
U.S. Department of Health and Human Services
National Study of Assisted Living for the Frail Elderly: Literature Review Update
Lewin-VHI, Inc.
February 1996
PDF Version: http://aspe.hhs.gov/daltcp/reports/litrev.pdf (98 PDF pages)
This report was prepared under contract #HHS-100-94-0024 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and Lewin-VHI, Inc. Additional funding was provided by HHS's Administration on Aging. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the office at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. The e-mail address is: webmaster.DALTCP@hhs.gov. The Project Officer was Gavin Kennedy.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
I. INTRODUCTION: BACKGROUND AND OVERVIEW OF THE ASSISTED LIVING LITERATURE REVIEW UPDATE
A. The Literature Review for the 1992 Policy Synthesis in Brief
B. The Procedure Used to Assemble the Literature Review Update
C. Findings of the Literature Review Update: A Literature Source Analysis
D. Conclusion
E. The Organization of the Literature Review Update
II. AN OVERVIEW OF ASSISTED LIVING: WHAT IS ASSISTED LIVING?
A. Definitions of Assisted Living at the Time of the 1992 Policy Synthesis
B. Current Definitions of Assisted Living
C. Suggested Typologies for Classifying the Range of Assisted Living Facilities
D. The Size and Growth of the Assisted Living Industry
III. ASSISTED LIVING -- PEOPLE, SETTINGS, AND SERVICES
A. People, Settings, and Services Described in the 1992 Policy Synthesis
B. Resident Profiles in Assisted Living Facilities and Admission and Discharge Criteria
C. Architecture as an Important Component of the Assisted Living Philosophy
D. The Services Provided by Assisted Living Facilities
E. Needs Assessments and Reevaluations
F. Staffing Needs and Staff-to-Resident Ratios in Assisted Living Facilities
IV. THE EFFECTIVENESS AND COSTS OF ASSISTED LIVING
A. 1992 Policy Synthesis Findings Regarding the Effectiveness and Costs of Assisted Living
B. The Current Literature on the Effectiveness of Assisted Living
C. Current Literature Regarding the Costs of Assisted Living
V. ISSUES AND TRENDS IN REGULATING ASSISTED LIVING
A. Regulatory Activities/Other Types of Residential Facilities for the Frail Elderly
B. Regulatory Activity Regarding Assisted Living Emerging from the States
C. Model Regulations and Accreditation
VI. FINANCING
A. Public Financing Programs and Issues Discussed in the 1992 Policy Synthesis
B. New Public Initiatives
C. Private/Public Initiatives
D. Private Initiatives
E. Emerging Issues and Concerns Regarding Financing
APPENDIX A. BIBLIOGRAPHY
LIST OF EXHIBITS
EXHIBIT 1.1: Content Analysis of Literature Since the 1992 Policy Synthesis
EXHIBIT 2.1: Formal Association Definitions of Assisted Living
EXHIBIT 2.2: Definitions of Assisted Living Used by Various Researchers in the Field
EXHIBIT 2.3: Definitions of Assisted Living from the Literature
EXHIBIT 3.1: Services Provided in Assisted Living Facilities
EXHIBIT 3.2: A Comparison of Residents' Need for Assistance
EXHIBIT 3.3: Admission and Retention Policies and Presence of at Least One Current Tenant with Selected Problems in 63 Assisted Living Settings
EXHIBIT 3.4: Reasons for Leaving Assisted Living Facilities
EXHIBIT 3.5: A Comparison of the Percentage of Facilities with Autonomy Enhancing Features from Two Studies -- in Percentage
EXHIBIT 3.6: Core Services Provided by Assisted Living Facilities: in Percentage of Facilities
EXHIBIT 3.7: Board and Care Survey Findings Regarding Services: in Percentage of Facilities, Both Licensed and Unlicensed
EXHIBIT 3.8: Other Services and Amenities Provided by Assisted Living Facilities: in Percentage of Facilities
EXHIBIT 3.9: Services Described in Non-Survey Literature Sources
EXHIBIT 3.10: Staffing Patterns in Four Major Surveys
EXHIBIT 3.11: Current Policy and Most Recent Policy Changes Made by State Legislatures
EXHIBIT 3.12: Issue-Specific Comparison of State Policies
EXHIBIT 4.1: Costs to Residents for Assisted Living
EXHIBIT 5.1: Selected Changes in Licensure Standards for "Residential Care Facilities" 1990-1993
EXHIBIT 5.2: Status of Legislative Activity in Each State
EXHIBIT 6.1: Recent State Financing Policy Changes
I. INTRODUCTION: BACKGROUND AND OVERVIEW OF THE ASSISTED LIVING LITERATURE REVIEW UPDATE
"Assisted living" is a term that generally refers to a type of care that combines housing and supportive services in a "homelike" environment and that strives to maximize the individual functioning and autonomy of residents. This document provides a review of published and unpublished literature on assisted living for the period 1992 through September, 1995. This literature review serves as an update to a review of the literature conducted for the Office of the Assistant Secretary for Planning and Evaluation (ASPE) in 1992. Like its predecessor, this review focuses on assisted living for the frail elderly.
This chapter provides a summary of the 1992 Policy Synthesis literature review, including the origin of the literature review and a discussion of the policy concerns that make assisted living for the frail elderly an increasingly important issue. A description of how the review update has been conducted, what it has yielded in numbers of articles and content, and how it has been organized are also provided in this chapter.
A. THE LITERATURE REVIEW FOR THE 1992 POLICY SYNTHESIS IN BRIEF
In 1992, Lewin-VHI conducted a Policy Synthesis on Assisted Living For the Frail Elderly for the Office of the Assistant Secretary for Planning and Evaluation (ASPE), hereafter referred to as the 1992 Policy Synthesis. The 1992 Policy Synthesis was undertaken because of policy concerns generated by a growing frail elderly population, a rapid increase in costs of delivering long-term care to that population, and growing interest in various types of supportive housing for the elderly as a potentially desirable arrangement for both housing and service delivery.
Between 1990 and 2030, the U.S. elderly population is expected to double to a total of 65 million people, an estimated 7.3 million of whom will be frail elderly. Costs of nursing home care for the elderly, both in public and out-of-pocket costs, are estimated to grow to more than $100 million annually by 2020. The special combination of housing and supportive services that characterize assisted living is identified with greater independence and dignity for the frail elderly and is bringing the fledgling assisted living industry national attention. Because of its unique physical and philosophical characteristics, assisted living may be a preferred living option for the frail elderly and, at least for some - - a less expensive alternative to nursing homes.
The 1992 Policy Synthesis was based on a review and analysis of over 350 books, reports, documents (both published and unpublished), and telephone interviews with related association representatives, policymakers, academics, and researchers. The 350 items in the 1992 bibliography span 15 years and include material on a wide range of housing options for the frail elderly. At the time that the original report was written, there were relatively few articles and reports available specifically concerning assisted living.
One result of the rapid evolution of the assisted living industry has been the voluminous increase in the number of articles and books published specifically on the topic in the years since the policy synthesis was produced. This literature review update identified 175 articles and reports related to assisted living. Although most of the 1992 literature was indirectly related to assisted living, most of literature included in this update is directly related to assisted living.
B. THE PROCEDURE USED TO ASSEMBLE THE LITERATURE REVIEW UPDATE
To conduct this literature review update, we began with an automated search of seven databases: 1) AgeLine; 2) EM Base; 3) Health Periodicals; 4) Health Plan Administration; 5) Medline; 6) Psychinfo; and 7) the Trade and Industry Index. Key words used for the database searches were: assisted living, congregate housing, board and care home, and domiciliary care. Additional automated searches were conducted by specifying the names of publications that are known to feature articles on assisted living (e.g., Provider, Spectrum, and Contemporary Long-Term Care). In addition, studies mentioned in that literature and reference lists from articles identified in the computer searches were used to identify additional sources. Finally, we asked members of our Technical Advisory Panel to help us identify articles and reports.
C. FINDINGS OF THE LITERATURE REVIEW UPDATE: A LITERATURE SOURCE ANALYSIS
We identified 175 articles and reports published or issued between January, 1992 and September, 1995. To assess recent trends in the literature, we classified the articles into nine categories, based on the source of the article: newspaper articles, provider trade publications, other trade publications, empirical research in peer-reviewed journals, consumer oriented publications, newsletters related to health and/or housing, public relations releases, business journals, and other sources (see Exhibit 1.1).
Growing interest in assisted living is illustrated by an accelerating rate of publication. We identified 108 articles and reports in the three years from January 1992, to January 1995; but we found 67 articles and reports published or issued in just the first nine months of 1995. The majority of articles (32 percent) identified since 1992 were found in provider trade publications. The second largest category of articles is "Other Sources." This category includes reports (not yet submitted for publication in peer-reviewed journals) by consultants and research organizations that typically perform "leading edge" work. The third largest category is "Other Trade Publications" (e.g., The Consultant Pharmacist ) (15 percent). "Empirical Research in Peer-Reviewed Journals" makes up the fourth largest category (10 percent).
| EXHIBIT 1.1: Content Analysis of Literature Since the 1992 Policy Synthesis | |||
| Literature Source | Number of Items: Jan 1992-Jan. 1995 | Number of Items: January-September 1995 | Total Number (% of total) |
| Newspaper Articles | 5 | 5 | 10 (6) |
| Provider Trade Publications | 30 | 26 | 56 (32) |
| Other Trade Publications | 21 | 6 | 27 (15) |
| Empirical Research in Peer-Reviewed Journals | 14 | 3 | 17 (10) |
| Consumer Oriented Publications | 3 | 0 | 3 (2) |
| Books or Newsletters Related to Health and/o r Housing | 9 | 4 | 13 (7) |
| Public Relations Releases | 4 | 4 | 8 (5) |
| Business Journals | 7 | 3 | 10 (6) |
Other Sources:
| 15 | 16 | 31 (18) |
| Total | 108 | 67 | 175 (100) |
| NOTE: Individual line percentages do not equal 100 percent due to rounding. | |||
Closer examination of the literature in the provider trade publication category, the largest of the nine categories, indicates that these articles are concerned largely with financing and the future of the industry. Fourteen of the provider trade publication articles focus on financing, another six articles review the benefits of Medicaid waivers and third-party reimbursement, six more articles are concerned with regulations, and five articles explore the future of the industry, particularly considering the growing influence of managed care.
Articles drawn from the empirical literature provide some of the most valuable information of all of the sources. The empirical literature includes various reports on the assisted living industry in general and two studies of health care utilization among those living in Continuing Care Retirement Communities (CCRCs) or assisted living facilities (Newcomer & Preston, 1994; Newcomer, Preston, & Roderick, 1995).
Articles included in the category "other trade publications" (i.e., from other than assisted living provider trade publications) are oriented to the insurance, architecture, and real estate industries. The insurance industry is concerned with long-term care insurance coverage of assisted living (Koco, 1992; Koco, 1994) and the real estate industry finds value in assisted living facilities as investment opportunities (Kramer, 1994, Real Estate Weekly, 1994).
D. CONCLUSION
The update review of the literature published since 1992 indicates a heightened interest in assisted living. In general, the articles written over the past two to three years have become increasingly more specific and more exhaustive of the subject of assisted living. Opportunities for HUD Section 232 financing and Medicaid waivers have inspired many of the recent articles and reports. In addition, research on the needs of dementia patients and "best practices" research on living arrangements for the frail elderly in general have also had an impact on recent writing on assisted living. However, a general consensus in the literature regarding definitions of assisted living and its attendant services and amenities continues to be lacking.
E. THE ORGANIZATION OF THE LITERATURE REVIEW UPDATE
With one exception, the chapter headings and topics used in the 1992 Policy Synthesis provide a structure for the literature review update. The exception is the chapter on the frail elderly and their living arrangements, which has been omitted from the update. Each chapter in the following report includes a brief summary of findings from the 1992 Policy Synthesis followed by analyses of more recent articles.
Chapter Two provides an overview of assisted living. This chapter follows the evolution of the term assisted living from the time of the 1992 Policy Synthesis to the present. It also focuses on the issues involved in defining the term assisted living, and the kinds of boundaries that may be relevant for establishing a formal definition.
Chapter Three addresses the issues of people, settings, and services. Both assisted living residents and staff are mentioned frequently in the literature covered in this chapter. In addition, we discuss the importance of environment and physical structure to the concept of assisted living. We also explore whether there is a minimum set of core services for assisted living facilities, and the extent to which these are scheduled versus non-scheduled services. The degree to which skilled nursing and ancillary services are provided is another topic of importance. Finally, the literature coverage of initial needs assessments and reevaluations is discussed.
Chapter Four addresses the issues of the effectiveness and costs of assisted living. Advocates of assisted living have maintained that assisted living facilities are a less expensive alternative to nursing homes. Empirical studies support the notion that assisted living may contribute to a different way of utilizing the health care system. This chapter also discusses different models of pricing assisted living that have developed over time, as well as the actual costs to the consumer that have been reported in the literature.
Chapter Five addresses issues involved in regulating assisted living. We focus on the contentious question of the need for industry regulation (with some attention given to the ability of the industry to self-regulate through a formalized accreditation process) and we review recent state regulatory changes. Recent changes in Certificate of Need (CON) regulations and the introduction of Medicaid waiver programs are both important topics addressed in this chapter.
Chapter Six addresses the issue of financing assisted living. Both new public initiatives and public/private initiatives are discussed in this chapter. In particular, the implications of the HUD Section 232 Mortgage Insurance Program and other new changes in institutional lending for assisted living facilities are reviewed.
II. AN OVERVIEW OF ASSISTED LIVING: WHAT IS ASSISTED LIVING?
In this chapter we provide an overview of assisted living. We discuss the conventional definition(s) of the term "assisted living" prior to the 1992 Policy Synthesis and the evolution of the term since that time. This chapter also addresses the fundamental problems in reaching a common understanding of the physical and philosophical characteristics of assisted living as well as developing profiles of assisted living residents and staff.
A. DEFINITIONS OF ASSISTED LIVING AT THE TIME OF THE 1992 POLICY SYNTHESIS
The 1992 Policy Synthesis found that the term "assisted living" was broadly used to refer to housing for the elderly with supportive services in a homelike environment. No precise definition of assisted living had developed at the time of the 1992 Policy Synthesis. In addition, other terms used to describe similar packages of services (e.g., board and care and residential care) were often used interchangeably with assisted living. At the time the 1992 Policy Synthesis was completed, federal regulations generally included assisted living facilities under the term "board and care." Most states did not use the term "assisted living" except in reference to programs for persons with mental retardation and related conditions.
Although the 1992 Policy Synthesis determined that the definition of assisted living was similar to that of board and care, the proponents of assisted living at the time asserted that a special philosophy distinguished assisted living from board and care. That philosophy was said to embody a set of principles regarding such things as maximizing the functional capability and the autonomy of the individual resident. These principles included using the environment as an aid to both independence and socialization.
By 1992, two views of the role of assisted living in long-term care had emerged. Some viewed assisted living as a type of service on a "continuum" from home care to skilled nursing facilities (SNFs). Others, those who advocate for "aging in place," saw assisted living as an approach and philosophy of care and living that could serve the needs of a very broad range of people (including those needing skilled nursing).
B. CURRENT DEFINITIONS OF ASSISTED LIVING
1. Trade Association and Organization Definitions
In the past three years, several trade associations affiliated with the assisted living industry and a number of research and policy organizations have developed formal definitions of assisted living. Exhibit 2.1 presents the formal definitions of the Assisted Living Facilities Association of America (ALFAA), the American Seniors Housing Association (ASHA), the American Association of Homes and Services for the Aging (AAHSA), the American Association of Retired Persons (AARP), the Health Care Financing Administration (HCFA), the U.S. Department of Housing and Urban Development (HUD), the National Academy of State Health Policy, National Association of Residential Care Facilities, and the National Association of State Units on Aging (NASUA).
| EXHIBIT 2.1: Formal Association Definitions of Assisted Living | |
| Association | Definition |
| American Association of Homes and Services for the Aging (AAHSA) | "Assisted living is a program that provides and/or arranges for the provision of daily meals, personal and other supportive services, health care, and 24 hour oversight to persons residing in a group residential facility who need assistance with activities of daily living and instrumental activities of daily living. It is characterized by a philosophy of service provision that is consumer driven, flexible, individualized and maximizes consumer independence, choice, privacy, and dignity." |
| Assisted Living Facilities Association of America (ALFAA) | "Assisted living is a special combination of housing, supportive services, personalized assistance and health care designed to respond to the individual needs of those who need help in activities of daily living. Supportive services are available, 24 hours a day, to meet scheduled and unscheduled needs, in a way that promotes maximum independence and dignity for each resident and encourages the involvement of a resident's family, neighbors, and friends." |
| American Seniors Housing Association (ASHA) | "A coordinated array of personal care, health services, and other supportive service s available 24 hours per day, to residents who have been assessed to need those services. Assisted living promotes resident self direction and participation in decisions that emphasize independence, individuality, privacy, dignity, and residential surroundings." |
| American Association of Retired Persons (AARP) | The following operational definition was used for the AARP's 1995 publication titled "Assisted Living and Its Implications for Long-Term Care" by Elizabeth Clemmer: "group or congregate living arrangements that provide room and board as well as social and recreational opportunities; assistance to residents who need help with personal needs and medications; availability of protective oversight or monitoring; and help around the clock and on an unscheduled basis." |
| US Health Care Financing Administration (HCFA), Medicaid Home and Community Based Waiver 1915(c) | Assisted living is one of two categories of Adult Residential Care under a 1915(c) waiver. It is defined as: Personal care and services, homemaker, chore, attendant care, companion services, medication oversight (to the extent permitted under State law), therapeutic social and recreational programming, provided in a licensed community care facility, in conjunction with residing in the facility. This service includes 24 hour on site response staff to meet scheduled or unpredictable needs and to provide supervision of safety and security. Other individuals or agencies may also furnish care directly, or under arrangement with the community care facility, but the care provided by these other entities supplements that provided by the community care facility and does not supplant it. Care is furnished to individuals who reside in their own living units (which may include dually occupied units when both occupants consent to the arrangement) which may or may not include kitchenette and/or living rooms as well as bedrooms. Living units may be locked at the discretion of the client except when a physician or mental health professional has certified in writing the client is sufficiently cognitively impaired as to be a danger to self or others if given the opportunity to lock the door. (This requirement does not apply where it conflicts with the fire code.) Each living unit is separate and distinct from each other. The facility must have a central dining room, living room or parlor, and common activity center(s) (which may also serve as living rooms or dining rooms). Routines of care provision and service delivery must be client-driven to the maximum extent possible. Assisted living services may also include:
However, nursing and skilled therapy services are incidental, rather than integral to the provision of assisted living services. Payment will not be made for 24-hour skilled nursing care or supervision. FFP is not available in the cost of room and board furnished in conjunction with residing in an assisted living facility. Payments for adult residential care services are not made for room and board, items of comfort or convenience, or the costs of facility maintenance, upkeep, and improvement. Payment for adult residential care services does not include payments made, directly or indirectly, to members of the recipient's immediate family. |
| US Department of Housing and Urban Development (HUD) | Assisted living means a public facility, proprietary facility, or facility of a private nonprofit corporation that is used for the care of the frail elderly, and that:
|
| National Academy of State Health Policy | NASHP declined to provide one concise definition of assisted living. However, extensive commentary on all aspects of services, admission and discharge criteria, and site standards make the "Guide to Assisted Living and State Policy" a definition in itself. |
| National Association of Residential Care Facilities | Residential care facility means a home or facility of any size, operated for profit or not-for-profit, which undertakes through its owner/s or management to provide food, housing and support with activities of daily living and/or protective care for two or more adult residents not related to the owner or administrator. Residential care homes are also known as assisted living facilities, foster homes, board and care homes, sheltered care homes, etc. |
| National Association of State Units on Aging (NASUA) | NASUA subscribes to a definition of assisted living which acknowledges the deep desire of America's elders to reside in their own homes or in a homelike environment. Accordingly, the Association views assisted living as referring to a homelike congregate residence providing individual living units where appropriate supportive services are provided through individualized service plans. Assisted living is first and foremost a home in which residents' independence and individuality are supported and in which their privacy and right to self-expression are respected. |
Most of the definitions from the nine organizations listed above refer to the "aging-in-place" philosophy of assisted living. The central tenet of that philosophy, the notion that the resident's dignity and autonomy are paramount, is made clear in most of these definitions. For example, the AARP definition emphasizes that the "aim of assisted living is to enhance the capabilities of frail older persons so that they can live as independently as possible in a home-like atmosphere. Assisted living accomplishes this through both building design and care practices that facilitate independent functioning and reinforce residents' autonomy, dignity, privacy, and right to make choices" (Clemmer, 1993).
The definitions from AAHSA, AARP, ALFAA, ASHA, and HCFA all specify that supportive services should be available 24-hours a day. The 24-hour requirement is significant because it indicates a facility's commitment to respond to unscheduled needs for assistance. In contrast, the National Association of Residential Care Facilities and HUD definitions do not mention any tenets of the assisted living philosophy nor do they specify when supportive services should be available.
2. Assisted Living/Seniors Housing Experts Definitions
Experts in the assisted living field increasingly include mention of a special assisted living philosophy in their working definitions (see Exhibit 2.2). Tangible evidence and results of this philosophy (e.g., "the dignity of risk" or "individual choice") are very difficult to quantify in survey research. In recognition of this, Kane and Wilson, two of the researchers most identified with the idea that assisted living includes a special philosophy of care, used a minimalist definition in their 1993 study for AARP.
| EXHIBIT 2.2: Definitions of Assisted Living Used by Various Researchers in the Field | |
| Researcher | Definition |
| Rosalie A. Kane & Robert L. Kane, 6/7/95, JAMA | "One attractive emerging option is assisted living, which under some state licensure features single-occupancy apartment units with full bathrooms and kitchenettes. Such programs serve three meals a day and provide on-site staff. Individually planned care is brought to the consumers' own apartments." |
| Rosalie A. Kane & Keren Brown Wilson, 1993, Assisted Living in the United States | "Assisted living is any group residential program that is not licensed as a nursing home, that provides personal care to persons with need for assistance in the activities of daily living (ADL), and that can respond to unscheduled need for assistance that might arise." |
| Victor A. Regnier, 1994, Assisted Living Housing for the Elderly | "Assisted living is a long-term care alternative which involves the delivery of professionally managed personal and health care services in a group setting that is residential in character and appearance in ways that optimize the physical an d psychological independence of residents." |
| Joann Hyde, 1995, draft report of People With Dementia: Toward Appropriate Regulation of Assisted Living and Residential Care Settings | "Assisted living is a service-rich residential environment designed to enable individuals with a range of capabilities, disabilities, frailties and strengths to reside in a homelike setting as long as possible." |
| Donna Yee, August 1995, cited in Currents in reference to a Brandeis University study. | Assisted living is defined in the study as "programs that offer congregate housing and supportive services with explicit or implicit commitment to respond to individual preferences for help with health-care access, personal care and household maintenance." |
3. General Article Definitions
A number of the general articles identified from 1992 to 1995 also provide definitions of assisted living. These definitions are found in Exhibit 2.3, where they are organized by date. In general, definitions appear to build on past work in a field, and this literature review update is no exception. One can follow the progressive development over time of the definition from a very vague listing of services to a much richer treatment of the philosophy of assisted living. While one might expect to observe a convergence on the definition of assisted living used in the literature, this has not yet been the case.
