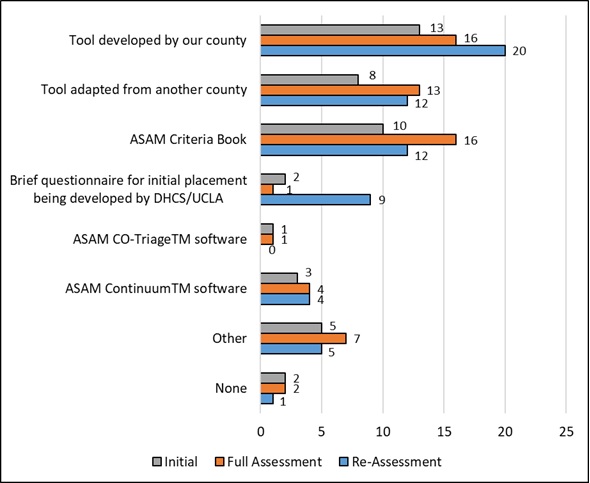 |
| SOURCE: California's Drug Medi-Cal Organized Delivery System 2018 Evaluation report. |
Across states, there is similar variability in the level of standardization of ASAM-based assessments. Massachusetts, Maryland, and Virginia require the use of the ASAM Criteria, but they do not specify a standardized assessment tool. Florida is starting to use the ASAM Continuum software and assessment tool, and Pennsylvania uses the Treatment Assignment Protocol (TAP), which is a structured protocol that helps providers gather information related to the ASAM Six Dimensions.
From our discussions, Maryland is the only state in which all public and private payers require the use of the ASAM Criteria, despite variability in precisely how they use the criteria. The state has recently passed a bill making this a requirement, and approaches to ensuring adoption and compliance have yet to be established.
Some years ago, the State of Virginia tried to implement the use of the ASI among their Community Service Boards (CSBs). However, there was significant pushback from the providers, who wanted to be able to do their own assessments and thought the ASI took too long to administer. Still, Virginia requires the use of the ASAM Criteria, and is starting to require the use of the Daily Living Activities-20 measurement tool in their CSBs in order to better track improvement in outcomes across the different levels of care.
For several years, Pennsylvania had their own placement criteria; however, when the state received a SUD 1115 waiver, they decided to switch to the use of the ASAM Criteria. The state now requires the TAP, which allows providers to gather the information necessary to make a placement recommendation. Reasons for switching were that the TAP seemed to be better suited for individualized care and it included a detailed assessment of the need for medication assisted treatment. Currently, to better align and overlap with the GPRA data collection tool that providers are also required to use, Pennsylvania's substance abuse division is considering switching their placement tool to use the ASI-Lite instead of the TAP. The ASI-Lite is a shortened version of the ASI and would still allow providers to gather information regarding the ASAM Criteria.
In Florida, the ASAM Continuum was viewedas the industry standard for patient placement assessment, and so the state recently used State Opioid Response funds to purchase about 4,000 licenses to the ASAM Continuum software. The state also purchased access to the Web Infrastructure Treatment System (WITS), which will store summary results from the ASAM Continuum assessments and information on other SUD treatment practices and patient outcomes.
Of the states spoken with for this project, only New York and Missouri do not require the ASAM Criteria. New York uses an alternative to the ASAM Criteria, and Missouri does not have any required placement criteria, although the state does set forth guidelines for core domains that should be discussed and included in the biopsychosocial assessment that providers choose. New York has required the use of the LOCADTR tool for several years (OASAS, n.d.). There are some similarities to the ASAM Criteria, but some differences as well--for example, it does not assess a patient's readiness to change, because the developers of the tool did not see this as crucial to determining the level of care. For this, New York developed their own tool, because they wanted something that was short, not proprietary, standardized, and tailored based on input from local providers. Researchers at Columbia University developed the tool and tested its reliability and validity (O'Grady, et al., 2018).
Some SMEs mentioned a biopsychosocial assessment known as the Global Appraisal of Individual Needs (GAIN) interview, which is owned by Chestnut Health Systems. Even though none of the states with which we had discussions required the GAIN-I (one of three GAIN tools), SUD providers across the country use it for diagnosis, placement, and treatment planning (Exhibit 4). It asks questions related to the ASAM Six Dimensions. There also shorter GAIN instruments that can be used throughout treatment pathways--such as the GAIN Quick, which takes about 20 minutes and is good for brief interventions and referrals, or the GAIN Short Screener, which takes only a few minutes and is good for an initial understanding of the severity of the problem. The GAIN assessment tools started in 1993, and as of the end of 2018, there were approximately 350,000 GAIN-I records and 900,000 GAIN assessments altogether (GAIN, 2019).
| EXHIBIT 4. Total Number of GAIN Sites by State in the U.S. Since 1993 |
|---|
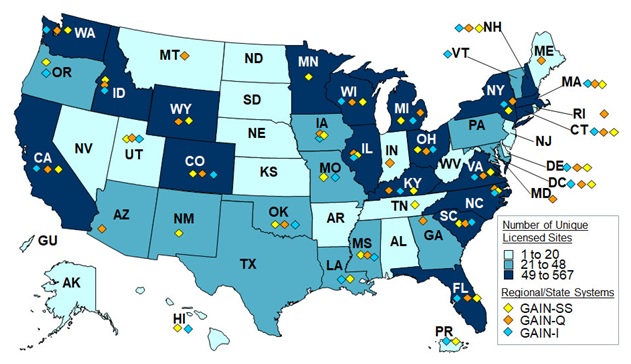 |
| SOURCE: http://gaincc.org/usa/. Accessed on July 15, 2019. NOTE: The number of sites represents GAIN licenses for GAIN-I/M90, GAIN Quick/Q3, and GAIN Short Screener (SS). |
