
U.S. Department of Health and Human Services
State Purchasing Strategies Drive State Contracts with Medicare Special Needs Plans
Jessica Kasten, Paul Saucier and Brian Burwell
Thomson Reuters
September 2009
PDF Version: http://aspe.hhs.gov/daltcp/reports/2009/stpur.pdf (11 PDF pages)
This issue brief was prepared under contract between the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy (DALTCP) and Thomson Health Care. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Hunter McKay, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201, Hunter.McKay@hhs.gov.
Summary
Beginning in 2010, new and expanding Medicare Special Needs Plans (SNPs) for dual eligibles must have contracts in place with state Medicaid agencies to coordinate Medicare and Medicaid benefits for their members. This brief provides information on the extent and nature of SNP-state contracting in 2008, the last year in which new SNPs were authorized prior to a federal moratorium. With the moratorium now lifted for plan year 2010, past contracting practices provide insight into how and why future SNP-state relationships will take shape. Key findings include:
-
Eighteen states contracted with dual eligible SNPs in 2008. This represented a slight change from the 2006-2007 period despite significant growth in the number of dual eligible SNPs between 2006 and 2008.1
-
SNP-state contracts fell into three categories, based on state purchasing strategy:
- Contracts which promoted Medicare-Medicaid coordination/integration;
- Medicaid managed care contracts which included duals, and where the Medicaid plan or its corporate sponsor held a parallel SNP contract;
- Medicaid contracts for Medicare cost-sharing only.
-
Existing state Medicaid contracts with SNPs raise important definitional questions about the dual SNP contracting mandate established under the Medicare Improvements for Patients and Providers Act (MIPPA) of 2008. A dual SNP is often operated as a distinct product within a larger corporate entity. The corporate parent may or may not also operate a Medicaid managed care contract that includes duals. What types of contracts between states and SNPs (or their corporate parents) meet the MIPPA requirement is ambiguous in many situations.
Placing the new federal contracting mandate in the context of existing state practice underscores the need for greater dual eligible policy coordination between the federal and state governments. While state and federal policy makers share the goal of greater service coordination for dual eligibles, state approaches to achieving this goal vary according a states Medicaid purchasing strategy more generally, and its approach to long-term care services more specifically. Federal mandates for more coordinated management of dual eligibles must recognize state Medicaid long-term care purchasing objectives as well as Medicare purchasing strategies for medical care.
Background
The high costs and fragmented care provided to persons dually eligible for Medicare and Medicaid are matters of increasing focus among the federal and state health policy communities. The 8.8 million persons eligible for both Medicare and Medicaid benefits accounted for 46% of all Medicaid spending in 2005, and about 25% of Medicare spending.2 Various models of health care financing and delivery which can more effectively address cost and quality issues for dual eligibles have been tested for two decades, but no single approach has yet been embraced universally and brought to national scale. Under the Medicare Modernization Act (MMA) of 2003, Congress authorized, for the first time, the establishment of Medicare managed care plans that focused solely on enrolling and managing care for persons with dual eligibility.3 These plans--called SNPs--grew rapidly in their first five years of federal authority, and by 2008, there were approximately 436 SNPs serving dual eligibles, with a total enrollment of approximately 906,000.4
While some observers believed SNPs could become the national model for serving dual eligibles, it became clear that more formal mechanisms would be needed if SNPs were to become the vehicle for integrating Medicare benefits with state-funded Medicaid services. In 2008, Congress created new requirements for dual eligible SNPs in the MIPPA, mandating increased Medicare-Medicaid coordination. Specifically, MIPPA requires all new SNPs established after January 1, 2010, and any existing SNP which wants to expand its service area, to have a contract with its respective state Medicaid agency for the coordination of Medicaid services.5
In order to better understand the MIPPA mandate for SNP-state contracting, it is important to understand the current status of SNP contracting with state Medicaid agencies for their dually eligible members. Prior to MIPPA, a number of SNPs already had state Medicaid contracts for their members and were already coordinating both Medicare and Medicaid benefits. Indeed, a number of SNPs were Medicaid managed care plans that served dual eligibles prior to applying for SNP certification status. Other SNPs were operating as special demonstrations to test integrated care models for dual eligibles, and converted from a demonstration authority to the SNP authority after the enactment of the MMA in 2003. This brief describes the extent of SNP-state contracting in 2008, and the nature of those contractual relationships, in order to better inform federal and state implementation of the new MIPPA mandate, as well as the broader policy objective of improving coordination of Medicare and Medicaid services for dual eligibles.
