
This study aimed to describe and characterize the published literature on disparities between racial and ethnic groups among individuals with Alzheimer’s disease and related dementias. To identify relevant studies, we searched electronic sources for peer-reviewed articles and research reports published through 2014 related to the Alzheimer’s population and their caregivers that provided evidence of racial and ethnic disparities, discussed reasons for disparities, or described interventions to address disparities. The literature shows consistent and adverse disparities among blacks and Hispanics compared to non-Hispanic whites in the prevalence and incidence of Alzheimer’s disease, mortality, participation in clinical trials, use of medications and other interventions, use of long-term services and supports, health care expenditures, quality of care, and caregiving. The literature suggests numerous underlying causes, including factors related to measurement of the disease, genetics, socioeconomic factors, cultural differences, lack of culturally competent providers, and discrimination. Although these disparities are well known, little is known about the effectiveness of various strategies, such as cultural competence training, to address these differences within the context of Alzheimer’s disease, with almost no studies available that evaluate possible interventions. [34 PDF pages]
"Abstract
This study aimed to describe and characterize the published literature on disparities between racial and ethnic groups among individuals with Alzheimer's disease and related dementias. To identify relevant studies, we searched electronic sources for peer-reviewed articles and research reports published through 2014 related to the Alzheimer's population and their caregivers that provided evidence of racial and ethnic disparities, discussed reasons for disparities, or described interventions to address disparities. The literature shows consistent and adverse disparities among Blacks and Hispanics compared to non-Hispanic Whites in the prevalence and incidence of Alzheimer's disease, mortality, participation in clinical trials, use of medications and other interventions, use of long-term services and supports, health care expenditures, quality of care, and caregiving. The literature suggests numerous underlying causes, including factors related to measurement of the disease, genetics, socioeconomic factors, cultural differences, lack of culturally competent providers, and discrimination. Although these disparities are well known, little is known about the effectiveness of various strategies, such as cultural competence training, to address these differences within the context of Alzheimer's disease, with almost no studies available that evaluate possible interventions.
About the Authors
Lisa M. Lines, PhD, MPH, is a health services researcher in the Aging, Disability, and Long-term Care group at RTI International, Waltham, MA.
Joshua M. Wiener, PhD, is a Distinguished Fellow and Program Director of the Aging, Disability and Long-Term Care group at RTI International, Washington, DC.
Acronyms
The following acronyms are mentioned in this report.
| AChEI | Acetylcholinesterase Inhibitors |
|---|---|
| APOE | Apolipoprotein E E3 is the normal/neutral form; E2 and E4 are variants |
| CLESE | Coalition of Limited English Speaking Elderly |
| ICU | Intensive Care Unit |
| IOM | Institute of Medicine |
| IQ | Intelligence Quotient |
| MeSH | Medical Subject Heading |
| MMSE | Mini-Mental Status Examination |
| REACH | Resources for Enhancing Alzheimer's Caregiver Health |
Introduction
Existing evidence for Alzheimer's disease and related dementias suggests that there are significant differences in prevalence, incidence, treatment, and mortality of Alzheimer's disease across racial and ethnic groups. There are also substantial differences in participation in clinical trials, the use of services, and disease-related expenditures. Disparities across racial and ethnic groups in diagnosis and treatment rates and in the use of services are concerns from an ethical and policy perspective. In an ideal world, the burden of disease and access to services would not vary based on a person's race or ethnic background.
As the population ages and minorities become a higher proportion of the older population, a higher percentage of people with Alzheimer's disease will be minorities. Among the population aged 85 and older, which is the age group most likely to have Alzheimer's disease, the proportion of the population that is White is projected to decline from 90% in 2010 to 81% in 2050 (Vincent & Velkoff, 2010). The proportion of the 85 and older population that is non-Hispanic White is projected to decline from 85% in 2010 to 67% in 2050. During the same time period, the proprtion of the population aged 85 and older that is Hispanic is projected to increase from 5% to 15%.
This research report describes evidence from the literature of racial and ethnic disparities in Alzheimer's disease, explores possible reasons for these disparities, and reviews interventions that have attempted to reduce disparities in this population.
Methods
To identify relevant studies, we searched PubMed, Google Scholar, and our in-house electronic library for peer-reviewed articles and research reports published in English through 2014 related to the Alzheimer's population and their caregivers. We also searched the Internet for gray literature using similar search terms. We included studies and reports that provided evidence of racial and ethnic disparities, discussed reasons for disparities, or described interventions to address disparities, including other reviews, books, government and non-profit research reports, and research studies published in peer-reviewed journals. Our searches of the peer-reviewed literature combined free text and Medical Subject Heading (MeSH) terms, such as "disparities," "disparity," and "discrimination," with free text and MeSH terms for Alzheimer's disease and dementia ("dementia" OR "alzheimer disease" OR "cognitive impairment"). Journal articles were required to have an abstract and pertain to human subjects. Our initial search located 151 article abstracts. After excluding articles that were clearly irrelevant based on their title or abstract, we reviewed the full texts of 35 refereed articles and 15 other sources (books, reports, web pages, etc.).
Evidence of Racial and Ethnic Disparities
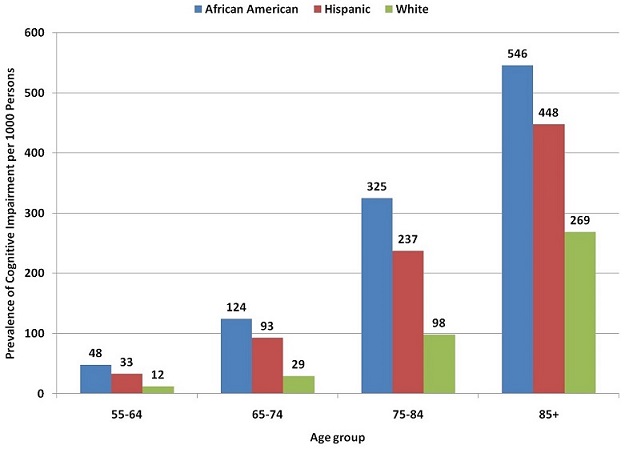
Incidence estimates also suggest higher risk of Alzheimer's disease among non-White populations. In a 7-year study in the Washington Heights and Inwood communities of New York City, overall adjusted incidence rates for probable and possible Alzheimer's disease (excluding vascular and other dementias) among Whites were 0.4% per person-year for ages 65-74, 2.6% for ages 75-84, and 4.2% for ages 85+ (Tang et al., 2001). Incidence was higher among African Americans (1.7%, 4.4%, and 11.4%) and Caribbean Hispanics (1.4%, 4.4%, and 8.8%) in the same community. One recent study found that the unadjusted hazard ratio for developing dementia over 12 years was 1.44 for Black participants compared to White, but after adjusting for demographics, apolipoprotein (APOE) E4, comorbidities, lifestyle factors, and socioeconomic status, the Black-White difference was reduced to 1.09 and was no longer significant (Yaffe et al., 2013).