3.1.4. Who Administers the Assessments and How are They Trained?
Which provider administers the assessment depends on the setting. In a specialty outpatient setting, the outpatient provider typically administers the needs assessment. For higher levels of care, this depends on the facility and their available staff. The person conducting the intake assessment may be a clinician who specializes in assessments, a master's or PhD psychologist, a social worker, a counselor, a nurse, a mid-level medical practitioner (e.g., a physician's assistant), or a medical doctor. Most SMEs and state stakeholders did not mention any restrictions on the type of provider. Pennsylvania was the only state that requires whoever administers the assessment to have received the ASAM training offered throughout the state. Other states offered, but did not require, training to help establish some level of consistency in how placement criteria are usedby various types of providers.
Train for Change, which is a part of the Change Companies, is the most widely used company for standardized ASAM Criteria training. They offer various training opportunities such as a 2-day in-person introductory training, supplemental online training, training on how to use motivational interviewing with the ASAM Criteria, and an implementation leader training. Pennsylvania has worked with Train for Change to offer ASAM Criteria training to approximately 7,000 providers and Virginia has worked with the company to train approximately 700 providers. In offering these trainings, the states found that there was a high demand and interest for training. The states tracked who received the training but there was no credentialing or certification process as a result of the training.
Other states and organizations have taken different approaches to training. Massachusetts offers an online training on the ASAM Criteria that is available to publicly-fundedproviders. Florida has offered presentations and webinars on the use of the ASAM Continuum as they work to make the tool available for up to 4,000 providers across the state. There are also less formal approaches to training. Intermountain Health uses a mentorship approach in which someone who is experienced with the ASAM Criteria trains new providers. SMEs noted that sometimes the ASAM Criteria Book is the only training that some providers receive.
Training can help improve the standardization of the assessments and adherence to established criteria and guidelines, but it can be very costly for states to offer high quality training to a substantial number of providers. Stakeholders in Maryland mentioned that it was difficult to provide training because it is an ongoing need due to staff turnover. The stakeholders who discussed their training efforts have used a blend of both state and federal dollars to help pay for training. Some states have drawn from the influx of opioid-related funds to help pay for training and changes to their SUD system of care. Despite these efforts to increase availability of training, the variability in how providers are trained across and within states can impact the standardization and comparability of assessments, even among states that use the same general criteria.
3.2. How could Data from Recorded Assessments be Obtained for Analysis?
Recorded assessments through third-party databases--specifically the GAIN database, the repository of ASAM Continuum responses, and the WITS system--provide the most accessible data. These databases are somewhat limited in scope but are growing in size. However, privacy concerns remain, even when the data are de-identified and used for aggregate reports. This has prevented some organizations from allowing their data to be used for research purposes.
3.2.1. Where are the Data Recorded and Who are They Shared With?
The results of needs assessments are recorded in three general areas: third-party databases specific to certain assessment tools, EHRs, and with MCOs prior authorization records.
Stakeholder discussions indicated there are three types of third-party databases that store information for multiple organizations or states. First, GAIN assessments are stored in a central database maintained by Chestnut Health Systems. As mentioned earlier, there are over 900,000 GAIN assessments and screeners captured in that database. Second, the ASAM Continuum database is maintained by ASAM and includes about 70,000 records, with approximately 5,000 records being added monthly. The third and largest database of standardized placement assessments is maintainedwithin the Health Commerce System in New York and houses approximately 1.8 million LOCADTR assessments.
Some states use the same centralized EHR system to store their assessment results. Many of these health records are stored within siloed databases; however, the WITS system run by FEI Systems is a web-based system that stores all the information centrally. It is used by 33 state and county substance abuse departments across the country. Within this system, summary results from standardized assessment tools like the GAIN and ASAM Continuum may be recorded. Regardless of the tool or criteria, many states use the WITS to record the recommended level of care, any clinical overrides for the recommended level of care, and the reason for the clinical override. The WITS system is the only database of its kind that is used across so many states and collects placement assessment results as well as information on a client's treatment pathways and outcomes.
MCOs that oversee the prior authorization of SUD services are likely to centrally store data on needs assessments. In some cases, MCOs have more detailed data than the state departments. For example, Virginia's Medicaid program requires the use of an Addiction Recovery Treatment Services (ARTS) Service Authorization Review Form which details a client's information regarding the ASAM Six Dimensions and the reasons for recommending a certain level of care. These forms are gathered and reviewed by the MCOs within the state; however, the detailed information is not shared with the state or used to examine the needs across different levels of care. Maryland also has a system of care in which they contract with Beacon Health Options to manage all SUD services. Beacon receives detailed client information that provides evidence and support for a recommended level of care, but the state only sees what level of care was recommended and what was received.
3.2.2. How Accessible are the Data?
There are varying levels of accessibility regarding the assessment data that are recorded. Chestnut Health Systems has created a publicly available database of GAIN intake and follow-up assessments from 2002 through 2012. They are in the process of developing a more expansive database covering the period 2002 to 2018, which should be available in early 2020 and include about 320,000 initial full assessments and 90,000 follow-up assessments.
As the ASAM Continuum database grows, ASAM has begun to develop a repository of recorded outcomes for research purposes. They are seeking approval from their clients to use de-identified responses to the ASAM Continuum to better study outcomes and patterns of responses. It is unclear at this point how accessible this database will be to the public.