Approach
We used numerous data sources to ascertain which dual eligible SNPs had contracts with state Medicaid programs in 2008. States with high-profile dual eligible programs (e.g., Massachusetts, Minnesota, Wisconsin) which were originally developed as demonstration programs are well documented in the literature and we were able to confirm the existence of contracts with officials in those states. To supplement this information, we reviewed:
- The federal evaluation of Medicare Advantage SNPs conducted in 2006-2007;6
- Proposals submitted by health plans to CMS in 2007 to establish or expand SNP products for the 2008 Medicare Advantage contract year; and
- CMS administrative data related to SNP enrollment and dual eligible enrollment in Medicaid managed care.
The federal evaluation identifies states with SNP contracts as of 2006-2007. The SNP proposals provide the most current information available on SNP-state contracts from Medicare Advantage Organizations requesting CMS approval to introduce new SNPs or make changes to existing SNPs in 2008.7
Using the SNP-state contracts cited in the federal evaluation as a starting point, we analyzed the 2008 SNP proposals to identify new contracts and developing contracts. Since the proposals represented only a subset of SNPs (new SNPs and existing SNPs requesting changes), we used additional sources to confirm the current status of SNP-state contracts referenced in the federal evaluation and to investigate other states we thought might have SNP contracts. We relied on a combination of CMS administrative data and strategic follow-up calls with state Medicaid officials, CMS Regional Office staff, and health plan administrators. First, we validated the possibility of a SNP-state relationship based on CMS reports on dual eligible enrollment in Medicaid managed care by state in 2007. We assumed a SNP-state relationship would be highly unlikely in states which do not permit dual eligibles to enroll in Medicaid managed care (with the exception of contracts pertaining solely to Medicare cost-sharing).8 For states that include dual eligibles in Medicaid managed care, we then checked whether the Medicaid managed care organizations (MCOs) operating in these states had companion dual eligible SNPs.9
For additional clarification on some states, we spoke with CMS and state Medicaid agency officials, and health plan administrators familiar with each states SNP-Medicaid relationship.
Findings
-
Eighteen states contracted with dual SNPs in 2008. This represented a very slight change from the 2006-2007 period, despite significant growth in the number of dual SNPs during that period.
As indicated in Table 1, we found a net increase of only one additional state contracting with dual eligible SNPs between 2006 and 2008. This is in contrast to the rapid growth of dual SNPs in the same period, during which the number of dual SNPs nearly doubled from 225 to 436.10
The federal evaluation of Medicare SNPs identified 17 states with SNP contracts in the 2006-2007 period.11 We identified 18 states with SNP contracts in 2008. We found two additional states, Alabama and Idaho, that had contracts with SNPs, and found that the previously reported contract in Illinois was no longer in effect. The shaded rows in Table 1 highlight differences between our findings and the previous findings.
-
Existing SNP-state contracts fall into one of three categories, based largely on state purchasing strategy:
- Medicare-Medicaid Coordination/Integration for Duals;
- Medicaid Managed Care for Duals; and
- Capitated Cost-Sharing for Duals
The presence of a SNP-state contract may be an indicator of Medicare-Medicaid coordination, but the range of existing contractual relationships points to a continuum of coordination efforts. Table 2 categorizes the relationships as demonstrated in the contracts themselves and in related program materials. Figure 1 provides a map of the type of contractual relationship by state.