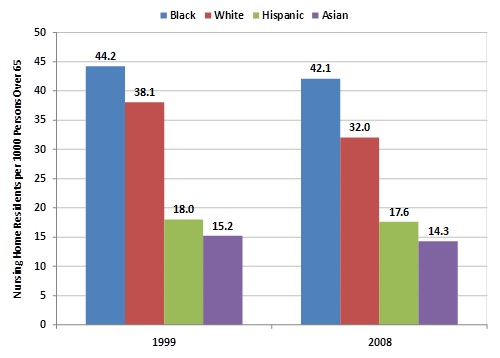
TABLE 1. Use of and Medicare Payments for Health Care Services among Medicare Beneficiaries with a Dementia Diagnosis, by Race/Ethnicity, 2006
| Overall | White | African American | Hispanic | |
|---|---|---|---|---|
| Total mean Medicare payment per beneficiary | $15,333 | $14,498 | $21,044 | $19,933 |
| Mean Medicare payment for hospital care per beneficiary | $4,964 | $4,563 | $7,687 | $6,632 |
| Mean hospital discharges per 1,000 beneficiaries | 660 | 632 | 887 | 731 |
| Mean number of hospital days per beneficiary | 4.2 | 3.9 | 6.4 | 5.2 |
| Mean Medicare payment for physician visits per beneficiary | $1,018 | $956 | $1,390 | $1,411 |
| Mean number of physician visits per beneficiary | 12.7 | 12.1 | 16.4 | 17.1 |
| Mean Medicare payment for home health care per beneficiary | $1,118 | $1,025 | $1,591 | $2,453 |
| Percentage of beneficiaries with at least one home health claim | 18.8% | 18.2% | 22.1% | 25.9% |
| Mean Medicare payment for hospice per beneficiary | $1,732 | $1,789 | $1,514 | $1,225 |
| Percentage of beneficiaries with at least one hospice claim | 13.7% | 14.2% | 11.3% | 8.8% |
SOURCE: Adapted from Alzheimer's Association, 2011.
Possible Reasons for Racial and Ethnic Disparities
Possible reasons for racial and ethnic disparities include factors related to measurement of Alzheimer's disease, genetics, cardiovascular and cerebrovascular disease, socioeconomic factors, cultural differences, and racial and ethnic discrimination. A range of pathways have been suggested that link race and ethnicity with cognitive impairment, some of which have implications for disparities (Figure 3) (Glymour & Manley, 2008). In this section, we describe the evidence underlying selected factors, mediators, and pathways associated with disparities in this population.
FIGURE 3. Pathways Linking Race/Ethnicity and Cognitive Impairment
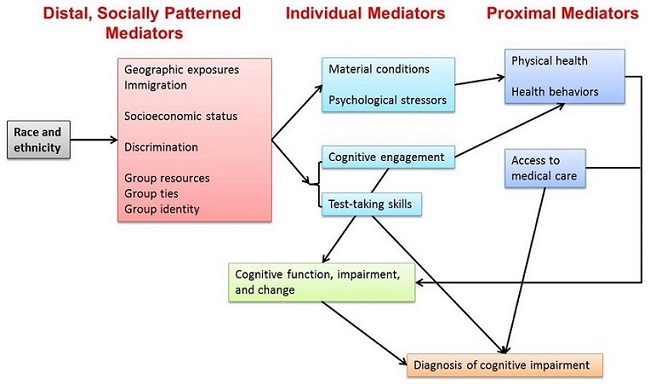
SOURCE: Adapted from Glymour and Manly, 2008.
Factors Related to Measurement of Alzheimer's Disease Prevalence and Incidence
The historically higher prevalence rates for community-dwelling African Americans than for Whites may be partially attributable to the measurement of disease prevalence and incidence. For example, historically, lower institutionalization rates among African Americans in the past left more people with dementia in the community, whereas comparable Whites were in nursing homes (Froehlich et al., 2001). The institutionalization rate of people with dementia would affect estimated prevalence rates because most studies are of the community-based population.
The effects of education on cognitive test results, and cultural biases in reporting of cognitive impairment are likely to substantially affect prevalence estimates. The number of years of education may not be equivalent between racial/ethnic groups because of disparities in school quality, particularly in older cohorts. Therefore, even prevalence studies that control for education may not be able to adequately control for differences in educational quality (Glymour & Manley, 2008).
Cognitive testing instruments--including the most widely used instrument, the MMSE--perform differently among individuals of different educational levels and racial/ethnic groups (Teresi et al., 2002). Instrument bias can result from lower literacy and education, lack of test-taking experience and stress related to test-taking, varying degrees of acculturation, and language issues such as poor translation. In addition, greater variability in scores for African Americans on standard cognitive tests makes it difficult to establish cutpoints for abnormal results (Froehlich et al., 2001).
Minorities seeking care are often more impaired at the time of their diagnosis, which suggests that they may be accessing services later in the disease process (Cooper et al., 2010). In addition, many community physicians are reluctant to diagnose Alzheimer's disease for reasons such as inadequate reimbursement for evaluation and management, lack of time to provide appropriate follow-up care, lack of knowledge of when and to whom to refer, lack of information about diagnostic criteria, cultural resistance, and belief that there is no treatment. Anecdotally, this reluctance is more prevalent in minority communities (National Institute on Aging, 2010). Moreover, there is some evidence that caregivers of Black elders with cognitive impairment report less cognitive decline in the care receiver than do their White peers, despite no significant differences in impairment, suggesting that Black caregivers may perceive changes in cognition differently (Rovner et al., 2012).
The issues of cultural framework, perception, and understanding of disability are important when interpreting scales that include items with different cultural connotations. Diagnosis is clearly problematic when physicians and patients do not speak the same language or do not share the same cultural perspective. Moreover, some diagnostic instruments contain items that may carry substantial cultural implications that vary by group. For example, a hangman's noose, one of the items on the Boston Naming Test, may have very different implications for elderly African American and White respondents (Jett, 2006).