Access to assessment data really depends on the willingness of the states to share it for research or evaluation purposes. This may be influenced by federal incentive programs and requirements in conjunction with Medicaid demonstrations. State stakeholders in New York said that they did not think the LOCADTR database would be made accessible to those outside of the state government and its contractors who are using the data to evaluate needs and outcomes within the state. Though the WITS database of EHRs is quite comprehensive and far-reaching, it would only be accessible with the approval of the states and counties who own the data. In our discussions, stakeholders in both Florida and Pennsylvania said they might consider sharing data from their WITS system given the proper approvals and de-identification of the data.
3.2.3. What are the Strengths and Limitations of the GAIN, ASAM Continuum, and WITS Databases?
A major strength of the GAIN database[3] is that it includes rich clinical detail on clients at baseline and at 3 and 6 months after intake. For the intake assessment, several questions are asked that pertain to each of the six ASAM dimensions. A 7-point severity scale is also recorded for each of the six dimensions. Information is also recorded regarding the client's SUD treatment history, involvement with the criminal justice system, past 90-day health care expenditures, employment challenges, physical health problems, and cognitive impairment.
A major limitation to the GAIN is that the recommended level of care is not recorded in any of the GAIN assessment data. The received level of care is recorded, but only among the approximately 25% of clients who remain in treatment and for whom 3-month follow-up assessment data are available. Moreover, data on the level of care is limited to the number of nights in residential treatment, days in intensive outpatient treatment, outpatient program visits, and days that any medications such as methadone were received to help with withdrawal symptoms. The data do not include further detail such as the type of medication received (e.g., buprenorphine vs. methadone) or the intensity of residential services.
Additionally, the GAIN has a limited scope of participating organizations. Many organizations have used SAMHSA grants to fund their use of the GAIN. Many of these grant programs focus on a specific population or setting such as adolescents or drug courts. As a result, the participating client population may not be generalizable to all those receiving SUD treatment. To have a more generalizable group of SUD clients, researchers using the GAIN database may want to restrict their analyses to regional projects--that is, where a county department, state department, or private treatment facility spanning multiple locations has decided to independently fund the use of the GAIN with its clients. In the 2002-2013 database, there were only eight regional projects. In the forthcoming 2002-2018 database, there will be many more regional projects included, although the final number is not yet known to us.
The main advantage of the ASAM Continuum database is its rich detail across all six ASAM dimensions. It includes data on whether the provider overrides the recommended level of care for reasons such as the availability of local treatment resources, clinical judgement, or the preferences of the client. The database also captures longitudinal outcomes with multiple assessments for the same individual over time.
Accessibility is a major challenge with the ASAM Continuum database. The ASAM Continuum questions and the algorithm for determining a recommended level of care are proprietary. ASAM does not want the questions to be replicated or the algorithm to be reverse engineered and used elsewhere. Despite this limitation in public accessibility, select researchers within ASAM could potentially examine the distribution of needs by level of care using this dataset.
The WITS has two main advantages: its clinical detail and its size in terms of the number of encounters captured. In addition to intake screening and assessment results, the WITS captures details regarding client outcome measures, diagnoses, program enrollment, treatment plans, services delivered, payor adjudication for those services, referrals to additional services, and discharges. The extent to which these elements are recorded varies by participating organization. There are over 1.7 million encounters where a client's recommended level of care was recorded as well as the client's county of residence. These data can potentially be used to understand geospatial patterns in the need for different SUD levels of care. There are also over 130,000 encounter records where there was a reason for a provider override of the recommended level of care.
The distributions of the client's recommended levels of care vary substantially across participating organizations within the WITS, and it may not be possible to use the data to identify the major reasons for this variation. The variation could be because organizations cover different levels of care, focus on different target populations, or differ in governance structure. Additionally, different assessment tools for determining a recommended level of care are used within and across the organizations. The ASAM criteria may not be reliably and consistently used across the participating organizations to allow for a consistent picture of needs by SUD level of care.
3.2.4. What are the Privacy Concerns?
There are limitations regarding the use of client's data as outlined in the 42 CFR Part 2 law. SMEs said that this law should not preclude the use and analysis of de-identified data that is reportedat an aggregate level. Despite aggregating results and de-identifying responses, some states have been reluctant, for example, to share their data with the ASAM Continuum repository. A similar reluctance to share data would be expected if someone were to try to use the data collected within the WITS system across several states.
3.3. How have States and Organizations Analyzed the Data?
States have not done many analyses of needs by level of care. Some states have looked at, or are planning to look at, needs assessments and outcomes by level of care in their evaluation reports for Medicaid SUD 1115 demonstrations. California, which was the first state to implement a SUD demonstration, has already published several evaluation reports (UCLA-ISAP, 2019). Despite variations in specific assessment tools, levels of care recommendations are being gathered and examined in California. The state's 2018 evaluation report provides the percentage of patients served by different levels of care and the levels of care that counties reported as being most challenging to expand. Exhibit 5 below shows data regarding the reasons for clinical overrides, or when there was a difference between the recommended level of care using ASAM Criteria and the placement decision. Note that although the "level of care not available" was not the most commonreason, it still was listed 21% of the time with clinical overrides, which may indicate the need to expand services in some areas of California.
