
Kelly Devers, Nicole Lallemand, Amanda Napoles, Brenda Spillman and Fred Blavin
Urban Institute
Gary Ozanich
HealthTech Solutions
ABSTRACT
This report provides an overview of current efforts for implementing electronic health information exchange (eHIE) by long-term and post-acute care (LTPAC) providers. The report describes the extent to which LTPAC providers are preparing for and implementing eHIE with their partners and assessing its impact. The report provides a review of the grey and published literature from the past 3 years and findings from discussions with 22 stakeholders representing 12 regions where eHIE initiatives involving LTPAC providers are completed or ongoing. The report also presents findings of in-depth case studies of three eHIE initiatives in which LTPAC providers participate (1 in Pennsylvania and 2 in Minnesota).
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
"Acronyms
The following acronyms are mentioned in this report and/or appendices.
| ACA | Affordable Care Act |
|---|---|
| ACC | Accountable Care Collaborative |
| ACO | Accountable Care Organization |
| ACTION | Accelerating Change and Transformation in Organizations and Networks |
| ADT | Admission Discharge Transfer |
| ALF | Assisted Living Facility |
| APCD | All-Payer Claims Database |
| API | Application Program Interface |
| ARRA | American Recovery and Reinvestment Act |
| ASPE | HHS Office of the Assistant Secretary for Planning and Evaluation |
| C-CDA | Consolidated-Clinical Data Architecture |
| CASPER | Certification and Survey Provider Enhanced Reports |
| CCD | Continuity of Care Document |
| CCW | Chronic Conditions Warehouse |
| CEHRT | Certified Electronic Health Record Technology |
| CIVHC | Center for Improving Value in Health Care |
| CMMI | Center for Medicare and Medicaid Innovation |
| CMS | HHS Centers for Medicare and Medicaid Services |
| CORHIO | Colorado Regional Health Information Organization |
| CRISP | Chesapeake Regional Information System for our Patients |
| DSM | Direct Secure Messaging |
| e-INTERACT | Interventions to Reduce Acute Care Transfers |
| eHIE | Electronic Health Information Exchange |
| EHR | Electronic Health Record |
| EMS | Emergency Medical Services |
| ER | Emergency Room |
| FFS | Fee-For-Service |
| FHIR | Fast Healthcare Interoperability Resource |
| FOA | Funding Opportunity Announcement |
| HCBS | Home and Community-Based Services |
| HEAL NY | Healthcare Efficiency and Affordability Law for New Yorkers Capital Grant Program |
| HHA | Home Health Agency |
| HHS | U.S. Department of Health and Human Services |
| HIE | Health Information Exchange |
| HIMSS | Health Information and Management Systems Society |
| HIO | Health Information Organization |
| HIPAA | Health Insurance Portability and Accountability Act |
| HISP | Healthcare Information Services Provider |
| HIT | Health Information Technology |
| HITECH | Health Information Technology for Economic and Clinical Health |
| HITPAC | Health Information Technology for Post-Acute Care |
| HL-7 | Health Level Seven |
| HRSA | HHS Health Resources and Services Administration |
| ICD-9 | International Classification of Diseases, ninth version |
| IDN | Integrated Delivery Network |
| IDSN | Integrated Delivery System or Network |
| IHIE | Indiana Health Information Exchange |
| IMPACT | Improving Medicare Post-Acute Care Transformation |
| IRB | Institutional Review Board |
| IRF | Inpatient Rehabilitation Facility |
| KeyHIE | Keystone Health Information Exchange |
| LAND | Local Adopter for Network Distribution |
| LTCH | Long-Term Care Hospital |
| LTPAC | Long-Term and Post-Acute Care |
| MAX | Medicaid Analytic Extract |
| MDH | Minnesota Department of Health |
| MDS | Minimum Data Set |
| MeHI | Massachusetts eHealth Institute |
| MiHIN | Michigan Health Information Network |
| MSIS | Medicaid Statistical Information System |
| MU | Meaningful Use |
| NF | Nursing Facility |
| NH | Nursing Home |
| OHIP | Ohio Health Information Partnership |
| ONC | HHS Office of the National Coordinator for Health Information Technology |
| PCC | PointClickCare |
| PCMH | Patient-Centered Medical Home |
| Portable Document Format | |
| PIPP | Performance-Based Incentive Payment Plan |
| QIO | Quality Improvement Organization |
| RCCO | Regional Care Collaborative Organization |
| REC | Regional Extension Center |
| RFP | Request for Proposal |
| RHIO | Regional Health Information Organization |
| ROI | Return on Investment |
| SEE | Surrogate Electronic Health Record Environment |
| SHADAC | State Health Access Data Assistance Center |
| SIM | State Innovation Model |
| SNF | Skilled Nursing Facility |
| T-MSIS | Transformed Medicaid Statistical Information System |
| TEFT | Testing Experience and Functional Tools |
Executive Summary
In this report, we describe findings related to electronic health information exchange (eHIE) involving long-term and post-acute care (LTPAC) providers. These questions cover three general areas: preparing for eHIE between LTPAC providers and their exchange partners, implementing eHIE between LTPAC providers and their exchange partners, and assessing the impact of those activities.
We addressed these questions through several methods, including:
-
A review of grey and published literature from the past three years.
-
Discussions with 22 stakeholders representing 12 regions where eHIE initiatives involving LTPAC providers are completed or ongoing.
-
In-depth case studies of three eHIE initiatives in which LTPAC providers participate (one project in the Northcentral and Northeast regions of Pennsylvania and two projects in and around Minneapolis, Minnesota).
Awareness is growing that LTPAC providers play a critical role in care coordination and related payment and delivery system reforms intended to improve quality and reduce costs. These include accountable care organizations (ACOs), hospital and post-acute care bundling, various integrated care delivery models, and Medicare's hospital readmission policy.1 eHIE between LTPAC providers and other providers is a promising and important strategy for achieving the goals of improving care coordination and quality, and reducing the cost of care.
Yet, despite the increased focus on the importance of LTPAC providers in the care continuum, results from this project indicate that integration into electronic data exchange is still in its infancy even among providers who were eligible to participate in the electronic health record (EHR) Incentive Programs. A recent Government Accountability Office report, for example, described 18 selected eHIE initiatives as being in their infancy.2 Moreover, integration of LTPAC providers into eHIE activities is generally not the robust, bidirectional exchange typically envisioned in earlier studies regarding the potential for improvements in care delivery and outcomes.3
LTPAC providers were sometimes involved in discussions and planning for eHIE in the region, However, LTPAC providers typically were not prioritized for early eHIE efforts by providers eligible for meeting meaningful use (MU), which required eHIE to meet Stage 1 and Stage 2 MU criteria for the Medicare/Medicaid EHR Incentive Programs. Additionally, since LTPAC providers were not eligible for Medicare and Medicaid EHR incentives, they often did not have certified EHR technology, necessary modules to support eHIE, or other technology solutions that would be needed to support exchange. Finally, some LTPAC providers and their trading partners were not yet convinced of the business case for exchange and/or wanted additional support (financial and technical) to implement EHRs, redesign workflows, and educate and train staff. While the fax and telephone have major limitations, moving to certified EHRs and eHIE is a significant challenge for LTPAC providers, their exchange partners, and any intermediary (e.g., Health Information Organization or vendor).
Despite these challenges, our stakeholder interviews and review of the gray literature identified 12 regions around the country where LTPAC providers are involved in the planning or implementation of eHIE and have started to engage in eHIE with key exchange partners. We conducted stakeholder discussions with stakeholders at the following organizations:
- Office of e-Health Initiatives (Tennessee);
- New York State Department of Health (New York);
- Keystone HIE (KeyHIE) (Pennsylvania);
- Massachusetts eHealth Institute (MeHI) (Massachusetts);
- Colorado Regional Health Information Organization (CORHIO) (Colorado);
- HealthInfoNet (Maine);
- Missouri Health Connection (Missouri);
- Michigan Health Information Network (MiHIN) (Michigan);
- Stratis Health (Minnesota);
- Ohio Health Information Partnership (OHIP) (Ohio); and
- Chesapeake Regional Information System for our Patients (CRISP) (Maryland).
The implementation of eHIE solutions between LTPAC providers and their exchange partners has been shaped by several factors including: the exclusion of LTPAC providers from MU Medicare/Medicaid EHR Incentive Program eligibility, an installed-base of technologies for the electronic reporting of administrative data (minimum data set, Outcome and Assessment Information Set), regional variation in the technical approaches to eHIE, the degree of hospital system competition and vertical integration within a region, financial resources for eHIE, and the strategies of national and regional LTPAC chains with facilities within a region.
In places where early progress has been made, the implementation experience has been slow and mixed. The challenges of creating an affordable, feasible and usable technological solutions is difficult--more difficult than many anticipated. As we describe further in this report, the technological solutions pursued have leveraged EHR technology that key exchange partners eligible for MU Medicare/Medicaid EHR Incentive Programs have developed, such as view-only portals, or eHIE efforts developed for other providers and now adding on LTPAC providers. Other implementation challenges have been changing technology, leadership turnover at key organizations, workflow redesign, provider concerns and misconceptions about federal and state privacy and security laws, and education and training. Other implementation challenges noted include competitive pressures and demands, lack of trust among some trading partners, and in some case legal concerns.
Lack of funding and the business case for LTPAC providers to participate in robust information exchange has led to use of opportunistic and often very local solutions. Even in markets where relatively robust exchange is occurring for acute care providers, including hospitals, laboratories, and outpatient care in clinics and physician offices, LTPAC providers most often are limited to view-only access to clinical documents and partial solutions that may be helpful short-term solutions (e.g., provider and hospital portals) but reduce incentives for adopting more robust, interoperable EHR systems.
However, a wave of new federal demonstrations and funding opportunities (e.g., ACOs, health information exchange (HIO) grants from the U.S. Department of Health and Human Services, Office of the National Coordinator for Health Information Technology and requirements and incentives is influencing eHIE initiatives and the states and providers that choose to participate in those initiatives, and could potentially encourage more widespread use of eHIE among LTPAC providers. For example, the presence of ACOs in many local markets across the United States is prompting some ACOs and key participants in portions of them (e.g., hospitals) to reach out to LTPAC providers and conversely LTPAC providers in those communities to develop eHIE capacity as a way to ensure that referrals from local hospitals continue in the future. The Improving Medicare Post-Acute Care Transformation Act also has the potential to accelerate LTPAC provider involvement in HIE through its provisions intended to encourage interoperable HIE with and by requirements for LTPAC providers reporting.
A potential wildcard in predicting LTPAC involvement in eHIE initiatives going forward is the technology used to engage in eHIE. Findings from the literature review, stakeholder discussions, and case studies suggest that those interested in advancing LTPAC involvement in eHIE initiatives should not wait for a so-called "silver bullet" that will produce seamless exchange between LTPAC providers and their exchange partners. Instead, findings suggest that the likely near-term migratory path going forward will involve Direct Secure Messaging, view-only portals through hospitals and HIEs, and, due to considerable regional variation, smaller implementation efforts and assessment of their impacts (i.e., test of specific use cases). Other new innovative pathways, such as Transform, surrogate exchange environment, application program interface, and EHR, offer promising but more mid-term and long-term solutions.