Genetics
APOE is a gene that comes in a normal or neutral form (allele), known as E3, and two variants, E2 and E4, which have been implicated in vascular and Alzheimer's diseases. The E4 variant is the most important known genetic risk factor for Alzheimer's disease.
In a recent review and meta-analysis, E4 has been shown to be associated with about 65%-75% of cases of sporadic (not genetically inherited) Alzheimer's disease and up to 20% of all dementias (Crean et al., 2011). The meta-analysis found that 39% of Alzheimer's disease patients from Asian countries carried the E4 allele; 43% of patients from Southern Europe and the Mediterranean; 54% from Central Europe; 59% from North America; and 64% from Northern Europe.
Having one or two alleles, or forms, of the APOE gene is a major predictor of Alzheimer's disease in Whites but a weak or inconsistent predictor in African Americans and Hispanics (Crean et al., 2011). In an earlier meta-analysis, the prevalence of E4 among those with Alzheimer's disease was highest in Whites (37%), followed by African Americans (32%), Japanese (28%), and Hispanics (19%) (Farrer et al., 1997). Two genetic studies have found that the E4/E4 genotype is more likely to be associated with dementia in African Americans than in Whites (Green et al., 2002; Maestre et al., 1995), but a third found that one or more E4 alleles was not associated with increased risk in African Americans or Hispanics, but was in Whites (Maestre et al., 1995). The E2/E4 and E3/E4 genotypes have been shown to be associated with an increased risk of Alzheimer's in Whites, but not African Americans, in one study (Green et al., 2002). However, an earlier study found an increased risk associated with the E2/E3 genotype among African Americans, but not Whites (Maestre et al., 1995).
Cardiovascular and Cerebrovascular Disease
Vascular factors and conditions that may be associated with cognitive decline and dementia include stroke, diabetes, hypertension, congestive heart failure, high fat intake, high cholesterol, smoking, alcohol misuse, atrial fibrillation, low folate, and obesity (Glymour & Manley, 2008). Although there is no definitive evidence linking cardiovascular disease and Alzheimer's disease, studies have found associations between cognitive impairment and cardiovascular disease (Purnell et al., 2009).
Most of the cardiovascular disease risk factors are more common in African Americans and Hispanics (Glymour & Manley, 2008). Geographic variation in the prevalence of cardiovascular disease risk factors may be related to differences in regional dietary patterns. More than 80% of Blacks aged 65+ in 2000 were born in the South, and Southern-born individuals have significantly higher rates of circulatory disease mortality (Glymour & Manley, 2008).
Vascular dementia accounts for a larger proportion of cases of related dementias in African Americans than in Whites (Froehlich et al., 2001). However, as with other dementia disorders, it is unclear whether differences in the prevalence of vascular dementia reflect true differences or are a result of measurement bias because of differences in education, socioeconomic status, or other cultural factors. One recent study found that reducing ethnic and racial disparities in the incidence of Type 2 diabetes could reduce the incidence of cognitive impairment and dementia by 17% (Noble et al., 2012).
A few studies suggest that differences in Alzheimer's disease prevalence cannot be attributed to differences in underlying cardiovascular disease rates. In one study, Black Alzheimer's disease patients had higher crude rates of hypertension than did Whites, but differences in other rates of cardiovascular disease (heart disease, stroke, diabetes) were not significantly different between the groups (Hargrave et al., 1998). In another study, although the cumulative incidence rate of Alzheimer's disease was twice as high among African Americans and Caribbean Hispanics, the presence of cardiovascular or cerebrovascular disease did not contribute to increased risk (Tang et al., 2001).
Socioeconomic Factors
Parental or early life socioeconomic position, childhood IQ, measures of early growth (such as infant head circumference and childhood height), educational attainment, occupational characteristics, and various measures of social integration have all been linked to cognitive function and neurocognitive disorders in adulthood and old age (Glymour & Manley, 2008). Individual socioeconomic position may affect cognitive status or diagnoses through: (1) material conditions; (2) psychosocial conditions (such as status); (3) direct cognitive stimulation; or (4) test-taking skills (Glymour & Manley, 2008) .
Geronimus et al. (2006) attributed many racial and ethnic disparities in health to "weathering," the accumulated consequences of exposure to economic and social adversity. Having financial resources leads to health-enhancing conditions such as healthy housing, high-quality food, safe working conditions, and access to high-quality medical care (and the reverse is true as well). Occupation influences health both through stress and material deprivation, and through toxic work conditions (Glymour & Manley, 2008).
Poverty often reduces access to educational opportunities or is associated with poor-quality education, thereby increasing the likelihood of adult poverty, which may increase the risk of depression and cognitive impairment (Glymour & Manley, 2008). If the effect of education on cognitive aging is primarily through material advantages, then credentials may be more important than quality. But if education's effect is because of cognitive skills or engagement, then school quality is more important. Resources available to parents are also very important to a child's cognitive development, and differences in parental socioeconomic status predict dementia. Extra schooling appears to have substantial benefits for memory function in the elderly (Glymour & Manley, 2008).
Additional evidence for the link between cognitive impairment and low income, less education, and having lived in a rural area comes from the 2006 Health and Retirement Study. All of these socioeconomic characteristics are more common among people with cognitive impairment, as shown in Figure 4 (Alzheimer's Association, 2011). For example, 89% of Hispanics over age 55 with cognitive impairment possess less than 12 years of education, compared to 49% of those with normal cognition.
FIGURE 4. Socioeconomic Characteristics by Cognitive Impairment and Race/Ethnicity, 2006 Health and Retirement Study
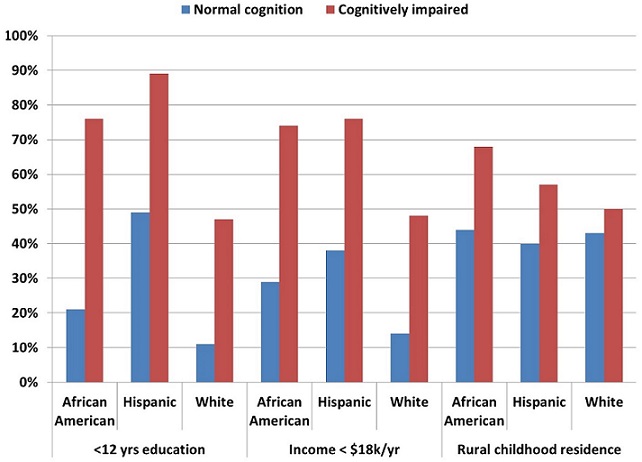
SOURCE: Alzheimer's Association, 2011.