FIGURE 1. Contracting Status of State Medicaid Programs with Dual Eligible Special Needs Plans in 2008 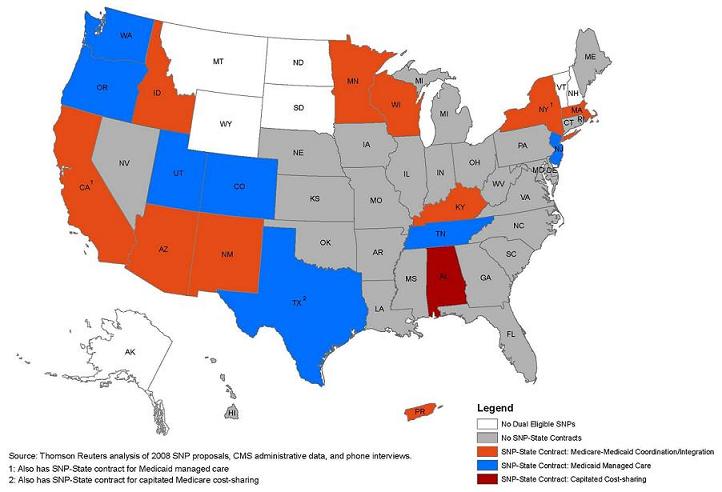
Category A, Medicare-Medicaid Coordination/Integration, includes state programs where coordination or integration of Medicare and Medicaid is a key program goal. These include the well-known dual demonstration programs in Massachusetts, Minnesota and Wisconsin, which were designed to integrate the full range of primary, acute and long-term care for dually eligible beneficiaries. Those programs are all voluntary, and members are choosing dual enrollment for both Medicare and Medicaid when they opt into the program. Also in this category are mandatory Medicaid managed long-term care initiatives, including the oldest state program (Arizonas Long Term Care System) and the most recent effort (New Mexicos Coordinated Long Term Services program). In these programs, the state promotes coordination by requiring their vendors to offer Medicare Advantage companion plans, but because Medicare enrollment may never be compulsory under federal law, only a subset of the state programs enrollees are also enrolled for Medicare services.
Category B, Medicaid Managed Care for Duals, is comprised of state programs in which dually eligible beneficiaries are included in Medicaid managed care, but as part of a broader strategy that is targeting Medicaid services across population groups. SNP status is not required by the state but is present because the participating Medicaid health plan has also chosen to become a SNP. In most of these programs, including the New Jersey HMO Program, the New York Managed Long Term Care Program, the Oregon Health Program and TennCare, only a subset of participating Medicaid plans are SNPs. Coordination of Medicaid and Medicare services is possible, but depends on the business model of the plan. Many of the plans in this category first became SNPs so they could continue providing pharmacy benefits to their existing dually eligible members when Part D was implemented in 2006. Others in this category developed SNPs with the hope of leveraging their state Medicaid relationships to identify and enroll dual eligibles into Medicare products.
Finally, Category C is comprised of contracts that address cost-sharing only. These contracts are narrowly written to address only one benefit: the state Medicaid programs obligation to pay Medicare cost-sharing for low income beneficiaries. In these programs, the primary goal appears to be administrative simplification by paying a set capitation to the plan for cost-sharing, rather than processing cost-sharing claims on an encounter-by-encounter basis.
-
Existing contracts raise an important definitional question about the MIPPA contracting requirement. SNPs are often operated as distinct products within a larger health carriers array which could include Medicaid managed care plans. In some instances, it is difficult to know whether the state contract is with the SNP or with a Medicaid plan owned by the same parent company. If the latter, the contracts application to the SNP is unclear.
As we reviewed the state contracts section of the 2008 SNP proposals to CMS, we noted some ambiguities in applicants responses as to the existence of state contracts. Some MCOs responded that they had contracts with state Medicaid agencies, but upon further examination it became clear that they were referring to contracts for participation in Medicaid managed care programs, some of which excluded dual eligibles. Even if dual eligibles were included in the managed care programs, some contracts were not necessarily for the specific SNPs services, nor did they necessarily include provisions for coordinating Medicare and Medicaid benefits.