Overall, progress is being made in involving LTPAC providers in efforts to engage in eHIE across the United States. New technology solutions offer better opportunities for more robust eHIE involving a wider swath of LTPAC providers. And new policy and market dynamics are convincing LTPAC providers, hospitals, medical groups, and other providers of the value to including LTPAC providers in eHIE efforts and are facilitating more robust eHIE more generally. Relatively little research is available on the impact of these eHIE exchange efforts because of the early stages of eHIE between LTPAC providers and their exchange partners, and there also are number of methodological challenges to these studies. However, the time is ripe for targeted research and evaluations to continue learning about what works and what does not work in eHIE initiatives involving LTPAC providers. The Urban Institute team describes promising approaches to conducting a targeted quantitative impact evaluation using ACOs or integrated delivery systems or networks. The results of such an evaluation as well as other evaluations already underway will help to identify and spread promising approaches to eHIE involving LTPAC providers across the country.
Purpose and Background
There is growing awareness that long-term and post-acute care (LTPAC) providers play a critical role in care coordination and related payment and delivery reforms intended to improve quality and reduce costs, such as accountable care organizations (ACOs), hospital and post-acute care bundling, and Medicare's hospital readmission policy. Additionally, timely electronic health information exchange (eHIE) between LTPAC providers and other providers is a promising and critical strategy for achieving these care coordination, quality improvement, and cost reduction goals.
Long-Term and Post-Acute Care Providers
LTPAC providers include a wide range of providers, such as: long-term care hospitals (LTCHs), inpatient rehabilitation facilities (IRFs), skilled and unskilled nursing facilities (NFs),4 and home health agencies (HHAs). Other providers that deliver related home and community-based services (HCBS) include hospice, assisted living facilities (ALFs), and adult day care. LTPAC and HCBS providers vary by relative emphasis on: (1) medical versus social service needs; and (2) restorative and recuperative services versus services intended to maintain functioning or slow deterioration (or in the case of hospice service the delivery of palliative care).
This project focuses on skilled and unskilled nursing facilities and HHAs to the extent possible. In addition to the request for proposal (RFP) requesting such a focus, NFs and HHAs are a major component of the LTPAC provider segment, with a relatively large number of facilities, beds, and residents/patients that are transitioning to and from other health care providers, such as hospitals. Below we provide additional information about LTPAC providers, their adoption of electronic health records (EHRs), and a conceptual framework for understanding eHIE involving LTPAC providers.
According to data from the American Health Care Association, there are 15, 632 certified NFs and 1,368,351 patients in certified beds in the United States.5 In 2012, approximately 3% of the over 65 years of age United States population resided in nursing homes (NHs), and approximately 11% of the 80 years of age United States population resides in NHs.6 Further, these segments of the United States population are growing and so NF use as well as use of alternative care settings will rise.7
Home health care is another LTPAC setting that offers a possible alternative to NF care and is a segment of the LTPAC provider market that is also growing rapidly.8 U.S. Department of Health and Human Services (HHS) Centers for Medicare and Medicaid Services (CMS) data indicates that as of 2010 there were 12,311 HHAs, and 3.4 million beneficiaries receiving home health services in the United States.9
A recent issue brief by CMS, titled Medicare Post-Acute Care Episodes and Payment Bundling,10 also provides some critical information about the volume and nature of transitions of care between hospitals and LTPAC providers. Specifically, the report notes that:
-
Nearly 40% of patients discharged from the hospital received post-acute care.
-
14.8% of those patients are readmitted to an acute hospital within 30 days.
-
Use of multiple post-acute care sites within 60 days is common occurs in more than half (50.5%) of post-acute care users.
Clearly, there is a major opportunity to improve the quality, safety, and efficiency of care as patients move through the continuum of care from acute to post-acute and long-term care and the various facilities and settings in which such services are provided. LTPAC provider engagement in eHIE could potentially help to achieve improvements in quality, safety and efficiency.
But what do we know about the certified EHR capabilities of LTPAC providers, particularly NFs and HHAs? There are no nationally representative data available about the current state of certified EHR adoption and eHIE by LTPAC providers.
It is very difficult to determine current rates of EHR adoption by LTPAC providers from prior studies because the best available evidence was collected before 2009.11 Additionally, our research indicates that there is not a shared definition between LTPAC providers and their trading partners of what functionality constitutes an EHR. For example, LTPAC providers appear to indicate that the ability electronic reporting of demographic and financial data is health information exchange (HIE), while their trading partners indicate that clinical data exchange and re-use as defined under Meaningful Use (MU) is the appropriate definition. Finally, other aspects of the methods and data, such as sample frames and sizes, differ substantially across studies.
Purpose of the Study
The general purpose of this project is to study and learn from early efforts to prepare for and implement eHIE between LTPAC providers and their exchange partners (e.g., hospitals, medical groups, pharmacies, and their staffs). This includes learning from the experiences of health plans (e.g., Medicare Advantage, Medicaid agencies, Medicaid managed care plans, and commercial plans), HIEs, state policy officials, and evaluators of eHIE initiatives in addition to the experiences of LTPAC providers and their exchange partners. This project also includes developing a plan for quantitatively assessing the impact of eHIE among these providers and their trading partners on key outcomes such as 30 day post-hospital discharge readmission rates, hospital admission rates from the emergency room (ER), and total Medicare resource utilization. More specifically, the project seeks to answer the following six major research questions:
-
What community characteristics and/or programs (e.g., service delivery and payment models, special initiatives, collaborations, etc.) enabled and continue to support the electronic exchange of health information between LTPAC providers and their HIE trading partners (e.g., physicians, hospitals, pharmacies/pharmacists, etc.)? What was/is the focus of these activities (e.g., improving coordination/continuity of care, increasing efficiencies and reducing costs, identifying information exchange needs, building trust, etc.)? Over what period of time were these activities implemented prior to and during implementation of HIE activities?
-
What types of health information do the LTPAC providers and their trading partners need to support continuity and coordination of care; and how were these information needs identified? What types of information do the LTPAC providers and their trading partners create and transmit? How has the type and timing of information exchange changed since implementing eHIE?
-
What business/organizational/quality/other factors lead to the LTPAC provider's decision to engage and invest in eHIE? What eHIE methods (i.e., what technology solutions) are used to transmit information to/from the LTPAC provider and their HIE trading partners? Does the method of exchange enable the interoperable exchange and re-use of needed clinical information? What are the costs of the technology solutions?
-
What activities (e.g., technological, policy, financial and human workflow) were undertaken by the LTPAC provider to prepare for and enable the provider/staff to engage in eHIE?
-
How has the creation, transmission, and receipt of eHIE (including interoperable exchange) at times of transitions in care and during instances of shared care impacted the clinical workflow in the LTPAC settings and that of their clinical trading partners (i.e., physicians, hospitals, and pharmacies/pharmacists)? What do the LTPAC providers and their trading partners describe as being the advantages and disadvantages of engaging in eHIE with LTPAC providers?
-
What is the measureable impact of eHIE on the quality, continuity, and cost of care for: (1) the LTPAC providers; and (2) their HIE trading partners? For example, how has eHIE affected 30 day post-hospital discharge readmission rates; hospital admission rates from the ER; and total Medicare resource utilization? What is the average number of eHIE message transmissions per LTPAC admission and discharge? Can the analyses being undertaken in selected communities be extended; and if so, how? Can these analyses be applied in other communities, and if so, how?12
As described further below in the methods, data, and findings sections, the scope and degree of exchange involving LTPAC providers was less than anticipated at the project's start. While our study was able to explore questions related to preparation for and implementation of eHIE involving LTPAC providers; our study was only able to partially address some of the research questions related to the impact of eHIE involving LTPAC providers on quality, continuity, cost of care, and workflow. Nonetheless, our team has developed a feasible, high-level quantitative and mixed research method plan for studying the implementation and impact of eHIE between LTPAC providers and their exchange partners that will help address other pressing questions in the near term.
The rest of this report is organized as follows. We first describe the rich methods and data sources used, specifically a review of the literature, conversations with stakeholders involved with eHIE initiatives with LTPAC providers, and in-depth case studies in two states (Minnesota and Pennsylvania). Then, we describe and discuss our findings from a structured literature review, stakeholder discussions, and case studies conducted in Minnesota and Pennsylvania (two eHIE initiatives in Minnesota and one in Pennsylvania). The sections describing the findings are organized by three topic areas: preparation, implementation, and evaluation. We also introduce each of these sections describing the specific research questions that are answered within that section. We sought to triangulate findings from the literature review, stakeholder discussions, and case studies, but in some research we obtained limited information from one data source. For example, the literature review yielded little information about the implications of eHIE involving LTPAC providers on human workflow (in terms of both preparation activities and impact). These areas are noted in the text to the extent possible. In each section we highlight where findings from the data sources were consistent with each other and where findings diverged. We close with a discussion of issues to consider in advancing eHIE involving LTPAC providers and evaluating the impact of those efforts on quality, cost, and utilization.
Conceptual Framework
To address the six major research questions and guide our case studies and quantitative plan, we developed a conceptual framework (Figure 1 below) based on our stakeholder discussions and literature review. Conceptual frameworks identify concepts of importance for addressing the research questions and the hypothesized relationships between them. They also can help clarify the different levels or units of analysis (i.e., national, state, regional, organizational, individual providers, patient population or sub-populations). Although this conceptual framework was based on our findings from the stakeholder discussions and literature review, described in detail in the "Methods" below, we introduce and provide an overview of the conceptual framework here because it informed our selection of states and regions for case studies and it also provides a roadmap for our background and findings sections.
| FIGURE 1. Conceptual Framework for Studying eHIE Involving NH and Home Health Providers |
|---|
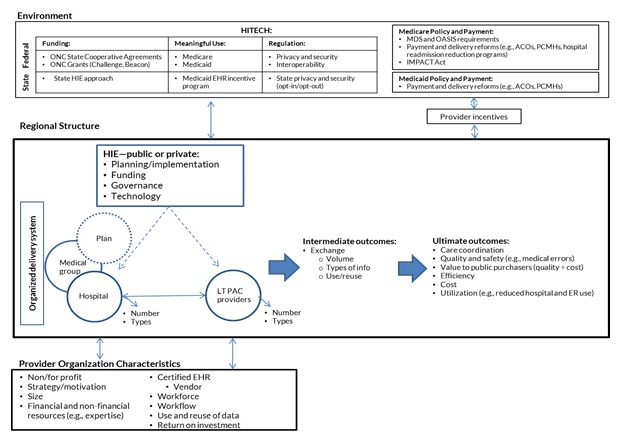 |
Several aspects of our conceptual framework are noteworthy. First, our conceptual framework is comprised of three major "levels." These include:
-
The environment or context (top row) in which specific regional eHIE efforts between LTPAC providers and their exchange partners are occurring. In general, this environment or context consists of major federal and state policies that are shaping eHIE and the behavior of LTPAC providers and their exchange partners. As Figure 1 shows, there are three major sub-components of the policy environment: American Recovery and Reinvestment Act (ARRA) Health Information Technology for Economic and Clinical Health (HITECH), Medicare Policy and Payment, and Medicaid Policy and Payment.