Cultural Differences
Culture has been defined as a group's values, beliefs, traditions, symbols, language, and social organization (Harwood & Ownby, 2000). The United States model of health care, which values autonomy in medical decision making, contrasts with preferences for more family-based, physician-based, or shared physician and family-based decision making in other cultures. Moreover, although United States culture emphasizes full disclosure by providers, it is common for health care professionals in other countries to conceal serious diagnoses from patients because disclosure can be viewed as disrespectful, impolite, or even harmful to the patient (Searight & Gafford, 2005).
Cultural influences on African Americans that may affect disparities in treatment or access to medical care include the legacy of slavery and Jim Crow laws, the Tuskegee syphilis study, the interaction of religion with health care, the use of home remedies, distrust of the medical system, being of a different or the same race as one's medical provider, and health literacy (Eiser & Ellis, 2010). Some African Americans have strong religious beliefs, including the belief that illness can be cured or is controlled by God. Strong spirituality has been correlated with lower medication adherence and later stage cancer diagnosis (Eiser & Ellis, 2010). Similarly, some elderly African Americans and other non-White patients are more likely to use traditional or herbal medicines instead of, prior to, or alongside allopathic medicines.
Many individuals and cultures perceive dementia-related symptoms as a natural part of aging (Ayalon & Arean, 2004; Eiser & Ellis, 2010; Gelman, 2010; Gray et al., 2009; Jett, 2006). For example, one study asked participants whether the following statement is true: "Significant loss of memory/mental ability, commonly known as senility, is a normal part of aging." Of Whites, 23% agreed, compared to 55% of Hispanics and 33% of Chinese (Gray et al., 2009). An earlier study used different wording and found very different results: "Alzheimer's disease is a normal process of aging, like graying of hair or wrinkles." In that study, 66% of Whites, 50% of African Americans, 24% of Latinos, and 17% of Asians agreed with the statement (Ayalon & Arean, 2004).
Numerous cultural differences around caregiving for patients with Alzheimer's disease may also contribute to racial and ethnic disparities (Gray et al., 2009; Napoles et al., 2010). The most frequently documented cultural differences for both African American and Hispanic caregivers (compared to White caregivers) are more positive views of caregiving, greater spirituality, a stronger sense of duty to family, and higher value placed on extended family networks (Napoles et al., 2010). In a review of the literature, seven studies found evidence of worse mental health among Hispanic caregivers compared to Whites, whereas among African American caregivers, 11 studies found evidence of better mental health compared to Whites (Napoles et al., 2010). African American caregivers of people with Alzheimer's disease also appear to have more social support than White caregivers.
Research focused on Asian American caregivers is more limited, but there is evidence of a strong sense of filial responsibility in those communities (Napoles et al., 2010). Confucian cultures have a tradition of first-born sons and their wives being responsible for elder care (Janevic & Connell, 2001); people from these cultures may also be less likely to seek outside help in dealing with their family member and be less affected by the stress of caregiving.
Racial and Ethnic Discrimination
Although discrimination by providers against racial and ethnic minorities in the United States is commonly asserted as the cause of racial and ethnic disparities, we were unable to find any empirical studies on this topic that focused on people with Alzheimer's disease. Indeed, there appear to be few empirical studies on this topic in health care.
A rare study of discrimination in health care used the implicit association test to assess the degree to which implicit racial bias affected physicians' decisions on thrombosis (Green et al., 2007). A total of 287 internal and emergency medicine residents from four hospitals in Boston and Atlanta participated in an online study. Half of the physicians received information about a White patient, and the other half received the same information but were told that the patient was African American. Although physicians self-reported that they did not prefer treating one group or the other and did not see either group as more cooperative, the test found a preference for treating Whites and the perception that African Americans were less cooperative. Similarly, Blanchard and Lurie (2004) found that minorities were more likely to report being looked down upon or treated with disrespect than Whites. Specifically, adjusting for sex, language, income, insurance coverage, and education, 20% of Asians, 19% of Hispanics, and 14% of Blacks reporting being treated disrespectfully or looked down upon by their provider compared to 9% of Whites.
Although not specifically about Alzheimer's disease, the Institute of Medicine's (IOM's) Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care (Smedley et al., 2003) identified racial bias and prejudice (conscious and unconscious) as obvious potential reasons for differences in treatment for a number of diseases. Provider lack of empathy and limited contact with people of other races/ethnicities were identified as potential factors. The IOM report also cites the theory that the pressures of the health care environment can lead to providers stereotyping patients as a cognitive shortcut, which reduces the amount of time they need to spend with patients. The common tendency to see the patient-provider relationship as one of a lower-status person coming to a higher-status person for assistance, rather than a relationship between collaborators--regardless of race or ethnicity--could be a barrier to quality care.
Interventions to Reduce Racial and Ethnic Disparities
Although there is extensive evidence documenting disparities among different racial and ethnic groups with Alzheimer's disease, there are few studies evaluating interventions to address disparities in this population. Almost all interventions designed to explicitly address racial and ethnic disparities focus on cultural competency on the part of the health care provider and/or health system. Interventions not specific to the Alzheimer's disease population include care coordination, care management, community health workers, and culturally tailored education interventions (Quinones et al., 2011).
Cultural Competence
Cultural competency is especially important in the health care setting, where barriers to communication and access to quality care can result in delayed diagnosis, inappropriate treatment, or worse. Cultural competence involves both awareness and knowledge about other cultures and skill in relating to people of other cultures. Cultural competence requires acknowledging that culture and ethnicity guide and affect behavior, and that all people are cultural beings (Betancourt et al., 2003).
A culturally competent health care environment includes the following characteristics (Anderson et al., 2003): a culturally diverse staff that reflects the communities served; bilingual staff or interpreters for the clients' languages; culture-specific and language-specific training for providers; and signs and materials in the clients' languages that are sensitive to cultural norms.