| EXHIBIT 5. Reasons for Difference between Indicated Level of Care and Placement Decision |
|---|
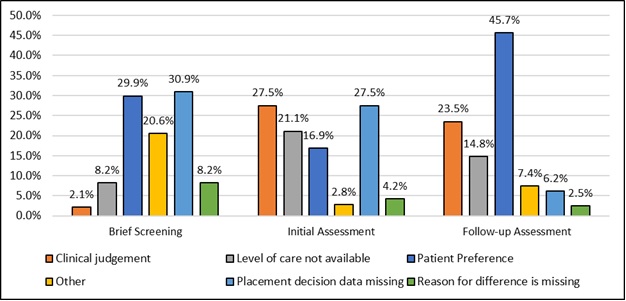 |
| SOURCE: California's Drug Medi-Cal Organized Delivery System 2018 Evaluation report. |
In the absence of needs assessment data in Virginia, the state has examined treatment needs by determining what levels of care are geographically inaccessible. Virginia's 2018 Annual Report for their SUD 1115 demonstration provides maps for each level of care offered in the state (VA DMAS, 2019). Exhibit 6 shows office-based opioid treatment programs in the state and provides insight into the regions where such treatment is inaccessible, and thus needed. Other maps in the 2018 Annual Report showed particular need for partial hospitalization and residential services due to inaccessibility in many regions of the state.
| EXHIBIT 6. Accessibility of Office-based Opioid Treatment Programs in Virginia |
|---|
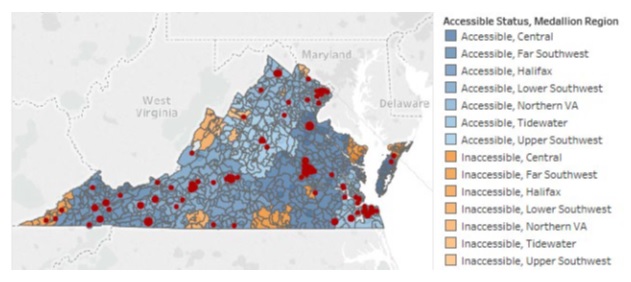 |
| SOURCE: The Virginia Governor's Access Plan (GAP), Addiction and Recovery Treatment Services (ARTS), and Former Foster Care Youth (FFCY) Delivery System Transfiguration Section 115 Annual Report, 2018. |
To understand need by level of care, Massachusetts is examining the patient waitlists for different services. Several states have also used medical claims to examine utilization by level of care and transitions between levels of care. New York is just starting to link information from their LOCADTR database with their claims database to examine outcomes by level of care recommendation; however, these analyses are not yet publicly available. Internally, Maryland used claims analyses to examine utilization by level of care and initiation of medication assistedtreatment following an assessment.
Given that Medicaid SUD 1115demonstrations require the use of evidence-based placement criteria and reporting (CMS, n.d.), we anticipate more analyses by level of care to be published as additional states begin submitting their monitoring and evaluation reports.
3.4. What Other Analyses could be Conducted with the Data?
SMEs shared that analyzing needs assessment data by level of care could help with capacity planning. For example, in Virginia, if the assessment data were collected from the ARTS Service Authorization Review Forms that are submitted to the MCOs, then the need for different services could be mapped out by county and overlaid with their maps of treatment accessibility across the state. These combined maps could then indicate areas with high need and low availability of certain levels of care. California could use their data on the reasons for clinical overrides of placement recommendations to generate a map of clients who did not receive the recommended level of care because it was not available locally. Additionally, proper capacity planning helps to ensure network adequacy. The levels of care available within a health plan could be compared to the assessed need for SUD levels of care among clients within that health plan.
As more providers and organizations begin to use the ASAM Continuum, the data gleaned from this database could help to generate many reports and analyses. One suggestion was made to establish a panel that could direct the development of some standardized reports using the ASAM Continuum data.
In addition, stakeholders from some states shared lists of other potential analyses that they are interested in doing with the data they have collected about the level of care recommendations and received services (Exhibit 7). Some common themes were examining the timeliness of entering treatment, the transitions between levels of care, and how receiving certain services and levels of care impact patient outcomes.
A state or multi-state assessment of needs by level of care may be limited by the scope of the data or the population of patients who received the assessments. For example, the TAP assessments recorded in the WITS system within Pennsylvania are doneamong patients who are primarily underinsured or uninsured and are receiving care through the county health system. Though TAP assessments result in a rich understanding of needs, it would not be very representative of all SUD needs across the state. Also, although the ASAM Continuum is being used by different providers across several states, participating providers may not be representative of other SUD providers throughout the states (with the potential exception of Florida, where it is being offered statewide).
| EXHIBIT 7. Types of Analyses State Stakeholders Expressed as Being Useful | ||
|---|---|---|
| California | Massachusetts | Pennsylvania |
|
|
|
Some states are limited by a lack of available resources to run analyses by level of care. Stakeholders in Virginia particularly mentioned this challenge, noting that they have limited staffing and limited time to perform analyses. They work with some third-party organizations to help conduct evaluations, but there are several additional analyses that state stakeholders would like to do but do not have the time or resources to carry out.
Additionally, many of the changes to assessments procedures and data collection are just starting to take place, and the changes are still too recent to analyze and evaluate. For example, Florida is just starting to make available the ASAM Continuum, and the state does not yet have much data collected. Pennsylvania has been implementing changes over the past year, and now they are finally starting to have the time and sufficient numbers of assessments to evaluate outcomes using their data. Some assessment and data collections activities need more time to mature before they can be used in analyses of need by level of care.