As described in the background and overview section and further below in our findings sections, ARRA HITECH programs have been the primary driver of eHIE efforts in various states and regions through particular programs such as the state HIE cooperative agreements and the Medicare and Medicaid EHR payment incentive programs. Although the state HIE cooperative agreements have largely ended, their experience and degree of success continues to shape whether and what kind of opportunities for eHIE that LTPAC providers and their exchange partners currently have in the region. In 2014, the HHS Office of the National Coordinator for Health Information Technology (ONC) also developed and released a ten-year vision to achieve Interoperable health information technology (HIT) infrastructure, prioritizing strategies and activities required to achieve interoperable exchange in the short and longer terms, including greater consumer and patient engagement.13
The Medicare and Medicaid EHR incentive programs defined the MU in stages and gave eligible hospitals and professionals (e.g., hospitals and medical groups but not LTPAC providers) incentives to adopt and use certified EHRs and engage in eHIE. Stage 2 MU in particular gave eligible hospitals and professionals greater incentive to engage in eHIE generally, so some began to engage in eHIE with LTPAC providers. Proposed modifications to MU in 2015-2017 and the proposed Stage 3 MU rules were released in April 2015 and the final rule was released on October 6, 2015. The 2015-2017 modifications restructures Stages 1 and 2 MU to: align them with Stage 3 in 2017 or 2018; refocus the existing program toward more advanced use of EHR technology; and align the required reporting periods for providers to support a flexible, clear framework, ensuring sustainability of the Medicare and Medicaid EHR Incentive programs. All providers will be reporting at the Stage 3 level by 2018 regardless of previous progress.14 Overall, the 2015-2017 and Stage 3 rules provide even further incentive for eHIE as the requirements related to eHIE have increased.
Finally, ONC and others at the federal and state levels have been working to further clarify, develop and strengthen privacy and security policies. Challenging issues remain in this area (e.g., trust and authentication protocols for providers, legal liability for data exchanged and accepted into an EHR, patients' ability to opt-out and/or access and control some or all of the information about their health).
Similarly, as shown to the right in the top row of Figure 1, there are major Medicare and Medicaid policy and payment changes underway that are shaping LTPAC providers and/or their trading partners incentives to engage in eHIE with one another. For example, both Medicare and Medicaid have a variety of provider payment and delivery system reform initiatives fully implemented (e.g., hospital readmission penalties) or underway (e.g., ACOs, patient-centered medical homes [PCMHs], Health Homes) that provide greater incentives to hospitals and medical groups to consider engaging in exchange with LTPAC providers. Conversely, Medicare requires LTPAC providers to collect and report assessment data such as the Outcome and Assessment Information Set (OASIS) data for home health patients and Minimum Data Set (MDS) data for NH patients and the Improving Medicare Post-Acute Care Transformation (IMPACT) Act also places additional requirements to standardize and make interoperable assessment data elements in LTPAC settings.
In some markets, private health plans with products and populations that may require NH care (e.g., Medicare Advantage Plans, Medicaid managed care organizations for certain sub-populations) are seeking to create preferred provider networks with LTPAC providers and require a willingness and ability to engage in eHIE to be in that preferred network.
Collectively, these major policy and payment areas can create greater financial and non-financial incentives for LTPAC providers and their partners to participate in eHIE.
Finally, it's important to note that in order for eHIE to occur, both parties (i.e., sender and receiver) have to be willing and able to engage in exchange. As we describe, sometimes there is a misalignment of incentives or willingness and ability between LTPAC providers and their exchange partners, so exchange does not happen at all or is constrained to particular uses and/or technological approaches. This is particularly true at this relatively early point in certified EHR adoption and use by Medicare/Medicaid EHR Incentive Program MU eligible providers, relatively limited availability of certified EHR technology (CEHRT) and use by LTPAC providers, and the early and rapidly changing nature of eHIE approaches in health care.
-
The characteristics of the region in which eHIE between LTPAC providers and their exchange partners are taking place (middle row). Of particular importance at this level are: (1) whether the region had developed a functioning and independent health information organization (HIO) and, if so, whether it was funded with federal and state funds or it was privately funded, what technological solutions it employs, and if it can be sustained; (2) the structure of the health plan, hospital, medical group and LTPAC markets; and (3) the financial and non-financial incentives present in the specific market, including things like provider payment and delivery reforms and or other major demonstrations, grants, or projects that are taking place.
Many of the regions in which we found early eHIE efforts between LTPAC providers had a relatively successful HIO (i.e., at least operationally, even if engagement with and involvement of LTPAC providers was still in the early phases) and/or one or more large integrated delivery system or network (IDSN) that dominated the market. As we describe further, in both of our case study states and regions, large IDSNs were either a founding member and sponsor of the public or private HIE (e.g., Geisinger helping start and support KeyHIE (Keystone HIE) in Pennsylvania) or served as an HIO and eventually become the certified HIO in the region or state (i.e., Allina in Minnesota).
When the HIO is either supported or closely aligned with an IDSN, it is important to consider the specific type or components of the IDSN (e.g., does it own and operate a health plan? Is it also operating as an ACO?) because these likely shape the systems incentives for and approach to engaging in eHIE with LTPAC providers, their ability to lead and organize an eHIE initiative in the region and sometimes state, and how their HIO or IDSNs actions are perceived.
Some IDSNs dominate the regional market and are perceived to have the financial resources and technical expertise to not only adopt and use EHRs but to either support a public HIO or serve as the HIO itself. However, in some case other providers fear that those IDSNs will use the information in the HIO to gain greater market power, for example, by strategically using the information in the HIO to assess referral patterns, performance of other organizations, and risk of various sub-populations. So, as one respondent noted, "eHIE often moves at the speed of trust."
Similarly, the structure of the LTPAC organizations that are not owned by the IDSN is important also. If the LTPAC providers are not owned by IDSNs, are they part of national chains (which are typically for-profit), smaller regional chains, or single or quite small providers (e.g., "mom-and-pops")? There is significant variation across regions in the structure of the LTPAC providers and their exchange partners and the hence the incentives (financial and non-financial) that they have to engage in exchange, the perceptions of the business case and/or return on investment (ROI) for adoption certified EHRs and engaging in eHIE in specific regions and states, as well as what technological solutions that are available and most desirable.
Finally, it important to note that when a public or private HIO is successfully operating, there is pressure to develop a funding mechanism and technological solution that is viable in the particular region. Initially, Medicaid and private health plans were thought to be an additional and longer term funding source for HIOs besides federal and state grant funds, but in some states Medicaid and private plans were less involved in eHIE efforts. More recently, Medicaid is playing a key role in some states, supporting HIOs and eHIE through 90-10 matching funds through the Medicaid EHR incentive program and related population health or Medicaid related provider payment and delivery reform efforts in the state, such as Medicaid ACOs, PCMHs, or Health Homes. Additionally, some private insurers have supported their own HIE (e.g., Blue Cross/Blue Shield in California). Many HIOs are reportedly struggling, but at least some HIOs appear to have developed viable, long-term funding models that serve as one viable mechanism and avenue for exchange moving forward. As noted, competitors are individual IDSNs and exchange with providers using the same EHR and EHR portals which we describe in greater detail in the findings sections.
-
The characteristics of the specific provider organizations (bottom row) in the region, including both the LTPAC providers and their exchange partners. Some key issues at this level are whether the organization has adopted a certified EHR, if so what kind, and whether they believe there is a strategic advantage and/or positive business case for engaging in exchange. If they believe there is a strategic advantage and/or positive business case for eHIE, there also is the question of what kind of data will be exchanged, for what purpose, and through which technological means.
The literature on EHR adoption and use points to a possible fourth level of analysis: that is the individual level. Specifically, individual providers (e.g., physician, nurse) and/or staff (e.g., managers, clerks) attitudes and views toward EHRs and eHIE may vary based on their own characteristics. For example, physician and other clinicians' age is negatively associated with willingness and ability to use an EHR or use all of its features, even when the practice or hospital they work in has one installed.15 Similarly, patients/residents and their family or guardians view of EHRs, eHIE, and privacy and security and related issues, such as willingness to provide consent, may vary by education, income, race/ethnicity or other individual characteristics. However, we do not include this level explicitly in our conceptual framework, as we were unable to collect much data on these issues through our case studies. Nonetheless, where our respondents reported on these issues in their own organizations, we report them.
The second noteworthy feature of our conceptual framework is that it allows for bidirectional effects of each level (e.g., environment or context) on others (e.g., region or community) and how characteristics of eHIE approaches in a specific region relate to implementation and outcomes (intermediate and ultimate) over time. For example, our stakeholder discussion, literature review, and case studies show that the federal and state environment or context has affected specific regional eHIE efforts and there is great variation across regions in both the level and types of eHIE. Conversely, promising initiatives and lessons learned about eHIE between LTPAC providers and their exchange partners can be used to help implement some ongoing HITECH programs (e.g., latest round of HIE cooperative agreement, 2015-2017 rule and Stage 3, use of Medicaid 90-10 matching funds) and other payment and delivery system reforms at the state and federal levels. As Yin has noted, one of the central contributions of case studies is to better understand what aspects of the environment or context are most important and how they affect planning, implementation, and outcomes over time.16 Others have also noted the importance of "multi-level" research and evaluation to better understand the complex environment, interactions, and outcomes of new programs or interventions.17
Finally, our conceptual framework includes both intermediate and ultimate outcomes. The ultimate outcome of interest (to the far right in the middle row) cannot be achieved until robust enough exchange occurs and this is likely to take time. That is, the volume and nature of exchange occurring clearly affects the ability to achieve improvements in care coordination and quality and reduction in total costs for the population served by the organizations in the region. Additionally, the ability to use and re-use exchanged data to achieve these ultimate outcomes requires robust but affordable technological solutions as well as workflow redesign and related education and training. While LTPAC providers and their exchange partners are in the early stages of exchange, as described in further detail in our finding section, we have identified some promising states and regions throughout the country where research and evaluation on intermediate and ultimate outcomes could potentially take place. Further information on possible outcome or impact analysis can be found in the "Impacts and Evaluation" portion of the paper.
Methods
This study sought to answer the research questions listed above by conducting a systematic review of the literature (peer-reviewed and gray) over the past five years, semi-structured discussions with key informants throughout the country (N=22), and site visits to two states (the Urban Institute team studied two initiatives in Minnesota, one in Pennsylvania) in the United States where eHIE involving LTPAC providers is more advanced in planning and early implementation activities compared to most areas of the country.
The Urban Institute team used each data source for a different purpose. The literature review was used to collect information on past and ongoing efforts to plan, implement, and evaluate eHIE involving LTPAC providers that was published over the past three years. The Urban Institute team built on this knowledge by engaging in discussions with key stakeholders in eHIE initiatives involving LTPAC providers across the United States. The Urban Institute team used these discussions to explore the latest planning, implementation, and early evaluation developments in eHIE involving LTPAC providers with an eye toward identifying two communities that could be the focus of more in-depth case studies. The Urban Institute team gained further more in-depth insight into the planning, implementation, and evaluation efforts of three eHIE initiatives involving LTPAC providers by conducting case studies of those initiatives.
The Urban Institute team used the information obtained through the targeted review of the literature and key informant discussions to also develop a conceptual framework for understanding how LTPAC providers and their trading partners prepared for the implementation of eHIE, and the impact of this exchange on clinical workflow, work force, and the quality, continuity, and cost of care the LTPAC providers and their HIE trading partners. The Urban Institute team used the information gained through the review of the literature, the stakeholder discussions as well as the newly developed conceptual framework to identify several sites of eHIE activating involving LTPAC providers that could be the subject of more in-depth case studies.