One example of a policy designed to address disparities at the systems level is the Culturally and Linguistically Appropriate Services standards issued in 2000 (Office of Minority Health, 2001). This policy mandates certain activities (e.g., competent language assistance services and signage/materials in different languages) and encourages others (such as culturally competent care and staff diversity). The evidence for improved outcomes as a result of interpreter services is mixed, but a few studies suggest that patients with limited English proficiency who receive language assistance are more satisfied with their care and have better clinical outcomes (Smedley et al., 2003).
Cultural competence education is mandated as part of medical licensure or continuing medical education requirements in New Jersey, Washington, and California, and other states are debating similar rules (Eiser & Ellis, 2010). The accrediting authority for medical schools in the United States also has standards for cross-cultural curricula as part of undergraduate medical education (Liaison Committee on Medical Education, 2012).
Many studies of cultural competence training, not specific to Alzheimer's disease, have found that it has a beneficial effect on the attitudes, knowledge, and skills of physicians and on patient satisfaction (Beach et al., 2005). For example, 17 of 19 studies of cultural competence training for health professionals found a beneficial effect in terms of knowledge; 21 of 25 studies found that such training improved attitudes; and 14 of 14 studies showed benefits of training in improving skills. In addition, three studies found that cultural competence training of health professionals improved patient satisfaction. No definitive evidence has yet linked this training to improved health outcomes (Beach et al., 2005; Betancourt et al., 2003). One study of counseling of Black female patients showed that cultural competence improved patient adherence (Beach et al., 2005) .
The goal of the Administration for Community Living-funded Alzheimer's Disease Supportive Services Program (previously called the Alzheimer's Disease Demonstration Grants to States program) is to provide or expand support services for traditionally underserved or hard-to-serve Alzheimer's patients and their caregivers, especially minorities and rural residents. The Illinois intervention focused on older persons who spoke Arabic, Assyrian, Bosnian, Hindi, and Urdu (Wiener & Mitchell, 2007). The grant worked with the Coalition of Limited English Speaking Elderly (CLESE), an organization representing 45 Chicago-area ethnic organizations that provide services to older people. Under the grant, CLESE organizations translated materials into the appropriate languages, identified home care clients with memory loss, made home visits to try to enroll elderly people into the program, conducted caregiver training, and trained providers to screen for dementia.
A recent comprehensive review of interventions focused on Alzheimer's disease and related disorders caregivers found 18 studies, of which 11 considered cultural factors in their design; eight of those 11 studies were from the REACH initiative (Napoles et al., 2010). Cultural tailoring in these studies addressed familism (i.e., the primacy of the family over individual interests), language, bicultural and bilingual staffing, health literacy, the need for advocacy, protecting elders, and logistical barriers.
Quality of care is related to cultural competence and diversity among providers (Daker-White et al., 2002; Means, 2002). Where service providers match clients with staff according to ethnicity and language, patient outcomes may be improved (Braun & Browne, 1998). Similarly, when staff receive training in cultural awareness and sensitivity and cognitive testing is language-appropriate, this may help address some disparities (Daker-White et al., 2002).
Caregiver interventions may be more effective if delivered by staff who are not only bilingual but also bicultural (Napoles et al., 2010). For example, the REACH and REACH II projects--multisite studies to evaluate culturally tailored interventions--were effective at reducing depression and improving quality of life among caregivers (Belle et al., 2006). One of REACH's strengths is the tailoring of the intervention materials individual caregivers, and the bilingual/bicultural staff.
Outreach to Minority Communities
Another approach to addressing disparities involves targeting programs and outreach to minority populations. For example, the Alzheimer's Disease Demonstration Grants to States program provided demonstration grants to Florida, Kentucky, and the District of Columbia, that focused on African Americans (Wiener & Mitchell, 2007). For example, in the District of Columbia, the intervention focused on educational efforts conducted within church communities. They also held awareness events and developed caregiver respite programs. More recently, several of the current Alzheimer's Disease Supportive Services Program grantees, including South Carolina, California, Florida, North Carolina and Puerto Rico, are targeting ethnic or racial groups.
Another intervention aimed at reaching minority populations is the Alzheimer's Disease Research Center Satellite Diagnostic and Treatment Clinics program (National Institute on Aging, 2010). Begun in 1990, the program established satellite clinics linked with one of the 30 existing Alzheimer's Disease Centers. In recent years, satellite clinics have been established on the Choctaw nation reservation, in Harlem, at Grady Hospital in Atlanta, and in St. Louis. The Alzheimer's Disease Centers are actively involved in formulating strategies and plans to recruit diverse populations to their clinics. Strategies that have met success include improved patient coordination, increasing the personal attention patients receive, home visits, and support groups (National Institute on Aging, 2010).
Cultural Competence
Cultural competency is especially important in the health care setting, where barriers to communication and access to quality care can result in delayed diagnosis, inappropriate treatment, or worse. Cultural competence involves both awareness and knowledge about other cultures and skill in relating to people of other cultures. Cultural competence requires acknowledging that culture and ethnicity guide and affect behavior, and that all people are cultural beings (Betancourt et al., 2003).
A culturally competent health care environment includes the following characteristics (Anderson et al., 2003): a culturally diverse staff that reflects the communities served; bilingual staff or interpreters for the clients' languages; culture-specific and language-specific training for providers; and signs and materials in the clients' languages that are sensitive to cultural norms.
One example of a policy designed to address disparities at the systems level is the Culturally and Linguistically Appropriate Services standards issued in 2000 (Office of Minority Health, 2001). This policy mandates certain activities (e.g., competent language assistance services and signage/materials in different languages) and encourages others (such as culturally competent care and staff diversity). The evidence for improved outcomes as a result of interpreter services is mixed, but a few studies suggest that patients with limited English proficiency who receive language assistance are more satisfied with their care and have better clinical outcomes (Smedley et al., 2003).
Cultural competence education is mandated as part of medical licensure or continuing medical education requirements in New Jersey, Washington, and California, and other states are debating similar rules (Eiser & Ellis, 2010). The accrediting authority for medical schools in the United States also has standards for cross-cultural curricula as part of undergraduate medical education (Liaison Committee on Medical Education, 2012).