4. DISCUSSION OF FEASIBILITY
Through discussions with SMEs, state stakeholders and treatment organizations, we identified several challenges to the feasibility of gathering and using data regarding SUD needs by level of care:
-
Assessments, provider trainings, and definitions of levels of care are not consistent across states and private payers.
-
Some of the assessments may be biased and may reflect where individuals are seeking and receiving care rather than their true need for a level of care.
-
Data collection systems for assessment data are fragmented.
-
Among states and organizations that collect assessment data, there are privacy concerns and fears of sharing the data even when it is de-identified and would be used for aggregate reports.
-
Collected data may be limited in scope and may not provide a comprehensive picture of SUD needs by level of care.
Despite these challenges, there are some data sources that can be used to assess the distribution of SUD needs by level of care. These are the GAIN database, the ASAM Continuum repository, and the WITS system. The GAIN database is the most accessible resource; however, the dataset does not distinguish between the level of care received and the level of care recommended. It does provide rich information concerning the characteristics of clients across the six ASAM dimensions. The ASAM Continuum repository is smaller than the GAIN, but is growing rapidly and is viewed as the industry standard for assessing and recording a client's need by level of care using the ASAM Criteria. The WITS system is used across the country and often collects outcomes from whatever needs assessments are used within participating states; however, in order to access the data and conduct a multi-state analyses of needs by level of care, states would need to provide their approval to access and analyze the data.
Working with parent firms of MCOs may be another approach to collecting and analyzing needs assessment data by level of care across multiple states. The MCOs already collect information necessary for prior authorization by level of care. The severity of patients' conditions across different domains of life could be examined by levels of care. This would also allow for a study of the most common reasons why a level of care is not authorized. One limitation to these data, however, is that they may indicate the utilization of treatment rather than the need for a specific level of care.
Finally, new data collection efforts could be designed to help individuals make informed decisions about their treatment and to gather information nationally on SUD needs by level of care. One possibility would be to create a free online placement assessment screeningtool, similar to those used with telephone access lines, that takes 5-10 minutes to fill out and results in a provisional level of care recommendation. If this platform were widely used, it could allow for estimates of need by general levels of care throughout the country. It could also potentially be integrated with the SAMHSA helpline or the SAMHSA treatment locator, so that individuals could first figure out the most appropriate level of care for themselves and then identify a local treatment facility that offers that level of care.
REFERENCES
American Society of Addiction Medicine (ASAM). (2019a). Level of Care Certification FAQs. [web page].
American Society of Addiction Medicine (ASAM). (2019b). What is the ASAM Criteria? [web page].
Andrilla, C.H.A., Moore, T.E., Patterson, D.G., Larson, E.H. (2019). Geographic distribution of providers with a DEA waiver to prescribe buprenorphine for the treatment of opioid use disorder: A 5-year update. Journal of Rural Health, 35, 108-112.
Centers for Medicare & Medicaid Services. (n.d.). Monitoring Metrics for Section 1115 Demonstrations with SUD Policies. https://www.medicaid.gov/medicaid/section-1115-demo/downloads/evaluation-reports/sud-monitoring-metrics.pdf.
Global Appraisal of Individual Needs (GAIN) Coordinating Center. (2019). GAIN by the Numbers. [web page].
Jones, C.M., Campopiano, M., Baldwin, G., McCance-Katz, E. (2015). National and state treatment need and capacity for opioid agonist medication-assisted treatment. American Journal for Public Health, 105, e55-e63. doi:10.2105/AJPH.2015.302664.
Kolsky, G.D. (2006). Current State AOD Agency Practices Regarding the Use of Patient Placement Criteria (PPC)--An Update. https://nasadad.org/nasadad-reports/. Accessed July 18, 2019.
New York State Office of Alcoholism and Substance Abuse Services (OASAS). (n.d.). Level of Care for Alcohol and Drug Treatment Referral (LOCADTR) and LOCADTR for Gambling Treatment. [web page].
O'Grady, M.A., Neighbors, C.J., Lincourt, P., Burke, C., Maldonado, A. (2018). Development and testing of an addiction treatment level of care determination tool. Journal of Behavioral Health Services & Research, 1-9. doi:10.1007/s11414-018-9623-x.
Sowers, W., George, C., Thompson, K. (1999). Level of care utilization system for psychiatric and addiction services (LOCUS): A preliminary assessment of reliability and validity. Community Mental Health Journal, 35, 545-563.
Stallvik, M., Gastfriend, D.R., Nordahl, H.M. (2015). Matching patients with substance use disorder to optimal level of care with ASAM Criteria software. Journal of Substance Use, 20, 389-398.
Substance Abuse and Mental Health Services Administration (SAMHSA). National Survey of Substance Abuse Treatment Services (N-SSATS). [web page].
Substance Abuse and Mental Health Services Administration (SAMHSA). (2018). Key Substance Use and Mental Health Indicators in the United States: Results from the 2017 National Survey on Drug Use and Health. (HHS Publication No. SMA 18-5068, NSDUH Series H-53). Rockville, MD: Center for Behavioral Health Statistics and Quality, SAMHSA. Retrieved from https://www.samhsa.gov/data/.
University of California Los Angeles, Integrated Substance Abuse Programs (UCLA-ISAP). (2019). California DMC-ODS Evaluation: Evaluation Reports and Presentations. [web page] http://www.uclaisap.org/dmc-ods-eval/html/reports-presentations.html.