Discussion
Our analysis of the status of SNP-state contracting prior to the MIPPA mandate demonstrates a broad range of relationships between states and SNPs. While there are a number of relationships in which the clear policy goal is integration of Medicare and Medicaid benefits for dual eligibles, the most interesting finding of our analysis was the large number of contracts which fell into Category B, where the nature of the SNP-state relationship is considerably more opaque, and whether or how Medicaid and Medicare benefits are coordinated remains unclear.
In the further evolution of policy regarding SNP-state contracting, it is important to recognize that most SNPs are part of larger corporate entities. The federal evaluation showed that 86% of SNPs were not stand-alone organizations. In our analysis of SNP-state contracting, we found many instances in which the SNP parent organization also had a Medicaid managed contract that served dual eligibles, at least some of whom could be members of both plans, but in which the coordination of care practices across the two plans was not explicitly addressed in the states Medicaid managed care contract.
Second, it is also important to recognize the enrollment patterns across Medicaid and Medicare SNP contracts held by the same parent organization are, in most cases, asynchronous. For example, a Medicaid managed care contract may cover a broad population of aged and disabled Medicaid recipients, some of whom are duals and others not. In another case, a Medicaid contract may mandate enrollment for duals, but Medicare SNP enrollment must remain voluntary. Thus, it is not possible for the Medicaid plan to capture and coordinate benefits for all of its duals on the Medicare side. A Medicaid plan may have large Medicaid dual enrollment, but low Medicare SNP enrollment, due to its voluntary nature. Indeed, it is entirely possible for dual eligibles enrolled in a large Medicaid plan to be enrolled in a number of different SNP plans, only one of which is associated with the Medicaid plan.
Third, it is important to recognize that unlike Medicare managed care, where Medicare Advantage organizations generally cover all Medicare benefits, Medicaid plans often cover only a subset of Medicaid benefits. For example, a number of states have initiatives in which dual eligibles are enrolled in specialty behavioral health care plans for the management of mental health services. In these cases, in order to effectively coordinate services, a SNP needs to coordinate with both Medicaid behavioral health vendors and other Medicaid providers who remain fee-for-service.
Better care coordination practices across the full spectrum of Medicare and Medicaid benefits for dual eligibles is a laudable policy goal. However, coordinated care models for dual eligibles must recognize that Medicare purchasing strategies for duals, and state Medicaid purchasing strategies for duals, have distinct, and sometimes inconsistent, objectives. The MIPPA mandate for SNPs to secure Medicaid contracts for their dually eligible members may help to promote integrated care models, but only from the Medicare perspective. States have their own purchasing strategies for dual eligibles, which are usually more focused on improved management of long-term service benefits.
For integrated care models for dual eligibles to enter the mainstream, there may be a need for greater collaboration between the Federal Government and the states in bringing their respective purchasing strategies into alignment.
| TABLE 1. States Contracting with Dual Eligible SNPs | |
| 2006-2007 | 2008 |
| Alabama | |
| Arizona | Arizona |
| California | California |
| Colorado | Colorado |
| Idaho | |
| Illinois | |
| Kentucky | Kentucky |
| Massachusetts | Massachusetts |
| Minnesota | Minnesota |
| New Jersey | New Jersey |
| New Mexico | New Mexico |
| New York | New York |
| Oregon | Oregon |
| Tennessee | Tennessee |
| Texas | Texas |
| Utah | Utah |
| Washington | Washington |
| Wisconsin | Wisconsin |
| Puerto Rico | Puerto Rico |
| TOTAL STATES: 17 | TOTAL STATES: 18 |
| SOURCE: For 2006-2007, Schmitz et al. (2008). | |
| TABLE 2. SNP-State Contracts Categorized by State Purchasing Strategy | |||
| A. Medicare-Medicaid Coordination/Integration | B. Medicaid Managed Care for Duals | C. Capitated Cost-Sharing for Duals | |
| Characteristics |
|
|
|
| State Programs |
|
|
|
Notes
-
We assessed SNP-state contracting for calendar year 2008. SNP-state contracting in 2006-2007 is reported in Chapter V of the federal evaluation of the SNP program: Schmitz, Robert, Angela Merrill, Jennifer Schore, Rachel Shapiro and Jim Verdier, 2008. Evaluation of Medicare Advantage Special Needs Plans, Summary Report. Submitted by Mathematica Policy Research, Inc. to the U.S. Department of Health and Human Services (HHS), Centers for Medicare and Medicaid Services (CMS).