Assisted living is described in most provider trade publications as a residential option for the elderly who need some help with activities of daily living (ADLs) and possibly some minimal nursing care. Most definitions from the literature refer to the provision of supportive personal care services and many explicitly mention either that assisted living residents do not require the intensity of care found in nursing homes or that residents have "limited medical needs" or require "minimal medical care."
| EXHIBIT 2.3: Definitions of Assisted Living from the Literature | ||
| Date | Source = Author & Publication | Definition |
| 12/4/92 | McCarthy, Wall Street Journal | "A new style of housing for frail elderly people who don't have serious medical problems." |
| 1/3/93 | Diesenhouse, NY Times | "Usually small developments (that) consist of private or semiprivate apartments, from studios with no kitchens to fully equipped one or two bedrooms...help (is) provided to residents in the form of housekeeping and meal services and minor medical care. Also provided is personal care such as getting out of bed, bathing, and dressing." |
| 1/3/93 | Stuart, NY Times | "Residents live independently...while receiving 24-hour supervision, assistance in daily living, meals, housekeeping, transportation, and recreational programming. Minimum health care or nursing assistance is provided as needed." |
| 2/93 | Rajecki, Contemporary Long Term Care | Housing and Community Development Act of 1992: Assisted living facilities are "public, proprietary or private/nonprofit facilities that: Are licensed and regulated by the state; make available to residents supportive services to assist residents in carrying out activities of daily living; and provide separate dwelling units for residents, each of which may contain full kitchen and bathroom." |
| 4/93 | PR Newswire | "Service-intensive housing for ...frail but functional seniors." |
| 8/6/93 | Garbarine, New York Times | "Hotel style rental project for elderly people who may need help with daily chores but do not need constant medical care." |
| 8/93 | Provider | Residential care setting "noted for its low-cost, homelike environment for individuals needing limited assistance and falls on the continuum between boarding homes and skilled nursing facilities. It is a social model of health care that maximizes independence while providing limited non-medical care and services." |
| 8/93 | Geran, Interior Design | Describes a CCRC " Assisted Living unit where nursing staff and doctors provide medical care." |
| 1993 | Older Women's League | Assisted living "covers a wide range of licensed an d unlicensed facilities: residential care facilities, adult congregate living facilities, personal care homes, retirement homes, board and care homes. These facilities offer housekeeping, meal services, personal care and minor medical care." |
| 1/94 | Walser, Harvard Health Letter | One of three types of care provided in continuing care retirement communities; a type of care for seniors "needing help getting out of bed, bathing, dressing, eating, walking, or going to the bathroom." ALFs provide access to 24-hour help. |
| 2/94 | Riegel, New Orleans Magazine | "Designed for the elderly who are still able to care for themselves....They offer pleasant, safe surroundings in which the elderly can live independently. But they also provide such services as nursing care, transportation and housecleaning as needed." |
| 3/94 | Kramer, Pension World | "A senior-living complex with physical feature s designed to assist the frail elderly, with staff personnel and programs that assist residents with the activities of daily living." |
| 6/5/94 | Cerne, Hospitals & Health Networks | "Suited for patients who, for a variety of reasons, cannot live alone but don't need the 24-hour skilled medical care provided by nursing homes." |
| 4/2/94 | Davis, Milwaukee Business Journal | Assisted living draws from two populations: 1) people who do not require continuous medical care, but occasionally need someone to help them get dressed, or to remind them to take medication" and 2) "healthy and active seniors who simply want to shed some of the burdens of home ownership." |
| 6/5/94 | Cerne, Hospitals & Health Networks | "Suited for patients who, for a variety of reasons, cannot live alone but don't need the 24-hour skilled medical care provided by nursing homes." |
| 7/7/94 | PR Newswire | Subsumed under congregate housing; "typically provide three daily meals and personal care as needed." |
| 8/15/94 | Wilson, Brown University Long term Care Quality Letter | "An alternative model of supportive housing.... In Oregon, private apartments are shared only by choice. Everyone agrees that assisted living should provide at least congregate services (meals, housekeeping, laundry, transportation, group activities)." |
| 8/94 | Building Design & Construction | "A communal residence for senior citizens who don' t require the 24-hour care of nursing homes, but who nevertheless need some assistance with the activities of daily living." |
| 1/5/95 | Pressler, Washington Post | "Bed-and-breakfast-like homes provide senior citizens with shared or private apartments, meals in a communal dining room, daily housekeeping services and limited medical care." |
| 12/94 | Folkemer, Intergovernmental Health Policy Project | "A care option generally designed around individualized service contracts and "managed risk." |
| 1/95 | Pfeiffer, Postgraduate Medicine | "Residential facilities that provide supervision and care for individuals who have lost some degree of self-care capacity...these facilities fill a niche between independent living arrangements and the full supervised care offered in nursing homes." |
| 1/9/95 | Vick, The Washington Post | "Assisted living facilities grew out of boarding homes -social places-and have prospered by offering the "frail elderly" greater independence in exchange for less security than assured by the rigid, essentially medical boarding of a nursing home." "What the industry calls 'assisted living,' the state knows variously as 'board and care,' 'sheltered living,' 'protect homes,' and 'domiciliary care,' either 'registered' or 'licensed.'" |
| 1-2/95 | Chisholm and Hahn, Geriatric Nursing | "Domiciliary care is a residential rehabilitation and health maintenance center for veterans who are ambulatory and can care for themselves, but who because of medical or psychiatric disabilities are unable to live independently. They reside in a structured, therapeutic, homelike environment." |
| 2/95 | Olson, Provider | "An ALF (assisted living facility) is defined by HUD as a not-for-profit or for-profit facility for the frail elderly that is licensed and regulated by the state, or, if there is no state law providing for such licensing and regulation, by the municipality or other political subdivision in which the facility is located. The ALF may be freestanding or a part of a complex of other facilities." |
| 4/19/95 | Business Wire | "Assisted living apartments are provided for people who need occasional to frequent help with activities of daily living." |
| 4/28/95 | Bruck and Widdes, Tampa Bay Business Journal | "The concept is simply to make senior citizens feel like they are at home rather than in an institution. The dwellings provided by the company come with a yard, a porch and a kitchen. Residents are encouraged to eat in a common dining area, which doubles as a game room and meeting area." |
| 5/95 | Braga, Nursing Homes | "there are few, if any, alternatives for patients in the middle of the spectrum-those who are unable to live independently, yet don't require skilled nursing care...because assisted living residences are not bound by the same regulations that govern nursing homes, we have the opportunity to be more flexible and creative with respect to physical environment and delivery of services....Each facility houses 50 to 60 residents, yet has a cozy, informal environment that is as home-like as possible." |
| 6/23/95 | PRNewswire | "Assisted living is an alternative lifestyle for individuals not requiring the medical surroundings of nursing home care." |
| 8/8/95 | PR Newswire | "Assisted living services provide greater opportunities for seniors to live independently through a selection of services such as assistance at meal time or wit h bathing." |
Although there is some recognition of the significance of physical environment in assisted living (Diesenhouse, Rajecki, Provider, Riegel, Kramer, Wilson, Pressler, Chisolm and Hahn, Bruck and Widdes, and Braga), there is less indication in the literature of a general understanding of the assisted living philosophy. Only the articles authored by Folkemer, Vick, Braga, and the editors of Provider, are explicit in their explanations of the importance of preserving the dignity and independence of assisted living residents through architectural and design strategies.
Despite similarities among the association definitions and the literature definitions of assisted living, there is little consensus concerning the details of care provision and the importance of an assisted living philosophy of care.
C. SUGGESTED TYPOLOGIES FOR CLASSIFYING THE RANGE OF ASSISTED LIVING FACILITIES
The 1992 Policy Synthesis classified assisted living facilities into three types: public housing, units in continuing care retirement communities (CCRCs), and freestanding facilities. This classification system was used because the available data and information were organized in this fashion.
Another typology, conceptualized by Lawton (1977; 1980) and further explained by MacDonald, Remus, and Laing's (1994) research with a small sample of elderly, contrasts "constant" and "accommodating" models of health and housing that can be used with assisted living. The constant model entails admission and discharge policies and procedures developed by management personnel. The environment facilitates resident independence, but does not change over time. The accommodation model is similar to an "aging in place" model where the environment changes over time and residents stay in the facility until they need 24-hour nursing care. MacDonald and associates conducted focus group interviews with 29 subjects from a random stratified sample to determine the subjects' attitudes toward housing. All subjects emphasized the importance of maintaining their independence and the importance of continuity of care. In attitudes toward housing, however, the researchers found that the subjects divided into two groups, based on health and disability. Those subjects who were in poorer health and who were more disabled favored adding services and modifying the environment, or the accommodating model. Those in better health and less disability favored the constant model where services provided and the environment would remain constant over time.
Heumann and Boldy (1993) have used another typology to classify international models of assisted living for low income and frail elderly. This typology has two primary categories: 1) "predisposing conditions" and 2) "environmental dimensions." Predisposing conditions are further divided into four secondary characteristics: 1) social values under which programs are conceived; 2) the extent of government resource commitment; 3) government operational level; and 4) the mix of program ownership and management, public or private. Social values includes four subcategories, ranging from the rejection model, the social service model, and the participation model, to the self-actualization model. Environmental dimensions have two secondary characteristics: 1) program support emphasis and 2) lifestyle emphasis. The program support emphasis is further categorized into four continua, ranging from the housing to community service focus, conventional to sheltered housing design, visiting to on-site service delivery, and incremental to holistic management. Lifestyle emphasis assesses the extent to which the neighborhood and facility are segregated or integrated by age and whether the units are private or communal. In an earlier work, Heumann and Boldy (1982) developed a way of categorizing and simplifying program variations by using three continua describing levels of services, privacy, and community sizes, respectively. The service continuum ranges from the minimal service model with no on-site support to the service rich model with full on-site services, including nursing staff. The privacy continuum ranges from a model with conventionally designed private units with no communal space to a model with only bedrooms remaining private. The size continuum ranges from one to ten units, which makes support staff costs prohibitive, to multiples of 100 plus units managed by a bureaucracy.
A typology developed by Gold and associates (1991) for nursing home special care units for seniors with cognitive impairment rates facilities dichotomously on 27 key variables, many of which are subjective (e.g., inside ambiance). The authors maintain that "each type represents a unique, model constellation of patient care, staff, and administrative characteristics of the settings included in it" (Gold et al., 1991, p. 470). The typology includes eight categories, including "ideal, uncultivated, heart of gold, rotten at the core, institutional, limited, conventional, and execrable."
An additional typology has been introduced by Mollica et al. in their May 1995 report for the National Academy for State Health Policy. The three models identified in that study were "institutional or board and care," a new "housing and services" model, and a "purely service-oriented" model. In the first model, aging-in-place is addressed in both traditional board and care facilities and in frail elderly housing projects. Facilities that fit into this model have residents with a range of ADL and other service needs; some residents may be totally independent and others may require significant assistance with ADLs. States which separate the housing and service components of assisted living provide greater flexibility to residents seeking to age-in-place, but they do not address the institutional character of traditional board and care facilities that still exist in many states. The service delivery model licenses or contracts with the agency providing assisted living services that may be provided in housing settings. Mollica et al. (May, 1995) included a chart in their report which classifies states according to the model that best characterizes current state policy. (See Exhibit 5.2 in Chapter 5 of this document.)
D. THE SIZE AND GROWTH OF THE ASSISTED LIVING INDUSTRY
The lack of a generally accepted definition of assisted living and lack of systematic counting of those facilities in large government surveys currently preclude precise counts of the current number of assisted living facilities, the current assisted living resident population, and the extent of industry growth.
Although the literature published since 1992 contains assertions that the number of assisted living facilities is increasing (e.g., Buss, 1994; Gamzon, 1993; Cook, January 1995; Nichols, January 1995; Vick, January 9, 1995; Currents, May 1995; Evans, September 18, 1995; Kane, 1995) there has been little concrete data available to assess growth systematically.
A 1993 "Overview of the Assisted Living Industry," produced by ALFAA and Coopers & Lybrand reports that "there may be as many as 65,372 Assisted Living Type facilities, housing between 104,803 and a million residents, depending on how assisted living is defined." The sources cited by the Overview include a 1992 study by Coopers & Lybrand and the 1992 Policy Synthesis. The 1992 Policy Synthesis estimate, from which the number of units mentioned above is taken, is drawn from a 1990 study of all potential licensed board and care facilities conducted by Lewin-ICF for ASPE. (This study did not count unlicensed board and care homes.) A number of articles included in this literature review update cite the Lewin-VHI 1992 Policy Synthesis or the 1993 ALFAA Overview. Thus, estimates of assisted living facilities appear to be circular rather than systematic.
Modern Healthcare, a trade publication, has conducted at least two surveys of multi-unit providers. Results indicate an increase of six percent in CCRCs operated by respondents to the survey from 1992 to 1993 (Pallarito, 1994). The survey reports on the number of CCRCs, as well as independent living, assisted living, and nursing home beds. Of the 87 entities reporting, 21 increased the number of their assisted living beds, while seven decreased the number of their assisted living beds. The total number of assisted living beds in 1993 among these 87 CCRCs was 12,369. Pallarito's 1995 article in Modern Healthcare titled "Assisted Living Captures Profitable Market Niche," indicates that there may be somewhere between 30,000 and 40,000 assisted living providers today.
A recent Consultant Pharmacist article similarly estimates that there are between 40,000 and 65,000 providers serving one million people. This article cites estimates that the assisted living target population is expected to increase sixfold over the next 25 years, when a large portion of the baby boom generation enters their seventies. It also cites predictions that more than seven million frail elderly persons will be candidates for assisted living by the year 2020 (Nichols, January, 1995). The Washington Post has also reported "industry estimates" of 40,000 assisted living providers in the United States, serving 1 million people. The Post, reflecting interviews with those in the industry, notes that the industry is expected to grow to serve three times that number of older people within the next ten years. Other experts have predicted that the industry will grow to become a $25 billion-revenue producing industry by the year 2000 (J. Baker, as cited in Pallarito, 1995).
III. ASSISTED LIVING -- PEOPLE, SETTINGS, AND SERVICES
This chapter focuses on the people, settings, and services of assisted living. We discuss resident profiles and review the literature in terms of admission and discharge conventions for assisted living residents. In addition, we summarize the literature on staff profiles for both professional and non-professional employees of assisted living facilities, review the literature concerning the importance of the physical environment in the philosophy of assisted living, and review the types of services that the literature associates with assisted living care packages. Furthermore, we investigate whether these services are described as scheduled or non-scheduled, bundled or unbundled. The presence or absence of skilled nursing and ancillary services and the scheduling of those kinds of services are additional issues addressed in the literature which we note in this chapter.
A. PEOPLE, SETTINGS, AND SERVICES DESCRIBED IN THE 1992 POLICY SYNTHESIS
1. Admission Criteria
The 1992 Policy Synthesis found that there was little agreement in the literature on eligibility conventions for assisted living residents or on the person or persons who should make those kinds of determinations. The literature generally indicated that assisted living was appropriate for medically stable individuals who did not require 24-hour nursing supervision or professional medical care. However, many authors disagreed about whether cognitively impaired seniors or individuals with a number of physical disabilities would be best served in assisted living facilities.
The 1992 Policy Synthesis identified three central criteria used in screening new applicants for assisted living: income, age, and functional capability. Public facilities targeted low income populations, while non-public facilities appeared to target wealthier seniors. With respect to age, we found that: HUD had no age eligibility restrictions; most state-funded programs were limited to residents over 60 years old; and a number of CCRCs were limited to residents over 62 years old, while other CCRCs were limited to 65 years as a minimum age. Criteria on functional disability ranged widely, depending on the type of facility and/or the location of the facility. For instance, in 1992, HUD's Congregate Housing Services Program (CSHP) required that residents need assistance in three or more ADLs/IADLs, including eating or preparing meals and must have no informal support network (Struyk, 1989). Although most state-funded facilities required that seniors have impairment in at least one ADL task, Massachusetts and New Jersey admitted seniors who were socially isolated but functionally intact. The 1992 Policy Synthesis pointed out that the Fair Housing Amendments Act of 1988, by including disabled individuals as a group protected from housing discrimination, and the Americans with Disabilities Act could have significant ramifications for assisted living and could have a direct effect on eligibility requirements.
The 1992 Policy Synthesis determined that transfer decisions appeared to be made systematically within assisted living facilities but the parties responsible for making transfer decisions varied between facilities. For instance, in public facilities housing managers generally performed the initial assessments, while in CCRCs and private assisted living facilities case managers were more likely to perform initial screening assessments. In some CCRCs and private facilities, a facility physician or nurse performed the assessment.
2. Services
Services provided by assisted living facilities varied widely across facilities, as shown in Exhibit 3.1, which is taken from the 1992 Policy Synthesis. This table synthesizes services provided in four surveys: 1) a survey of Section 202 Housing (Gayda & Heumann, 1989); 2) a seven state survey of 602 non-Medicaid certified facilities (Moon et al., 1989); 3) a survey of 200 assisted living facilities (Seip, 1990); and 4) a survey of 10 assisted living facilities in Florida (Kalymun, 1990). These surveys demonstrate that there was little consensus on a core set of services.
3. Staff
The 1992 Policy Synthesis determined that staffing patterns, ratios, and professionalism also varied widely across assisted living facilities. Although it was difficult to generalize, the 1992 Policy Synthesis found that staff roles in assisted living facilities were less differentiated than those found in facilities providing more traditional care. The literature described the following staff positions: housekeepers, kitchen workers, maintenance personnel, transportation staff, and managerial and clerical staff. A 1992 American Health Care Association (AHCA) study found that the average member residential care facility who typically had 50 beds employed 3 management personnel, 5 nurses, 13 aides, 9 dietary staff, and 4 housekeepers. The AHCA member facilities also reported employing a number of other types of staff: an activities director (82 percent), a pharmacy consultant (70 percent), a RN consultant (60 percent), a dietitian (45 percent), a physical therapist (36 percent), and a social worker (46 percent). With regard to staff ratios, Moon (1989) found a mean staffing ratio of 3.2 residents per staff member in the seven states studied with a staff to resident ratio range from 2.8 to 4.7.
| EXHIBIT 3.1: Services Provided in Assisted Living Facilities | ||||
| Author | Gayda and Heumann(1989) | Moon, M., et. al.,(1989) | SEIP(1990) | Kalymun(1990) |
| Sample | Approximately 2,000 Section202 Housing Facilities Across Nation | Seven State Survey of 602 Non-Medicaid Certified Facilities, Licensed or Non-licensed That Provided Room and Board, Personal Care and Protective Oversight to Four or More People | A Survey of 200 Assisted Living Facilities Across the United States | 10 Assisted Living Facilities Certified as Adult Congregate Living Facilities in Florida |
| SERVICES | ||||
| Housekeeping | 18% | 100% | 100% | |
| Transportation | 22% | 65% | 91% | 100% |
| Personal laundry | - | 97% | 100% | |
| Personal Care | 20% | - | - | |
| Grooming | - | 59% | 92% | 100% |
| Dressing | - | 62% | 93% | 100% |
| Bathing | - | 82% | 95% | 100% |
| Toileting | - | 42% | 78% | - |
| 3 Meals/Day | 50% | 97% | 100% | |
| Assist with Medications | - | 96% | 100% | |
| Physical Therapy | - | 71% | - | |
| Psychological Counseling | - | 61% | - | |
| 24-Hour Licensed Nurse | - | 70% | - | |
| * 50 percent of the states offer meals; the number per day is not specified. | ||||
B. RESIDENT PROFILES IN ASSISTED LIVING FACILITIES AND ADMISSION AND DISCHARGE CRITERIA
The literature from 1992 to the present provides some general information about the residents of assisted living facilities, but provides little information about who is eligible, how and by whom eligibility is determined, or who is excluded from assisted living. Most of the information about residents of assisted living facilities comes from two studies: 1) a study by ALFAA and Coopers & Lybrand (1993), reported in An Overview of the Assisted Living Industry and 2) the Kane and Wilson (1993) study of assisted living for the American Association of Retired Persons (AARP) reported in Assisted Living in t he United States: A New Paradigm for Residential Care for Frail Older Persons.
The study by ALFAA and Coopers & Lybrand (1993) is a survey of assisted living providers conducted in the Spring of 1993. The data come from 201 facilities, representing 6,119 units in 25 states. For-profit assisted living facilities represented 75 percent of the sample, 4 percent were publicly-held and 21 percent were non-profit.
The Kane and Wilson (1993) study had two components: a national study of assisted living and a study of assisted living in the state of Oregon. The national study included interviews with a national sample of administrators of 63 assisted living facilities; 65 percent of the facilities were for-profit, 35 percent were non-profit programs. In most cases, this study was restricted to facilities with 15 or more residents. Oregon was studied separately because the state has "gone further than any other in defining assisted living through regulations, encouraging purpose-built assisted living programs through incentives for developers, and providing a reimbursement source for the care component of the program" (Kane & Wilson, 1993, p. 51). The Oregon sample includes 20 of the 22 licensed programs in the state with 947 tenants in residence at the time of the study. Data from the national study and the Oregon study are reported separately by Kane and Wilson and are treated separately in this review.
1. Vital Statistics: Average Age, Gender, and Marital Status
The ALFAA study provides a resident profile drawn from the assisted living facilities responding to their survey: 79 percent of residents are female with an average age of 85; male residents average 83 years (ALFAA and Coopers & Lybrand, 1993). In their national study, Kane and Wilson (1993) found that the average age for residents was 83 years. The Oregon residents were predominately female (75 percent) with an average age of 85, and 97 percent were unmarried. In a study of the relationship of assisted living residents to health care utilization, Newcomer and Preston (1994) found that the average age of residents in two CCRCs was 82.2 years and that 76.7 were female. In a second study the average age at entry was 79.3 years and 72.4 percent were female (Newcomer, Preston, & Roderick, in press).
In addition to the aforementioned studies, Coopers & Lybrand in conjunction with the American Seniors Housing Association have produced The State of Seniors Housing 1994 (1995), a project that surveyed senior housing executives in congregate housing, CCRC's, and assisted living facilities for information on financing and development, resident characteristics, and financial performance indicators. This study found that assisted living facilities generally serve a population of single females in their early 80's. The prototypical assisted living resident was an 81.8 year-old female. In fact, only 19 percent of assisted living residents were male, according to the findings of this study.
Finally, the vast majority of residents (more than 97 percent) in these facilities are unmarried or are not living with their spouse.
2. ADL Impairment
The ALFAA study found that assisted living residents have a mean number of 3.06 ADL impairments and 42 percent have some cognitive impairment. They also found that typical residents were females needing "moderate or heavy care." The residents frequently needed help with ambulating, medicines, bathing and/or dressing and were forgetful. Kane and Wilson report that a summary classification scheme used by the State of Oregon to classify Medicaid clients determined that the Oregon sample had more physical and cognitive impairment than the national sample studied by Kane and Wilson, as shown in Exhibit 3.2.
| EXHIBIT 3.2: A Comparison of Residents' Need for Assistance | ||
| Residents' Need for Assistance | National Residents Sample | Oregon Residents |
| Low Need for Assistance | 25 percent | 10 percent |
| Medium Need for Assistance | 50 percent | 61 percent |
| Medium Need for Assistance | 25 percent | 29 percent |
| SOURCE: Kane and Wilson, 1993 | ||
3. Admission and Discharge
a. Factors Influencing Admission and Discharge Patterns
Researchers report in recent literature that, among other things, age at entry into a senior housing facility "significantly affects the likelihood of assisted-living and nursing unit use in all residents' models..." More extensive analysis of admission and discharge patterns between assisted living facilities and nursing units is greatly needed in order to provide a more comprehensive picture of the role that assisted living plays in the larger chronic care industry, and to inform interested parties about the impact of transfers on total costs. The effect of transfers on residents' health care utilization will be discussed in the section on effectiveness of assisted living (Newcomer, Roderick, and Preston, June 1995).