Virginia Department of Medical Assistance Services (DMAS). (2019). The Virginia Governor's Access Plan (GAP), Addiction and Recovery Treatment Services (ARTS), and Former Foster Care Youth (FFCY) Delivery System Transformation: Section 1115 Annual Report Demonstration Year 4. https://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Waivers/1115/downloads/va/Governors-Access-Plan-GAP/va-gov-access-plan-annl-rpt-2018.pdf.
APPENDIX A. SEARCH TERMS USED FOR THE ENVIRONMENTAL SCAN
Below is a list of many of the search terms that were used in the environmental scan:
Google, Bing Searches*
-
States use of ASAM criteria
-
1115 SUD Waivers
-
Virginia ARTS provider credentialing checklist
-
Virginia ARTS uniform services review request form
-
Blue Cross Blue Shield use of ASAM criteria
-
New York Level of Care for Alcohol and Drug Treatment Referral (LOCADTR)
-
ASAM Continuum
-
Pennsylvania substance user's patient placement criteria
-
Kaiser Permanente addiction research placement criteria
-
Intermountain Healthcare addiction placement criteria
-
Beacon Behavioral health placement criteria
-
Florida ASAM Placement
-
ASAM assessment in FQHC
-
ASAM Performance Measures
-
Substance use disorder telephone access line, Virginia
Pub Med, Google Scholar Searches*
-
("placement criteria" or "ASAM criteria" or "needs assessment") and ("substance use disorder" or addiction or abuse or dependence) and state
-
ASAM Needs assessment
-
(((American Society of Addiction Medicine) AND Criteria) AND addiction) AND state
-
(((("American Society of Addiction Medicine") AND "needs Assessment") OR "Placement Criteria") OR "1115 SUD Waiver")
-
((("placement criteria" or "asam criteria" or "needs assessment") and ("substance use disorder" or addiction or abuse or dependence) and state)) AND addiction, substance[MeSH Terms]
* These search terms are not an exhaustive list; rather they are examples of what was usedto identify relevant literature. In addition to search engines, we utilized a snowball approach by examining 'references' and 'related article' sections to identify additional documents and publications relevant to the research questions.
APPENDIX B. SUBJECT MATTER EXPERTS AND REASONS FOR SELECTION
The table below outlines what subject matter experts (SMEs) were spoken with and the original reasons for their selection.
| EXHIBIT B-1. SMEs, Their Affiliation, and the Reason for Selecting Them to Participate in this Study | |
|---|---|
| SME and Affiliation | Reason for Selection |
| Tyler Sadwith (Technical Assistance Collaborative) | He served as the project lead for the SUD track of the Medicaid Innovation Accelerator Program and is very aware of the state SUD 1115 demonstrations and how different states are using the ASAM criteria. |
| Rick Harwood (NASADAD) | He is well connected with State Alcohol and Drug Abuse Directors and is aware of their use of needs assessments and placement criteria. He could direct us to states that would be good for future discussions. |
| Marion Haas & Sarah Moore (FEI Systems) | They were recommended by Rick Harwood as an organization that operates WITS, a web-based application that is designed to capture client services data. |
| Mady Chalk (The Chalk Group) | She was recommended by the ASPE Project Lead. She has been an expert consultant on developing ASAM performance and quality measures. She is an expert in the field of screening for SUDs. |
| David Gastfriend (ASAM) | He was the chief architect of the ASAM Continuum and could speak to its use across organizations and states. |
| Kathryn Modisette (Chestnut Health Systems) | She was chosen because she could speak about the GAIN, a biopsychosocial assessment tool for SUD treatment needs, and she could speak about the databases of GAIN responses. |
| Janice Pringle (University of Pittsburgh) | She is at the University of Pittsburgh and has directed the Pennsylvania SBIRT program. She is well connected to addiction treatment centers in the state and could speak to changes that are taking place regarding the use of ASAM criteria. |
| Debbie Scovill (Intermountain Healthcare) | She is the SUD Coordinator at Intermountain Healthcare and could provide a clinical perspective on how needs assessments are done within a large organization that functions independently from the states where it functions. |
| Alyssa Forcehimes (Train for Change) | She could speak to the training that is done across the country regarding the ASAM criteria. Her company has worked with different states to help train providers. |
APPENDIX C. SUBJECT MATTER EXPERT DISCUSSION GUIDE
Discussions with subject matter experts followed the general protocol outlined below:
-
Introduce those on the call and introduce the purpose of the study: to determine the feasibility of using recorded SUD needs assessments (e.g., intake assessments or placement assessments) to understand the distribution of need by level of care, so that state and federal governments can ensure there are enough resources allocated to each of these levels of care for SUD.
-
Ask: How are SUD needs assessments administered and recorded across organizations and states? This question is related to the second research question in the scope of work and is to better understand the context of collecting needs assessment data and the variability in this process across organizations and states. Below are potential follow-up questions:
-
Who administers the assessment?
-
Who is assessed? Is it only for those entering residential settings?
-
When are they assessed?
-
What information must be recorded? Is there a standardized approach?
-
How is the recorded information stored?
-
Who is the recorded information shared with?
-
-
Ask: How can recorded needs assessment data be obtained for aggregate analyses regarding the distribution of SUD needs by level of care? This is related to the first research question in the statement of work. Below are potential follow-up questions:
-
If needs assessment data are not stored centrally, what are ways to gather the data?
-
How could data from different types of needs assessments be combined?
-
When data are stored centrally, what is the protocol for accessing and analyzing them?
-
What are the privacy concerns and how could these concerns be addressed?
-
-
Ask: Are you aware of states or organizations that collect and analyze their needs assessment data? If so, what have been the findings? This is related to the third research question in the statement of work.