Literature Review
A systematic approach was used to identify and synthesize current literature (peer and non-peer-reviewed) on the planning, implementation, and impact of eHIE, particularly as they pertain to LTPAC settings, providers, and care coordination. First, in consultation with a research librarian, search terms were developed. Second, the search terms were applied to the databases EBSCOhost, Medline and Scopus to identify relevant literature. We initially focused our initial search to the last five years (2009-2014). We also conducted a targeted review of websites from government and professional associations to identify any relevant materials. Using these two literature review approaches, the research team identified a total of 2,021 articles for review.
Researchers then reviewed abstracts. Articles published prior to 2011 (the last three years of literature) that did not meet inclusion and exclusion criteria were eliminated, reducing the total to 303 articles. Finally, the 303 full articles were reviewed by members of the research team, and extraneous articles were eliminated. This process resulted in a final set of 74 peer-reviewed and non-peer-reviewed articles or materials. Appendix A contains citations for all considered (fully reviewed and included) articles.
Stakeholder Discussions
The research team used the stakeholder discussions to explore the latest planning, implementation, and early evaluation developments in eHIE involving LTPAC providers with an eye toward identifying two communities that could be the focus of more in-depth case studies. Using information from informal discussions with federal officials overseeing eHIE programs and the non-peer-reviewed literature; the research team developed an initial list of informants. In total, 17 discussions were held with 22 individuals representing 12 regions around the country.
Case Studies
Using the information obtained through the literature review and key informant discussions as well as our conceptual framework (described above), the Urban Institute team identified several sites of eHIE activity involving LTPAC providers that could be the subject of more in-depth case studies. The sites selected for more in-depth case studies were chosen in part because their markets for exchange between LTPAC providers (especially NFs and HHAs) and their exchange partners were considered relatively mature. The Urban Institute team developed and used a number of criteria in conjunction with the project officer's input to select alternative case study sites. Overall, these criteria allowed the research team to assess the potential pros and cons of various regions/states, their potential complementarity, and generalizability of case study results. For example, we sought to identify a region with a relatively mature market for exchange between LTPAC providers (especially NFs and HHAs) and their trading partners so they had more experience on which to draw and perhaps some early insights into impacts. Additionally, we considered the technological approach using, including public HIEs, private HIEs, vendor networks, and portals, allowing us to capture the diverse ways eHIE is being achieved, technologies that are more likely to be scaled up and spread (rather than unique, homegrown systems), and the implications for things like workflow and impact. Finally, we sought to identify sites that would welcome the research team.
After reviewing and discussing that list, our HHS Office of the Assistant Secretary for Planning and Evaluation (ASPE) project officer selected three initiatives across two states for case studies and site visits: KeyHIE in the Northcentral/Northeast region of Pennsylvania and the Fairview-Ebenezer and Benedictine initiatives in and around Minneapolis, Minnesota.
In summer 2015, the Urban Institute team conducted 43 interviews with 47 respondents in site visits to Pennsylvania and Minnesota. In Pennsylvania, the team held 19 interviews with 21 respondents; in Minnesota, 24 interviews with 26 respondents.
After completing the site selection process, the Urban Institute team began identifying the key organizations and informants that should be targeted for interviews during the in-person site visits as well as the most appropriate points of contact for securing those interviews. The types of informants sought for interviews included:
-
Clinical personnel such as physicians, nurses, medical assistants, office managers, and EHR/HIT staff from providers participating in the programs in the selected sites (including NFs, HHAs, hospitals, organized delivery systems, and medical groups).
-
Local and state leaders.
-
Plan and payer representatives.
-
eHIE evaluators.
-
Other stakeholders with experience and knowledge of eHIE.
To identify the most appropriate organizations and respondents for site visit interviews, the Urban Institute team used several strategies. First, the team had informal discussions with key stakeholders including state staff and, in the case of KeyHIE, HIE leadership. Second, the Urban Institute selected participating providers for interviews with the goal of having some variation in the following characteristics:
- Ownership or type (e.g., hospital or system owned, non-profit or for-profit);
- Geographic setting (urban/suburban/rural);
- Size; and
- Teaching status.
Third, the Urban Institute team inquired about other people informants thought we should interview. Through this "snowball sampling" procedure, we built a more robust list of individuals and organizations potentially able to participate in interviews.
The Urban Institute team developed and received approval from the Urban Institute's institutional review board (IRB) to use four interview protocols targeting different types of respondents. The use of four protocols (rather than one) allowed interviewers to more easily direct questions to the most appropriate respondent. For example, we directed more technical questions about a provider's technology tools toward the organization's EHR/HIE lead, and workflow related questions toward that provider's clinical staff. Since the interviews were semi-structured, interviewers were able to ask other questions and probes as needed.
The Urban Team conducted the site visits in summer 2015 using two pairs of interview teams. Each interview team consisted of a lead interviewer and a note taker. Interviews were also recorded to facilitate polishing interview notes taken during the site visit and to produce interview notes for the interviews in which there were only audio recordings. The team conducted some interviews after the site visit due to scheduling conflicts and the geographic distance of some respondents. All interview notes were cleaned and analyzed at the end of each respective site visit. In addition, during the site visit, the team discussed preliminary findings, which covered key topics to describing findings from the site visits and was used to inform the site visit memoranda. The Urban Institute team also received follow-up materials from some respondents to provide additional information on the topics covered during the interview. Findings from each site visit were summarized in memoranda.
Findings from both site visit memoranda were synthesized in the final report to illustrate how the initiatives examined overlapped and where they differed in approach and outcomes in order to identify key lessons learned and potentially generalizable findings.
|
Description of Case Study Site: Minnesota Our team studied two initiatives in Minnesota at varying stages of eHIE implementation and usage. The first was the Benedictine-Allina initiative. Exchange of patients' clinical information between the one participating Benedictine Health System (BHS) NF (St. Gertrude's) and the one participating Allina hospital (St. Francis) is performed by creating, sending, and receiving a Continuity of Care Document (CCD) using each facility's EHR. The two facilities are located on the same property, share many patients, but do not have the same EHR vendor. Exchange with other trading partners is still largely performed via fax. The second initiative is the Fairview-Ebenezer initiative, which is in the planning phases and builds off previous grant-funded work. This project focuses on improving the eHIE capacity of providers serving Burnsville, Minnesota. Fairview Health Services is the lead organization of a collaboration that includes Ebenezer and Burnsville Emergency Medical Services (EMS). Fairview owns Ebenezer but not the Burnsville EMS. Fairview-Ebenezer eHIE implementation is pending award of the State Innovation Model (SIM) testing grant. In both initiatives, hospital portals are the most common way that LTPAC providers view patient data from trading partners, which only provides information about a patient's most recent acute care encounter and is only uni-directional exchange. Minnesota was selected in part because it has a unique provider landscape. Most of the hospitals and physicians serving the region are owned or affiliated with one of several systems (e.g., Allina Health, Fairview Health Services) or multi-specialty group practices (e.g., Fairview Physicians Associates). There is also a high preponderance of LTPAC providers in Minnesota, many of which are part of senior service health systems including both initiatives studied (e.g., BHS and Fairview Health Services). Additionally, ACOs are common in Minnesota. For example, both Fairview and Allina are ACOs under CMS' Pioneer ACO Program. Minnesota's approach to eHIE is also unique. Rather than supporting a state-wide HIE or regional public HIOs, the state has taken a market-based approach to HIE, granting funds to private organizations to stand up exchange within communities. This has created a relatively decentralized and market driven model that operates within the boundaries of an overarching state plan and regulatory framework. Finally, Minnesota has implemented state laws to spur adoption of eHIE including a 2005 EHR mandate for most providers. There are also two active and influential associations in Minnesota for "older adult services" (LeadingAge and Care Providers) that have been instrumental in securing exemptions for post-acute care providers from the state's EHR mandate18 (described below) and will be contributing to the LTPAC Roadmap, which further defines the future of eHIE with LTPAC providers in Minnesota. Despite these favorable conditions, eHIE with LTPAC providers remains limited in Minnesota. |
|
Description of Case Study Site: Pennsylvania KeyHIE is a national leader in HIT. Founded in 2005. KeyHIE is one of the oldest and largest HIEs in the country. Originally under the umbrella of Geisinger Health Systems, KeyHIE is backed by decades of health care innovation and serves close to 4 million patients in the Northcentral/Northeast region of Pennsylvania. KeyHIE currently has 18 LTPAC facilities connected, and has plans to bring on an additional 55 over the next three years as part of a grant from the HHS Health Resources and Services Administration (HRSA). KeyHIE offers participating providers three HIT solutions: KeyHIE (query-based) Transform, MyKeyCare and is now implementing Direct Secure Messaging (DSM). KeyHIE was selected because the Northcentral/Northeast region of Pennsylvania is further advanced in implementing eHIE with LTPAC providers than most regions of the country. This is largely a result of the leadership provided by the Geisinger Health System as one of the initial sponsoring organizations for KeyHIE. Geisinger dominates the region; it currently shares data with KeyHIE and also extends its network through EpicCare Link, a portal for community providers. Finally, KeyHIE was selected because of its development and use of the Transform tool, which takes MDS and OASIS data and converts the clinically meaningful information to a CCD. This CCD can be exchanged using KeyHIE so that the all participating provides could access the CCD. The Transform tool is inexpensive relative ($500 per year for facilities with 99 beds or below) to the cost of interfacing with an exchange, which appeals to LTPAC facilities who may otherwise not be able to afford to participate in information exchange. Use of the Transform Tool is spreading to other regions and communities (e.g., Colorado, Delaware, and Illinois). |
Below, we discuss findings from the literature review, stakeholder discussions, and case studies related to
- Preparing for eHIE between LTPAC providers and their exchange partners;
- Implementing eHIE between LTPAC providers and their exchange partners; and
- Assessing the impact of eHIE between LTPAC providers and their exchange partners.
Findings: Preparing for Ehie Between Ltpac Providers and Exchange Partners
This section seeks to answer the following research questions:
-
What community characteristics and/or programs (e.g., service delivery and payment models, special initiatives, collaborations, etc.) enabled and continue to support the electronic exchange of health information between LTPAC providers and their HIE trading partners (e.g., physicians, hospitals, pharmacies/pharmacists, etc.)? What was/is the focus of these activities (e.g., improving coordination/continuity of care, increasing efficiencies and reducing costs, identifying information exchange needs, building trust, etc.)? Over what period of time were these activities implemented prior to and during implementation of HIE activities?
-
What business/organizational/quality/other factors lead to the LTPAC provider's decision to engage and invest in eHIE?
-
What activities (e.g., technological, policy, financial and human workflow) were undertaken by the LTPAC provider to prepare for and enable the provider/staff to engage in eHIE?
There was one research question in the RFP relating to cost of eHIE solutions that we were unable to answer. Federal and state grants that were used to stand up the exchange initiatives are identified in this section. However, fees used to sustain HIE were deemed proprietary information and HIEs unwilling to publicly disclose fee schedules. This section will instead focus on the costs associated with standing up eHIE in a region and the grants that supported those efforts. We will additionally discuss federal and state policies, programs and reforms that impact a regions planning for eHIE.
Funding and Financing
As shown in the environment or context (top row) level of the Conceptual Framework, federal cooperative agreements, grants, or demonstrations were the initial source of funding for eHIE initiatives with LTPAC providers. Nearly every organization that we spoke with in our stakeholder discussions and on our case study site visits, save for one, had been the beneficiary of federal funds for enabling eHIE. Specifically, cooperative agreements and grants administered through ONC programs played a major role. A few initiatives also received state funds to stand up exchange.