The development of widely applicable admission and discharge criteria is an important issue facing the assisted living industry. Some industry experts believe that as much as 20 to 30 percent of nursing home residents would be more appropriately served in assisted living communities (Clipp, 1995). The magnitude of that estimate suggests that these so-called "inappropriate" placements may have a significant impact on overall health care costs for the frail elderly in this country.
b. Source of Admission
The ALFAA-Coopers & Lybrand study (1993) found that more than one-half of the residents lived in their own homes prior to admission to the assisted living facility (57 percent) while 16 percent came from living with their family, 14 percent came from a retirement community, and 13 percent came from a nursing home.
To better understand how elders are referred to residential care settings, one researcher has recently studied patterns of decision making for seniors' transfers into residential care facilities (Bear, 1993). Using a sample of 86 primary caregivers of elderly residents newly admitted to central Florida residential care settings, this study examined the admission patterns of residents described as unable to stay in their current residence (prior to residential care placement) and their subsequent referral to the residential care facility. The majority (68.5 percent) of seniors were labeled "out-of-place" and 75.6 percent were referred by informal primary caregivers. Physicians labeled 25.6 percent of the seniors out-of-place and referred 15.1 percent of the seniors to the residential care setting. Health professionals were more likely to do the labeling during a hospitalization. The study found that caregivers of this sample of residents differed from a national sample of caregivers; they were more frequently white, younger, and better educated than the national sample.
ALFAA's survey reports somewhat different referral patterns in its Overview of the Assisted Living Industry: 25 percent of the residents in the facilities responding to the survey were referred by family members, while 20 percent were referred by hospitals, 14 percent were referred by physicians, and 14 percent were self-referrals.
c. Admission and Retention Criteria
Some useful background to the discussion of admission criteria for assisted living facilities is provided in a recent national study on board and care homes (Hawes, et al., 1995). The authors do not explicitly describe a set of characteristics or eligibility requirements for board and care residents, except that such residents tend to need temporary, part-time nursing care and some assistance with ADLs. In terms of discharge conventions, 44 percent of licensed board and care homes and 56 percent of unlicensed board and care homes (assisted living facilities would most likely fall under this category) reported that they would discharge a resident who needed nursing care for more than 14 days. The discharge sites listed were hospitals (acute or Veterans Administration) and nursing homes (Hawes et al., 1995, p. 17).
The Kane and Wilson (1993) national study also examined admission and retention policies for the assisted living facilities they studied. All but one of the 63 facilities surveyed would admit an individual who was mildly confused. All 63 facilities would retain a resident who was mildly confused and all had at least one mildly confused resident. In contrast, 45 of the 63 facilities would admit an individual with moderate confusion and 55 of the 63 would retain an individual with moderate confusion. Fifty-three out of the 63 facilities actually had residents with moderate confusion. In addition, only 12 of the 63 facilities would admit individuals using a ventilator and 12 of the 63 would retain a resident on a ventilator. Of those 12 facilities, only three actually had one or more residents on a ventilator. Exhibit 3.3 presents the table on admission and retention policies from the Kane and Wilson study. Although the authors found that a certain number of facilities would admit and/or retain individuals conditionally with selected conditions, these facilities have been omitted from the table.
State regulations increasingly influence who is eligible to become an assisted living resident as well as the length of time that a resident may remain in a particular facility. The recent Guide to Assisted Living and State Policy (Mollica et al., May, 1995) provides some important analysis of admission and discharge regulations. This report indicates that 17 states have admission criteria that admit only those residents who require nursing facility level of care or skilled services (Mollica et al., 1995, ix). However, it seems that resident policies which prohibit anyone needing nursing home level of services from being served are being reexamined. As Mollica et al. argue, "assisted living has been developed as an alternative for people who qualify for placement in a nursing facility in most states" (Mollica et al., p. 45).
| EXHIBIT 3.3: Admission and Retention Policies and Presence of at Least One Current Tenant with Selected Problems in 63 Assisted Living Settings | |||
| Condition or Problem | Will Admit | Will Retain | Current Have Residents with Condition |
| Wheelchair bound | 56 | 57 | 50 |
| Electric Cart | 46 | 46 | 22 |
| Incontinent | 55 | 60 | 56 |
| Chair Bound | 19 | 24 | 28 |
| Help Transfer | 32 | 42 | 32 |
| Help Feed | 28 | 32 | 24 |
| Mildly confused | 62 | 63 | 63 |
| Moderately confused | 45 | 55 | 53 |
| Using catheter/ostomy | 53 | 56 | 31 |
| Using Oxygen | 55 | 49 | 44 |
| Using Ventilator | 12 | 12 | 3 |
| With Behavior Problems | 38 | 46 | 42 |
| (Kane & Wilson, 1993) | |||
Currently, the State of Virginia does not allow bedfast residents to enter assisted living facilities, although those residents who become bedfast after admission to the facility may remain. In addition, the state of Missouri requires that assisted living residents be capable of walking within 45 days of admission (Provider, August, 1993). Regulations prepared for the state of Florida prohibit residents with certain conditions from remaining in assisted living facilities (called extended congregate care in Florida). These conditions include: needing 24-hour nursing supervision, being bedridden for more than two consecutive weeks, dependency in four or more ADLs, or being unable to make simple decisions due to cognitive impairment (Rajecki, 1992).
Mollica et al. also contributed some valuable information on the topic of admission criteria. Their Guide to Assisted Living and State Policy specifically differentiated state licensing rules that specify admissions criteria from the program requirements that establish such criteria. In addition, Mollica et al. explored two important distinctions in the determination of admissions criteria. Their study explains that state licensure rules often establish guidelines regarding who may be served in an assisted living facility regardless of payer source. However, state reimbursement policy may establish specific criteria for residents that will be reimbursed through Medicaid in assisted living.
c. Length of Stay
The average length of stay reported by ALFAA is 2.2 years with a median of 2.0 years. Kane and Wilson's national study of 63 assisted living facilities for AARP found that assisted living residents had an average length of stay of 26 months. The most frequently cited reasons for residents leaving in the Kane and Wilson national study were: 1) the need for greater care; 2) behavioral problems; 3) improvement in functioning; 4) not enough funds; and 5) spouse died/moved. In contrast, other researchers have found a mean length of stay in seven CCRCs to be 7.5 years (Newcomer, Preston, and Roderick, June, 1995). It has also been reported that females average more than six month longer lengths of stay than males in both assisted living and nursing units (Newcomer, Preston, and Roderick, June, 1995).
d. Discharge Criteria
Literature produced in the last six months has contributed to the body of information on discharge patterns among assisted living residents. A report on one 400-resident facility with independent living units, assisted living units, and skilled nursing in the same setting indicates anecdotally that transfers between levels of care are frequent (Young & Hegyvary, 1993). Both the ALFAA study and Kane and Wilson's national study appear to confirm that transfers out of assisted living are frequent. ALFAA reports an annual mean turnover rate of 34 percent and that the greatest number of residents discharged from the assisted living facilities surveyed go to nursing homes (46 percent) with the next greatest numbers of residents discharged due to death (24 percent) or discharged to the hospital (12 percent). The Coopers & Lybrand and ASHA 1994 report, The State of Seniors Housing 1994, supplies recent turnover data to complement that of the Kane and Wilson research. Coopers & Lybrand studied the reasons for turnover and developed a chart based on their results (Exhibit 3.4).
| EXHIBIT 3.4: Reasons for Leaving Assisted Living Facilities |
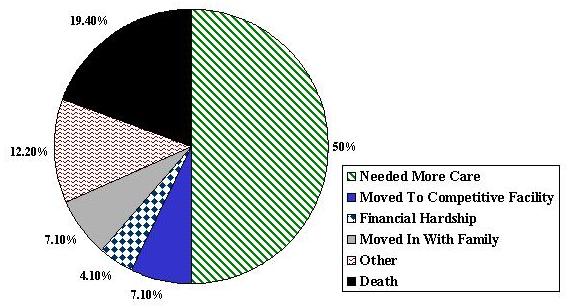 |
| SOURCE: ASHA-Coopers & Lybrand, 1994. |
Mollica et al. explain that in many states "maximum thresholds" are established, that is, some states specify which types of residents must be discharged. Although the report indicates that these discharge rules are fairly broad, they do allow facilities to determine the types of needs that can be met within their facility through the resident agreement process.
e. Discharge Destinations
In examining resident discharge destinations from assisted living facilities involved in their national study, Kane and Wilson found that, in the previous year, 26 of 59 assisted living facilities reported that 25 percent or more of their residents who moved out went to a nursing home and 11 of 59 reported that 50 percent or more of move-outs went to a nursing home. Twenty out of 59 facilities reported that 25 percent or more of their residents go to the hospital and do not return while 17 of the 59 facilities reported that 25 percent or more went to the hospital and died. Six of the 59 facilities reported that 25 percent or more of residents who moved out went to an independent living setting while two reported that 25 percent or more went to other assisted living facilities. Kane and Wilson point out that "substantial numbers died in the assisted living setting or died after a short hospitalization" and that "depending on one's view of the desirable capacity for assisted living, these figures are encouraging because they suggest many people can remain in the setting until death or shortly before" (Kane & Wilson, 1993, p. 30).
Kane and Wilson (1993) also studied the discharge destinations of 371 Oregon residents who left the 20 facilities since 1990. They found that 66 died in the assisted living facility, 64 were discharged to a nursing home, 49 were discharged to their own home, 48 went to a hospital and died after hospitalization.
C. ARCHITECTURE AS AN IMPORTANT COMPONENT OF THE ASSISTED LIVING PHILOSOPHY
A core tenet of the philosophy of assisted living is that the assisted living setting is important to both the physical and psychological well-being of the frail elderly. Many recent definitions of assisted living employ words like "homelike" to describe the ideal assisted living setting, and some experts argue that caregivers and health professionals should use "the residential environment as the basis for therapeutic intervention" (Regnier, 1994, p. 3).
A growing interest in the role of physical environment and architecture, in particular, as issues in assisted living is demonstrated by a burgeoning literature on the topic. Two recent books on architecture and assisted living (Regnier, 1994; Salmon, 1993) and seven articles (Bauer, 1992; Building Design & Construction, 1994; Dorn, 1993; Geran, 1993; Hoglund, 1992; Progressive Architecture, 1994; Regnier, 1992) explain the importance of architecture.
1. Regnier's Architectural Criteria for Assisted Living and His Influence on the Current Literature on Architectural Criteria
Regnier uses nine criteria to define assisted living facilities. They are: 1) appear residential in character; 2) perceived as small in size; 3) provide residential privacy and completeness (i.e., with a full bathroom and a kitchenette at a minimum); 4) recognize the uniqueness of each resident; 5) foster independence, interdependence, and individuality; 6) focus on health maintenance, physical movement, and mental stimulation; 7) support family involvement; 8) maintain connections with the surrounding community; and 9) serve the frail elderly (Regnier, 1992, 1994).
Technological advances may change assisted living facilities even more in the future. Regnier maintains that "as new forms of robotics and communications technology challenge the concept of institutional control, assisted living will become an even more popular avenue for caring for the frail" (Regnier, 1994, p. 1).
To support Regnier's nine-point analysis, recent non-architectural literature is beginning to define assisted living facilities in terms of several of his criteria. Robert and Rosalie Kane note in their 1995 JAMA article that many states now license facilities with the name "assisted living" only if they feature single-occupancy apartment units with full bathrooms and kitchenettes. In addition, in consideration of Regnier's other criteria of "independence, interdependence, and individuality," many experts are promoting the notion of "aging in place." Closely linked with planning and development around physical structure, "aging in place," as discussed by Ivry and others, requires that the assisted living unit be adaptable in its design so that a resident with increasing ADL needs could be accommodated in that same unit over a period of time.
The AARP has also contributed to the literature regarding the confluence between architecture and the philosophy of assisted living. Citing Regnier's work and consistent with the findings of the ALFAA study and the Kane and Wilson study, a recent AARP policy brief describes the range of design elements found in assisted living facilities. Two unit types are described: the first is a private room with bath, individual temperature controls, and locking doors and the second is a small apartment with a kitchenette. The policy brief also indicates that many assisted living facilities include a laundry, central kitchen, and recreational areas in order to support the services that are included with the residents' rental packages. Resident choice over decor, including the increasingly popular option for residents to supply their own furnishings, is one of many steps toward the goal of creating a home-like environment. Another step is the creation of small sitting rooms around the facility to encourage residents to interact with one another and with guests. In addition, many facilities avoid the use of fluorescent lighting, long corridors, tiling and other design features that are more consistent with the bygone institutional paradigm. While promoting this home-like interior design idea, many assisted living facilities must also provide standard safety features to aid frail residents with mobility problems. Handrails, wide hallways, grab bars, emergency call systems, and other security features are present in many facilities.
2. Autonomy-enhancing Features
Many design features are thought to contribute to residents' independence and autonomy in assisted living facilities. Kane and Wilson (1993) found in their national study that 26 of the 63 facilities exclusively had private units with 24 more having more private than double-occupancy units and four with equal numbers of single- and double-occupancy units. The ALFAA study (1993) does not provide any indication of how many units are single or double occupancy. In Exhibit 3.5, a comparison of some features considered to be autonomy-enhancing from the ALFAA and Kane and Wilson studies are presented.
In their national study, Kane and Wilson (1993) found that residents in 47 out of 63 facilities had the capability to lock their doors. (This issue is not discussed in the ALFAA report.)
| EXHIBIT 3.5: A Comparison of the Percentage of Facilities with Autonomy Enhancing Features from Two Studies -- in Percentage | ||
| Autonomy Enhancing Feature | ALFAA Study | Kane & Wilson Study |
| Bath or Shower in unit | 90% | 95% |
| Refrigerator in unit | 90% | 52% |
| Stove in unit | 76% | 27% |
They also found that residents were not allowed to have stoves in 44 facilities, although they were not allowed to have refrigerators in only 14 facilities. The prohibition against stoves may reflect concerns about fire hazards. The conflict between autonomy-enhancing features of assisted living and state regulatory and licensure stipulations will be discussed in a later chapter.
The 1995 Guide to Assisted Living and State Policy also addressed this issue of autonomy-enhancing features. Mollica et al. argue that "while some contend that apartment style models raise costs and require features that residents may or may not use or that may be harmful (stoves, microwaves), others contend that kitchens or kitchenettes do not add significant costs, can be safe and provide an ambiance that is familiar and encourages autonomy" (Mollica et al., p. iii).
3. Current Architectural Prototypes and Standards
Assisted living buildings themselves vary a great deal between freestanding facilities with relatively few residents, to large multi-structure complexes supporting three levels of housing: independent housing, assisted living, and skilled nursing. The AARP policy brief (February, 1995) reports that assisted living facilities vary in size from those that accommodate 15 or fewer residents to those which house 100 or more residents. Newly constructed facilities are typically designed to accommodate between 30 and 70 residents, which planners and developers believe is small enough to ensure that the facility will retain a non-institutional atmosphere but large enough to allow economies of scale in the provision of services. Other researchers have found that the proportion of total units allocated to assisted living may in some way contribute to a predisposition in the facility to rely on institutional service approaches. They suggest that this institutional quality may be reflected in operational practices developed in large complexes or in the mix of residents self-selecting admission into these facilities (Newcomer et al., 1995).
Recent research on assisted living and nursing unit use among CCRC residents found a significant difference in use between so called "high-rise" and "garden" complexes. Total days of assisted living use are decreased by almost six months for those frail elderly who reside in high rise facilities. Many factors, including the recent evidence that the proper residence for dementia patients is a garden complex as opposed to a potentially disorienting high-rise, may partially explain the results of this research (Newcomer et al., 1995).
4. State Architectural Models
Mollica et al. discussed the issue of architecture in their report as well. They reviewed the three general architectural requirements of various state policies: 1) some states required apartment settings in order to maximize the home-like quality sought through assisted living; 2) other state regulations required private bedrooms with attached baths or double occupancy bedrooms shared by agreement of residents; and 3) a last category of states mandated that assisted living facilities offer shared bedrooms or bathing facilities that may not be attached to the room and can be shared by more than two residents of the facility.
5. Architectural Comparisons With European Models
One researcher has identified a number of basic elements in assisted living facilities in the United Kingdom (also known as residential care homes) (Salmon, 1993). In the United Kingdom, some of these typical basic elements include a private bed-sitting room with its own front door opening into a corridor, and communal sitting rooms for residents who wish to socialize. The entrance is welcoming and has places for residents to sit outside. There is a larger, main communal lounge for larger social activities. There are planned group activities and outings. There are qualified care staff on call 24-hours a day, all housekeeping is provided, lunch and the evening meals are served in a communal dining room. Regnier maintains that there are 20 differences in practice and philosophy between U.S. and European assisted living facilities. Differences in community services, the relationship of the facility to its surrounding context, and participatory models that incorporate residents in decision-making are a few of the distinctive issues. Regnier points out that while we can learn from the European models of assisted living, the U.S. is not going to become a heavily socialized welfare state. He predicts that as a result, the European model will not become the American model.
D. THE SERVICES PROVIDED BY ASSISTED LIVING FACILITIES
This section focuses on the services provided by assisted living facilities. A number of general articles in the assisted living literature mention services or the fact that facilities provide assistance with ADLs, but are not specific about the services provided. In reviewing the definitions of assisted living in Exhibit 2.3, a number of authors define assisted living primarily by its bundled and unbundled services (e.g., Diesenhouse, 1993; Stuart, 1993; Walser, 1994; Business Wire, 4/19/95; PR Newswire, 8/8/95).
1. Survey Literature On Services
Two surveys published since 1992 have addressed the issue of services in assisted living facilities. The Coopers & Lybrand-ALFAA study of 201 assisted living facilities (1993) has systematically assessed the types of services provided in the typical assisted living care package. In addition, the Kane and Wilson (1993) national study of 63 providers for AARP also has examined services provided in assisted living facilities. These two studies, with some anecdotal information from other sources, provide most of the information included in this section.
The numbers and kinds of services available may be dependent on residents' ability to pay. Both ALFAA-Coopers & Lybrand and Kane and Wilson found that a number of facilities provided services to residents at an additional charge or on a fee-for-service basis. These services are commonly called "unbundled" services or "amenities."
Kane and Wilson (1993) found that "when asked to list the services provided, respondents typically listed meals, housekeeping, transportation, laundry and linen service, activities, medication monitoring, and assistance with bathing and dressing. Many settings mentioned having add-on levels of care that could be purchased separately" (Kane & Wilson, 1993, p. 34). The authors categorized facility responses into three levels of services: 1) relatively heavy services provided; 2) relatively light services provided; and 3) graduated services provided. Due to the diversity of services provided in the facilities, the authors did not quantify the number of facilities in each category.
One respondent involved in the Kane and Wilson study described "heavy services" as "24hour supervision; emergency call system, nurse on staff so there is nursing supervision around the clock; assistance with ADLs; medication supervision; personal care staff; beautician comes weekly-extra charge; daily exercise program; daily social activities (i.e., recreation, rides, shopping); transportation program; housekeeping services; three meals a day; provide for special diets; bathrooms are safety equipped; laundry" (Kane & Wilson, p. 34). Relatively "light" services were described by another provider: "We provide housekeeping every two weeks and a daily continental breakfast. Dinner is purchased off a meal card and must be selected by 1:00 p.m. We have an 'I'm O.K.' system where a button needs to be pressed by 9:30 a.m. and 9:30 p.m. daily or we will check; 24-hour emergency call system; on-site caretaker to residents after 10:00 p.m.; bus provides transportation to MD's appointment, bank and so on. [Home health agency] provides any personal care services on a fee-for-service basis" (Kane & Wilson, p. 35). Finally, an example of a respondent's description of graduated services provided is given: "Medication monitoring--if we dispense medications there is an additional charge; option of three meals; activities; transportation; housekeeping; and maintenance. Base line personal care--one bath per week, help with dressing, grooming, and ambulation. Podiatrist and physician within our building can be seen for fee-for-service" (Kane & Wilson, p. 36).
The ALFAA-Coopers & Lybrand study categorizes services included in the basic daily rate, those provided at an additional charge, and those that are not provided by assisted living facilities (ALFAA & Coopers & Lybrand, 1993), as shown in Exhibit 3.6.
| EXHIBIT 3.6: Core Services Provided by Assisted Living Facilities: in Percentage of Facilities | |||
| Service | Included in Basic Rate | Provided at Extra Charge | Not Provided |
| 24-hour security | 100% | 0% | 0% |
| Social activities | 98% | 2% | 0% |
| 3 meals a day | 96% | 4% | 0% |
| Emergency call system | 96% | 4% | 0% |
| Snacks | 93% | 5% | 2% |
| Special diets | 89% | 7% | 4% |
| Daily maid services | 89% | 9% | 2% |
| Linens | 88% | 5% | 7% |
| Assistance with ADLs | 84% | 14% | 2% |
| Transportation | 78% | 16% | 6% |
| Medication Administration | 71% | 18% | 11% |
| Weekly health checkup | l57% | 11% | 32% |
| Furnishings | 52% | 9% | 39% |
| Incontinence care | 52% | 27% | 21% |
| Telephone | 21% | 59% | 20% |
| Physical Therapy | 14% | 32% | 54% |
| Incontinence products | 5% | 64% | 31% |
| SOURCE: Adapted from An Overview of the Assisted Living Industry, ALFAA & Coopers & Lybrand, 1993. | |||
In addition to the Kane and Wilson and ALFAA-Coopers & Lybrand surveys, Hawes et al. have recently completed a survey of the impact of regulation and licensure standards on quality in Board and Care homes in ten states. Because assisted living is a subset of the larger Board and Care category of seniors housing, the findings of the Hawes et al. study are valuable as an additional source of information. Moreover, the Board and Care study results can be a useful tool for analysis because it may show discrepancies due to the absence of the assisted living philosophy in many Board and Care facilities. We would expect, therefore, to identify characteristics of these "non-autonomy-enhancing" and "non-aging-in-place" facilities in the data of the Hawes et al. study results.
Exhibit 3.7 is a compilation of the results of the national board and care study (Hawes et al., 1995) and it shows several points of similarity with the ALFAA-Coopers & Lybrand results. Meal services, personal care services, and administration of medication are the three most prevalent services cited in board and care homes. Personal care services are reportedly less often included in the package of services in board and care facilities as compared to the ALFAA-Coopers & Lybrand study which was more strictly limited to assisted living facilities. These lower percentages (92 percent for licensed board and care homes and 62 percent for unlicensed board and care homes compared to 98 percent of assisted living facilities) may be due to the board and care homes that do not adhere to the philosophy of assisted living. Instead, these facilities may concentrate on the housing that they provide, rather than creating a balance between housing and services that is sought in assisted living facilities. In addition, it is interesting to note that medication administration appears to be slightly more common in board and care homes (99 percent of licensed board and care homes and 76 percent of unlicensed board and care homes compared to 89 percent of assisted living facilities).
| EXHIBIT 3.7: Board and Care Survey Findings Regarding Services: in Percentage of Facilities, Both Licensed and Unlicensed | |||||||
| Skilled Nursing Care | Money Management | Meal Services | Admin. of Medications | Personal Care Services | Structured Social Activities | Transportation | |
| Hawes et al. (1995) | 39% (l)45% (ul) | 39% (l)45% (ul) | 97% (l)90% (ul) | 99% (l)76% (ul) | 92% (l)62% (ul) | 88% (l)81% (ul) | 89% (l)87% (ul) |
| NOTE: "l" indicated licensed facilities and "ul" indicates unlicensed facilities surveyed by Hawes et al. | |||||||
2. Other Services and Amenities
ASHA, in conjunction with Coopers & Lybrand, conducted a survey of assisted living facility managers which yielded information about additional services and amenities included in ASHA survey respondents' facilities (Exhibit 3.8). The survey found that a large number of assisted living providers offer amenities. Transportation, social programming, and beauty/ barber shop services were the most common unbundled services offered.
| EXHIBIT 3.8: Other Services and Amenities Provided by Assisted Living Facilities: in Percentage of Facilities | |
| Service | Included in Basic Rate |
| Beauty/Barber Shop | 95% |
| Chapel/Meditation Room | 41% |
| Emergency Response System | 100% |
| Exercise Room | 79% |
| Full Kitchen in Units | 10% |
| Personal laundry | 99% |
| Recreation Facilities | 92% |
| Electronic Security | 75% |
| Nighttime Security Guards | 58% |
| Social Programs | 99% |
| Transportation | 95% |
| SOURCE: adapted from ASHA & Coopers & Lybrand, 1995. | |
3. Non-Survey Literature on Services
In addition to the major survey sources, a number of other articles have addressed the issue of services. A summary of the core services and amenities contained in these articles can be found in Exhibit 3.9. A comparison of these articles demonstrates that the consensus being developed in the area of services is based around meal services (generally three meals a day), housekeeping services (including laundry), and personal care (including assistance with ADLs).