-
Ask: How helpful do you think it would be to have aggregated needs assessment or placement assessment data at a state or national level? This is related to the fourth research question in the statement of work, which pertains to the conclusions that could be drawn from collecting and assessing needs assessment data. Below are potential follow-up questions:
-
What conclusions could be madeabout the distribution of SUD needs, SUD treatment gaps, or SUD capacity planning in the general population?
-
What additional information could be understood from needs assessment data that is not already understood from current state or national surveillance efforts?
-
Could needs assessment data be gathered at a national scale? If so, what would be required to do that and who might be included in the final sample?
-
What are the limitations of the needs assessment data?
-
-
Ask about states we should target in our analysis and other SMEs that we should speak with to learn more about this topic.
APPENDIX D. STATE DISCUSSION GUIDE
Discussions with state stakeholders followed a semi-structured format. We used the general protocol outlined below, but additional questions were tailored to each discussion:
-
Introduce those on the call and introduce the purpose of the study: to determine the feasibility of using recorded SUD placement and intake assessments to understand the distribution of need by level of care.
-
Ask: How are SUD placement assessments administered and recorded in your state or county? (This question is related to the second research question in the scope of work and is to better understand the context of collecting needs assessment data and the variability in this process across organizations and states.) Below are potential follow-up questions:
-
How does an individual enter specialty care for SUD, and at what point in this entry process are they administered a placement assessment?
-
Who administers the placement assessment?
-
What information must be recorded? Is there a standardized approach?
-
How is the recorded information stored?
-
Who is the recorded information shared with?
-
How does the state verify the assessment is done correctly? Does this verification vary by the level of care of the treatment facility?
-
How and when are placement assessments re-administered?
-
-
Ask: How can recorded needs assessment data be obtained for aggregate analyses regarding the distribution of SUD needs by level of care within the state or county? (This is related to the first research question in the statement of work.) Below are potential follow-up questions:
-
If needs assessment data are not stored centrally within the state, what are potential ways to gather the data?
-
How could data from different types of needs assessments be combined?
-
When data are stored centrally, what is the protocol for accessing and analyzing them?
-
What are the privacy concerns and how could these concerns be addressed?
-
-
Ask: How has your state or county collected and analyzed placement and intake assessment data? (This is related to the third research question in the statement of work.) If the state or county has not collected or analyzed the data, then ask the following:
-
What data do you think are feasible to collect?
-
What analyses might you perform with the data?
-
-
Ask: How helpful do you think it would be to have aggregated placement or intake assessment data at a county, state, or national level? (This is related to the fourth research question in the statement of work, which pertains to the conclusions that could be drawn from collecting and assessing needs assessment data.) Below are potential follow-up questions:
-
What conclusions could be madeabout the distribution of SUD needs, SUD treatment gaps, or SUD capacity planning in the general population?
-
What additional information could be understood from placement and intake assessment data that is not already understood from current county, state or national surveillance efforts?
-
What are the limitations of the placement and intake assessment data?
-
-
Thank the person for participating in the discussion.
APPENDIX E. HISTORY AND EVIDENCE REGARDING PLACEMENT ASSESSMENTS
A regular part of clinical care is identifying the severity of needs and directing patients to the treatments that best help them address those needs. This process became much more standardizedfor SUD services with the increased involvement of MCOs in the 1980s. These MCOs identified situations where patients were receiving much more care and a higher intensity of care than was necessary, and so they started to develop tools and guidelines to help save costs by directing patients into levels of care that better matched needs with resources. States often developed their own criteria for placing individuals into an appropriate level of care.
As the value of placementassessments became more evident, national tools and guidelines were established and developed. One of the first national set of guidelines, or patient placement criteria, was established in the private sector by ASAM and the National Association of Addiction Treatment Providers (ASAM, 2019). As these criteria became more widespread in the private industry, some states also began to adopt the ASAM criteria. The Addiction Severity Index (ASI) was also a tool that was developed in the 1980s and became widely used by providers and states for assessing the SUD needs of individuals (McLellan, et al., 1980). The ASI was a semi-structured assessment tool, whereas the ASAM criteria was more flexible in what was askedas long as it focused on six main dimensions of an individual's life. Both overlapped in general content areas for determining the appropriate level of care of a patient. Despite these national tools and guidelines, many states still used their own tools and approaches that had been tailored to the resources and levels of care offered within their own state.
Different studies have been done to further support the use of these widespread patient placement criteria and assessments. These typically have focused on the outcomes for those whose treatment matched what was recommended compared to those whose treatment mismatched what was recommended in the placement assessment. One study found that patients receiving a lower level of care than what was recommended had significantly more hospital bed-days in the following year (Sharon, et al., 2003). Another study among patients with an alcohol use disorder found that people receiving outpatient services when intensive outpatient was recommended had poorer drinking outcomes at 3 months compared to those whose treatment matched what was recommended (Magura, et al., 2003). This study also found that overmatching, or providing a level of care higher than what is recommended, was not related to improved outcomes. A third study examined matching among those with addiction and a psychiatric comorbidity and found that both undermatching and overmatching increased no-show rates for treatment in this population (Angarita, et al., 2007). Finally, a more recent study that validated the ASAM Criteria software tool or ASAM Continuum, found that matched patients had both better treatment retention and lower drug use at follow-up (Stallvik, Gastfriend, & Nordahl, 2015).