Though ARRA HITECH provided the initial spark for federal and state funding for EHR adoption, HIE, and MU, all of our data sources affirmed that private efforts and funding for eHIE and LTPAC providers will become increasingly critical to sustaining eHIE with LTPAC providers in the future. This means an intensified search for cost-effective eHIE solutions that show a ROI for not only Medicare and Medicaid but key provider groups that must participate in and support exchange.
Federal
Our stakeholder interviews highlighted the many sources of federal funding that HIEs could capitalize on to recruit and initiate exchange with LTPAC providers. Some HIEs leveraged funds under their State HIE Cooperative Agreement Programs. For example, some stakeholders were the recipients of ONC Challenge grants, which provided additional funds for breakthrough innovations in HIE to regions participating in the State HIE Cooperative Agreement Program.19 Four states targeted in our stakeholder discussions focused their efforts as Challenge Grant awardees on HIE involving LTPAC providers (e.g., Colorado, Indiana, Massachusetts, and Maryland).20 Similarly, several states that participated in our stakeholder discussions (e.g., Indiana, Maine, and Pennsylvania) targeted LTPAC providers as part of their Beacon Community Program Agreement efforts.21
Through our stakeholder discussions we identified one CMS Medicare Quality Improvement Organization (QIO) initiative that operated from 2012-2013 provided technical assistance to LTPAC and other providers in Colorado, Minnesota, and Pennsylvania through the HIT for Post-Acute Care Special Innovation Project (HITPAC).22 This initiative helped providers optimize their use of HIT to support medication management, care coordination in transitions of care, and advancements in HIE.23
We further studied some of the LTPAC providers involved in this initiative during our case study site visit to Minnesota. In September 2012, the Minnesota-based QIO Stratis Health was awarded a one-year $1,139,858 contract with CMS through its 10th Scope of Work24 to help NFs further adopt EHRs and work towards eHIE. After completing the HITPAC project, eHIE activities were suspended, but Ebenezer sought opportunities to keep eHIE momentum going from and continue pursuing eHIE between NFs and acute care. As a result, Ebenezer pursued a Performance-Based Incentive Payment Plan (PIPP) grant from the State of Minnesota to continue pursuing eHIE in the form of DSM, Tiger Texting, lab integration and CCD exchange (described below).
CMS Center for Medicare and Medicaid Innovation (CMMI) Demonstration Program provides grant funds to support a variety of activities, including to identify solutions that reduce hospital admissions. Some of the stakeholders we interviewed are using these funds to pursue eHIE between hospitals and targeted LTPAC providers. For example, the Curators of the University of Missouri was awarded a Health Care Innovation Award Initiative to develop and strengthen eHIE between hospitals and NHs and HHAs.25
Finally, some states may apply for and receive SIM grants to support eHIE and related efforts with LTPAC providers. SIM grants provide funding and technical assistance to states to develop and test delivery models to improve performance and quality while decreasing costs.26 The Fairview-Ebenezer initiative studied in Minnesota, for example, sought but has not yet received a SIM Model Test Award to enable exchange of data between NFs and EMS.
As of our case study site visit, Ebenezer had received a developmental grant, which provided about one year of funding, from June 2014 to May 1, 2015. They have since solicited an implementation grant from the state, and anticipate learning whether they will be awarded funds by end of summer 2015. As of September 30, 2015 Ebenezer has not been awarded a Round 2 grant to pursue implementation of eHIE.
On the other hand, the Benedictine initiative also studied in Minnesota, was unable to apply for SIM dollars because they proposed using funds to continue developing software capabilities. Reportedly, the state cannot or will not pay for development of software capabilities through this grant.
One of our case study sites (KeyHIE) leveraged many of the federal grants described above to implement eHIE. In 2004, AHRQ awarded Geisinger a $1.5 million grant to "develop a secure web-based network that links participating hospitals and other health care providers in the region, providing seamless and secure access to patients' health information, including diagnoses, test results, allergies, and medication lists."27 In 2010, ONC awarded Geisinger a three-year Beacon Community grant totaling $16 million. Geisinger used the grant to build on its KeyHIE efforts and extend the benefits of other Geisinger-led HIT initiatives to other providers in the community.28 KeyHIE, incorporated as an independent corporation under the Geisinger Foundation in December 2013, is now its own legal corporate entity that reports to Geisinger leadership but is governed as a community resource. Soon after, in 2014, HRSA awarded KeyHIE a three-year grant for $900k to expand its network to 55 LTPAC providers in Pennsylvania. Grant funds will be used to develop on three HIT solutions within KeyHIE--KeyHIE Transform, MyKeyCare and DSM.
Some other federal resources--financial and non-financial, direct or indirect--are available to help financially support eHIE efforts generally or with LTPAC providers more specifically. For example, under the Medicaid EHR Incentive program states are eligible for a 90-10 match for certain Medicaid HIE related activities and while states cannot directly support HIE efforts with LTPAC providers, development of the HIE infrastructure may indirectly facilitate HIE between LTPAC providers and other providers over time. The 2015-2017 modifications restructures Stages 1 and 2 MU requirements for MU of certified EHRs supports settings and use cases across the care continuum. Several criteria are applicable to LTPAC providers including those around transitions of care, care plans, privacy and security, and potentially other areas.29
As note previously some of the major federal ARRA HITECH programs specifically designed to foster eHIE development and innovation came to an end (i.e., first major phase of state HIE cooperative agreements, Beacon). According to our stakeholder interviews, this has left some eHIE organizations and providers struggling to find funding sources to support further HIE infrastructure development and to sustain and expand current efforts. An ONC funding opportunity announcement (FOA) to support additional HIE efforts was released in early summer 2015. Initially only $28 million of awards were anticipated; the final FOA also resulted in ten $1 million grants for a total of $38 million in HIE investment.30 Through this effort three states (Colorado, Delaware, and Illinois) will be supporting eHIE with LTPAC providers. This level of funding is much lower than at the high of the ONC State HIE Cooperative Agreement program, which awarded $540 million.31
State
The literature identified some sources of state funding for HIE with LTPAC efforts. The most notable example is the Healthcare Efficiency and Affordability Law for New Yorkers Capital Grant Program (HEAL NY).32 HEAL NY, which started in 2006, represents more than an $800 million investment of public-private funds in EHRs and eHIE and aims to develop a health information network for New York State by linking together community-based regional health information organizations (RHIOs) that adhere to common standards and policies. RHIOs' roles included convening and governing community stakeholders, promoting collaboration and data sharing, and implementing technology for eHIE. As of 2012, 12 non-profit RHIOs provided eHIE services across New York State in compliance with state requirements using a variety of commercial products. Notably, 54% of the grantees targeted long-term care providers (though the article does not specify the types of providers falling into that category) and 24% targeted home care providers.33
The initiatives studied in our case study site visit to Minnesota were the recipient of state grants to implement eHIE with LTPAC providers. The Fairview-Ebenezer initiative was the recipient of state funds to enable eHIE with LTPAC providers. For example, they received PIPP, a two-year grant for approximately $385,000 that will end September 2016. Ebenezer is using PIPP dollars to further exchange using secure health care messaging applications such as Tiger Texting, advancing their CCD exchange with non-business affiliates and expanding exchange with state and commercial labs. The state was also a recipient of a Testing Experience and Functional Tools (TEFT) grant by CMS (about $500k) in March 2014. TEFT funded a demonstration for organizations to bring personal health records to deliver LTSS data to beneficiaries and their caregivers. One respondent noted that this state funding solicitation built on learnings from past projects such as SIM, the Fairview-Ebenezer PIPP project, and other efforts to integrate and improve care.
Benedictine was awarded $375,000 from the State of Minnesota to develop MatrixCare software such that it can exchange CCDs with Allina's Epic system peer-to-peer to support transitions of care between the Allina hospital and the Benedictine NF. The Benedictine-Allina project is primarily funded through the state grant and provider investment.
Subscription Fees
As demonstrated in the regional structure (middle row) level of the Conceptual Framework, a complement to federal funding sources, many of the initiatives studied charge a subscription fee to participants. For example, the Colorado Regional Health Information Organization (CORHIO) was an ONC Grantee (through the State Health Information Exchange Cooperative Agreement and the Challenge Grant). However, CORHIO transitioned to a $25 per user per organization subscription fees in 2014 to fund itself as ONC cooperative agreement and grant resources wound down.34 These subscription fees were not waived for LTPAC providers.
The Indiana Health Information Exchange (IHIE), a private HIE, has a subscription fee financial model as well. However, federal resources related to eHIE and policies (e.g., Stage 2 MU of the Medicaid/Medicare EHR Incentive Program) played an early role in the development of infrastructure that is now being sustained through subscription/user fees. As of December 2014, there were approximately four Kindred long-term care facilities working with IHIE, with plans to bring more on. Kindred is a national chain with 2,730 locations in 47 states.35 IHIE was initially affiliated with Regenstrief Institute, but has been an independent entity for more than two years.
KeyHIE now charges participating providers a subscription fee, priced by provider type and size, for ongoing use. This has been critical to the sustainability of the HIE since many of the federal grants that were leveraged to stand up eHIE (described above) have expired. Startup costs vary depending on the technology solution; an EHR connection can be quite expensive, particularly for larger facilities, while Transform is a much lower cost option.
The initiatives studied in Minnesota are not driven by a Health Data Intermediary or HIO, which would typically serve as a data aggregator and charge ongoing fees for connecting and querying for health information. As a result, participating facilities are not charged subscription fees. Allina, the hospital system working with Benedictine, is becoming an HIO but it envisions eHIE serving the development of their ACO and does not have plans to charge subscriptions. Providers will have to pay their vendors to develop the integration in order to connect to the HIE product. Reportedly those costs range from $2,000-30,000 per entity, which can be substantial for certain entities.
Apart from efforts to facilitate robust bidirectional eHIE, facilities involved in all of the initiatives studied reportedly have access to hospital portals to view patient information at partner organizations. These are highly affordable solutions, costing facilities only about $75/year.
Health Information Technology for Economic and Clinical Health Programs
In 2009, Congress passed the ARRA, which contained provisions collectively known as "HITECH"36 (shown in the Environment or Context level of the Conceptual Framework). The purpose of ARRA HITECH was to accelerate the digitization of the American health care system through greater adoption and the MU of EHRs and eHIE. The Medicare and Medicaid EHR incentive programs are the main mechanism through which providers, specifically eligible hospitals and eligible professionals, can access the financial resources to support the purchase or upgrade their EHRs. Additionally, through the successive stages of MU (Stages 1, 2, and 3, and for Medicaid providers only, a preliminary stage called Adopt, Implement, and Upgrade), the Medicare and Medicaid EHR incentive programs make available incentive payments to eligible providers who use certified EHR technology in the ways intended to improve the quality and efficiency of care.
Of particular importance to this project, LTPAC providers were not defined as eligible hospitals or eligible professionals under HITECH, so they were ineligible for the Medicare and Medicaid EHR Incentive programs or technical assistance through the Regional Extension Center (REC) program. Despite their ineligibility, the literature shows that the LTPAC provider community has worked to shape EHR Incentive Program MU criteria at the federal level. For example, per an August 1, 2012, letter from the President of American Physical Therapy Association to ONC regarding 2015-2017 modifications restructures Stages 1 and 2 MU requirements for the Medicaid/Medicare EHR Incentive Programs related to eHIE and transitions of care with LTPAC providers: "It is important that input from [LTPAC] providers is considered in the evolution of MU requirements so that patient data are accurate, accessible and transferred with the highest degree of security protocols in place to protect patient privacy."