Many studies of cultural competence training, not specific to Alzheimer's disease, have found that it has a beneficial effect on the attitudes, knowledge, and skills of physicians and on patient satisfaction (Beach et al., 2005). For example, 17 of 19 studies of cultural competence training for health professionals found a beneficial effect in terms of knowledge; 21 of 25 studies found that such training improved attitudes; and 14 of 14 studies showed benefits of training in improving skills. In addition, three studies found that cultural competence training of health professionals improved patient satisfaction. No definitive evidence has yet linked this training to improved health outcomes (Beach et al., 2005; Betancourt et al., 2003). One study of counseling of Black female patients showed that cultural competence improved patient adherence (Beach et al., 2005) .
The goal of the Administration for Community Living-funded Alzheimer's Disease Supportive Services Program (previously called the Alzheimer's Disease Demonstration Grants to States program) is to provide or expand support services for traditionally underserved or hard-to-serve Alzheimer's patients and their caregivers, especially minorities and rural residents. The Illinois intervention focused on older persons who spoke Arabic, Assyrian, Bosnian, Hindi, and Urdu (Wiener & Mitchell, 2007). The grant worked with the Coalition of Limited English Speaking Elderly (CLESE), an organization representing 45 Chicago-area ethnic organizations that provide services to older people. Under the grant, CLESE organizations translated materials into the appropriate languages, identified home care clients with memory loss, made home visits to try to enroll elderly people into the program, conducted caregiver training, and trained providers to screen for dementia.
A recent comprehensive review of interventions focused on Alzheimer's disease and related disorders caregivers found 18 studies, of which 11 considered cultural factors in their design; eight of those 11 studies were from the REACH initiative (Napoles et al., 2010). Cultural tailoring in these studies addressed familism (i.e., the primacy of the family over individual interests), language, bicultural and bilingual staffing, health literacy, the need for advocacy, protecting elders, and logistical barriers.
Quality of care is related to cultural competence and diversity among providers (Daker-White et al., 2002; Means, 2002). Where service providers match clients with staff according to ethnicity and language, patient outcomes may be improved (Braun & Browne, 1998). Similarly, when staff receive training in cultural awareness and sensitivity and cognitive testing is language-appropriate, this may help address some disparities (Daker-White et al., 2002).
Caregiver interventions may be more effective if delivered by staff who are not only bilingual but also bicultural (Napoles et al., 2010). For example, the REACH and REACH II projects--multisite studies to evaluate culturally tailored interventions--were effective at reducing depression and improving quality of life among caregivers (Belle et al., 2006). One of REACH's strengths is the tailoring of the intervention materials individual caregivers, and the bilingual/bicultural staff.
Outreach to Minority Communities
Another approach to addressing disparities involves targeting programs and outreach to minority populations. For example, the Alzheimer's Disease Demonstration Grants to States program provided demonstration grants to Florida, Kentucky, and the District of Columbia, that focused on African Americans (Wiener & Mitchell, 2007). For example, in the District of Columbia, the intervention focused on educational efforts conducted within church communities. They also held awareness events and developed caregiver respite programs. More recently, several of the current Alzheimer's Disease Supportive Services Program grantees, including South Carolina, California, Florida, North Carolina and Puerto Rico, are targeting ethnic or racial groups.
Another intervention aimed at reaching minority populations is the Alzheimer's Disease Research Center Satellite Diagnostic and Treatment Clinics program (National Institute on Aging, 2010). Begun in 1990, the program established satellite clinics linked with one of the 30 existing Alzheimer's Disease Centers. In recent years, satellite clinics have been established on the Choctaw nation reservation, in Harlem, at Grady Hospital in Atlanta, and in St. Louis. The Alzheimer's Disease Centers are actively involved in formulating strategies and plans to recruit diverse populations to their clinics. Strategies that have met success include improved patient coordination, increasing the personal attention patients receive, home visits, and support groups (National Institute on Aging, 2010).
Conclusions
This paper reviews the research literature on ethnic and racial disparities as it relates to Alzheimer's disease. The literature shows consistent and adverse disparities among Blacks and Hispanics compared to non-Hispanic Whites in the prevalence and incidence of Alzheimer's disease, mortality, participation in clinical trials, use of medications and other interventions, use of long-term services and supports, health care expenditures, quality of care, and caregivers.
The reasons for these disparities are not well understood, but include possible genetic differences, prevalence of other diseases that may increase the risk of Alzheimer's disease, higher rates of poverty, and lower levels of education. In addition, differences in the use of services and expenditures may be related to cultural differences and racial and ethnic discrimination. Although these disparities are well known, little is known about the effectiveness of various strategies, such as cultural competence training, to address these differences within the context of Alzheimer's disease, with almost no studies available that evaluate possible interventions.
In seeking to alleviate these disparities, one of the important points made in the IOM's Unequal Treatment report is that matching needs to services is a more important goal than trying to provide equal amounts of services to different groups (Smedley et al., 2003). Both undertreatment and overtreatment can be a problem, and it would be undesirable to insist on all patients being equally overtreated. Instead, the goal should be the right care, delivered to the right patient, at the right time, in the right setting (Fowler et al., 2011).
References
Alzheimer's Association. (2011). "2010 Alzheimer's Disease Facts and Figures." Retrieved May 11, 2012, from http://www.alz.org/documents_custom/report_alzfactsfigures2010.pdf.
Alzheimer's Association. (2012). "2011 Alzheimer's Disease Facts and Figures." Retrieved May 11, 2012, from http://www.alz.org/downloads/facts_figures_2011.pdf.
Alzheimer's Association. (2014). "2013 Alzheimer's Disease Facts and Figures." Retrieved January 21, 2014, from http://www.alz.org/alzheimers_disease_facts_and_figures.asp.
Anderson, L.M., S.C. Scrimshaw, M.T. Fullilove, J.E. Fielding, & J. Normand. (2003). "Culturally competent healthcare systems: A systematic review." Am J Preventive Medicine, 24(3 Suppl), 68-79.
Ayalon, L., & P.A. Arean. (2004). "Knowledge of Alzheimer's disease in four ethnic groups of older adults." Int J Geriatr Psychiatry, 19(1), 51-57; doi: 10.1002/gps.1037.
Beach, M.C., E.G. Price, T.L. Gary, K.A. Robinson, A. Gozu, A. Palacio, et al. (2005). "Cultural competency: A systematic review of health care provider educational interventions." Med Care, 43(4), 356-373.
Belgrave, L.L., M.L. Wykle, & J.M. Choi. (1993). "Health, double jeopardy, and culture: The use of institutionalization by African-Americans." Gerontologist, 33(3), 379-385.