The June 1995 policy brief published for the AARP describes in some detail the kinds of services that can be expected from an assisted living facility. This brief explains that the "typical" assisted living facility offers assistance with at least one ADL and assistance can usually be obtained 24-hours a day. Most facilities offer a standard "package" of services, but they bundle them differently and some provide additional "unbundled" services at extra charge. Skilled nursing and ancillary care are noted as examples of care that may be packaged through third-party providers. Social services like assistance with arranging doctors appointments and other activities are also usually provided. The scheduling of services is cited as an important issue for assisted living facilities because of the need to follow the philosophy of resident autonomy. Accordingly, residents often have the option of carrying out some tasks on their own and family members are often encouraged to participate in food preparation and other tasks.
Kane and Kane assume in their 1995 JAMA article that assisted living, by definition, should supply three meals a day and provide on-site staff. In addition, they describe assisted living as an approach which allows residents to be treated as "tenants" with full rights of refusal of care. In this rather subtle point emerges one of the most contentious issues in the assisted living industry. The issue of residents' rights to self-medicate, to ignore prescribed diets, or to take on some tasks not included in their care plan has served to further complicate a discussion of "core services" in assisted living. State regulatory and licensure issues and legal battles regarding "managed risk" make it difficult to define assisted living by its services, because inherently, those services will vary by patient as well as by facility.
Another industry observer lists meal services, housekeeping services, administration of medications, assistance with personal care, and some structured social activities as a typical package of assisted living services (Pfeiffer, 1995). Currents, a publication of the American Association of Homes and Services for the Aging, lists its set of core services in the May 1995 issue. The editors included daily meal service, basic housekeeping, laundry, help with bathing, medication assistance, emergency medical services, 24-hour security, transportation, activity and wellness programs, and service coordination in their version of the assisted living service package.
ALFAA's Assisted Living Today (Clipp, Summer 1995) compiled a similar list based on interviews with three assisted living providers. Core services were defined as three meals per day, weekly housekeeping and linens, emergency response, seven hours per week of assistance with activities of daily living (ADLs), weekly transportation to and from doctors appointments (two trips per week, average distance of five to ten miles), activities (three per week), medication reminders, care management, and over-night companion service.
| EXHIBIT 3.9: Services Described in Non-Survey Literature Sources | |||||||||||||
| Skilled Nursing | Ancillary Care | Scheduling Of Svcs (Including Arranging Physician Appointments, Etc.) | Meal Services | Housekeeping Services; Includes Laundry | Administration Of Medications | Personal Care Services; Includes Help With Bathing | Structured Social Activities | Emerg. Medical Services | 24-hour Security | Transportation | Case Management | Overnight Companion Service | |
| Clemmer (June 1995) | X | X | X | ||||||||||
| Pfeiffer (January 1995) | X | X | X | X | X | ||||||||
| Currents (May 1995) | X | X | X | X | X | X | X | X | X | ||||
| Assisted Living Today Clipp (Summer 1995) | X | X | X | X | X | X | X | X | X | ||||
| Diesenhouse (1/3/93) | X | X | X | X | X | ||||||||
| Stuart (1/3/93) | X | X | X | X | X | ||||||||
| Walser (1994) | X | ||||||||||||
| Business Wire (4/19/95) | X | X | X | X | X | ||||||||
| Selis (5/8/95) | X | ||||||||||||
| Clipp, (Summer 1995) | |||||||||||||
| PR Newswire (8/8/95) | X | ||||||||||||
| EXHIBIT 3.10: Staffing Patterns in Four Major Surveys | ||||||||||
| Author(s) | Scope of Study | Median Staff Size | Staffing Ratio* | Staff Category 1: Administration | Staff Category 2: Kitchen | Staff Category 3: Housekeeping | Staff Category 4: Care Staff | Staff on Contract | Awake Staff | Staff Training |
| Kane and Wilson (1993) | National: 63 facilities | 20.5 | The authors insist that there were too many variables in their sample to come up with a reasonable ratio. | receptionists, marketing personnel, managers, and activity directors | cooks and dishwashers | Housekeeping staff and maintenance. | care aides; few used medically skilled nursing staff); 7/63 listed some nursing staff but not by type; RNs staff (22/63 had no (13/63); LPNs (15/63) but very few physicians; tenant's own physician used in most cases. Free-standing or purpose-built tended to have fewer nursing staff, except Washington and Florida, which have established assisted living regulations. | 46/63 had outside consultants; wide-range, from beauticians to physicians. Podiatrists and nutritionists were very common. 48/63 had at least some outside home health agency employees. Some contracted out all personal care; these contractors either provided just PCAs or provided PCAs with skilled nursing staff. | Almost all had at least one staff member awake and on duty all night | |
| Coopers & Lybrand, ALFAA study, 1993 | 25 states; 201 facilities/6,11 9 units | range: .1-1.4 | 90% of facilities reported providing some level of medication management; 58% provide medication reminders; 54% dispense medication | 8% of facilities contracted with an outside agency for medication management | ||||||
| Hawes et al., RTI, July 1995 | Study of Board and Care homes in 10 states 512 facilities | 25% of licensed facilities reported having RNs or LPNs on staff; 27% of unlicensed facilities reported having RNs or LPNs; 21% of all homes had RNs or LPNs who worked full or part time; 73% of staff who reported passing medications were not licensed nurses; and 28% of staff giving injections were not licensed nurses. | 18% of licensed facilities contract with a home health agency; 27% of unlicensed facilities contract with a home health agency. 53% of the facilities reported that outside Personal care is contracted in 25% agencies provide temporary or episodic nursing care. or licensed and 33% of unlicensed facilities. In 40% of facilities, therapy services were provided by outside providers. | 20% of licensed facilities and 33% of unlicensed facilities reported that they did not require training for staff. | ||||||
| Coopers & Lybrand, The State of Seniors Housing for ASHA (1994) | National: 326 facilities; 60,000 units | by ownership status: .28 for profit CCRCs: .44 not-for-profit: .37 | ||||||||
| * Staff per resident | ||||||||||
Finally, another industry observer maintains that the typical services provided by assisted living facilities include: "three meals a day, regular housekeeping and laundry service, assistance in dressing, bathing, and walking, social activities; (and) some limited medical supervision" (Evans, 1994).
4. Current State Policy on Assisted Living Services
Mollica et al. review state policies on assisted living in the NASHP study published in 1995. They explain that state rules all allow or require the provision of personal care or personal assistance services arranged by assisted living facilities. However, the authors warn that there is significant variance in the extent to which skilled nursing services may be provided. In fact, they point out that some states specifically limit the number of days that skilled nursing may be provided. In general, Mollica et al. have found that state policies on assisted living allow for the provision of a service package that includes some nursing services, the need for services on an unscheduled basis, the development of an individualized service plan, access to ancillary services, and the opportunity for special services (e.g., extra assistance for dementia patients) (Mollica et al., p. 10).
Many observers believe that it is good for the assisted living industry to develop differently in various regions of the country. Some observers, however, suggest that the lack of standardization of services provided by assisted living facilities in different states and regions can lead to unrealistic expectations of the long-term care model and resulting vulnerability to liability suits (Olson, 1994). Indeed, a recent Washington Post story on the death of an assisted living resident asserts that expectations about the services provided may not match the actual services being provided (Vick, 1994).
E. NEEDS ASSESSMENTS AND REEVALUATIONS
In addition to the development of a core set of services for the assisted living industry, many experts are also interested in assessing the delivery of those services to residents in the form of care plans or "needs assessments." The literature produced in the last several years offers few insights into the actual organization and oversight of initial needs assessments and reevaluations. Kane and Wilson (1993) in their national study for AARP asked questions about admission procedures in order to determine how care planning was accomplished and how individualized care plans are developed and implemented in these facilities. They found that 30 of the 63 facilities had a pre-admission evaluation process and that 26 of the 63 used a systematic formal care plan. Twenty-three completed a formal assessment form. Families were involved in assessments in 31 of the 63 facilities and a nurse was involved in 26 of the facilities. In general, "the assessment described varied enormously in their content, their degree of standardization, and their intensity" (Kane & Wilson, 1993, p. 38). The authors further found that reevaluations were common in approximately 25 percent of the facilities, with some having a formal reevaluation system and some an informal system.
Kane and Kane indicate in their 1995 JAMA article that individually planned care is a critical part of the assisted living concept, but they give no additional information regarding how that care is planned, from admission through an organized re-evaluation process. More extensive analysis of the prototypical evaluation and care planning process is included in the June 1995 AARP policy brief. That brief describes a process by which "before moving in, the resident or family member describes the resident's needs and works with the staff to decide what help will be provided and how and when."
F. STAFFING NEEDS AND STAFF-TO-RESIDENT RATIOS IN ASSISTED LIVING FACILITIES
Since the services provided in assisted living facilities and the care plans that are developed for residents are created by people, it is important to explore the role of staffing in assisted living. Topics in the literature on the issue of staffing include staff-to-resident ratios, the education and skill levels of staff in assisted living facilities, the position of staff as direct employees or contracted staff, and the impact that staff make on the quality of life and improvement of health among residents.
Exhibit 3.10 compares the staffing patterns described from three surveys of assisted living facilities and the National Board and Care survey. Kane and Wilson (1993), ALFAA (Coopers & Lybrand, 1993), ASHA (Coopers & Lybrand, 1995), and Hawes et al. (July, 1995) all contribute some information on the topics of median staff size, staffing ratios, labor categorization, staff regulations, and staff training. The discussions below compare these four surveys on several topics relevant to staffing.
1. Variations in Staffing Patterns
As Exhibit 3.9 demonstrates, there is a lack of systematic, comparable information on the topic of staffing. Thus, it is difficult to assemble a model of staffing patterns for the assisted living industry as a whole, especially due to the wide range of staffing patterns. This wide range of staffing patterns may reflect, in part, the diversity of residents served by assisted living. Kane and Wilson found that "staffing patterns related to whether the setting was freestanding, part of a nursing home or CCRC, or a housing complex; whether the setting was large or small; how the state regulated assisted living; and so forth" (Kane & Wilson, p. 30).
2. Staffing Statistics: Median Staff Size and Staff-to-Resident Ratios
a. Survey literature on staffing statistics
The Kane and Wilson study, found that the median staff for the national study of 63 settings was 20.5 (range 3 to 60). Due to the complexity of non-comparable labor categories, staffing variation by time of day, and the level of detail involved in the data collection, Kane and Wilson report that they were unable to create a staff-to-resident ratio that was meaningful across all facilities.
Staffing ratios may be related to the level of care and time of day. One facility described in recent literature has staff-to-resident ratios of .08 to .10 during the day and .03 at night while another provider has staff-to-resident ratios of .076 in their assisted living facility (Evans, 1994). ALFAA-Coopers & Lybrand (1993) reports that the mean staff-to-resident ratio in their survey sample is .37 (range .1 to 1.4). A similar staff-to-resident ratio (.33) for one facility specializing in residents with head trauma was reported in another recent research article (Bowe, 1993).
b. Non-Survey Literature on Staffing Statistics
Staffing patterns have also been discussed in the non-survey literature. One article reports one 50 to 60 resident facility had 35 caregivers, programming personnel, service coordinators, and assistants (Bruck and Widdes, 1995). The staff-to-resident ratio for each "house" in the facility was .16. This is considerably lower than the ASHA-Coopers & Lybrand study, but well within the range of the ALFAA-Coopers & Lybrand study. The ratio in the facility at large (which reflects the consideration that residents will come into contact with staff who do not necessarily concentrate on their particular "house") was closer to .25 (Bruck and Widdes, 1995).
3. Labor Categories: Types of Staff and Staffing Responsibilities
a. Survey Literature on Labor Categories
In addressing the types of staff employed directly and under contract by assisted living facilities in their national sample, Kane and Wilson identified four general labor categories. These four groups, administration, kitchen, housekeeping, and care staff were the most frequently directly employed by facilities.
In general, Kane and Wilson found that few medically skilled staff were used by facilities in their national study. They found that RNs and LPNs were used by some of the facilities, but few facilities employed a facility physician. The Board and Care study results from Hawes et al. confirm the findings of Kane and Wilson. Kane and Wilson found that 21 percent of assisted living facilities had RNs on staff and that 24 percent had LPNs on staff. Similarly, Hawes et al. found that 21 percent of homes employed full- or part-time RNs or LPNs. Both studies found extensive use of nurses aides and personal care aides in place of RNs or LPNs. This trend, considered by some observers of the assisted living industry to be a potential cause for concern, will be discussed further below.
The number of staff employed on contract with outside agencies is another topic addressed in the survey literature on staffing patterns. In the Kane and Wilson study, outside consultants were used by 46 of the 63 settings, with a wide variety of specialty consultants, including beauticians, nutritionists, podiatrists, and physicians. Home health agencies provided care to at least some of the residents at 48 of the 63 facilities. A comparison between Kane and Wilson and the Hawes et al. study suggests that assisted living facilities employ a larger number of contracted staff. Kane and Wilson found that 73 percent of the facilities in their study had outside consultants of several types (beauticians to physicians), and 76 percent had at least some outside home health agency employees. In contrast, board and care homes used outside contractors much less frequently. Only 18 percent of licensed facilities contracted with a home health agency (27 percent of unlicensed facilities did the same). In other categories of ancillary care, Board and Care homes consistently used very few outside contractors. Only in the category of episodic nursing care did Board and Care homes approach a significant use level (53 percent of Board and Care homes reported that outside agencies were contracted for episodic nursing care).
In assessments of both the care staff patterns and the frequency of outside contracting, it is useful to note the Hawes et al. data for unlicensed board and care homes. The data for these homes appears to more closely match those of the Kane and Wilson data. Hawes et al. have speculated that a large number of the unlicensed homes they surveyed are in fact assisted living facilities that do not yet have a licensure category under their particular state statutes. This hypothesis would help to explain the convergence in staffing patterns between assisted living facilities in the Kane and Wilson study and the unlicensed Board and Care homes in the Hawes et al. study.
b. Non-Survey Literature on Labor Categories
There are several different staffing models common to assisted living facilities. The types of staff hired and the patterns of their daily work vary widely from facility to facility. The non-survey literature provides detailed descriptions of a number of these staffing models and the characteristic labor categories involved.
One provider, quoted in a non-survey literature source, maintains that "food service accounts for approximately 27 percent of staff time and housekeeping for 13 percent at the average assisted living community" (Evans, 1994, p. 55). Since Evans reports that a total of 40 percent of staff time is devoted to meals and housekeeping, one might assume that assisted living facilities staff concentrate on services unrelated to nursing functions.
At Arden Courts, another facility cited in the literature, the core staff team is made up of "Resident Caregivers" who are also known as "houseparents.'' The role of the Resident Caregiver is to assist with ADLs. Assigned to a particular house (the facility is composed of several self-contained houses), they work with a group of residents every day and get to know their individual care needs. The staff work in three shifts, like nursing home staff, but in all other ways, this facility and other similar assisted living facilities, are staffed in very different ways. Experience and personality are two key factors in hiring policy that are highly valued by the operators of Arden Courts (Bruck and Widdes, May, 1995).
Another staffing model discussed in the provider trade literature involving facilities sponsored by National HealthCare L.P. has RNs on site, supervision and administration of medication, counseling and health assessments (Business Wire, April 19, 1995).
The non-survey literature has also contributed some substantive commentary on the subject of ancillary care provided by outside contractors. One industry observer argues that future growth in the assisted living industry will come in the greater availability of ancillary and physician services on-site (Cook, 1995). These relationships between providers of ancillary care and assisted living operators often will be developed through contracts and lease arrangements, but they will also be expanded through contracts with contractors who will provide complete packages of home health services to assisted living facilities.
4.Current State Staffing Policy
Exhibit 3.11 lists the current policy and most recent policy changes made by state legislatures regarding staffing in assisted living facilities. These state summaries are taken from the 1995 Guide To Assisted Living And State Policy and should not be used as comprehensive accounts of state activity on this topic.
| EXHIBIT 3.11: Current Policy and Most Recent Policy Changes Made by State Legislatures | |
| State | Staffing Regulations |
| Alabama | The regulations require at least 1 staff member per 6 residents (.16) 24 hours a day and personal care staff to meet the needs of residents. |
| Alaska | Homes must have the type and number of staff needed to operate the home and must develop a staffing plan that is appropriate to provide services required by resident care plans. |
| Arizona | The center manager may employ or con tract with staff for supportive services, supervision, food service, housekeeping and maintenance, social and activity programs, and general supervision. At least one staff must be awake and on-duty. An RN must be available to provide nursing service specified in each plan of care. No staff ratios are included in the regulations and centers are required to have sufficient personnel available to provide services identified in resident care plans. Managers must receive 20 hours of continuing education credits each year. Staff are required to receive an orientation from the center and complete a 16-hour training program, approved by the county within 60 days of their employment, as well as 20 hours of in-service training a year. |
| Connecticut | ALSAs must have at least 1 RN and an on-site supervisor 20 hours a week for every 10 or fewer RNs and aides and a full-time supervisor for every 20 RNs and aides. A sufficient number of aides must be available to meet residents' needs. All aides must be certified Nurses Aides or Home Health Aides and complete 10 hours of orientation and one-hour of in-service training every 2 months. Twenty four hour awake staff are not required since the needs will vary among managed residential communities. However, 24 hour staffing could be required if indicated by resident plans of care. An RN must be available on-call 24 hours a day. |
| Florida | Facilities are allowed to establish their own staffing plan based on the amount and type of services needed by residents and reflected in resident plans of care. Certified nursing assistants and certified home health aides must receive training in the concepts and requirements of extended congregate care. |
| Iowa | Providers will have to develop a core service capacity which will be defined by regulations. |
| Maryland | In both Senior Assisted Housing (SAH) models, staff must be adequate to provide the required services. Under the Medicaid waiver, at least one staff person must be on duty at all times for every 8 residents. Providers may be a physician, nurse or persons with three years of applicable experience. |
| Massachusetts | No specific staffing guidelines are included concerning the type and number of staff. However, the residence must maintain an ability to provide timely assistance to residents and to respond to urgent or emergency needs through on site staffing, personal emergency response or other means. Under draft regulations, all staff and contracted providers must receive a 6-hour orientation which includes the philosophy of independent living, resident bill of rights, abuse, safety and emergency measures, communicable diseases, communication skills, the aging process, and resident health and related problems. Staff providing personal care must complete an additional 54-hour training course that includes 20 hours of personal care and 34 hours of general training. The personal care component must be taught by an RN. Personal care staff will be reviewed twice a year by a qualified nurse. |
| Minnesota | The Department of Health's standards for home care services licenses do not apply to the building itself. |
| New Jersey | The regulations require at least one awake staff member and one additional staff member at night and sufficient staffing to provide the services indicated by the assessments of resident needs. A registered nurse must be available on staff or on call 24 hours a day. Administrators must either be licensed as a nursing home administrator or complete an assisted living training course approve d by the Department of Human Service or equivalent training approved by the Department of Health within one year of their employment as an administrator. In addition, they must complete 10 hours of continuing education a year. Personal care assistants must complete a nurses aide training course, a homemaker-home health aide training program or equivalent training approved by the Department of Health. |
| New York | Adult homes must have a case manager and staffing that is sufficient to provide the care needed by residents. Staff providing personal care must complete a home health aide training course or other examination approved by the Department of Health. Adult home staff must provide 3.5 hours of service staff time per resident per week for personal care, 1 hour per resident per week for housekeeping and 2 hours of food service time per resident per week. Enriched housing programs must staff to provide a total of 6 hours per resident per week for housekeeping, personal care and food service which can be allocated based on aggregate resident needs. |
| North Dakota | Must be able to deliver the necessary services required by plans of care. |
| Ohio | At least one staff member must be on-site at all times. In addition, sufficient staff time must be available to meeting the residents' care in a timely manner, supervisory and emotional needs and reasonable requests for service, including ongoing supervision of residents with increased emotional needs or presenting behaviors that cause problems for the resident or other residents and to properly provide dietary, housekeeping, laundry and facility maintenance services and recreational activities. An RN, LPN or physician must be on duty when medications are being administered. Staff may be shared with other licensed facilities in the same building or in the same lot as long as staffing requirements for all facilities are met. |
| Oregon | The regulations do not specify staffing requirements. Each facility must have sufficient staff to deliver the services specified in resident plans of care. |
| Rhode Island | Must be sufficient to provide the necessary care and services to attain or maintain the highest practicable physical, mental and psychological well-being of the residents, according to appropriate level of licensing. |
| Utah | Direct care staff are required on-site 24 hours a day to meet resident needs as determined by assessments and service plans. |
| Virginia | Staffing patterns must be appropriate to deliver the services required by the residents as described in the plans of care. |
| Washington | RNs or LPNs are required to be available on site 5 hours a day, 7 days a week and on call 24 hours a day to provide services listed in the negotiated service agreements. Other staff must be sufficient to deliver services identified in service agreements. New staff must receive 5 hours of training and monthly in-service training on assisted living values and principles. |
| Wisconsin | The draft report would require that providers submit staffing plans which would be approved by the Department of Health and Social Service. Minimum standards would require 24-hour awake staff, full-time administrator/manager, sufficient staff to meet resident needs as identified in plans of care, licensed or certified staff to provide or arrange for nursing, dietary evaluation and services and pharmaceutical services. Cross training of staff to provide personal care, basic nursing care, cooking, laundry, housekeeping and other services would be encouraged. |
Exhibit 3.12 compares state policies on a number of important staffing issues: staff size, staff-to-resident ratio, 24-hour staff, awake staff, nursing requirements, aide requirements, physician participation, and staff training. As this chart demonstrates, state policies concerning staffing patterns vary widely. The one point of consensus among the statutes is the obligation of facility operators to employ an "adequate" number of employees to deliver the level care described in residents' care plans.
| EXHIBIT 3.12: Issue-Specific Comparison of State Policies | ||||||||
| Staffing Ratio | 24-Hr. Staff | Awake Staff | Nursing Requirements | Aide Requirements | Physician Participation | "Adequate" Numbers of Staff to DeliverCare Listed in a Care Plan | Training of Staff:- Orientation- In-Service | |
| AL | X | X | X | |||||
| AK | X | |||||||
| AZ | X | X | X | X | X | |||
| CT | (onsite and on-call) | X | X | X | X | |||
| FL | X | X | ||||||
| IA | ||||||||
| MD | X | (onsite) | X | X | ||||
| MA | X | X | X | X | ||||
| MN | ||||||||
| NJ | (onsite) | X | X | X | X | X | ||
| NY | X | X | X | |||||
| ND | X | |||||||
| OH | (onsite) | X | X | X | ||||
| OR | X | |||||||
| RI | X | |||||||
| UT | (onsite) | X | ||||||
| VA | X | |||||||
| WA | (oncall) | X | X | X | ||||
| WI | X | X | X | X | ||||
| SOURCE: Mollica et al., 1995. | ||||||||
Consistent with this observation, in the Oregon component of the Kane and Wilson study, researchers found that there were no staff requirements other than the need "to implement individualized care plans" (Kane & Wilson, p. 52). They found that Oregon facilities generally utilized an administrator, nurse, and a social worker although the nurse and social worker frequently were part-time contract employees in smaller facilities. Under Oregon statute, nurses have the capacity to delegate care tasks.