The Federal Government has also supported policies that facilitate EHR adoption in LTPAC facilities. For example, ONC's 2014 "Health Information Technology: Standards, Implementation Specifications, and Certification Criteria for Electronic Health Record Technology, Final Rule" encourages EHR technology developers to certify EHR Modules to the transitions of care certification criteria (§170.314(b)(1) and (2)) as well as any other certification criteria that may make it more effective and efficient for eligible professionals, eligible hospitals, and critical access hospitals to electronically exchange health information with health care providers in other health care settings.37
And many of LTPAC providers' key exchange partners (e.g., hospitals, medical groups) were defined as eligible hospitals and eligible professionals and the MU requirements for the Medicaid/Medicare EHR Incentive Programs (along with other health care reforms) are beginning to give more incentive for these eligible hospitals and eligible professionals to engage in eHIE with LTPAC providers. Findings from the literature review38 and stakeholder discussions indicate that Stage 2 MU provided some incentives for eligible hospitals and eligible professionals to begin engaging in eHIE with LTPAC providers. This perspective is consistent with findings from the project's two case studies, with respondents in Minnesota also mentioning Stage 3 MU requirements as a motivating factor for hospital, organized delivery system, and medical group engagement in eHIE with LTPAC providers.
However, conversations with stakeholders across the United States indicate that competition for HIT resources within acute care provider organizations continues to be a challenge. For example, in the Missouri Quality Initiative there was an indication that organization delivery systems and hospitals were hesitant to allocate the resources needed to make DSM operational, and there was a general surprise in the technical complexity of what was required to make DSM operational. Acute care providers also continue to report staffing and information technology budget cutbacks due to financial pressures and multiple competing demands and projects. Although some HIEs indicated that the Medicaid/ Medicare EHR Incentive Program Stage 2 MU requirement for data exchange with non-affiliates was the lever used to get some acute and primary care providers as well as specialists to begin to exchange data with LTPAC providers, During this stage of the program, attestation was the priority. As a result, efforts to facilitate eHIE with LTPAC providers were often sidelined. While not specifically cited in the Pennsylvania case study, this finding is consistent with the Minnesota case study. Several respondents in Minnesota noted that provider efforts to meet MU requirements for the EHR Incentive Programs can sometimes have the opposite effect on eHIE involving LTPAC providers; in some instances, provider efforts to meet these requirements more generally have left fewer resources for developing interoperability with LTPAC providers, resulting in delays in investments in this area.
Privacy and Security Laws and Regulations
Privacy and security policies and requirements (shown in the Environment or Context level of the Conceptual Framework) are critical but can pose barriers to HIE with LTPAC providers and their exchange partners. Although all providers must meet Health Insurance Portability and Accountability Act (HIPAA) and other federal privacy and security requirements, states can pass additional requirements related to privacy and security and penalties for data breaches. One important way in which state privacy and security policy varies is whether patients or their legal guardians must opt-in or opt-out of HIE (i.e., actively give consent for all or some parts of their data to be exchanged).
Opt-in policies have been found to increase the cost of HIE participation for providers and therefore decrease participation in HIE efforts, while opt-out policies decrease costs and increase provider participation. In Maine, which adopted an opt-out policy for patient consent for general medical data sharing, the eHIE includes the records of over 88% of the population. Only 1.1% of the state's population has opted out of participating in the eHIE. This is not to say that opt-in policies create an insurmountable barrier to eHIE for providers but additional thought about workflow redesign is required. For example, Massachusetts has an opt-in policy but providers reportedly have integrated the consent process into their workflows so that consent can be obtained efficiently.
This experience is consistent with findings from the KeyHIE case study. KeyHIE currently has a more restrictive approach to security than Pennsylvania requires. KeyHIE employs an opt-in privacy model, which requires providers to actively seek consent from patients in order to exchange their health information, and limits access to patient information to organizations that consent to follow KeyHIE's RHIO agreement.39 Some respondents suggested that in order to encourage greater eHIE, KeyHIE will synchronize with state laws and providers will soon be able to elect to implement the less restrictive opt-out policy. Granting this option may improve a providers' ability to actively exchange their patients' data. For example, one respondent commented that once Pennsylvania became an opt-out state in 2012, "it made things easier."
A related issue is whether and how much state privacy and security law varies from federal policies. If states do not harmonize their policies with federal law, providers must understand how the two differ and follow the more stringent policy. For this reason, Wisconsin is planning to harmonize state law with HIPAA so that no additional consent is required and patient health information is automatically included without an option for patients to opt-out. Findings from the Minnesota case study indicate that within the state there are diverse opinions on what state privacy laws and regulations require and prohibit. Interpretation of the state's HIE statute (Minn. Stat. §62J.498 sub. 1(f)),40 which defines requirements around privacy and security, varies by provider organization. Some organizations are more conservative than others. For example, some organizations could interpret the HIE law as meaning that patient consent needs to be obtained annually while others could require patient permission for each data sharing with each provider. One organized delivery system is working on moving from an opt-out to an opt-in model but has run into some "political" challenges from organization leadership in making that shift.
The Improving Medicare Post-Acute Care Transformation Act of 2014
One policy area that has the potential to impact future LTPAC provider involvement in eHIE (and eHIE activities more generally) but does not appear to be on the radar of most of the stakeholders interviewed yet is the IMPACT Act (shown in the Environment or Context level of the Conceptual Framework). The IMPACT Act requires that CMS standardize post-acute care patient assessment data, including data with regard to specified patient assessment instrument categories and quality measures. In addition, the IMPACT Act intends for data comparability to allow for cross-setting quality comparison in settings including skilled nursing facilities (SNFs), HHAs, IRFs, and LTCHs, and, importantly, it conveys the inclusion of patient-centeredness in its references and requirements related to capturing patient preferences and goals.41 The IMPACT Act also requires that standardized post-acute care assessment data elements be made interoperable so as to support the exchange of such data among post-acute care and other providers in order to support access to longitudinal information and coordinated care. The provisions in the IMPACT Act will drive data standardization in post-acute care settings and will support the use of interoperable HIT systems within the LTPAC and interoperable HIE with and by this sector.
Case study respondents in every category were asked how the passage of the IMPACT Act has affected eHIE in their region. A minority of respondents recognized the name of the law, and a few respondents could briefly describe the law and its implications for LTPAC providers and eHIE. Those respondents who were aware of the Act were very positive about its potential impact.
Medicare and Medicaid Programs: Reform of Requirements for Long-Term Care Facilities; Proposed Rule (CMS-3260-P)
On July 16, 2015, CMS announced a proposed rule that would update long-term care facility requirements for participation in Medicare and Medicaid (shown in the Environment or Context level of the Conceptual Framework). The proposed rule includes best practices for resident care, implements safeguards previously identified by stakeholders, and includes additional protections required by the Affordable Care Act (ACA). Changes include improvements to care planning (e.g., discharge planning with an interdisciplinary team, taking into account the caregiver's capacity, providing follow-up information to residents, and ensuring that instructions are transmitted to receiving facilities).42 Of interest for this study is that the proposed rule would require long-term care facilities to send patient care summaries in the event of a transfer. While the proposed rule does not require the summary to be in digital form, the rule "encourage[s] facilities to explore how the use of certified health IT can support their efforts to electronically develop and share standardized discharge summaries...".
The proposed rule's 60-day comment period, which should have ended on September 14, 2015, was extended for an additional 30 days, until October 14, 2015.43
Though the proposed rule was announced after the Urban Institute team conducted the project's review of literature, stakeholder discussions, and site visits, the rule's requirements around care planning could have implications for LTPAC involvement in eHIE (if and when the rule is issued as final). This remains an issue to watch going forward.
Payment and Delivery Reforms
As already noted, payment and delivery reforms have the potential to impact LTPAC involvement in eHIE (shown in the Environment or Context level of the Conceptual Framework). The Federal Government is pushing many of these reforms (e.g., CMMI's ACO Medicare Shared Savings Program, Medicare's hospital readmission policy) while others are led by local providers (e.g., Geisinger's bundled payments program) or state governments (e.g., Minnesota's bundled payments program, called "baskets of care"). Many of these payment and delivery reforms require providers to engage in care coordination and population management.
An important component of any effort to provide those types of services is access to patient health care data across the continuum of care, which includes primary, acute, post-acute, and long-term care. Access to this range of data enables providers to form a better, more holistic picture of their patients' care needs and the care delivered by a range of providers to meet that need. HIE between LTPAC providers and other providers is a promising if not critical tool for giving those providers access to information across the continuum of care.
Findings from both the review of literature and stakeholder discussion indicate that payment and delivery reforms in general provide financial incentives for hospital and organized delivery systems to engage in eHIE with LTPAC providers. These findings are generally consistent with those from the case studies but the Urban Institute team found important differences in the experiences of providers in the KeyHIE region and the Minneapolis region.
In the KeyHIE region, LTPAC provide reaction to these reforms in the context of KeyHIE differs by provider type--these reforms seem to be driving NF interest to join KeyHIE more so than HHAs. NFs and HHAs seem to differ in the extent to which these providers see ACOs, CMS' readmission penalties, and bundling as a motivating factor for greater involvement in KeyHIE. NFs seem more motivated by the potential future impact of these reforms on their organization and its relationship with local hospitals and organized delivery systems. Some NFs feel that these reforms are pushing hospitals and organized delivery systems to institute preferred provider networks and that their involvement in KeyHIE could position them to become the preferred providers of those local hospitals and organized delivery systems in the future. Geisinger's health plan, which would have a powerful role in setting provider networks, also seems to be providing an additional push for LTPAC providers to participate in KeyHIE. HHAs seem to be less motivated by the potential future impact of these reforms on their prospects on becoming a preferred provider for area hospitals and are more interested in the potential for KeyHIE to improve efficiency and the quality of care their patients receive.
As a result, HHAs are generally easier to recruit for participation in KeyHIE and are more likely to be in the initial phase of data exchange. The value proposition of participating in KeyHIE--the potential for efficiency gains and quality improvement--is clearer for HHAs compared to NFs. In general, HHAs were farther ahead than the NFs in KeyHIE implementation and in thinking about and experiencing the impact of their participation in KeyHIE on their workflow.
In the Minneapolis region, payment and delivery system reforms may affect acute provider interest in exchanging health data with LTPAC providers differently.
-
Medicare' hospital readmission penalty policy has fostered hospital and integrated delivery system interest in becoming connected to LTPAC providers. Since LTPAC providers take responsibility for many patients discharged from hospitals, ensuring smooth transitions and sufficient information exchange about a patient's care can help to limit unnecessary hospital readmissions and help hospitals and integrated delivery systems avoid incurring financial penalties from the Medicare's readmission policy.
-
ACOs are common in Minneapolis and in Minnesota in general. Many stakeholders expect that their proliferation will facilitate interoperability with LTPAC providers in the state. However, provider adoption of the ACO model of care seems so far to be a weak motivating force for [primary and acute care providers] engaging in eHIE with LTPAC providers.