-
Holahan, J., Miller, D. and Rousseau, D. 2009. Dual Eligibles: Medicaid Enrollment and Spending for Medicare Beneficiaries in 2005. Kaiser Commission on Medicaid and the Uninsured.
-
Saucier, P., Kasten, J., and Burwell, B. Federal Authority for Medicare Special Needs Plans and their Relationship to State Medicaid Programs. Prepared under contract to the Office of the Assistant Secretary for Planning and Evaluation, HHS, January 2009. Available at http://aspe.hhs.gov/daltcp/reports/2009/leghist.htm.
-
CMS Special Needs Comprehensive Report, November 2008, available at http://www.cms.hhs.gov/MCRAdvPartDEnrollData and CMS Special Needs Plan Fact Sheet available at http://www.cms.hhs.gov/SpecialNeedsPlans/Downloads/FSNPFACT.pdf.
-
Public Law 110-275, July 15, 2008.
-
Schmitz et al., Table V.1 SNP Activity by State, 2006-2007.
-
Starting in contract year 2008, CMS included a series of questions on state contracts in the Medicare Advantage SNP application.
-
See the Kaiser Family Foundations 50-state report of dual eligible enrollment in Medicaid managed care by plan type as of June 2007 (based on CMS data), available at http://www.statehealthfacts.org/comparetable.jsp?ind=220&cat=4. See Verdier et al. 2008, Schmitz et al. 2008 for discussion of the link between the development of SNP-state contracts and Medicaid managed care.
-
To identify the Medicaid MCOs, we referred to a CMS Medicaid managed care summary statistics report at http://www.cms.hhs.gov/MedicaidDataSourcesGenInfo/Downloads/mmcer06.pdf. And, to verify the SNP, we used CMS SNP Comprehensive Report which shows SNP enrollment by SNP, SNP type, and state (available at http://www.cms.hhs.gov/MCRAdvPartDEnrollData/SNP/list.asp).
-
CMS Special Needs Comprehensive Report, November 2008, available at http://www.cms.hhs.gov/MCRAdvPartDEnrollData and CMS Special Needs Plan Fact Sheet available at http://www.cms.hhs.gov/SpecialNeedsPlans/Downloads/FSNPFACT.pdf.
-
SNP-state contracting in 2006-2007 is reported in Chapter V of the federal evaluation of the SNP program: Schmitz, Robert, Angela Merrill, Jennifer Schore, Rachel Shapiro and Jim Verdier, 2008. Evaluation of Medicare Advantage Special Needs Plans, Summary Report. Submitted by Mathematica Policy Research, Inc. to HHS/CMS.
Issue Briefs on Special Needs Plans
A total of three Issue Briefs are available from the Office of Disability, Aging and Long-Term Care on this subject:
-
Federal Authority for Medicare Special Needs Plans and Their Relationship to State Medicaid Programs, http://aspe.hhs.gov/daltcp/reports/2009/leghist.htm (Posted April 2009)
-
State Purchasing Strategies Drive State Contracts with Medicare Special Needs Plans, http://aspe.hhs.gov/daltcp/reports/2009/stpur.htm (Posted June 2010)
- Medicaid Contracts with Medicare Special Needs Plans Reflect Diverse State Approaches to Dually Eligible Beneficiaries, http://aspe.hhs.gov/daltcp/reports/2009/SNPdual.htm (Posted June 2010)
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services Home [http://www.hhs.gov]