Even though these studies have shown that matching to the appropriate level of care can have some impact on outcomes, there are important limitations to this evidence. One is that these studies all focused on general levels of care and do not provide evidence yet that there is value in distinguishing between sublevels of care (e.g., providing Level 3.1 vs Level 3.5 or residential services). There also may be unadjusted differences in the patients' characteristics and preferences that drive the differences in outcomes for those that receive mismatched care. The outcomes may be very different for a patient who is willing to receive a level of care but the treatment is not available compared to when a patient prefers a lower level of care. More research can and should be done in this area.
References
American Society of Addiction Medicine (ASAM). (2019). What is the ASAM Criteria? [web page].
McLellan, A.T., Luborsky, L., Woody, G.E., O'Brien, C.P. (1980). An improved diagnostic evaluation instrument for substance abuse patients: The Addiction Severity Index. Journal of Nervous and Mental Disease, 168, 26-33. doi:10.1097/00005053-198001000-00006.
Sharon, E., Krebs, C., Turner, W., Desai, N., Binus, G., Penk, W., & Gastfriend, D.R. (2003). Predictive validity of the ASAM Patient Placement Criteria for hospital utilization. Journal of Addictive Diseases, 22, 79-93.
Magura, S., Staines, G., Kosanke, N., Rosenblum, A., Foote, J., DeLuca, A., Bali, P. (2003). Predictive validity of the ASAM Patient Placement Criteria for naturalistically matched vs. mismatched alcoholism patients. American Journal on Addictions, 12, 386-397.
Angarita, G.A., Reif, S., Pirard, S., Lee, S., Sharon, E., Gastfriend, D.R. (2007). No-show for treatment in substance abuse patients with comorbid symptomatology: Validity results from a controlled trial of the ASAM Patient Placement Criteria. Journal of Addiction Medicine, 1, 79-87.
Stallvik, M., Gastfriend, D.R., Nordahl, H.M. (2015). Matching patients with substance use disorder to optimal level of care with ASAM Criteria software. Journal of Substance Use, 20, 389-398.
APPENDIX F. PATHWAYS INTO SUBSTANCE USE DISORDER TREATMENT
SMEs and state stakeholders described five general pathways into SUD treatment that impacted when and how needs assessments were done. First, individuals may enter treatment through a screening and referral process. Some primary care facilities regularly do screening, brief intervention, and referral to treatment (SBIRT). This process will identify need for specialized SUD treatment, but it is not designed to direct an individual to a specific level of care. State stakeholders shared that a pilot study was recently donein Massachusetts to explore how the ASAM CO-Triage could be used within Federally Qualified Health Centers to expand on SBIRT and refer people to a provisional level of care. The results have not yet been published.
Second, with more states receiving SUD 1115 waivers to expand Medicaid coverage of SUD services, many are also offering telephone access lines to help direct patients to available and appropriate levels of care. Some people's pathway into treatment involves these access lines. They are typically available 24/7 and involve lay personnel with some training or experience around SUD services. The extent of screening done through these access lines varies widely between and within states. In Pennsylvaniathey use a standardized screener that assesses whether an individual has any immediate crises that should be addressed. Counties that do contract with SUD providers and do not directly offer services typically do not do screening on the access line. Some access lines in California use standardized screening tools that even determine a provisional level of care recommendation; however, they vary widely in length and content ranging from 5 minutes to 30 minutes long. They are working with researchers at the University of California Los Angeles (UCLA) to develop a standardized screening tool that could be available to county access lines across the state. Many other states do not have any formal screener that is used as a part of their telephone access line.
Third, in addition to access lines some states have a centralized intake system for people seeking to enter SUD services. The intake centers conduct an initial assessment and then direct people to the appropriate level of care for treatment. New Hampshire has a program they call The Doorway which has centers throughout the state that do needs assessment, help people start on treatment, and connect people to an appropriate level of care for further SUD treatment (NH DHHS, 2019). Florida also mentioned that they have a central receiving system in which they use CO-Triage to place individuals into a provisional level of care. Missouri tried a central intake process many years ago, but they found that many people did not make the transition from the central intake and assessment process to the treatment facility and so they discontinued that practice.
Fourth, another pathway into treatment is a result of accidents, injury, or involvement with the criminal justice system. Accidents or injuries requiring medical attention that occurred while under the influence of drugs may prompt providers to refer patients to specialized treatment. In Missouri, a treatment-first approach is being implemented so that patients visiting the emergency department for an opioid use disorder will be helped into medication assistedtreatment ideally within 24 hours of discharge regardless of a placement assessment. Ohio is piloting a similar program across different facilities (OhioMHAS, 2019). Others may enter SUD treatment because it is mandated by a judge. In these situations, a specific level of care may be mandated which may differ from the recommended level of care determined through patient placement criteria.
Lastly, one of the most common pathways into treatment is self-referral. An individual may find a treatment based on an internet search or talking with a friend or colleague, and then make an appointment or show up at the door.
References
New Hampshire Department of Health and Human Services (NH DHHS). (2019). The Doorway. [web page].
Ohio Department of Mental Health and Addiction Services (OhioMHAS). (2019). 21st Century CURES Act. [web page].
NOTES
-
Olmstead v. L.C., 527 U.S. 581 (1999).
-
As of July 16, 2019, 24 states had received a Medicaid 1115 SUD waiver (https://www.kff.org/medicaid/issue-brief/medicaid-waiver-tracker-approved-and-pending-section-1115-waivers-by-state/).
-
Data dictionaries of the different instruments used are located at http://gaincc.org/instruments/.