-
Renewed interest in Minnesota's baskets of care program may actively shift the integrated delivery systems' focus away from achieving interoperability with LTPAC providers. One respondent from an integrated delivery system noted that as the policy conversation within that organization shifts from hospital readmission penalties to bundled payments, interoperability with LTPAC providers becomes less important. That respondent indicated that the bundled payments ultimately chosen would likely revolve around specialty services, where there is likely high variability in rates, not LTPAC services. To the extent that integrated delivery systems have to partner with specialty physicians outside of their network to offer those bundles, interoperability with specialty providers becomes a high priority, and LTPAC providers become less important
Size and Scale of Current eHIE Efforts in the United States
The exact numbers and types of providers participating in initiatives designed to promote eHIE involving LTPAC providers were sometimes difficult to discern in both the literature and stakeholder discussions. Some of these projects targeted SNFs, NHs, or home health specifically, but many aimed to include "LTPAC providers," which was defined broadly without further describing the exact setting of care. However, the information we were able to gather through our stakeholder discussions demonstrates that there is significant variation in the number and types of LTPAC and other providers (e.g., hospitals, medical groups, laboratories, pharmacies) participating in eHIE (shown in the Regional Structure level of the Conceptual Framework).
Through the stakeholder discussions, the Urban Institute team was able to ascertain estimates of participating hospital and LTPAC providers and gain a sense of the range of hospital and LTPAC participation and scale of the HIE effort. In some regions and states (Massachusetts, Minnesota, and Missouri), around 1% of hospitals and medical groups in the state are participating. In other regions and states at least 35 hospitals are participating in the HIE. For example, in Colorado, 95% of hospitals are participate in the HIE, and in Ohio 90% do. About 18% of hospitals in Maine participate in the HIE. KeyHIE falls roughly in the middle of these two tails of the distribution with about 7% hospitals.
Similarly, there is significant variation across states in the number of LTPAC providers participating in eHIE. Massachusetts and Minnesota have a relatively small number of participating LTPAC providers (i.e., ten LTPAC facilities). Colorado (N=120) and Ohio (N=175) are among the states with the largest number of participating LTPAC providers. Maryland, Maine, and Missouri, fall in between with 11-40 participating LTPAC providers. In Pennsylvania, reportedly about 30% of long-term care facilities are participating in KeyHIE. We were unable to discern an exact number in Indiana, but LTPAC provider involvement there is noteworthy because it consists of two of the largest national, for-profit chains, Golden Living and Kindred Healthcare, that have or are implementing an EHR (e.g., PointClickCare [PCC]).
LTPAC Providers' eHIE Capacity
The best available information in the literature suggests that LTPAC providers are lagging behind other key providers (e.g., 58% of hospitals now have a basic EHR) in the adoption and use of certified EHRs (shown in the Provider Organization level of the Conceptual Framework).44 See the "LTPAC Providers and EHR Adoption" section for further information on this topic.
Our stakeholder discussion informants, who were primarily from HIEs, reported that LTPAC providers in their region generally had low rates of EHR adoption and ability to engage in more robust eHIE. Some LTPAC providers may have EHRs but not have activated and started using HIE modules for various reasons (e.g., too expensive, no perceived ability to exchange with partners). Hospitals and physicians, themselves, are struggling with eHIE. According to a recent article, only four in ten hospitals reported they can electronically share data with other providers45 and only 14% share data with ambulatory care providers or hospitals outside their organizations.46 However, there appears to be considerable variation between different LTPAC provider types (e.g., NFs versus residential care facilities) and within LTPAC providers (e.g., different types of NFs) so comparisons are challenging.
The sites selected for more in-depth case studies were chosen in part because their markets for exchange between LTPAC providers (especially NFs and HHAs) and their exchange partners were considered relatively mature. Findings from the KeyHIE case study confirm that is more advanced than most regions of the country and has the potential to expend LTPAC provider involvement well beyond current levels, while the two initiatives included in the Minnesota case study were farther behind.
Market Consolidation and Competition
The Urban Institute team found the following patterns regarding market consolidation and competition in our stakeholder discussions and the literature (see Provider Organization Characteristics level of Conceptual Framework). With respect to acute care providers, large organized delivery systems (e.g., Cleveland Clinic, Kaiser) or hospitals often play a major role in initiating eHIE involving LTPAC providers, particularly skilled nursing facilities (SNFs) and HHAs, and related care coordination efforts. These arrangements can take the form of preferred provider contractual arrangements or be more informal, based admission, discharge, transfer patterns and referral arrangements. Much of the research reporting exchange between LTPAC and other providers is occurring for LTPAC providers with strong affiliations and close proximity to large hospitals or health systems.47
This finding is consistent with the KeyHIE case study and, with one exception, the Minnesota case study. KeyHIE was driven by the initial leadership provided by the region's dominant provider organization, Geisinger Health System, as one of the initial sponsoring organizations for KeyHIE. Geisinger serves approximately 3 million residents in the Northcentral, Southcentral, and Northeast regions of Pennsylvania and employs 23,500 staff, including about 1,200 physicians, 400 residents/fellows, and 4,600 registered nurses and licensed practical nurses.48 Recent Geisinger actions have pushed the region's provider community toward even greater consolidation. As one respondent put it, Geisinger is in an "acquisitions phase"; the system has made a number of small acquisitions in recent years, mostly hospitals and small systems, but more recently Geisinger has reportedly become interested in purchasing LTPAC providers. For example, SUN Home Health, which has several facilities operating in Pennsylvania, was recently acquired by Geisinger. Several respondents indicated that this shift was due to the emergence of ACOs, hospital readmission penalties and other payment policies.
Minnesota's provider landscape is mostly made up of large integrated delivery systems or multi-specialty group practices, with small independent providers serving rural parts of the state. The hospitals and physicians serving Minneapolis and the surrounding area are generally owned or affiliated with one of several system (e.g., Allina Health, Fairview Health Services) or multi-specialty group practices (e.g., Fairview Physicians Associates, which is independent but affiliated with Fairview Health Services). In the Minnesota case study, both eHIE initiatives involved LTPAC providers that were owned or closely linked to a nearby hospital system.
A key difference in the Minnesota experience relates to the organization that initiated eHIE between LTPAC providers and their exchange partners. The Fairview-Ebenezer initiative was driven by the organized delivery system itself, which is consistent the majority of eHIE initiative discussed with stakeholders and in the literature and the KeyHIE case study. However, HIE in the Benedictine-Allina initiative was pushed by the LTPAC side (Benedictine). BHS is a non-profit health system based in Minnesota. Though it is not a large national chain provider, it does have facilities in multiple states (Minnesota, North Dakota, Missouri, Wisconsin, South Dakota, and Illinois). Information obtained through the stakeholder discussions and the literature indicates that LTPAC providers rarely are the lead organization in eHIE initiatives or on the board of a regional HIE.
Many of the NFs and HHAs in Minnesota are owned and operated by senior service health systems and large integrated delivery systems, respectively, which may facilitate LTPAC provider leadership and involvement in eHIE initiatives. BHS, for example, provides complete long-term care services for aging adults, including independent housing, assisted living, skilled nursing and rehabilitation services. Fairview Health Services, a non-profit health care system includes hospitals, aligned physicians, and clinics as well as "senior adult services" which include NFs. These senior services fall under the Ebenezer arm of the organization and have been a part of Fairview Health Services since 1995. The major national chains (Brookdale, Sunrise and Golden Living) also have a presence in Minnesota and may be better positioned for exchange and inclusion in delivery system reform than smaller facilities.
Finally, the stakeholder discussions and literature point to a second potential pattern: groups of hospitals and hospital associations can also play a role in supporting eHIE with LTPAC providers in the state. Our stakeholder discussions suggest that this kind of collective action appears to depend on how competitive systems or hospitals are in a region and the extent to which they see eHIE with LTPAC providers as an area in which cooperation rather than competition is to their advantage. In other words, hospitals and hospital associations support eHIE with LTPAC providers when it can benefit them and their strategies.
The Urban Institute team found limited involvement from provider associations in the Minnesota case study and little to no involvement in the Pennsylvania case study. There are two active and influential associations for "older adult service" providers in Minnesota: LeadingAge and Care Providers. LeadingAge Minnesota is the largest association of organizations serving Minnesota seniors. Care Providers is a long-term care trade association representing NFs, assisted living, home care, and hospice, with over 800 members. These organizations supported and publicized state efforts in administering a survey to LTPAC providers which showed that 69% of NFs had an EHR in 2011. They were also instrumental in securing exemptions for post-acute care providers from the state's EHR mandate and will be contributing to the LTPAC Roadmap, a component of their SIM grant (mentioned above).49
Business Case for LTPAC Engagement in eHIE Initiatives
Several stakeholders reported during discussions with the Urban Institute team that it is sometimes difficult to get the interest of acute care providers in exchanging data with LTPAC providers (see Provider Organization Characteristic level of Conceptual Framework). The principal reasons identified are the acute care providers' current focus on their internal EHR system implementation and Medicare/Medicaid EHR Incentive Program Stage 2 MU attestation. It appears that the competition for HIT resources within acute care provider organizations continues to be a challenge. Acute care providers also continue to report staffing and information technology budget constraints due to financial pressures and multiple competing demands and projects. Although some HIOs indicated that the Stage 2 MU requirement for data exchange with non-affiliates was the lever used to get some acute and primary care providers as well as specialists to begin to exchange data with LTPAC providers, attestation was the priority and competed with demand for eHIE with LTPAC providers.
Findings from the literature review indicate that some professional association activity supports this notion that sometimes it is difficult for LTPAC providers to engage acute care providers. For example, in the recent Health Information and Management Systems Society (HIMSS) LTPAC Task Force meeting (December 10, 2014) there was a consistent view voiced by LTPAC providers (national chains) that they are having a difficult time "getting the attention" of acute care providers.
Even in initiatives like the ones included in this project's case studies, where acute care providers were willing to include or participate in eHIE initiatives involving LTPAC providers, some reluctance from the acute care side remains due workflow issues described below.
The literature and stakeholder discussions included little information about factors that contribute to an LTPAC provider's decision to engage in eHIE, but findings from the two case studies shed some light on this topic. Generally, LTPAC providers who recognize the potential for eHIE to improve quality, increase efficiency, or secure referral sources from local hospitals tend to be more interested in engaging in eHIE.
Several LTPAC providers in Pennsylvania recognize that having an interoperable EHR may lead to strategic partnerships with acute care trading partners, especially HHAs. Many commented that having an interoperable EHR and access to KeyHIE could be used as a "public relations" tool to communicate to acute care providers that, "we'll make your referral process easier." Respondents in Minnesota also recognized the strategic value of possessing interoperable EHRs. One respondent noted that referral sources will likely eventually depend on whether a provider has an interoperable EHR. Though not specifically articulated by the respondent, this would likely apply to LTPAC providers in addition to other types of providers. In fact, one prominent EHR vendor said that NFs are beginning to understand the value they can bring to acute care providers by implementing eHIE. The respondent said this is the "main conversation we engage with [NFs] on".
In addition, improved outcomes, efficiency, and quality of care were a major motivation for both the Benedictine-Allina and Fairview-Ebenezer initiatives. Fairview includes LTPAC providers in their system but even within that system they want a better exchange strategy. The driver is improving patient care and transitions of care. Fairview believes that if they improve process, they can improve outcomes. Moreover, Fairview recognized the impending staff shortages, especially in the LTPAC arena. They believed the technology would allow Fairview to continue to operate efficiently in spite of shortages. Though Fairview did not provide examples of efficiency gains, a respondent in Pennsylvania indicated that technology can reduce time spent on intake processes.