In North Carolina, the Intergovernmental Health Policy Project (IHPP) has identified a particular interest in staffing. New regulations in that state require that a study of the fiscal impact of all residential facilities be conducted to measure the effects of staff size, staff turnover ratios, wages and benefits, and staff training (Folkemer, IHPP, 1995, p. 23).
5. Emerging Issues and Concerns
a. Staffing Ratios Are Becoming More Common
Although there is general acceptance of the standard of "adequate" staffing patterns as described above, Mollica et al. insist that the trend in state policy is moving away from such vague prescriptions. The authors insist that while "a few states require ratios of awake or on-site staff,...the clear trend substitutes flexible staffing plans and schedules for specific staffing ratios" (Mollica et al. p. 22).
b. Staffing Patterns Specific to Dementia Patients
One example of the trend toward specialization is in the area of assisted living for dementia patients. In a summary of a recently published draft report titled "People With Dementia: Toward Appropriate Regulation of Assisted Living and Residential Care Settings," Joan Hyde proposes that "there shall be adequate staff to meet the personal care and activity needs of the residents as documented in their service plans. The facility shall maintain written staffing schedules and actual hours worked by each employee shall be documented" (New Report Offers Draft Regulations for Assisted Living for People with Dementia, ALFAA Advisor, July 1995, 1-2). The Hyde proposal on the standard that there should be "adequate" numbers of staff awake and on the premises 24-hours a day to meet both scheduled and unscheduled needs and to ensure the safety of the residents, does not include specific ratio goals for an assisted living facility.
The draft report insists that "a facility that holds itself out to be particularly equipped to meet the needs of people with dementia or which operates a specialized dementia unit shall make public its staffing patterns. These shall include, at a minimum, 24-hour awake staff." Like the general standards, Hyde expects the staff working with dementia patients shall keep written records of the actual hours that they have worked to ensure that consumers are receiving the services promised by the facility. Additional standards specifically designed for facilities housing dementia patients are also outlined by Pfeiffer (Postgraduate Medicine, January 1995).
c. Nurse Delegation
Mollica et al. also specifically addresses the question of nursing needs in assisted living facilities. They conclude that there is currently a significant movement nationwide away from the use of nurses for medication administration and injections. This trend toward "nurse delegation" reflects concerns about cost effectiveness and the fact that many tasks traditionally performed by nurses can be safely performed by nurses aides and other non-licensed employees. The Mollica et al. assessment of nurse delegation is borne out by the research findings of Hawes et al. (1995). They found that 73 percent of staff in Board and Care homes who reported passing medications were not licensed nurses and 28 percent of staff in Board and Care homes who reported giving injections were not licensed nurses. They further found that 26 percent of the non-nursing staff passing medications reported that they received no training on medication supervision or management, and only one state (Oregon) has a program to train and certify nursing assistants to pass medications (Hawes et al., 1995, p. 18).
d. The Role of Geriatric Social Workers
In addition to the concern for adequately trained care staff, some experts in the field of geriatric social work have raised questions about the mental health and social work needs of assisted living residents. Some industry experts have argued for an expanded role for geriatric social workers in the assisted living setting. They insist that geriatric social workers have special skills that are needed to assist the frail elderly in navigating the gray area between preserving their independence and conceding to the need for assistance in ADL's. Conflicts may arise between housing managers and social workers over the often overlapping roles that they assume in assisted living facilities, and these disputes must be resolved so that the residents receive the benefits of appropriately trained staff.
e. Exploring The Relationship Between Staff and Quality
In a survey of 16 developers, Kane and Wilson (1992) identified three general staffing issues related to quality: 1) the supply and turnover of assisted living staff, who generally receive low pay; 2) training staff for the assisted living model; and 3) the relationship of staff to quality. No empirical studies have been undertaken since 1992 to evaluate the impact of different staffing patterns or employment arrangements on assisted living. However, such evaluations have been undertaken in the nursing home industry. This research has found that increased numbers of RNs in particular, but also increased numbers of all types of staff, lead to better quality outcomes in the nursing home setting.
In addition, anecdotal reports allege staffing deficiencies in reference to several recent accidental deaths at assisted living facilities. Former employees of Sunrise Retirement Homes & Communities have been quoted in several Washington Post articles in reference to the question of staff quality and experience concerns. One former RN at the Falls Church Sunrise facility indicated that "they (the facility administrators) made the families feel that their loved ones would be watched over and that staff could take care of emergencies, which was not true" (Washington Post, September 18, 1995). In a October 1995 press release, Sunrise insists that its staffing problems have been blown out of proportion, and that identified problems have been ameliorated. Specifically, Sunrise states that it has developed additional training programs for staff at the facilities where problems have been reported. In addition, Sunrise states it has begun staffing a full-time nurse at all facilities this year.
Assisted living facilities staffing problems are also one result of the fact that their work force is largely under-educated and paid a wage that reflects their relatively low level of skills and training (Washington Post, January 9, 1995). For example, Sunrise reportedly pays its employees $6 to $9 per hour. Yet, Sunrise and other assisted living providers question the extent to which they are really responsible for medical supervision. Sunrise senior management has argued with the media that assisted living should not be held to the same standards as skilled nursing facilities where medication management and a concentration on precise record keeping is the norm.
f. Elder Abuse
The potential for elder abuse also has been a growing concern for experts in geriatric social work. Watson, Cesario, Ziemba, and McGovern (1993) have conducted research on abuse in institutional settings using Long-Term Care Ombudsman abuse reports and found that abuse, although an important problem, was relatively rare in both the nursing home and residential care setting, and that the incidence of abuse was lower in residential care settings than in nursing homes (.008 per bed per year for the residential care setting compared to .03 per bed per year for nursing homes). Concern about abuse and the vulnerability of the frail elderly in all types of group and institutional settings seems to have prompted the State of Washington to take some preventative measures. Wolcott (1994) reports that a new law in the State of Washington requires criminal background checks on all long-term care facilities and that the law applies to employees in assisted living facilities. According to the Intergovernmental Health Policy Project, some other states are now following suit.
IV. THE EFFECTIVENESS AND COSTS OF ASSISTED LIVING
This chapter focuses on the effectiveness and costs of assisted living. A number of industry experts have asserted in the recent literature that the elderly prefer assisted living over nursing homes, that assisted living can result in more positive outcomes for the frail elderly, and that assisted living is a less expensive alternative to nursing homes. After a brief summary of what the 1992 Policy Synthesis found about the effectiveness of assisted living and its costs, this chapter discusses the current "conventional wisdom" regarding the value of assisted living as a seniors health and housing opportunity, and notes the general absence of research on costs.
A. 1992 POLICY SYNTHESIS FINDINGS REGARDING THE EFFECTIVENESS AND COSTS OF ASSISTED LIVING
While many industry observers believe that assisted living is a more desirable living environment than nursing facilities, the 1992 Policy Synthesis found that there was little direct empirical evidence that the frail elderly prefer assisted living to nursing homes. There is an absence of research on the topic, but some studies support the conclusion that the frail elderly prefer to stay in their own home or reside in congregate living facilities rather than live in nursing homes. Such findings may reasonably be generalized to assisted living.
Although some researchers suggest that the elderly living in assisted living facilities are happier than nursing home residents and that their caregivers exhibit higher levels of satisfaction, the 1992 Policy Synthesis found limited research suggesting that either assertion was generally true. Empirical evidence supporting the strongly-held conventional wisdom that assisted living residents avoid institutional placement is very weak and is generally grounded in anecdotal information. The research on health and functioning outcomes, while preliminary and limited in scope, does offer some substantiation of the claim of improved health outcomes for assisted living residents.
The 1992 Policy Synthesis found that there was clear evidence of cost savings when assisted living substituted for nursing home care, but found no evidence that assisted living would reduce the aggregate system-wide costs related to caring for the frail elderly.
B. THE CURRENT LITERATURE ON THE EFFECTIVENESS OF ASSISTED LIVING
Relatively little current literature has been written on the subject of the "effectiveness" of assisted living with respect to producing desired outcomes. One empirical study has been completed on the psychological well-being of residents of congregate living settings, and another has addressed CCRC residents' health care utilization. However, major outcomes studies of the effectiveness of assisted living have yet to be produced.
1. Psychological Outcomes Research
One recently published study reports results on the psychological well-being and relocation adjustment for the frail elderly moving to a congregate living setting. No known studies have been conducted that compare residents of congregate settings to nursing home residents. In a study of seniors moving to a rural congregate setting, researchers examined the factors influencing relocation adjustment with a sample of 50 residents aged over 60 without cognitive impairment or "debilitating health problems" (Armer, 1993). The vast majority of seniors in the sample perceived their move to a congregate setting as positive (92 percent) and 66 percent reported being satisfied with their new residence. Having had a choice in relocating and the relocation setting, and a combined choice factor, all were positively and significantly correlated to scores on both the Philadelphia Geriatric Center Moral Scale and the Index of Relocation Adjustment. Predictability of the setting, the social support and the challenge of the relocation were all associated with higher scores on the adjustment scale. Since the subjects in the sample were not cognitively impaired and had no "debilitating health problems," it may not be appropriate to generalize these results to all residents of assisted living.
2. Impacts on Health Care Utilization
In two separate studies, Newcomer et al. examined the relationship of residence in a CCRC to health care utilization. In the first study, they investigated health care utilization of CCRC residents compared to a matched sample of community residents. Researchers found that when using a multivariate model to control for age, living arrangement, gender, disability, and type of residence (community or CCRC), CCRC residents were significantly more likely to use SNFs and have more nursing visits compared to community residents. CCRC residents also were less likely than community residents to use hospitals and more likely to use physician visits and outpatient surgery. Being a CCRC resident was the strongest predictor of SNF stays and nursing visits. This study confirmed previous research that found skilled nursing utilization higher among CCRC residents at the same time that it found that 40 to 50 percent of the nursing home admissions were for post-hospital or recovery from outpatient surgery. The researchers conclude that there is a substitution effect between personal care in CCRCs and nursing services (Newcomer & Preston, 1994).
In a second study, Newcomer et al. examined lifetime utilization of assisted living and skilled nursing beds for residents in seven CCRCs, excluding short-term stays in either the assisted living or skilled nursing beds. Researchers found that assisted living was a substitute for skilled nursing beds, although they cautioned that in consideration of the other variables in their model, this effect was "modest" (Newcomer et al., 1995).
These and other recent research efforts support the hypothesis that assisted living residents use more skilled nursing care than community residents, and provide empirical support for assisted living advocates' assertions that assisted living can provide a less expensive alternative to skilled nursing care. Recent research also appears to support the view that assisted living residents may be using the health care system in a new, more flexible way by using personal care in the CCRC to substitute for skilled nursing. Fewer hospital inpatient visits but more outpatient surgery, combined with either skilled nursing care or personal care in the CCRC, may indicate a change in utilization.
C. CURRENT LITERATURE REGARDING THE COSTS OF ASSISTED LIVING
This section of the literature review update focuses on systems of pricing assisted living as well as the actual costs to the consumer. Mollica et al. cite a Kane study that concluded that the general variation in long-term care costs among states was due to differences in staffing standards rather than to variations in wage levels and real estate costs in different regions (Mollica et al., p. 37). These and other variations will be discussed in this chapter.
1. Pricing Systems
A number of systems of pricing assisted living are in effect around the country. One industry observer maintains that pricing is evolving and ranges from a fixed monthly fee system to an a la carte pricing system. "This a la carte pricing flexibility typically takes one of two approaches. One approach involves approximately $4 to $6.50 a day for each 15 minutes of assistance in daily living provided. The alternative involves defining levels of assistance on a case management analysis" (Moore, 1993, p. 78).
The recent work of Mollica et al. represents an even more comprehensive examination of pricing systems nationwide. Their report indicates that all of the states use either a daily or monthly capitated rate for publicly subsidized residents. Private pay residents are charged on the basis of either a flat, fixed fee or an a la care cost structure. Oregon, Arizona, Ohio, and North Dakota all have tiered cost structures which reimburse providers based on the type and degree of ADL needs of the residents. Massachusetts, Texas, and Washington all use flat rates. New York, Minnesota, and Wisconsin have modeled their reimbursement rates on their case-mix system for reimbursing nursing homes (Mollica et al., 1995, pp. 18-19). It has been estimated that 90 percent of assisted living residents are private paying (Nichols, January 1995, p. 60).
2. Pricing Systems for Low-Income Residents: Medicaid and Supplemental Security Income (SSI)
For low-income assisted living residents, costs are reimbursed jointly by Medicaid and SSI. Medicaid pays for health care costs, while SSI pays for the housing portion of assisted living. The SSI payment is designed to pay all room and board costs, which include real estate, raw food and food service costs. Residents with incomes below $458 per month would be eligible for Medicaid, and some states may offer a Special Income Level (SIL) option. SIL allows a state to set eligibility at up to 300 percent of the federal SSI payment, or $1374 a month in 1995. For those residents who do not qualify for Medicaid due to other income, states can offer an SIL eligibility standard through a Medicaid 2176 waiver or they may establish a state supplement to the federal SSI payment. The SIL allows residents with incomes above the Medicaid eligibility level to use their own income to pay the rent in an assisted living facility (as long as the facility does not receive rent subsidies) and to use the Medicaid SIL funds to pay for the service portion. The state SSI supplement option helps those who do not have enough income to pay their rent, while preserving their Medicaid eligibility.
A wide range of costs exists for the assisted living consumer, depending on a number of factors. These factors include whether the facility is a CCRC, requires an entrance fee, is a rental congregate setting, the unit is private or semi-private, the size of the unit, the age of the facility, and the services provided and covered in the basic fee. A summary of the prices mentioned in the literature is provided in Exhibit 4.1.
3. Overall Cost Effectiveness
Mollica et al. (1995) report that assisted living has become an increasingly valuable option in the seniors housing market. State policymakers interviewed for the NASHP report indicated that assisted living has reduced reliance on nursing homes and has offered residents a more home-like environment in which to "age-in-place" (Mollica et al., 1995, p. 42). Specifically, Mollica et al. report that assisted living costs between 50 percent and 80 percent of nursing home costs in many states. The authors caution that assisted living is probably more expensive than home health care because services are needed seven days a week. However, they explain that for those persons for whom services are needed seven days a week in their home, that setting might not be the most appropriate given the strain on caregivers.
4. Cost Projections
Industry observers have also indicated that policymakers will have to address a number of questions regarding the future of costs and effectiveness in the assisted living industry. These include: will assisted living reduce spending on nursing homes? Some argue that the pattern of nursing home spending will depend on how states respond to increasing demand for seniors housing as the population ages and lives longer. Some states are said to ignore this trend and maintain a fixed supply of all long-term care services. Finally, for those states that do recognize the trend and expand supply of long-term care services, it is as yet unclear whether the growth will occur in nursing homes, community or home health care, or residential options like assisted living (Mollica et al., p. 56).
| EXHIBIT 4.1: Costs to Residents for Assisted Living | ||||||
| Name of Facility | Type of Facility | Entrance Fee | Refundable? | Monthly fee | Other | Source |
| General, national | CCRCs | $30,000 to $500,000 | $500 to $2,000 | Older Women's League | ||
| General, national | Assisted Living | $995 to $1,639 | These are median low & high rates | Kane & Wilson, 1993 | ||
| General, national | Assisted Living | $620 to $3,565 | ALFAA & Coopers & Lybrand, 1993 | |||
| Charlestown, MD | CCRC | $94,430 for 1 bedroom | 100% | $890 single rate | Multi-housing News, nd | |
| Hidden Lakes, OR | Rental congregate | None | $850 to $1,100 | Some units have a la carte meals | Multi-housing News, nd | |
| Freedom Village, CA | CCRC | $55,000 to $190,000 | 50 to 100% refundable | $900 to $1,500 | Multi-housing News, nd | |
| Victoria Manor, PA | Rental congregate | $5,735 to $6,200 | Specializes in residents with head trauma | Bowe, 1993 | ||
| Florida | Assisted Living | $750 to $2,900 | Older Women's League | |||
| Oregon | Assisted Living | $1,714 | Mean private pay | Kane & Wilson, 1993 | ||
| Oregon | Assisted Living | $1,416 | Medicaid rate | Kane & Wilson, 1993 | ||
| Washington State | Assisted Living | $1,000 to $3,700 | May depend on age of facility | Wolcott, 1994 | ||
| Standish Care, Massachusetts | Assisted Living | $1,500 to $2,000 | May depend on size of unit | Clements, 1992 | ||
| Kensington Cottages, NY, MN, ND, IA | Assisted Living for dementia patients | $2800 to $3500 | May depend on single or double occupancy | Lafreniere, 1995 | ||
| Sunrise, Kensington Park, MD | Assisted Living | $1340 to $2700 | May depend on room size and level of care | Vick, 1995 | ||
Documenting cost savings in assisted living is difficult. Projections about future use (the costs of care and the types of services that will be needed by the frail elderly) can only be estimated with current information and data. However, one empirical study does report that assisted living has reduced nursing home costs in the state of Oregon. A reduction in the supply of nursing home beds and a concomitant increase in assisted living and other residential service options have caused a decline in nursing home occupancy in Oregon. Occupancy has dropped to 83 percent at the same time that supply has dropped. These combined forces have reduced aggregate costs (Mollica et al., 1995, p. 56). In addition, a report on the Massachusetts Medicaid program projected annual savings in net state costs of $2398 per participant in assisted living (as compared to their five-year costs in a nursing home) (Mollica et al., p. 74).
V. ISSUES AND TRENDS IN REGULATING ASSISTED LIVING
As background, this chapter begins with relevant information regarding public regulation with respect to residential facilities other than assisted living. An overview of the state-level regulatory activity regarding assisted living and a discussion of the forces driving increased regulation are also provided in this chapter. Finally, we include several examples of model regulations being considered and we report on the progress being made toward industry-led accreditation.
A. REGULATORY ACTIVITIES/OTHER TYPES OF RESIDENTIAL FACILITIES FOR THE FRAIL ELDERLY
1. Board and Care
Board and care is a category of residential housing that includes assisted living (under many current state definitions). Recently, board and care has been the subject of an extensive study of the impact of regulation on quality outcomes (Hawes et al., 1995). A key finding of this study is that states with extensive (and enforced) regulations had homes with "better quality," variously measured. However, the authors found that the presence of regulations did not necessarily decrease the number of unlicensed board and care homes. Moreover, well-developed regulatory systems were not associated with more hours of staff training, more cleanliness, or less institutional character to a facility.
2. Developments in State Regulations Regarding Resident Needs and Nursing Related Services: "High Level Residential Care Facilities" (1990-1993)
In 1990 and in 1993, the Intergovernmental Health Policy Project (IHPP) collected information from the states regarding licensed facilities that met three principal requirements: (1) they serve primarily the elderly and care for a minimum of three residents; (2) they are not nursing facilities; and (3) they provide health services and licensed nurse supervision as part of residential care or are the level of licensed residential care providing the most extensive personal care support services available in the state (Lipson, 1994).
The results of the surveys indicated that between 1991 and 1993, a substantial number of states were either adding a new level of care or modifying existing regulations to expand the admission criteria and/or add provisions regarding health-related services such as medication administration. As can be seen in Exhibit 5.1, derived from the IHPP report, about one-third of the states were reported to be changing their licensing rules and nearly one-quarter were considering policy changes, frequently related to assisting living.
| EXHIBIT 5.1: Selected Changes in Licensure Standards for "Residential Care Facilities" | ||||||
| States | New Level of Care | Name Change | Expanded Care Needs/ Admissions Criteria | Addition of Medication Administration | Additional Nursing Services | Current Policy Discussions |
| Alabama | X | X | X | X | ||
| Arizona | X | X | X | X | ||
| Colorado | X | Unlicensed Staff | ||||
| Connecticut | AL | |||||
| Florida | X | X | X | X | ||
| Georgia | Extended care needs and services | |||||
| Illinois | To "demedicalize" | |||||
| Maine (1994) | X | AL | ||||
| Massachusetts | AL | |||||
| Minnesota (in process) | X | X | X | X | ||
| Missouri | X (ICF) | X | ||||
| Montana (7/1/94) | X | X | X | X | ||
| Nevada | A continuum of care | |||||
| New Hampshire | X | X | X | X | ||
| New Jersey (in process) | X | X | X | X | ||
| New Mexico (proposed) | X (Consolidataion) | X | X | |||
| New York | X | X NH | X | X | ||
| North Carolina | AL | |||||
| North Dakota (Legislative change) | X | X | ||||
| Ohio (1994) | X | X NH | X | X | ||
| Rhode Island (1/1/94) | X | X | ||||
| South Dakota | X (AL) | Medication Administration | ||||
| Utah | Allow nursing | |||||
| Vermont (1994) | X | X | X | |||
| Virginia (6/94) | X | X | X | X | ||
| Washington (Early 1994) | X | X | ||||
| West Virginia | X (for smaller homes) | |||||
| Wisconsin (1994) | X | X | AL | |||
| Wyoming (Early 1994) | X | X | X | X | ||
| Total Number of States | 12 | 2 | 17 | 16 | 18 | 10 |
| % of Responding States (47) | 26% | 4.0% | 36% | 34% | 38% | 21% |
| SOURCE: Intergovernmental Health Policy Project (IHPP) Survey, The George Washington University, 1993. KEY: AL Assisted Living ICF Intermediate Care Facility NH Nursing Home | ||||||
B. REGULATORY ACTIVITY REGARDING ASSISTED LIVING EMERGING FROM THE STATES
1. Defining Assisted Living in State Policy
Mollica et al. include an appendix in their NASHP report which lists the 18 states that have formally defined assisted living in order to categorize assisted living within a specific regulatory framework. However, these definitions vary significantly, both in their level of detail and in their focus. Like the definitions found in the trade literature, state policymakers either emphasize the role of assisted living as a supportive housing option or as a health care option for the frail elderly. A publication of AAHSA has explained the definitional problems inherent in state regulation of assisted living. Some states may define an assisted living facility (and thus, regulate it according to pertinent laws) as an adult residential care facility, while others might define it as either a home for the aged, a personal care home, or an assisted living facility (Currents, May 1995). These varying definitions create a confusing regulatory environment, and probably cause problems for assisted living operators who own facilities in several states.
2. Overview of State Regulatory Policy: What is Driving Increased Regulation?
a. State Regulatory Bodies and their Methods of Enforcement
In June, 1995, the AARP published an overview of assisted living regulatory issues. This policy brief explains that in most states Departments of Health or Social Services license and inspect assisted living facilities, usually following regulations for board and care, residential care, or domiciliary care. Enforcement of these standards is reportedly lax and few sanctions are ever imposed on facilities not meeting these standards. In addition, the sanctions are weak because few housing alternatives exist for low-income residents should their residence be closed.