Belle, S.H., L. Burgio, R. Burns, D. Coon, S.J. Czaja, D. Gallagher-Thompson, et al. (2006). "Enhancing the quality of life of dementia caregivers from different ethnic or racial groups: A randomized, controlled trial." Ann Intern Med, 145(10), 727-738.
Betancourt, J.R., A.R. Green, J.E. Carrillo, & O. Ananeh-Firempong. (2003). "Defining cultural competence : A practical framework for addressing racial/ethnic disparities in health and health care." Pub Health Rep, 118(August), 293-302.
Connolly, A., E.L. Sampson, & N. Purandare. (2012). "End-of-life care for people with dementia from ethnic minority groups: A systematic review." J Am Geriatr Soc, 60(2), 351-360; doi: 10.1111/j.1532-5415.2011.03754.x.
Cooper, C., A.R. Tandy, T. Balamurali, & G. Livingston. (2010). "A Systematic Review and Meta-Analysis of Ethnic Differences in Use of Dementia Treatment, Care, and Research." Am J Geriatr Psychiatry, 18(3), 193-203.
Crean, S., A. Ward, C.J. Mercaldi, J.M. Collins, M.N. Cook, N.L. Baker, et al. (2011). "Apolipoprotein E4 prevalence in Alzheimer's disease patients varies across global populations: A systematic literature review and meta-analysis." Dement Geriatr Cogn Disord, 31(1), 20-30.
Eiser, A.R., & G. Ellis. (2010). "Cultural competence and the African American experience with health care: The case for specific content in cross-cultural education." Academic Med, 82(2), 176-183.
Farrer, L.A., L.A. Cupples, J.L. Haines, B. Hyman, W.A. Kukull, R. Mayeux, et al. (1997). "Effects of age, sex, and ethnicity on the association between apolipoprotein E genotype and Alzheimer disease. A meta-analysis." APOE and Alzheimer Disease Meta Analysis Consortium. JAMA, 278(16), 1349-1356.
Feng, Z., M.L. Fennell, D.A. Tyler, M. Clark, & V. Mor. (2011). "Growth of racial and ethnic minorities in US nursing homes driven by demographics and possible disparities in options." Health Aff, 30(7), 1358-1365.
Fowler, F.J., C.A. Levin, & K.R. Sepucha. (2011). "Informing and involving patients to improve the quality of medical decisions." Health Aff, 30(4), 699-706.
Froehlich, T.E., S.T. Bogardus, & S.K. Inouye. (2001). "Dementia and race: Are there differences between African Americans and Caucasians?" J Am Geriatr Soc, 49(4), 477-484.
Gelman, C.R. (2010). "Learning from recruitment challenges: Barriers to diagnosis, treatment, and research participation for Latinos with symptoms of Alzheimer's disease." J Gerontol Social Work, 53(1), 94-113.
Gilligan, A.M., D.C. Malone, T.L. Warholak, & E.P. Armstrong. (2012). "Racial and ethnic disparities in Alzheimer's disease pharmacotherapy exposure: An analysis across four state Medicaid populations."American Journal of Geriatric Pharmacotherapy, 10(5), 303-312; doi: 10.1016/j.amjopharm.2012.09.002.
Gilligan, A.M., D.C. Malone, T.L. Warholak, & E.P. Armstrong. (2013). "Health disparities in cost of care in patients with Alzheimer's disease: An analysis across 4 state Medicaid populations." American Journal of Alzheimer's Disease and Other Dementias, 28(1), 84-92.
Gillum, R.F., & T.O. Obisesan. (2011). "Differences in mortality associated with dementia in U.S. Blacks and Whites." J Am Geriatr Soc, 59(10), 1823-1828.
Glymour, M.M., A. Kosheleva, V.G. Wadley, C. Weiss, & J.J. Manly. (2011). "Geographic distribution of dementia mortality: Elevated mortality rates for Black and White Americans by place of birth." Alzheimer Disease and Associated Disorders, 25(3), 196-202.
Glymour, M.M., & J.J. Manly. (2008). "Lifecourse social conditions and racial and ethnic patterns of cognitive aging." Neuropsychology Review, 18(3), 223-254.
Gray, H.L., D.E. Jimenez, M.A. Cucciare, H.Q. Tong, & D. Gallagher-Thompson. (2009). "Ethnic differences in beliefs regarding Alzheimer disease among dementia family caregivers." Am J Geriatr Psychiatry, 17(11), 925-933.
Green, A.R., D.R. Carney, D.J. Pallin, L.H. Ngo, K.L. Raymond, L.I. Iezzoni, et al. (2007). "Implicit bias among physicians and its prediction of thrombolysis decisions for Black and White patients." J Gen Intern Med, 22(9), 1231-1238.
Green, R.C., L.A. Cupples, R. Go, K.S. Benke, T. Edeki, P.A. Griffith, et al. (2002). "Risk of dementia among White and African American relatives of patients with Alzheimer disease." JAMA, 287(3), 329-336.
Gruber-Baldini, A.L., B. Stuart, I.H. Zuckerman, L. Simoni-Wastila, & R. Miller. (2007). "Treatment of dementia in community-dwelling and institutionalized Medicare beneficiaries." J Am Geriatr Soc, 55(10), 1508-1516.
Gruneir, A., S.C. Miller, Z. Feng, O. Intrator, & V. Mor. (2008). "Relationship between state Medicaid policies, nursing home racial composition, and the risk of hospitalization for Black and White residents." Health Serv Res, 43(3), 869-881.
Gurland, B.J., D.E. Wilder, R. Lantigua, Y. Stern, J. Chen, E.H. Killeffer, et al. (1999). "Rates of dementia in three ethnoracial groups." International Journal of Geriatric Psychiatry, 14(6), 481-493.
Hargrave, R., M. Stoeklin, M. Haan, & B. Reed. (1998). "Clinical aspects of Alzheimer's disease in Black and White patients." Journal of the National Medical Association, 90(2), 78-84.
Harwood, D.G., & R.L. Ownby. (2000). "Ethnicity and dementia." Current Psychiatry Reports, 2(1), 40-45.
Hernandez, S., M.J. McClendon, X-H.A. Zhou, M. Sachs, & A.J. Lerner. (2010). "Pharmacological treatment of Alzheimer's disease: Effect of race and demographic variables." Journal of Alzheimer's Disease, 19(2), 665-672.