The AARP policy brief argues that one explanation for the weak, unenforced regulations is a lack of consensus among the states regarding a model for assisted living. (We will discuss in the next section what models do exist.) Without a model and without any federal guidelines, state laws vary considerably with respect to services provided, admission and discharge criteria, and other issues. Recent reports of accidental deaths at several Sunrise assisted living facilities have raised the question of enhanced state oversight of assisted living in Maryland and Virginia.
The IHPP report on 1994 state legislative changes in chronic care specifically named assisted living as the residential care setting that is receiving the most attention nationally. Because it is a care option that is designed around individualized service and "managed risk," states see assisted living as a potentially cost-effective and preferred residential setting for many frail elderly who would otherwise be inappropriately admitted to a nursing facility.
b. Increased Regulation
In the findings of the NASHP report, Mollica et al. explain the conflict inherent in federal and state policy that results from the dichotomy drawn between the services and service providers involved with the frail elderly and the physical site where services are provided. The confusion created by this distinction is compounded by the funding problems facing low-income elderly persons. Chapter Four's discussion of eligibility requirements for SSI and Medicaid demonstrates the complexity of multi-policy involvement in assisted living. As Mollica et al. argue, "these incongruities highlight the contradictions of many regulatory policies and provide a sound basis for re-examining how states license, regulate, and finance long-term care for their citizens" (Mollica et al., p. 4).
Mollica et al. cite a number of reasons for the recent legislative activity around the issue of assisted living. First, as state policymakers watch residents in board and care settings grow (as a population) older and frailer, they are amending regulations to allow for a higher level of service provision in those settings in order to prevent an explosion of demand for more expensive nursing home beds.
In addition, the NAHSP report explains the significance of the aging-in-place argument in the development of new state policy. A number of states have adopted assisted living policies in order to allow older residents in subsidized housing to remain in one facility and receive higher levels of service.
A third reason for the increase in legislation is the concern that for some residents, the level of ADL need is more than their families or other caregivers can accommodate, but far less than is standard in a nursing home facility. Moreover, the home-like atmosphere of assisted living has appealed to many who support the creation of alternatives to institutional environments. Thus, policymakers have encouraged the development of assisted living for those who fall somewhere in between independent living and nursing home-eligibility.
3. Recent Specific Policy Changes Made By State Legislatures
Based on the NASHP interviews and analyses of the states' regulations and legislation, Mollica et al. report that 22 states either have legislation authorizing assisted living, a licensure category for assisted living, or an assisted living service program. The authors explain that industry representatives, like assisted living owners and developers, have played a key role in the development of the task forces and other bodies that have helped to create new assisted living legislation. Just as the report went to print, Maine and Utah finalized their regulations. The report also indicated that authorization legislation was pending in Idaho, Iowa, North Carolina, and Wisconsin. Task forces in Illinois, Louisiana, Michigan, Oklahoma, and Vermont are working to develop assisted living policies, and the state of Indiana has completed its study of assisted living. Legislation failed to pass in Montana, and that repeal or modification legislation passed in Florida (modification legislation), New York (repeal legislation), and Ohio (repeal and substitute a service program for a licensure category). Despite these modifications and repeals, Mollica et al. conclude that the trend toward development of assisted living residential options will continue in the future.
Exhibit 5.2 lists the status of legislative activity in each state. The regulations vary widely because of a number of key differences in state governance protocols and state laws. Definitions of assisted living, as stated before, differ widely. In addition, the types of financing mechanisms used and the degree of low- and moderate-income targeting are different. Finally, the reason for creating assisted living is varied among states (Mollica et al., pp. 91-92). Hawes et al. have identified additional sources of regulatory difference among the states. These issues include: 1) licensing standards that vary in terms of admission and discharge criteria, staffing ratios and training, residents' rights, etc.; 2) inspection procedures that vary in the frequency of facility inspection, the notification procedure for inspection, and the level of inspector team training; 3) the range of "enforcement remedies" that are used; and 4) the resources available to supplement the federal SSI payment (Hawes et al., 1995, p. 23).
4. Key Regulatory Issues
a. Living Unit Requirements
Mollica et al. argue that perhaps the most contentious issue in state regulation of assisted living is the question of living unit requirements. A number of states require apartment settings in order to ensure that the units are consistent with the goal of achieving a home-like environment in assisted living. The 1995 Guide to Assisted Living and State Policy focuses on regulations as they pertain to the definition of assisted living, requirements for the living unit, admissions criteria, services provided, medication, and staffing. Other literature produced recently (Clemmer, Bianculli, Fitzgerland and others) provides additional detail and informs the reader of issues around certificate of need (CON) and the implications of other legislative changes on assisted living facilities.
b. Managed Risk
Certainly one of the most significant emerging regulatory issues is the concept of "managed risk." While the regulation of risk is not directly under the purview of state policy-makers (it is a legal issue akin to durable power of attorney assignment), the expansion of this practice may become increasingly important for policymakers to consider as they begin to more extensively regulate the physical plant and care service provision of assisted living facilities. In a very concise explanation of the concept of managed risk, Mollica et al. argue that "assisted living represents a new attempt to build long-term care services on a set of principles that gives more status to individual preferences and control rather than safety" (Mollica et al., p. 58).
| EXHIBIT 5.2: Status of Legislative Activity in Each State | ||
| State | Status | Model |
| Alabama | Multiple categories are licensed based on size. | Institutional model. |
| Alaska | Statute passed in 1994. Draft regulations were issued in January 1995. | Board & Care/housing model. |
| Arizona | Demonstration program operating. | New housing and services model. |
| Connecticut | Regulations were effective December 1994. Licensure process implemented. | Licensed as a service in settings meeting certain requirements. |
| Florida | Regulations issued in 1992. Regulatory and legislative amendments are pending. An HCBS waiver has been approved to serve Medicaid recipients. | Service model in multiple settings. |
| Hawaii | A task force has been formed to pursue assisted living. Legislation directing the development of assisted living regulations modeled after Oregon and Washington and a study of Medicaid HCBS waiver options passed in April. A task force is revising the nurse practice act. | New housing and services model. |
| Idaho | A concept paper has been developed by the Residential Care Council. Legislation will be submitted by the Council for the next legislative session. | |
| Illinois | An effort is in the early phases of development through an initiative of the Illinois affiliate of the AAHSA. | |
| Indiana | Study completed in 1994. No follow up activity to date. | |
| Iowa | Legislation has passed the Senate and amendments have been added by a House committee. The bill, SF 454, has been carried over to the 1996 session when final action will be taken. Legislation is pending. | New housing and services model. |
| Louisiana | Draft regulations are being prepared as a cooperative effort by the Aging, Health and Medicaid Departments. | |
| Maine | New regulations are effective in April, 1995 that re-classify current programs. | Service model in public housing and residential care settings. |
| Maryland | Service model in elderly housing and small group homes. | Service in multiple settings model. |
| Massachusetts | Legislation creating an assisted living certification process was signed in January 1995. Regulations are being drafted. Certification process created for settings meeting specified criteria. Financing for services and housing (SSI) are available for purpose built and conventional elderly housing projects. | New housing and services model. |
| Michigan | The Department on Aging chairs a work group charged with developing recommendations. | |
| Minnesota | Assisted living has been implemented as a Medicaid HCBS service. | Licensed as a service in settings meeting certain requirements. |
| Montana | Legislation creating an assisted living category is pending. | |
| New Jersey | Regulations creating a new licensure category were implemented. Three facilities have been licensed and 35 applications are pending. | Service in multiple settings model. |
| New York | Contracts with 63 projects and 3500 units have been approved. An RFP for 700 units in New York City is being issued. Budget proposal may repeal the program. | Service in multiple settings model. |
| North Carolina | A report and recommendations were submitted March 1st. Legislation has passed and the state is currently drafting rules. | |
| North Dakota | Assisted living services are funded through the state's Medicaid waivers and two state funded service programs. | Service model in apartment settings. |
| Ohio | Legislation was passed in 1993. Regulations implementing the bill were postponed pending review by a special committee in 1994. Legislation repealing the statute, and authorizing funding for development of an assisted living Medicaid waiver has been requested by the governor. Further direction from the legislature is expected. | New housing and services model. |
| Oklahoma | A task force has been created to review and develop assisted living recommendations. A draft bill has been circulated and is being revised by the task force. | Service model. |
| Oregon | Program rules operational. | New housing and services model. |
| Rhode Island | About 45 residential care and assisted living facilities are licensed. Newer buildings offer units with private bath. | Institutional model. |
| South Dakota | Assisted living category exists in statute. Limited services allowed. | Institutional model. |
| Texas | Assisted living has been added to the Medicaid HCBS waiver. | Licensed as a service in settings meeting certain requirements. |
| Utah | Program rules have been approved; rules governing the buildings were approved by a state board in March. An amendment to the HCBS waiver will be submitted in May 1995 to add assisted living. | Covers apartment style units and models with single/double occupancy rooms with shared bathrooms. |
| Vermont | Department of Aging and Disability is developing a program as part of the process to renew their Medicaid HCBS waiver. An advisory group has been established with a subcommittee on assisted living. | |
| Virginia | Regulations allowing assisted living services in adult care residences are pending. | Institutional model. |
| Washington | A demonstration program has been expanded to 35 facilities and 1200 units. Further expansion approved. Draft rules have been developed based on the demonstration experience. | New housing and service model. |
| Wisconsin | Legislation permitting development of assisted living and providing funding for a Medicaid HCBS program was submitted as part of the governor's budget. | New housing and services model under HCBS. |
| Wyoming | Regulations upgrading board & care rules were issued. New rules allow skilled nursing and medication administration. | Institutional model. |
| SOURCE: Mollica et al., "Guide To Assisted Living And State Policy," May 1995. | ||
Many experts in the industry foresee a conflict between the goals of regulators to protect the frail elderly, and the interests of the elderly themselves who seek to retain some level of independence through managed risk contracts with assisted living operators. The recent criticism of Sunrise, for example, demonstrates that the states of Maryland and Virginia are experiencing such a conflict. While the two states appear to be responding with greater oversight of assisted living, they may have to address the arguments made by Sunrise management and the caregivers of Sunrise residents who cite the facilities' appreciation of the assisted living philosophy as the key to optimal quality of life for residents. The conundrum around risk is well illustrated in the opinion of one industry observer, "our ideas about risk in this country are changing. Risk is a moving target in this country right now" (Elizabeth Clemmer as quoted by The Washington Post, January 9, 1995).
c. Certificate of Need (CON) Laws
One of the most intriguing issues in assisted living, and in fact in the entire residential care arena, is the impact of Certificate of Need (CON) laws. In one article, an assisted living developer cited the absence of CON as a significant source of financial strain on his company because such laws often limit the competition in particular market areas. As this developer explained, "there is currently no requirement in Florida that a certificate of need or other approval need be obtained before new facilities can be constructed or existing ones expanded. Unlike the construction of new homes, which require such regulatory determination, there are few barriers to entry into the adult assisted living business. The ease of entry could cause an oversupply of facilities which could result in low occupancy levels and price cutting" (Tampa Bay Business Journal, April 28, 1995, p.3).
d. The Implications of the Americans With Disabilities Act (ADA) and the Fair Housing Amendments Act (FHAA)
As the 1992 Policy Synthesis anticipated, indirect legal and policy issues have had important implications for the assisted living industry, one of those being the implementation of the Americans With Disabilities Act (ADA). One recent article explores the impact of ADA provisions on the operations of assisted living facilities. While the ADA is a federal law, its provisions have been widely litigated in state courts. As one industry observer explains, "recent court decisions indicate that ADA does not supersede state licensure regulations restricting assisted living facilities from admitting residents with specified disabilities" (Bianculli, Provider, January 1995, p. 38). In addition, the ADA may not require an assisted living facility to apply for broader licensure status to accommodate the needs of a resident with a disability. However, because the ADA was designed to protect people with disabilities from discrimination, the law is fairly strict in its requirement that a facility have a very high standard of proof to justify a restriction on a resident with a disability. The ADA does prohibit any restriction on a resident's participation in a facilities programs, unless the restriction is the only way that the facility can appropriately respond to the resident's disability. As this article concludes, "accommodating less-able residents clearly poses significant operational and resident relations issues."
In addition to the ADA, federal amendments made to the Fair Housing Act in the 1980's potentially impact the development of assisted living facilities. Certain portions of the FHAA may serve to limit certain local regulations when those laws impinge on the rights of the disabled to equivalent housing (note that the law does not ensure "equal" housing) opportunities. The federal government, through the Department of Justice, has committed itself to defend the rights of the disabled in cases of discriminatory zoning and fire codes, which sometimes take the form of "protective" legislation, put forth in local ordinances. Those defending the cause of managed risk in the assisted living environment may ultimately conflict with supporters of protective legislation.
e. Medicaid Waiver Issues
Another central issue in regulatory policy concerns Medicaid waivers. Some industry observers have suggested, using the state of Oregon as an example, that waivers are associated with greater regulation of assisted living. One recent article explores the implications of expanded Medicaid waiver opportunities on assisted living facilities in terms of the potential for greater oversight and regulation (Fitzgerald, 1995). Oregon, which has used Medicaid waivers more extensively than any other state, is reportedly also the most strict in its regulation and oversight of assisted living. Industry leaders in Oregon, Minnesota, and Florida have indicated that states will continue to use regulations of assisted living as a way to contain Medicaid costs as waivers make assisted living a viable option for a large number of low-income frail elderly persons for the first time (Fitzgerald, 1995).
Another recent article on the links between Medicaid reimbursement and state regulation of the assisted living industry suggests that reimbursement requirements make it imperative that states tighten up their regulations for assisted living (Pallarito, 1995). This article also refers to a recent Massachusetts law (not included in either the IHPP or Mollica reports because it was signed into law in 1995) which links the use of SSI for assisted living with a very strict set of regulations for assisted living facilities. The new Massachusetts law requires state review of all assisted living facilities on a bi-annual basis, establishes certain facility standards, and confirms resident rights. In addition, the law requires that assisted living operators provide proof of their "fiscal soundness." Of all of the literature written recently on the subject of regulation, only this article suggests a link between increased regulation and positive quality outcomes.
C. MODEL REGULATIONS AND ACCREDITATION
1. No National Regulatory Model Exists
Model regulations per se have not yet appeared in the literature on assisted living. It is notable that major provider organizations (AHCA, AAHSA, ALFAA) associated with assisted living have not developed or officially endorsed formal, comprehensive model regulations. However, draft reports of possible regulatory models have emerged, and regulatory and licensure standards in a number of states may serve as models for other states considering the development or the expansion of assisted living facilities. For example, ALFAA has developed a model for its members to follow, ASHA has developed a general outline of standards, the Institute of Medicine is reviewing whether it should develop a certification process for assisted living, and the AARP has commissioned a paper with proposed model standards (Mollica et al., p. 59).
2. Potential Model Regulations
In July of 1995, ALFAA's publication, ALFAA Advisor announced the forthcoming publication of a report titled, "Draft Regulations for Assisted Living for People With Dementia." This report, summarized in great detail in the periodical, is the first-ever of its kind, and represents a benchmark against which future regulations might well be judged. Joann Hyde, the gerontologist who developed the regulations, argues that special concern for the needs of dementia patients is critical, given that they represent 30 to 40 percent of people living in assisted living facilities. Areas subject to regulation in Hyde's report include: 1) an extensive definition of assisted living; 2) licensure, registration, or certification; 3) financial support for low income residents; 4) admission and transfer criteria; 5) resident rights, risk, and autonomy; 6) medication management; 7) staff ratios and patterns; 8) staff ratios and staffing patterns for special care units; and 9) building codes and life safety.
The 1995 Guide to Assisted Living and State Policy and the AARP policy brief also examine the possibility of model regulations. The rather strict regulatory policies of the state of Oregon and other states who have implemented similar changes in assisted living regulations serve as models for other states just embarking on their own regulatory adventures. In a recent meeting of the Technical Advisory Panel for the National Study of Assisted Living, participants noted that many states appeared to be formulating their own regulations by drawing from other states' rules. "Model regulations" can provide potential alternatives, but few models are readily or completely transferable to every state.
The American Seniors Housing Association (ASHA) model regulations require certain basic services (e.g., personal care up to all ADLs) and prohibit other services (e.g., continuous nursing care defined as 24-hour nursing supervision and continued monitoring of vital signs and health status). The American Association of Homes and Services for the Aged (AAHSA) has not published model regulations, but has included "examples of outcome-oriented regulatory guidelines," related to the physical characteristics of facilities in a workbook for developers. The workbook also includes a state-by-state inventory of physical plant requirements for assisted living (HCFA Review, 1993).
The AARP, in collaboration with several industry experts, will introduce a set of model regulations in 1996 which should add an additional voice to the growing number of those interested in the regulation of assisted living.
3. Accreditation: An Alternative to or a Participant in State Regulation?
With the prospect of increased state oversight and regulation of assisted living on the horizon, many industry leaders are beginning to advocate for some sort of self-regulation through an organized accreditation process. Some believe that the industry can avoid "undesirable" licensure rules if it can regulate itself and raise all facilities to a common standard. Others disagree and argue that state regulation is inevitable. These experts insist that the assisted living industry must prepare to "meet or beat" regulatory standards. If they can exceed state regulatory expectations early on, they believe that the industry can avoid a serious financial setback at the time that the regulations are implemented.
One recent article on this topic was published in Assisted Living Today by ALFAA's Secretary (Doyle, Spring, 1995). Echoing the sentiments of the second group discussed above, Doyle argues, "I believe we need to develop an accreditation standard that promotes quality operations without stifling new operational and development approaches. If we do not promote and insist on quality operations in assisted living, the federal or state governments will mandate standards for us." Doyle lists a number of potential benefits of accreditation, including:
-
Consumers will have more choice; they will be able to discern quality more easily.
-
Lenders will be able to more readily recognize facilities to which they feel comfortable lending.
-
Managed care providers will have comfort in providing reimbursement for residents residing in accredited facilities.
-
Long-term care insurance providers will be better able to differentiate good providers.
-
The accreditation process should make regulators feel comfortable that the industry is proactively setting a standard for quality operations.
-
Accreditation could be the catalyst to bring together many national organizations in a very productive and collaborative manner.
VI. FINANCING
This chapter focuses on issues regarding financing of assisted living. In the first part of the chapter, we present a brief synopsis of the discussion of financing programs that appeared in the 1992 Policy Synthesis. In the following sections we present information on new public, public/private, and private initiatives reviewed in the literature.
A. PUBLIC FINANCING PROGRAMS AND ISSUES DISCUSSED IN THE 1992 POLICY SYNTHESIS
As the 1992 Policy Synthesis indicated, public payment programs played a limited role in financing the development of assisted living for the frail elderly, but over the past several decades a variety of programs to support housing with services have been developed. Three major trends have occurred with regard to financing. First, over time, public resources were shifted from producing new housing units to increasing support for rental assistance in existing housing. In the late 1960s, a congressional committee saw the country's primary housing problem as the lack of adequate housing for low-income families. The commission proposed a major housing construction and rehabilitation program to consist of six million units for low-income families. A Reagan commission in the 1980s found that the quality of housing had steadily improved due to earlier investments in new housing. The commission considered the new problem to be the lack of affordability of housing that was readily available and recommended cuts to the numbers of new units funded. Because housing assistance is provided through multi-year contracts, the impact of these cuts is just being felt in the early 1990's (U.S. Code Congressional and Administrative News, 1991).
A second major trend in the housing industry, as evidenced by new programs authorized by the National Affordable Housing Act of 1990 and the earlier Congregate Housing Services programs, involves efforts to combine the financing of development and construction with the financing of services. These programs have largely been in the domain of the Department of Housing and Urban Development (HUD). HUD has considered human services to be in the domain of other agencies and has traditionally avoided responsibility for even small supportive services programs (Tilson, 1990; U.S. Code Congressional and Administrative News, 1991).
The third trend, demonstrated by the new HOME initiatives, is for Congress to encourage partnerships between the federal government and states.1 These partnerships would develop such that the federal government will set broader policy direction and will rely on states to develop solutions tailored to their local needs.
In the next section, public financing programs used for assisted living are briefly introduced.2
1. Federal Programs that Can Promote the Construction of New Units by Providing Incentives For Other Investors to Fund Units
Federal incentives designed to generate investments in low-income housing by other investors are federal mortgage insurance, tax-exempt bonds, and, more recently, low income tax credits. These incentives are available to both the for-profit and non-profit sectors.
2. Federal Programs that Can Promote Assisted Living by Paying Rental Subsidies Directly to Low-Income Households
In addition to providing project-based housing assistance, the federal government provides rental subsidies directly to households. These subsidies are in the form of rental certificates which are limited to the difference between 30 percent of the tenants income and fair market rent as set by HUD, and, more recently, rental vouchers which, unlike rental certificates, allow tenants to pay any excess between 30 percent of income and fair market rents out-of-pocket. Housing vouchers are intended to provide tenants with more flexibility in their choice of housing arrangements.
3. Traditional Sources of Federal/State Funding that Can Be Used to Provide Services In Housing for the Elderly
Traditional sources which have been used to finance services in elderly housing include Medicare, Medicaid, Social Services Block Grants, the Older Americans Act, and the Supplemental Security Income Program. Medicare and Medicaid, in particular, largely have been limited to funding medical models of care in institutional settings.
4. Options for Financing Additional Home and Community-Based Services in Assisted Living Settings Under Medicaid Waivers and New Optional Service s Provisions
Some long-term care experts have voiced concerns that the availability of Medicaid to pay for nursing home care and the limited public funds for community-based care creates a "bias" toward institutionalization. Partly in response to those concerns, Congress amended the Social Security Act (which governs state options under Medicaid) to expand states' ability to pay for home and community care. The federal government has authorized a selective expansion of Medicaid services to the frail elderly in the community under Medicaid Home and Community Based Service Waivers (HCBS).
5. Federal Programs Designed to Integrate Financing for Housing and Services
A major criticism of policies for funding assisted living is that, historically, disparate funding sources for housing and services have created a fragmented delivery system that does not optimally address the needs of the frail elderly. Recently, more coordinated programs (albeit limited in scope) have been developed to begin to address these concerns. One of the earlier programs was the congregate housing services program; more recently, the National Affordable Housing Act of 1990 has generated combined housing/services initiatives as well.
6. Additional Ways In Which States Finance Assisted Living
States rely on a variety of sources to finance assisted living that include: state general revenue appropriations, state-levied fees or trust funds, and state general obligation bonds.
The 1993 State of the Senior Housing Industry Report (Gamzon, 1993), a survey of 27 individuals reputed to be leaders in the proprietary and nonprofit sectors of the retirement housing industry indicates that industry panelists thought that "principal public expenditures and regulatory actions...will be initiated primarily on the state and local government levels" (Gamzon, 1993, p. 31). These panelists maintain that the state and local emphasis will be on demonstration projects rather than sweeping funding initiatives.
B. NEW PUBLIC INITIATIVES
1. Medicaid Waiver Programs
As one result of the Omnibus Budget Reconciliation Act (OBRA) of 1981, Congress established a waiver program through Section 1915(c) of the Social Security Act to offer states alternatives to traditional long-term care services. In the past several years, a number of additional waivers have been offered through various provisions, like the Older Americans Act and OBRA 1987 and 1991. The more recent waivers went beyond funding case management, homemaker services, adult day care, and personal services, to offer funding for program design as a means of developing cost-effective alternatives for delivering long-term care services.
As of May, 1995, 14 states had federal waivers permitting Medicaid funding of services in assisted living. At this writing (February, 1996), bills restructuring Medicaid and passed by both the House and Senate eliminate the need for states to obtain federal permission (through a waiver) to use Medicaid money in assisted living.
2. FHA Mortgage Insurance
Several other noteworthy public initiatives have been discussed in the recent literature. Effective December 1994, HUD regulations are amended by Section 511 of the Housing and Community Development Act of 1992 to authorize mortgage insurance for assisted living facilities and to expand existing regulations to include refinancing of conventional assisted living facilities and to insure additions to these facilities (Federal Register, 11/29/94). A definition of assisted living facilities also was published with the announcement (see definitions in Exhibit 2.1). Occupancy by more than one person without the express consent of all is prohibited and funding must be sufficient to ensure that the facility contains dwelling units and facilities for the provision of supportive services.
In the area of financing the construction of new facilities, the 1992 Housing Act extended Section 232 of the Federal Housing Administration's (FHA) mortgage insurance program to include assisted living facilities. As the AARP policy brief has observed, "the availability of mortgage insurance for assisted living should make reliable financing easier to obtain, thereby reducing financing costs. The resulting savings can enable developers to make assisted living more available to persons with lower incomes" (Clemmer, AARP Policy Brief, 1995, p. 11).
Before the change to Section 232 was made, the HUD program was available only to skilled nursing, intermediate care, and board and care facilities. In addition, the new rules provides for improvements to the loan application process. Loans underwritten pursuant to Section 223(f) are now eligible for a streamlined application process. An article written in Provider (February 1995) explains that the FHA guarantee backing the Section 232 program will ensure that facilities participating in the program will be rated as some of the most creditworthy. The article explains that "projects may be funded with either conventional or publicly sold debt at the most advantageous rates, and not-for-profit owners may be able to access tax-exempt funding." Assuming that certain shortages are covered by FHA, ratings as high as "AAA" could be achieved by participating facilities. Industry observers have concluded that the extensions to Section 232 in addition to its central components (a 35-year amortization schedule for acquisition and refinancing of existing facilities and up to 40 years for substantial rehabilitation of existing facilities) make the program an excellent financing option for assisted living developers (Olson, 1995).
Assisted Living Today (Winter, 1995), reports that in addition to the AAA rating possibilities, the new program includes:
-
Refinance/purchase loan-to-value ratios of up to 85 percent for for-profit owners and up to 90 percent for not-for-profit owners
-
Debt service coverage ratios as low as 117 percent for for-profit borrowers and 111 percent for not-for-profit borrowers
-
The ability to fund additions and improvements as part of a purchase or refinance without a full scale renovation of the facility as was formerly required.
In order to facilitate the use of the new Section 232 mortgage insurance program, it has been reported that HUD held interactive distance learning sessions with its field offices in August 1995. HUD officials reportedly wanted to convey to state representatives that the new source of funding could be used to advance funds during project construction. It was also reported in recent literature that HUD plans to hold additional training through "distance learning" regarding assisted living in the next year.
HUD has also recommended the use of "empowerment zones" in the development of assisted living facilities. These zones, of which there are over 100 designated around the country, are slotted to receive as much as $100 million plus tax incentives for businesses to locate within their boundaries. ALFAA included an article in one of its more recent publications that suggested the use of empowerment zones by assisted living developers.
3. Other Publicly-Funded Programs
Financing for construction and mortgage costs is also available through tax-exempt bonds, and depending on the model, HUD's 202 and Congregate Housing Services Programs (Mollica et al., p. 55). HUD's 202 program is partially funding service coordinators to act as case managers, i.e., to link residents with needed services from the community. In addition, the 202 program is used as a funding source for service coordinators to act as case managers, linking residents with needed services from the community.
4. Recent State Policy Changes Regarding Assisted Living Financing
Mollica et al. report the most recent state policy changes in the NASHP study. A summary table of the findings of that report can be found in Exhibit 6.1 These state summaries reflect a growing interest in Medicaid waiver programs as a way to finance assisted living for low-income residents. Only a few states (Connecticut, Hawaii, and Wyoming) have mentioned development and construction loan incentives in recent legislation, according to Mollica et al.
Other sources have also commented on specific state policy changes regarding assisted living financing in Ohio, Texas, and Massachusetts.
The state of Ohio has established a set-aside fund that has been collecting a daily one dollar surcharge on private pay nursing home residents, and that reportedly will be used to subsidize assisted living residency for low income frail elderly without informal caregiver support if Senate Bill 192 passes (Kemper, 1994).
Texas has obtained a Medicaid waiver for 22,000 slots that will be used to place eligible frail elderly in assisted living facilities (Bowe, 1993).
| EXHIBIT 6.1: Recent State Financing Policy Changes | |
| State | Financing Policy |
| Alabama | Other than SSI, no public financing is available for assisted living. |
| Alaska | When the recently passed regulations are implemented, rates will be adjusted to reflect the level of care and regional variations across the state. |
| Arizona | Rates have been negotiated with each project within guidelines specified in the Medicaid waiver. Program administrators used rates set for adult foster care, nursing facilities, the Oregon assisted living program and the Arizona HCBS program as guidelines. Three classes of rates are negotiated based on the level of care. The SSI payment is $446 per month of which $391.10 is paid to the residence to cover room and board charges and $66/90 is retained by the resident. |
| Connecticut | The Health and Education Facilities Authority provides loans for the development o f assisted living facilities. No specific program exists to subsidize services for low-income residents of assisted living. |
| Florida | $2.3 million was approved in 1994 for 220 Medicaid HCBS waiver slots as a pilot program. The SSI benefit is $586 per month. The program reimburses the facility $750 per month for services for a total payment of $1336 (a personal allowance is subtracted from this sum). To be eligible for the pilot program, recipients must be a SSI recipient, have income under 300% of the federal SSI benefit or, for elderly and disabled applicants, have incomes under 90% of the federal poverty level. |
| Hawaii | State loans and bonds would be made available at favorable interest rates to stimulate development of assisted living. An HCBS waiver program is currently being considered. |
| Iowa | A Medicaid waiver is being considered. |
| Maryland | Eligible low-income residents may be subsidized through state general funds, based on a sliding scale. The state subsidy is capped at $550 per month in non-waiver facilities. Participants pay the difference between the state subsidy and the monthly fee. The monthly fee is capped at $1200 for residents eligible for the GSAH Medicaid waiver. These residents pay 20% of the monthly fee for room and board. |
| Massachusetts | Loans are provided by the Massachusetts Housing Finance Agency and the Massachusetts Industrial Finance Agency for the construction of assisted living projects. A supplement to the federal SSI payment would set the rate at $920 per month for single individuals in assisted living. |
| Minnesota | Under the HCBS waiver, rates for assisted living services are capped at the state share of the average nursing home payment and the total costs cannot exceed 100% of the average cost for the resident's case mix classification. |
| New Jersey | New financing options for low-income residents are being considered. |
| New York | Subsidies are available for Medicaid recipients. The service reimbursement is set at 50% of the resident's Resource Utilization Group (RUG) which would have been paid in a nursing home. |
| North Carolina | A task force re port has recommended that the Division of Medical Assistance investigate the use of funds to reimburse for personal care and that the allowance either be increased or that personal care supplies be included in the standard rate. |
| North Dakota | The state has four sources of financing: an HCBS waiver for the aged, blind, and disabled, an HCBS waiver for people with traumatic brain injuries, and two state-funded programs-a service payment for elderly and disabled and the exceptional service payment for the elderly and disabled. The programs pay providers a rate based on the resident's car e needs. The maximum payment is $50 per day. |
| Ohio | An HCBS waiver is being sought. A state SSI supplement of $700 per month will be paid to cover room and board costs. |
| Texas | The Medicaid waiver provides $29.39 per day for services for individuals in assisted living facilities. The SSI payment is $11.98 per day. |
| Utah | The state intends to amend its HCBS waiver to include assisted living. |
| Virginia | A service rate of $180 per month to cover personal care services is anticipated. Nursing care would not be included. |
| Washington | The reimbursement rate for Medicaid recipients who meet the nursing home level of care criteria is $47.37 per day, including an SSI payment of $20.31 per day and a Medicaid payment of $27.06. |
| Wisconsin | State reimbursement is limited to 85% of the average statewide Medicaid nursing home rate. |
| Wyoming | A task force report has recommended that the state offer loans to finance the development, remodeling, and construction of assisted living facilities. No subsidies exist for low-income residents. |
The Massachusetts Department of Public Welfare has applied for approval to supplement federal SSI payments to eligible individuals living in assisted living facilities (Rajecki, 1993). Assisted Living Today (Winter, 1994) reports that the Massachusetts Housing Finance Agency's ElderCHOICE program is able to issue both tax-exempt and taxable bonds for assisted living facility construction. The Group Adult Foster Care Program funds services for assisted living residents and Massachusetts can use this funding to "offset the cost of services for low income elders when underwriting a loan" (Assisted Living Today, Winter, 1994, p. 26).
C. PRIVATE/PUBLIC INITIATIVES
The recent literature refers to a few private/public initiatives in assisted living that are targeted to providing assisted living to low income frail elderly. One article proposes specific private/public collaboration ideas that can minimize costs and also provides several examples of facilities that have been developed through collaborative ventures. A second article provides two examples of private/public collaboration.
One observer argues that the future of assisted living's ability to provide housing for seniors with low or moderate income levels is dependent on the industry's innovation. He recommends using "donated lands and funds and minimize use and cost of debt" and details five strategies for non-profit and for-profit developers (Frymier, 1993):
- Create a 501(c)(3) joint venture organization to qualify for real estate tax exemption and other benefits;
- Raise community donations, combine these funds with donated land to qualify for community development block grants, and other grants;
- Leverage private donations, land, and grant funds to qualify for tax-exempt financing;
- Negotiate low-cost developer and architect fees; and
- Design facilities frugally, have smaller units and conservative common areas.
Several examples of public/private collaboration exist. One example is a municipality that has used tax-exempt bonds to construct a low-income assisted living facility; the county housing authority operates the facility. Another facility built by a for-profit developer uses community-based services to keep operating costs lower. A 501(c) (3) used church donated land and community fund-raising to obtain a state grant; the assets were leveraged to generate tax-exempt bond revenue. Qualified residents in this latter facility are funded by state personnel and congregate care reimbursement and special demonstration project funds (Frymier, 1993).
Woodside Place and Rosewood Estate are two examples of public/private collaborations in assisted living. Woodside Place in Oakmont, Pennsylvania, has leveraged grants and contributions from public foundations to obtain funding from tax-exempt bonds in a collaboration between the Presbyterian Association on Aging and Western Pennsylvania Hospital. The sliding-fee arrangement provides for higher-income residents to subsidize lower-income residents (Hamilton, 1992). Rosewood Estate in Roseville, Minnesota, has used HUD 221 funding (that no longer is available) and provision of home health services through a partnership "among residents, family, friends, and staff" keeping the costs of formal services minimal. An on-site home health agency bills services in 15-minute increments at $5 per increment, keeping costs of services low. Residents only pay for services used (Hamilton, 1992).
D. PRIVATE INITIATIVES
1. The Assisted Living Industry Is Seen As An Increasingly Attractive Investment Opportunity
While assisted living has historically had some difficulty attracting private investment, many industry leaders now believe that this trend is changing. One article reported that over the next five years, billions of dollars will be required to satisfy the assisted living industry's capital demands (Pallarito, 1995).
As AAHSA argues, financing options will increase as the lending community becomes more educated and comfortable in financing assisted living facilities (Currents, May 1995). The anticipation of greater investment community involvement in the development of assisted living projects appears to be borne out in the recent literature. According to a survey of more than 250 capital lenders across the country, lenders are becoming increasingly interested in the financial needs of long-term care facility developers. The survey, conducted by Cambridge Realty Capital Ltd. of Chicago, found that lenders have already allocated larger amount of funds toward the health care sector in 1995. Specific areas of interest for those health care funds include the long-term care and senior housing sectors. As a result of their findings, the survey researchers anticipate increased capital for senior housing over the next 24 months. With regard to specific financing preferences, the survey results (published in the ALFAA Advisor, June 1995) found that:
-
Fixed or floating rate mortgages were cited most. This is the favored approach of commercial banks, HUD, Wall Street, insurance companies, pension funds and credit companies.
-
The sales/leaseback format is the favorite approach of REITs and private investors. This method allows for ownership of real estate without operating responsibility, taking on an equity-oriented structure.
-
Construction loan/mini-perm loans work well for commercial banks and, to a lesser extent, for REITs and for HUD, which offers the most popular format.
Industry leaders have been coordinating their efforts recently so that they might better attract members of the investment community to finance the development of assisted living facilities. One tool that has been developed is a model financial feasibility study, produced by AAHSA. The guidelines produced through a joint project with Ernst and Young and KPMG Peat Marwick represents the first attempt to establish generally accepted guidelines for preparing a comprehensive financial and market feasibility study for an assisted living facility. The standards cover all of the major components of development, including the project description, proposed financing, and analysis of market demand.
2. Criteria Used By Investors To Evaluate Assisted Living Facilities
Listed briefly, the three major qualifications for investor interest in an assisted living facility are "experience, education, and equity," according to Assisted Living Today (Winter, 1994, p. 24). Members of the long-term care investment community interviewed for that article support those three criteria and they provide clarification on all points.
Experience in this case means the experience of the operator, the credit of the operator, the development team qualifications as a whole, and market acceptance as demonstrated by a reasonable historic market penetration rate in the assisted living industry.
Education involves a successful marketing strategy for both the investors and the potential market. The marketability of the proposed project, its service program and concept, the architectural design and site characteristics, the quality and maintenance of the facility, demographic information, and the ability of the facility to compete in the marketplace are all issues which the facility owner/operator must "sell" to the investors. As a representative of the Massachusetts Housing Authority has said: "developers and operators must be able to articulate their objective or mission, identify an appropriate and sufficient target market, demonstrate the ability to implement an appropriate program of services, and design a building which supports the desires and needs of its frail residents while minimizing construction and operating costs (Assisted Living Today, Winter, 1994, p. 27).
Finally, with respect to Equity, it is reported that investors like to see debt service coverage of at least 1.15. In addition, at least one of the interviewed investment sources requires lease-up reserves, as well as letters of credit for the construction and operating periods.
3. Barriers to Private Financing
One representative of a financing company has argued that the most significant barrier for the financing of assisted living is the absence of CON laws in many states. Without CON, assisted living facilities face much greater competition than nursing homes, which may be perceived by investors as a better risk (Assisted Living Today, Winter, 1994, p. 27). In addition, other investment experts have suggested that the assisted living industry needs to educate the investment community better about the growth potential of the industry and of the demographic trends that indicate a steady population for assisted living facilities. Moreover, the industry is viewed as management-intense and subject to intense regulation in the near future, two things that serve to further alienate investors. Finally, some lenders are wary of the seniors housing industry in general, due to a large number of loan defaults in the 1980's by poorly qualified developers (Assisted Living Today, Winter, 1994, p. 27).
4. Private Financing Innovations
Joint ventures in the development of assisted living have become more common recently. One article reviewed the relationship between Karrington Communities (a well-established assisted living developer) and the Sisters of Charity Health Care System, Inc. The collaboration and the unique governance structure of the joint venture are used as examples of the opportunities available for cooperative schemes in the assisted living industry. As one partner was quoted as saying, "these types of collaborative ventures should be more prevalent in the assisted living industry" (Assisted Living Today, Spring, 1995, pp. 13-14).
5. Public Offering
An additional strategy being used by some assisted living companies is the option of going public. Several articles actively followed the initial public offering (IPO) and subsequent public offerings of Assisted Living Concepts, Inc. and the Standish Care Company and there has been much speculation as to whether other assisted living companies will follow suit. At ALFAA's Spring 1995 conference, public offerings were the topic of one of the panel sessions. Capital investment opportunities were cited as the largest benefits of public offerings. SEC oversight of financial records and activities was cited as the most significant disadvantage, along with the great risk involved in a public offering.
6. The Future of Private Financing: Which Types of Investors Will Be Interested in Assisted Living in the Future?
Most respondents to the Assisted Living Today financing survey agreed that selected real estate investment trusts (REITs), commercial finance companies, community banks and savings and loans will provide most of the capital for assisted living facilities in the next five years. As the industry expands and secures its market niche, commercial banks and insurance companies are expected to join the aforementioned in the financing of new assisted living projects (Assisted Living Today, Winter, 1994, p. 28). REITs are expected to be most involved in financing loans for construction and permanent financing to some of the larger multi-home assisted living companies. Community and regional banks, on the other hand, will play a larger role in financing stand-alone facilities. The larger banks will be involved in construction/mini-perm projects and will seek takeout financing opportunities (Assisted Living Today, Winter, 1994, p. 29).
E. EMERGING ISSUES AND CONCERNS REGARDING FINANCING
Some industry experts expressed concern in recent literature that for-profit assisted living facilities serving largely private pay residents are not paying close enough attention to their financial health. In particular, these articles focused on debt burdens of senior housing facilities. Recently published benchmarks for assisted living facilities appear in the AAHSA publication, "Financial Ratios and Trend Analysis of CCAC's," AAHSA's "Operational Practices in Assisted Living," and ASHA's "State of Senior Housing 1994" report.
Proposed changes to HUD housing programs also attracted the attention of Mollica et al. The authors argue that initial reports regarding the forthcoming legislation suggests that states will be offered greater flexibility in financing the housing portion of assisted living. However, the benefits of this flexibility may be tempered, Mollica et al. suggest, if funding levels are not commensurate with the current demand for assisted living housing (Mollica et al., v.).
Finally, the impact on the development of assisted living for lower income residents of changes to Medicaid is unpredictable at this point. Some predict that reduced federal matching funds combined with fewer federal prescriptions regarding payments to nursing facilities (i.e., possible elimination of the Boren Amendment) will encourage states to shift Medicaid money to the assisted living sector. Others see the potential for states restricting scarce Medicaid dollars to the sickest of those dependent on state funds, who are more likely to be in nursing homes.
APPENDIX A. BIBLIOGRAPHY
A Caring Partnership. (1995, Spring). Assisted Living Today, 2 (3), pp. 13-14.
AAHSA Crafts First-Ever Standards On Feasibility Studies. (1995, May). Currents, 10(5), C.
AAHSA Expands Assisted Living Products. (1995, May). Currents, 10(5), C.
ALFAA Offers Guidelines For Assisted Living Regulation. (1994, Winter). Assisted Living Today, pp. 14-23.
Altman, W. M., & Parmelee, P. A. (1991). Discrimination based on age: the special case of institutionalized aged. Handbook of Psychology and the Law.
Altman, W. M., et al. (1992). Autonomy, competence and informed consent in long term care: legal and psychological perspectives. Villanova Law Review.
Armer, J. M. (1993). Elderly relocation to a congregate setting: factors influencing adjustment. Issues in Mental Health Nursing, 14, 157-172.
Assisted Living Comes Of Age. (1993). Provider, pp. 25-28.
Assisted Living Concepts Inc. Announces Closings On Three Assisted-Living Residences. (1995, March 2): Business Wire.
Assisted Living Concepts Inc. Announces Construction On Six Assisted Living Residences. (1995, April 6): Business Wire.
Assisted Living Concepts Inc. Announces Convertible Debenture Sale. (1995, August 16): Business Wire.
Assisted Living Concepts Inc. Announces Management Additions For Expanded Operations. (1995, June 15): Business Wire.
Assisted Living Concepts Inc. Announces Results For The Quarter Ended March 31, 1995. (1995, May 3): Business Wire.
Assisted Living Concepts Inc. Announces Results For The Quarter Ended June 30, 1995. (1995, July 31): Business Wire.
Assisted Living Concepts Inc. Announces Sale Of Convertible Debentures. (1995, August 3): Business Wire.
Assisted Living Concepts Inc. Breaks Ground On Three Assisted Living Residences And Announces 1995 Development Plans. (1995, January 31): Business Wire.
Assisted Living Detailed In AARP Report. (1993). Brown University Long-Term Care Quality Letter, 5, 8.
Assisted Living Facilities Create New REIT Niche. (1994). Real Estate Weekly, 40(41), A6.
Assisted Living Institute Faculty Announced. (1994, December). ALFAA Advisor, pp. 1-2.
Assisted Living Slows Decline Of Residents With Alzheimer's. (1995, June). Currents, 10(6), pp. 7.
Avalon Announces New Assisted Living Center, New Administrative Personnel. (1995, June 23): PR Newswire.
Baer, M. (1993). The differential roles of caregivers, caregiver networks, and health professionals in residential-care-home entry. The Journal of Applied Gerontology, 12(4), pp. 411-424.
Bauer, S. (1992). Sun spot: an assisted living facility provides seniors with bright indoor spaces. Restaurant-Hotel Design International, 14(3), pp. 36.
Bianculli, J. L. (1995, January). Balancing Residents' Rights. Provider, pp. 37-8.
Binstock, R. H. (1993). Aging in many places: wonderful alternatives -- for a few. The Gerontologist, 33(4), pp. 568-570.
Bowe, J. (1993, March). Specialization gains momentum -- assisted living provider adds head trauma care. Contemporary Long Term Care, pp. 38-40.
Bowe, J. (1993, September). Medicaid takes the plunge into assisted living -- cash strapped states turn to nursing home alternative. Contemporary Long Term Care, pp. 33-5, 90.
Braga, M. (1995, April 28). Assisted Living Company Plans A $3.5 Million IPO (Just Like Home Inc.; Initial Public Offering). Tampa Bay Business Journal, 15(17), pp. 3.
Brecht, S. (1994, November/December). Issues in feasibility studies. Spectrum, pp. 22-26.
Bruck, L., & Widdes, T. (1995, May). Assisted living for alzheimer's patients. Nursing Homes, 44(4), pp. 32.
Buss, D. D. (1994, January). Assisted living -- this LTC infant already has grabbed a respectable slice of market. Contemporary Long Term Care, pp. 60-1.
Caring For The Resident With Alzheimer's -- Some Practical Tips From The Alzheimer's Association. (1994). Assisted Living Today, 1(4), pp. 35-36.
Cerne, F. (1994, June 5). Consumer choice could give big boost to assisted living. Hospitals and Health Networks, pp. 72.
Chisholm, S. W. & Hahn, M. A. (!995, January/February) Emerging veterans health administration geriatric and extended care initiatives. Geriatric Nursing, pp. 42-44.
Clements, J. (1992). Developers see bright future for assisted living. Boston Business Journal, 12(23), pp. 11.
Clemmer, E. (1995). Issue brief: assisted living and its implications for long-term care, IB 20. Washington DC: American Association of Retired Persons.
Clemmer, E. (1995, February). Assisted living and its implications for long-term care. AARP, Public Policy Institute Issue Brief Number 20, pp. 1-15.
Clemmer, E. (1993, October). Developments, trends, foresight revealed in new AARP study. Provider, pp. 56.
Clipp, J. Pursuing The Frail Elderly. (1995, Summer). Assisted Living Today, 2(4), pp. 12-15.
Coleman, N., & Fairbanks, J. (1991). Licensing and new board care for the elderly. St. Louis University Public Law Review, 10, pp. 521-530.
Consumer Demand For Assisted Living Escalating. (1995, May). Currents, 10(5), A-D.
Converted Hotels Host Senior-Living Communities. (1994). Building Design & Construction, 35(8), pp. 9.
Cook, M. H. (1995, January). To ensure survival, providers will hunt for missing links. Long-Term Care News.
Coopers & Lybrand. (1993). An overview of the assisted living industry. The Assisted Living Facilities Association of America.
Davis, S. (1994). Boom in assisted-living facilities fills the care continuum gap. The Business Journal - Milwaukee, 11(26), pp. 2A.
Department of Housing and Urban Development, Office of the Assistant Secretary for Housing-Federal Housing Commissioner. (1994). Federal Register (No. R-94-1695; FR-3374-F-02).
Development Initiatives. (1995, January). NASLInews, pp. 2.
Diesenhouse, S. (1993). Housing the elderly who do not require nursing home care. The New York Times, pp. F 12(N).