Husaini, B.A., D.E. Sherkat, M. Moonis, R. Levine, C. Holzer, & V.A. Cain. (2003). "Racial differences in the diagnosis of dementia and in its effects on the use and costs of health care services." Psychiatric Services, 54(1), 92-96.
Janevic, M.R., & C.M. Connell. (2001). "Racial, ethnic, and cultural differences in the dementia caregiving experience: Recent findings." Gerontologist, 41(3), 334-347.
Jett, K. (2006). "Mind-loss in the African American community: Dementia as a normal part of aging." Journal of Aging Studies, 20(1), 1-10.
Liaison Committee on Medical Education. (2012). "Accreditation Standards." Retrieved May 12, 2012 from http://www.lcme.org/.
Maestre, G., R. Ottman, Y. Stern, B. Gurland, M. Chun, M.X. Tang, et al. (1995). "Apolipoprotein E and Alzheimer's disease: Ethnic variation in genotypic risks." Annals of Neurology, 37(2), 254-259.
McClendon, M.J., S. Hernandez, K.A. Smyth, & A.J. Lerner. (2009). "Memantine and acetylcholinesterase inhibitor treatment in cases of CDR 0.5 or questionable impairment." Journal of Alzheimer's Disease, 16(3), 577-583.
Mehta, K.M., K. Yaffe, E.J. Pérez-Stable, A. Stewart, D. Barnes, B.F. Kurland, et al. (2008). "Race/ethnic differences in AD survival in US Alzheimer's Disease Centers." Neurology, 70(14), 1163-1170.
Miller, S.C., J.C. Lima, & S.L. Mitchell. (2010). "Hospice care for persons with dementia: The growth of access in US nursing homes."American Journal of Alzheimer's Disease and Other Dementias, 25(8), 666-673.
Napoles, A.M., L. Chadiha, R. Eversley, & G. Moreno-John. (2010). "Developing culturally sensitive dementia caregiver interventions: Are we there yet? Am J Alzheimers Dis Other Demen, 25(5), 389-406.
National Institute on Aging. (2010). "Health Disparities Strategic Plan: Fiscal Years 2009-2013." Retrieved May 12, 2012 from http://www.nia.nih.gov/about/health-disparities-strategic-plan-fiscal-years-2009-2013/40-areas-emphasis-integration.
Noble, J.M., J.J. Manly, N. Schupf, M.X. Tang, & J.A. Luchsinger. (2012). "Type 2 diabetes and ethnic disparities in cognitive impairment." Ethnicity and Disease, 22(1), 38-44.
Office of Minority Health. (2001). "National Standards on Culturally and Linguistically Appropriate Services (CLAS)." Retrieved from http://minorityhealth.hhs.gov/templates/browse.aspx?lvl=2&lvlID=15.
Perryman, M., M. Lewis, & P.A. Rivers. (2009). "Treatment disparities in medication prescribing for Alzheimer's: disease among ethnic groups." Journal of Health Care Finance, 35(4), 64-73.
Purnell, C., S. Gao, C.M. Callahan, & H.C. Hendrie. (2009). "Cardiovascular risk factors and incident Alzheimer disease: A systematic review of the literature." Alzheimer Dis Assoc Disord, 23(1), 1-10; doi: 10.1097/WAD.0b013e318187541c.
Quiñones, A.R., M. O'Neil, S. Saha, M. Freeman, S.R. Henry, & D. Kansagara. (2011). "Interventions to Improve Minority Health Care and Reduce Racial and Ethnic Disparities Health Care." VA-ESP Project #05-225. Available at http://www.hsrd.research.va.gov/publications/esp/healthcare-disparities.pdf.
Roff, L.L., L.D. Burgio, L. Gitlin, L. Nichols, W. Chaplin, & J.M. Hardin. (2004). "Positive aspects of Alzheimer's caregiving: The role of race." J Gerontol B Psychol Sci Soc Sci, 59(4), P185-190.
Rovner, B.W., R.J. Casten, C. Arenson, B. Salzman, & E.B. Kornsey. (2012). "Racial differences in the recognition of cognitive dysfunction in older persons." Alzheimer Dis Assoc Disord, 26(1), 44-49; doi: 10.1097/WAD.0b013e3182135f09.
Samper-Ternent, R., Y.F. Kuo, L.A. Ray, K.J. Ottenbacher, K.S. Markides, & S. Al Snih. (2012). "Prevalence of health conditions and predictors of mortality in oldest old Mexican Americans and non-Hispanic Whites."Journal of the American Medical Directors Association, 13(3), 254-259; doi: 10.1016/j.jamda.2010.07.010.
Searight, H.R., & J. Gafford. (2005). "Cultural diversity at the end of life: Issues and guidelines for family physicians."Am Fam Physician, 71(3), 515-522.
Sink, K.M., K.E. Covinsky, R. Newcomer, & K. Yaffe. (2004). "Ethnic differences in the prevalence and pattern of dementia-related behaviors." J Am Geriatr Soc, 52(8), 1277-1283.
Smedley, B.D., A.Y. Stith, & A.R. Nelson. (2003). "Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care." Washington, DC: National Academies Press.
Tang, M.X., P. Cross, H. Andrews, D.M. Jacobs, S. Small, K. Bell, et al. (2001). "Incidence of AD in African-Americans, Caribbean Hispanics, and Caucasians in northern Manhattan." Neurology, 56(1), 49-56.
Teresi, J.A., D. Holmes, M. Ramirez, B.J. Gurland, & R. Lantigua. (2002). "Performance of Cognitive Tests Among Different Racial/Ethnic and Education Groups: Findings of Differential Item Functioning and Possible Item Bias Multicultural Measurement In Older Populations." New York, NY: Springer.
Vincent, G.K., & V.A. Velkoff. (2010). "The Next Four Decades--The Older Population in the United States: 2010 to 2050. U.S. Department of Commerce, Economics and Statistics Administration, Bureau of the Census.
Wendler, D., R. Kington, J. Madans, G. Van Wye, H. Christ-Schmidt, L.A. Pratt, et al. (2006). "Are racial and ethnic minorities less willing to participate in health research?" PLoS Medicine, 3(2), e19-e19.
Yaffe, K., C. Falvey, T.B. Harris, A. Newman, S. Satterfield, A. Koster, et al. (2013). "Effect of socioeconomic disparities on incidence of dementia among biracial older adults: Prospective study." BMJ, 347, f7051; doi: 10.1136/bmj.f7051.