Dobkin, L. (1993, January). The world or retirement housing according to AARP: opportunities and obstacles. The Spectrum, pp. 15-21.
Donabedian, A. (1988). Quality and cost: choices and responsibility. Inquiry, 25, pp. 173-190.
Dorn, S. (1993). At home again: an assisted-living residence in Minnesota offers the warmth and comfort of a big traditional house. Hospitality Design, 15(5), pp. 30.
Doyle, M. J. (1995, Spring). Assessing accreditation. Assisted Living Today, 2(3), pp. 5.
Empowerment Zones Offer Assisted Living Opportunities. (1995, July). ALFAA Advisor, pp. 1-2.
Evans, M. (1994). Seniors housing finally scores. Journal of Property Management, 59(3), pp. 28.
Evans, S. (1995, September 18). Sunrise retirement company has had its share of problems. officials, however, say things have changed. The Washington Post.
Fannie Mae pilot product increases availability of financing for elderly congregate housing. (1994). First deals recently closed in Arizona: PR Newswire.
Financing Options for Assisted Living. (1994, Winter). Assisted Living Today, pp. 24-28.
Financing Options for Assisted Living. (1994, Winter). Assisted Living Today, 1(2), pp. 24-29.
Financing Options for Assisted Living. (1994, Winter). Assisted Living Today, pp. 24-29.
Fitzgerald, S. (1995, Winter). Increased Access. Assisted Living Today, 1(2), pp. 15-19.
Fitzpatrick, B., & Taylor, R. (1994). A comparative study of quality criteria. Nursing Standard, 8(8), pp. 26-29.
Fitzpatrick, B., & Taylor, R. (1994). Patients' criteria in assessing quality. Nursing Standard, 8(38), pp. 35-39.
Folkemer, D. C. (1994). Chronic Care: An overview of 1994 state legislative activity. Intergovernmental Health Policy Project, The George Washington University.
Frymier, J. W. (1993, February). Developing a market niche for low- to moderate-income seniors. Provider, pp. 43.
Gamzon, M. (1993, June). Assisted living reigns. Contemporary Long Term Care, pp. 31-2, 91-6.
Garbarine, R. (1993, August 6). Former hotel is recast as housing for elderly. The New York Times.
Gayda, K., & Heumann, L. (1989). The 1988 national survey of section 202 housing for the elderly and handicapped (No. Pub. No. 101-736). House Select Committee on Aging, Subcommittee on Housing and Consumer Interests Committee.
Geran, M. (1993). Seccombe design. Interior Design, 64(8), pp. 96.
Gilloran, A. J., McGlew, T., McKee, K., Robertson, A., & Wight, D. (1993). Measuring the quality of care in psychogeriatric wards. Journal of Advanced Nursing, 18, pp. 269-275.
Gold, D. T., Sloane, P. D., Matthew, L. J., Bledsoe, M. M., & Konanc, D. A. (1991). A typology of care settings for memory-impaired older adults. The Gerontologist, 31(4), pp. 467-475.
Goldberg, C. (1995, February 20). Axed: LI's long term care. LI Business News, 8,1.
Gorey, K. M., & Brice, G. C. (1992). A training needs assessment among managers of federally subsidized housing: facilitating support service use by vulnerable older tenants. The Journal of Applied Gerontology, 11(3), pp. 326-342.
Hamilton, J. (1992). Partnerships: A promising mechanism for financing assisted living. Supportive Housing Options, pp. 6-7.
Hardwick, S. E., Pack, P. J., Donohoe, E. A., & Aleksa, K. J. (1994). Across the states 1994 -- profiles of long-term care systems. Washington, DC: American Association of Retired Persons.
Hasiak, M. A. (1993, March). Geriatric wellness programs promote independence for residents. Provider, pp. 68.
Hawes, C., Wildfire, J. B., & Lux, L. J. (1993). The regulation of board and care homes: results of a 50-state survey. National study. American Association of Retired Persons.
HealthCare REIT Inc. (1993, August 12). The Wall Street Journal, pp. A4.
Heumann, L. F., & Boldy, D. (1982). Housing for the elderly. St. Martin's Press.
Heumann, L. F., & Boldy, D. P. (1993). Aging in place with dignity -- International solutions relating to the low-income and frail elderly. Westport: Praeger.
HHS To Probe Subacute Market. (1995, January). NASLInews, pp. 3.
Hillhaven Expanding Assisted Living Services; Developing Eight Communities. (1995, August 8): PR Newswire.
Hodder, S. L., Ford, A. B., FitzGibbon, P. A., Jones, P. K., Kumar, M. L., & Mortimer, E. A. Acute respiratory illness In older community residents. (1995, January). Journal Of The American Geriatrics Society, 43(1), pp. 24-29.
Hoglund, J. D. (1992). Woodside place: an architectural model for serving the mentally frail. Supportive Housing Options, pp. 8.
Holbrook, A. (1992, March). Turning gray green -- The future of senior housing in America: Getting a handle on the enormity, diversity of the next century's most promising market. Multi-Housing News, pp. 22-25.
Holbrook, A. (1992, March). Underwriting housing for seniors. Urban Land, pp. 11.
Holbrook, A. (1994, April). Operational success -- the future of assisted living depends on providers' ability to maintain a personalized care philosophy and promote residents' value systems. Provider, pp. 59-60.
Housing For The Elderly. (1994). Progressive Architecture, 75(7), pp. 94.
HUD Holds First Distance Learning Session on Assisted Living. (1995, August). ALFAA Advisor, pp. 1-2.
Impallomeni, M. & Starr, J. (1995). The changing face of community and institutional care for the elderly. Journal Of Public Health Medicine, 17(2), pp. 171-178. (Great Britain)
Kalymun, M. (1990, January). Assisted living with residents in mind. Contemporary Long Term Care, 25, pp. 28-29.
Kalymun, M. (1990, January). Toward a definition of assisted living. Journal of Housing for the Elderly, 7, pp. 97-131.
Kane, R. (1995, Winter). Expanding the industry while keeping the vision. Assisted Living Today, 2(2), pp. 32-33.
Kane, R. A., & Wilson, K. B. (1993). Assisted living in the United States: a new paradigm for residential care for frail older persons? American Association of Retired Persons.
Kane, R. L. & Kane, R. A. (1995, June 7). Long-term care. Journal of the American Medical Association, 273(21), pp. 1690.
Katz, I. R., Beaston-Wimmer, P. B., Parmelee, P., Friedman, E., & Lawton, P. (1993). Failure to thrive in the elderly: exploration of the concept and delineation of psychiatric components. Journal of Geriatric Psychiatry and Neurology, 6, pp. 161-169.
Kelly Assisted Living Honors Alzheimer's Association During National Alzheimer's Disease Awareness Month. (1992): PR Newswire.
Kemper, K. (1994, August 22). Assisted living funds still denied to elderly. Business First Columbus, pp. 31.
Kirk Ridge, D. (1993). Nursing home or board & care -- making the right choice. Bedford: Mills & Sanderson.
Koco, L. (1992). Flexibility is theme of new LTC plan. National Underwriter Life & Health-Financial Services Edition, 24, pp. 13.
Koco, L. (1994). Travelers enhancing individual LTC. National Underwriter Life & Health-Financial Services Edition, 28, pp. 11.
Kolb, J. M., & Risser, S. (1993, September). Development approaches unique in rural communities. Provider, pp. 99-100.
Kramer, R. G. (1994, March). Sixty-something market: An investment niche for the 1990s. Pension World, pp. 45-46.
LaFreniere, A. (1995, July). How one builder plans to tap the elderly market. Professional Builder, 60(11), pp. 16.
Lender Survey Shows Interest in Elderly Health Care. (1995, June). ALFAA Advisor, pp. 1-2.
Lipson, L. (1994). An overview of state regulation of residential care and assisted living for the elderly: 1993. Intergovernmental Health Policy Project, The George Washington University.
Low-Income Elderly Access Continuing Care. (1995, June). Currents, 10(6), pp. 7.
MacDonald, M., Remus, G., & Laing, G. (1994). Research considerations: The link between housing and health in the elderly. Journal of Gerontological Nursing, pp. 5-10.
Macedonia, D. (1994, February). The client of the decade. Provider, pp. 53-54.
Macedonia, D. (1994, June). Design for dementia care -- treating residents with dementia in ALFs requires a facility design and philosophy that optimizes safety and autonomy. Provider, pp. 57-58.
Manard, B., Altman, W., Bray, N., Kane, L., & Zeuschner, A. (1992). Policy synthesis of assisted living for the frail elderly (No. HHS-100-89-0032). Lewin-VHI, Inc. [http://aspe.hhs.gov/daltcp/reports/polsynes.htm]
Marketing That Pays. (1994). Assisted Living Today, 1(4), pp. 15-20.
Marriot Assisted Living Community Acquired By Limited Partnership. (1995, August 11): PR Newswire.
McCarthy, M. J. (1992, December 4). Home of one's own: search for alternatives to the nursing home yields 'assisted living' -- facilities let elderly keep independence, privacy and, if they like, a pet perking up at Rackleff House. The Wall Street Journal, pp. A4.
McCroskey, E., & Gilfix, M. (1992). Housing options for the elderly: tax, care and other issues. Trusts & Estates, 131(7).
Mendelson, D. N., & Arnold, J. (forthcoming). Certificate of need revisited. Journal of State Government.
Molis. (1993, August). New directions in long term care. Provider, pp. 22-32.
Mollica, R. L., Ladd, R. C., Dietsche, S., Wilson, K. B., & Ryther, B. S. (1992). Building assisted living for the elderly into public long term care policy: a technical guide for states. The Center for Vulnerable Populations.
Mollica, R. L., Wilson, K. B., Ryther, B. S., & Lamarche, H. J. (1995). Guide to assisted living and state policy. (No. HHS-100-94-0024). National Long Term Care Resource Center, University of Minnesota, School of Public Health and The National Academy For State Health Policy. [link]
Mollica, R. L. (1995, December). Setting policy for assisted living: key issues. National Long Term Care Resource Center (University of Minnesota and the National Academy for State Health Policy). Portland, ME.
Monroe, S. M. (1995, January). Provider rates the top multifacilities. Provider, pp. 59-66.
Moon, M., Gaberlavage, G., & Newman, S. (1989). Preserving independence. Supporting needs. AARP, Public Policy Institute.
Moore, J. (1995, August). Retirement communities need a financial checkup. Contemporary Long Term Care, pp. 70-71.
Moore, J. (1993, February). Increased sophistication necessary. Contemporary Long Term Care, pp. 24,78.
Netting, F. E., & Wilson, C. C. (1994). CCRC Oversight: Implications for public regulation and private accreditation. The Journal of Applied Gerontology, 13(3), pp. 250-266.
New Assisted Living Workbook Available (No. 14, 3). (1993). Health Care Financing Review.
New NASLI Resource. (1995, January). NASLInews, pp. 4.
New Report Offers Draft Regulations for Assisted Living for People with Dementia. (1995, July). ALFAA Advisor, pp. 1-2.
Newcomer, R., & Preston, S. (1994). Relationships between acute care and nursing unit use in two continuing care retirement communities. Research on Aging, 16(3), pp. 280-300.
Newcomer, R., Preston, S., & Roderick, S. S. (in press). Assisted living and nursing unit use among continuing care retirement community residents. Research on Aging.
Newcomer, R., Preston, S., & Roderick, Sue Schock. (1995, June). Research On Aging, 17(2), pp. 149-167.
NHC Starts Construction On Two Assisted Living Projects Totaling $14 Million. (1995, April 19). Business Wire.
Nichols, S. A. Assisted Living Forum. (1995, January). The Consultant Pharmacist, 10(1), pp. 60.
Old Folks Welcome. (1995, June 17). Forbes, 156(2), pp. 98.
Olson, S. R. (1994, January). Linking services to standards -- misconceptions about alternatives to nursing facility care have created unrealistic expectations about assisted living. Provider, pp. 51-53.
Olson, S. R. HUD Toasts Assisted Living. (1995, February). Provider, pp. 31-2.
Ourand, C. (1994, July/August). Swimming upstream: retirement community attracts not-so-traditional residents. Spectrum, pp. 7-8.
Ourand, C. (1994, May/June). The era of vertical integration in senior housing. Spectrum, pp. 6-7.
Pallarito, K. (1995, May 8). Assisted living captures profitable market niche. Modern Healthcare, pp. 72-76.
Pallarito, K. (1995, May 8). States bolster industry rules. Modern Healthcare, pp. 72-76.
Pallarito, K. (1992, May 18). Opportunities await in retiree communities. Modern Healthcare, pp. 96-101.
Pallarito, K. (1994, May 23). CCRCs see slow growth, challenges in HMO care. Modern Healthcare, pp. 76-80.
Perry, C. B., & Applegate, W. B. (1985). Medical paternalism and patient self-determination. Journal of the American Geriatrics Society, 33, pp. 353-359.
Pfeiffer, E. (1995, January). Institutional placement for patients with alzheimer's disease. Postgraduate Medicine, 97(1), pp. 125-132.
Pressler, M. W. (1995, January 4). Sunrise gets $32 million investment -- Fairfax firm provides residences for elderly. The Washington Post.
Pynoos, J. (1992). Linking federally assisted housing with services for frail older persons. Journal of Aging and Social Policy, 4(3/4), pp. 157-177.
Rajecki, R. (1992, September). New REGS promote aging in place -- assisted living reaches for expanded role. Contemporary Long Term Care, pp. 46-48.
Rajecki, R. (1993, February). Assisted living gets two boosts -- HUD, Massachusetts take steps to encourage growth of projects. Contemporary Long Term Care, pp. 48.
Regnier, V. (1993, June). Innovative concepts in assisted housing -- Northern Europeans have long thrived on urban life. Lessons learned from this tradition are proving useful in designing housing and other services for elderly city dwellers. Ageing International, pp. 46-51.
Regnier, V. (1992). Assisted living: promoting independence, choice and autonomy. National Eldercare Institute on Housing and Supportive Services, 1(1), 1, pp. 4-5.
Regnier, V. (1994). Assisted living housing for the elderly -- Design innovation from the United States and Europe. New York: Van Nostrand Reinhold.
Reschovsky, J. D., & Ruchlin, H. S. (1993). Quality of board and care homes serving low-income elderly: structural and public policy correlates. The Journal of Applied Gerontology, 12(2), pp. 225-245.
Residents, Providers Identify Goals For Assisted Living. (1995, August). Currents, 10(8), pp. 7.
Retisinas, N. (1994, March/April). HUD's plan for the future of senior housing. Spectrum, pp. 23-25.
Riegel, S. (1994, February). Caring for parents: a local how-to. New Orleans Magazine, pp. 58.
Room For Improvement: The Lack Of Affordable, Adaptable And Accessible Housing For Midlife And Older Women. (1993). Older Women's League.
S., G. A. (1993, September/October). Home health agencies, assisted living, and the continuum of care. Spectrum, pp. 24-27.
Salmon, G. (1993). Caring environments for frail elderly people. New York: Longman Building Studies.
Schiffer, D. (1995, Winter). At Last, FHA financing for assisted living facilities! Assisted Living Today, 2(2), pp. 8-11.
Schnelle, J. F., Ouslander, J. G., & Blumenthal, S. (1993). Total quality management: administrative and clinical applications in nursing homes. Journal of American Geriatric Society, 41(11), pp. 1259-1266.
Seip, D. E. (1990). The survival handbook for developers of assisted living. The Seip Group.
Sheehan, N. (1986). Informal support among the elderly in public senior housing. The Gerontologist, 26, pp. 171-175.
Sheehan, N. W. (1986). Aging of tenants: termination policy in public sector housing. The Gerontologist, 26, pp. 505-509.
Smith, T., & Park, S. (1994). Deductibility of resident fees paid to assisted living facilities. Assisted Living Today, 1(4), pp. 34.
Speaking With Senator William J. Cohen. (1995, Spring). Assisted Living Today, 2(3), pp. 21-23.
Standish Care Company Announces Acquisition In Conjunction With Assisted Living of America, The. (1995, January 6): Business Wire.
Standish Care Company announces signing of a letter of intent to acquire three assisted living communities in North Carolina, The. (1993): PR Newswire.
Standish Care Company announces signing of a purchase and sale. (1993). Agreement for the acquisition of three assisted living communities in Virginia. Business, General: PR Newswire.
Standish Care Company To Acquire A Regional Chain Of Four Assisted Living Communities, The. (1995, August 1): Business Wire.
Standish Care Company To Develop, Market, And Manage A 74-Unit Assisted-Living Facility In Cambridge, Massachusetts, The. (1995, March 7): Business Wire.
State of Seniors Housing 1994, The. (1995). Coopers & Lybrand and the American Seniors Housing Association.
States Seek Medicaid Waivers For Assisted Living. (1995, May). Currents, 10(5), D.
Struyk, R., Page, D., & Newman, S. (1989). Providing supportive services to the frail elderly in federally assisted housing (No. Report 89-2). The Urban Institute.
Stuart, L. (1993, January 3). "Assisted Living" builder regroups for '90's. The New York Times, pp. 27.
Tilson, D. (Ed.). (1990). Aging in place: Supporting frail elderly in a residential environment. Glenview, IL: Scott, Foresman and Co.
Tinker, A. M. (1992). Housing for frail elderly people. The Society of Public Health, 106, pp. 301-305.
Turner, L. (1995, July 24). Boston opens supportive housing community: Huntington at symphony provides range of state-funded medical and social services. Nation's Cities Weekly, 18(30), pp. 6.
United States General Accounting Office. (1994). Older Americans Act: Funding formula could better reflect state needs (No. GAO/HEHS-94-41). Washington, DC: US Government Printing Office.
Vandervanter, P. (1993). Calculating the costs of communities with health care. Where to Retire, 2(1), pp. 63-66.
Vick, K. (1995, January 9). Death prompts Md. probe of "Assisted Living" facility -- Incident raises new issues in elderly care. The Washington Post, pp. A1, A9.
Walser, N. (1994). Picking a place. Harvard Health Letter, 19(3), pp. 9.
Want To Develop Assisted Living? Some Cautionary Advice. (1994). Nursing Homes, 43(2), pp. 58.
Watson, M. M., Cesario, T. C., Ziemba, S., & McGovern, P. (1993). Elder abuse in long-term care environments: a pilot study using information from long-term care ombudsman reports in one California county. Journal of Elder Abuse & Neglect, 5(4), pp. 954-111.
Wee, E. & Vick, K. (1995, September 10). Man dies after falling out nursing home window. The Washington Post.
WHCoA Endorses Assisted Living. (1995, May). ALFAA Advisor, pp. 1,4.
Wilson, K. B. (1992). Management philosophy: A critical element in implementing assisted living. National Eldercare Institute on Housing and Supportive Services, 1(1), pp. 1, 11-12.
Wilson, K. B. (1994). Assisted living: model program may signify the future. Brown University Long-Term Care Quality Letter, 6(15), pp. 1-4.
Witt, T. (1993, May). Admission standard contributes to long-term operating success. Provider, pp. 63.
Wolcott, J. (1994). Assisted-living centers multiply. Puget Sound Business Journal, 15(9), pp. 19.
Wright, S. P. (1995, January). Nursing facilities will reshape the assisted living market. Long-Term Care News.
Young, H. M., & Hegyvary, S. T. (1993, December). Progress report on a "Continuum of Care" partnership -- an experiment in linking up long-term care services is achieving success. Nursing Homes, pp. 29-30.
NOTES
-
The HOME program provides funding for new construction, rehabilitation acquisition, and rental assistance.
-
It should be noted that this discussion does not include any changes that may be made in final Congressional budget legislation, as debates are ongoing at the time of this writing.
OTHER REPORTS AVAILABLE
A National Study of Assisted Living for the Frail Elderly: Discharged Residents Telephone Survey Data Collection and Sampling ReportHTML http://aspe.hhs.gov/daltcp/reports/drtelesy.htm PDF http://aspe.hhs.gov/daltcp/reports/drtelesy.pdf
A National Study of Assisted Living for the Frail Elderly: Final Sampling and Weighting Report HTML http://aspe.hhs.gov/daltcp/reports/sampweig.htm PDF http://aspe.hhs.gov/daltcp/reports/sampweig.pdf
A National Study of Assisted Living for the Frail Elderly: Final Summary Report HTML http://aspe.hhs.gov/daltcp/reports/finales.htm PDF http://aspe.hhs.gov/daltcp/reports/finales.pdf
A National Study of Assisted Living for the Frail Elderly: Report on In-Depth Interviews with DevelopersExecutive Summary http://aspe.hhs.gov/daltcp/reports/indpthes.htm HTML http://aspe.hhs.gov/daltcp/reports/indepth.htm PDF http://aspe.hhs.gov/daltcp/reports/indepth.pdf
A National Study of Assisted Living for the Frail Elderly: Results of a National Study of FacilitiesExecutive Summary http://aspe.hhs.gov/daltcp/reports/facreses.htm HTML http://aspe.hhs.gov/daltcp/reports/facres.htm PDF http://aspe.hhs.gov/daltcp/reports/facres.pdf
Assisted Living Policy and Regulation: State Survey HTML http://aspe.hhs.gov/daltcp/reports/stasvyes.htm PDF http://aspe.hhs.gov/daltcp/reports/stasvyes.pdf
Differences Among Services and Policies in High Privacy or High Service Assisted Living Facilities HTML http://aspe.hhs.gov/daltcp/reports/alfdiff.htm PDF http://aspe.hhs.gov/daltcp/reports/alfdiff.pdf
Family Members' Views: What is Quality in Assisted Living Facilities Providing Care to People with Dementia? HTML http://aspe.hhs.gov/daltcp/reports/fmviews.htm PDF http://aspe.hhs.gov/daltcp/reports/fmviews.pdf
Guide to Assisted Living and State Policy HTML http://aspe.hhs.gov/daltcp/reports/alspguide.htm PDF http://aspe.hhs.gov/daltcp/reports/alspguide.pdf
High Service or High Privacy Assisted Living Facilities, Their Residents and Staff: Results from a National SurveyExecutive Summary http://aspe.hhs.gov/daltcp/reports/hshpes.htm HTML http://aspe.hhs.gov/daltcp/reports/hshp.htm PDF http://aspe.hhs.gov/daltcp/reports/hshp.pdf
National Study of Assisted Living for the Frail Elderly: Literature Review Update Abstract HTML http://aspe.hhs.gov/daltcp/reports/ablitrev.htm Abstract PDF http://aspe.hhs.gov/daltcp/reports/ablitrev.pdf HTML http://aspe.hhs.gov/daltcp/reports/litrev.htm PDF http://aspe.hhs.gov/daltcp/reports/litrev.pdf
Residents Leaving Assisted Living: Descriptive and Analytic Results from a National SurveyExecutive Summary http://aspe.hhs.gov/daltcp/reports/alresdes.htm HTML http://aspe.hhs.gov/daltcp/reports/alresid.htm PDF http://aspe.hhs.gov/daltcp/reports/alresid.pdf
State Assisted Living Policy: 1996Executive Summary http://aspe.hhs.gov/daltcp/reports/96states.htm HTML http://aspe.hhs.gov/daltcp/reports/96state.htm PDF http://aspe.hhs.gov/daltcp/reports/96state.pdf
State Assisted Living Policy: 1998Executive Summary http://aspe.hhs.gov/daltcp/reports/98states.htm HTML http://aspe.hhs.gov/daltcp/reports/98state.htm PDF http://aspe.hhs.gov/daltcp/reports/98state.pdf
INSTRUMENTS AVAILABLE
Facility Screening Questionnaire PDF http://aspe.hhs.gov/daltcp/instruments/FacScQ.pdf
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services Home [http://www.hhs.gov]