The Benedictine-Allina initiative had two primary drivers. First, information technology staff at Benedictine examined office efficiencies and found that systematic documentation of services provided, which determines payment, was poor. Benedictine staff believe that the use of technology will enable more complete service delivery documentation. Second, Benedictine's leadership recognized the move in health care towards quality, which is enabled by interoperable technology. Some respondents also felt the CCD process would save them time on admissions--even if only demographic information is re-used to populate various documents. One respondent said that amount of paperwork NFs have to do has grown exponentially as a result of new regulations, which requires 4-5 FTE in admissions to complete. If this process saves 15 minutes just by prepopulating the admissions form, it could result in real savings. This was echoed by a respondent from Fairview Health Services who, though lacking hard evidence, expects that being technologically progressive will result in FTE savings.
In contrast, in the Pennsylvania case study LTPAC providers did not consistently believe that their participation in KeyHIE would lead to quality and efficiency improvements though they generally believed that their participation could potentially preserve referral streams from local hospitals in the future. Moreover, the perceived value of eHIE seemed to differ by provider types. Respondents from KeyHIE indicated that HHAs are generally easier to recruit for participation in KeyHIE and are more likely to be in the initial phase of data exchange. Many of the individuals with whom we spoke believe the value proposition of participating in KeyHIE--the potential for efficiency gains and quality improvement--is clearer for HHAs compared to NFs. Many respondents from HHAs agreed. One indicated that "HH is a no brainer...(exchange) allows the HHA a much better picture of what's going on with the patient's care in real-time. The discussion with home health, it only takes a minute.". Efficiency and quality gains seem more obvious for HHAs compared to NFs partially due to differences in referral patterns and the physical proximity to patients (see the section below on workflow for details).
HHAs and NFs have very different workflow patterns that have important implications for incorporating eHIE into their organizations. Differing referral patterns and physical proximity to patients yield different eHIE needs. For example, HHAs receive patient referrals from a variety of settings, including hospitals, NFs, primary care practices, and specialty practices; NFs on the other hand receive referrals primarily from a few local hospitals. Without eHIE, HHA staff spends considerable time reaching out to these different referral sources and tracking down the information needed to serve their patients.
Another workflow issue that affects LTPAC involvement in eHIE is the proximity of HHA and NF patients to the facility and clinicians providing their care. HHA patients are located in their home while NF patients reside in the facility. As a result, staff at HHAs are not always aware of a change in patient health status or the doctor's orders. One problem was frequently described in both case study sites visits: if a home health patient visits an ER or is admitted to the hospital, the HHA will not know unless the patient or a family member calls the HHA. When the home health nurse arrives at the patient's home and no one answers the door, the nurse will have to spend time trying to figure out if the patient is in the home and in need of assistance or at a hospital. NFs on the other hand typically have their patients' onsite and are aware of a change in patient status when it occurs. In one of the case study sites (Pennsylvania), these workflow patterns resulted in HHAs that were more motivated to exchange information than NFs.
Long-Term and Post-Acute Care Provider Preparation Activities
Technological
Historically staff at LTPAC facilities has used a variety of mechanisms, including telephone calls and faxes, to obtain critical patient information. Using eHIE to gather information, in contrast, may require use of new technologies such as desktop computers, EHRs, and portable devices such as tablets or notebook computers, to capture data during the patient encounter as well as support exchange (e.g., data transport mechanisms and tools in use by partners). Moreover, new data transport methods and formats such as DSM and the Transform tool developed by KeyHIE which require technological infrastructure, have been introduced in LTPAC facilities.
The literature review and stakeholder discussions described how much of the preparation for the new technologies (e.g., transport methods, formats) were centered on the regional HIEs; historically LTPAC providers were uninvolved in developing the national vision for eHIE. However, LTPAC providers have been involved in national collaborative groups such as the LTPAC Health Information Technology Collaborative, which develops and defines LTPAC providers' vision for HIT and the ONC-convened LTPAC Roundtable, which expands the national vision for HIT to include LTPAC providers.50 For example, experts who participated in the ONC LTPAC Roundtable suggested that strategies to collect and exchange data need to consider the needs of both senders of receivers.
In both case study sites, initiative leaders played a big role in determining the technological changes necessary for eHIE. In Pennsylvania, KeyHIE performs an analysis of LTPAC facilities ahead of installation of new technologies to determine which of its tools would be the "best fit" for the facility based on EHR capabilities. In Minnesota, information technology staff from Benedictine was instrumental in working with vendors to develop the technology to enable exchange of the CCD (see Provider Organization Characteristics level of Conceptual Framework).
Human Workflow
Implementing the technological changes to enable eHIE by LTPAC facilities with other providers creates a disruption in workflow for staff at all levels in the LTPAC facility, from providers to front office staff (see Provider Organization Characteristics level of Conceptual Framework). The literature revealed that a number of factors create challenges for introducing new technology in LTPAC facilities. There are high staff turnover rates in LTPAC facilities,51 and nursing staff working in LTPAC facilities may be relatively older and have less education and training compared to nurses in other settings. As a result, they likely have less experience with computer systems generally and HIT specifically.52 Additionally, there are large number of nurses at SNFs that work part time. All of these staffing issues pose challenges for conducting EHR or other HIT education and training sessions.53
Our stakeholder discussions suggested that there were limited resources dedicated to staff education and training. However, in both of our case study sites LTPAC staff were provided significant support from within and without the LTPAC facilities.
Staff Education and Training
All of the data sources we explored in this research highlighted the need for staff education and training at LTPAC facilities. Findings from the literature, stakeholder discussions, and case studies indicate that staff at LTPAC facilities tended to be older and less technologically adept and therefore in need of more extensive education and training compared to staff at hospitals and other providers (see Provider Organization Characteristics level of Conceptual Framework). Discussions with key stakeholders revealed that despite the high need for HIT training, LTPAC providers have limited options to provide EHR and HIE education for their staff. Generally, federally supported technical assistance programs that could potentially assist LTPAC providers, such as the ONC RECs and HIT work force training programs have ended,54 and few vendors provide this training free of charge or at a price point that many LTPAC providers can afford.
However, some of the initiatives to promote exchange in LTPAC facilities that we examined have provided staff education and training, including CORHIO and those studied during our site visits. Respondents from both site visits were reportedly provided extensive training through either their HIE Organization (e.g., KeyHIE) or by the LTPAC facilities themselves (e.g., Ebenezer and Benedictine), which enabled ease of use.
In Pennsylvania, the burden of training LTPAC facility staff largely fell on KeyHIE. Because of the intensive training and follow-on technical assistance provided by KeyHIE, few providers who were using KeyHIE to exchange data reported workflow issues in using KeyHIE to exchange data. KeyHIE staff reportedly provides two full-day sessions of training to users and were highly responsive to any phone inquiries in the event of issues after the technology was in place. Training from KeyHIE is included in the ongoing subscription fee.
In Minnesota, the LTPAC facilities provided training to their own staff. At St. Gertrude's, one of the younger staff members indicated that learning to use MatrixCare to exchange CCDs took "five minutes of training". However, as indicated in the literature and stakeholder discussions, the transition to electronic operations has been more challenging for older staff, who still prefer working with paper. Fairview also manages staff education and training in-house for both HHAs and NFs. Upon hire, every new Fairview Health Services employee must complete a two-day HIT course. This suggests that large integrated delivery systems that own LTPAC facilities may be able to leverage existing HIT staff and training capability that may have been developed with EHR Incentive payments to extend training to their affiliated LTPAC entities. These incentive payments are not available to LTPAC providers.
Findings: Implementing Ehie Between Ltpac Providers and Exchange Partners
This section seeks to answer the following research questions:
-
What types of health information do the LTPAC providers and their trading partners need to support continuity and coordination of care; and how were these information needs identified? What types of information do the LTPAC providers and their trading partners create and transmit? How has the type and timing of information exchange changed since implementing eHIE?
-
What eHIE methods (i.e., what technology solutions) are used to transmit information to/from the LTPAC provider and their HIE trading partners? Does the method of exchange enable the interoperable exchange and re-use of needed clinical information? What are the costs of the technology solutions?
-
What do the LTPAC providers and their trading partners describe as being the advantages and disadvantages of engaging in eHIE with LTPAC providers?
Types of Information Required to Support Continuity of Care
Some of the types of information LTPAC providers and their trading partners require to support the continuity of care and general care coordination are encompassed under the 2014 Edition of EHR Certification Criteria and Stage 2 MU Objectives. However, the investments have not generally been made by LTPAC providers or HIE organizations to support the infrastructure required to support cost-effective and bidirectional exchange and re-use of information with and by LTPAC providers. Instead, at this point in time, hybrid or partial solutions with limited functionality are being implemented which are perceived as "good enough" substitutes for interoperable exchange.
The National Learning Consortium as developed by the Health Information Technology Research Center identified some of the specific types of information required to support care coordination between LTPAC providers and their trading partners.55 The interviews and site visits conducted under this project have found results consistent with this report. Specific elements of importance that were identified include: current medication list, allergy list, current problem list, and a discharge summary. These are well-established components of consolidated-clinical data architecture (C-CDA) requirements.
The issue becomes exchanging and re-using these data within evolving hybrid or limited exchange systems. LTPAC providers are not using MU-certified technologies and are opting for lower cost, feasible solutions in the short term such as view-only portals and the printing and scanning of exchanged CCDs into patient records (see Provider Organization Characteristics level of Conceptual Framework). These lower cost solutions often do not support the interoperable exchange and re-use of information. The interviews also suggest that a further barrier to adoption of EHRs and/or eHIE is providing solutions that provide perceived and actual benefits that justify their use over well-established faxed-based workflows within LTPAC organizations. The types of information required to support the continuity of care on behalf of LTPAC patients by LTPAC providers and their partners are known and available, but typically they are not exchanged in a functional manner that supports electronic re-use.
Electronic Health Record Penetration in Long-Term and Post-Acute Care Facilities
Interviews indicated that adoption of data exchange by LTPAC providers is inconsistent, even within an HIE service region. For example, in the interviews, some LTPAC and HIE respondents indicated that Medicare/Medicaid EHR Incentive Program Stage 2 MU requirements resulted in hospitals reaching out to NHs in order to meet non-affiliate exchange requirements. Others stated that their trading partners indicated that they were too busy meeting EHR Incentive Program MU requirements to deal with exchanging data with LTPAC facilities. Overall, the result has been an isolation of LTPAC providers away from larger evolving interoperable and integrated system of exchange. One result of this isolation is a narrowing of EHR vendors targeting the LTPAC market. Respondents indicated that many larger vendors of certified EHRs indicated a disinterest in the LTPAC market segment because the vendors were resources constrained by meeting MU certification requirements for existing customers and/or viewed LTPAC providers as inferior customers due to the lack of incentive dollars.
There appears a pronounced difference in the definition and functionality of EHRs between LPTACs and their partners. This has created confusion in understanding the capacity and characteristics of exchange. Studies and industry surveys have indicated that LTPAC providers have EHR adoption rates that are close to those of Medicare/Medicaid EHR Incentive Program-eligible providers. For example a March 2015, study by LeadingAge of LTPAC providers in the state of New York found 73% of NHs and 68% of health home agencies have partially or fully implemented an EHR.56 The authors identified a likely bias in respondents with a low response rate by non-adopters. More importantly, as occurred in earlier survey-based studies, respondents may be including electronic information systems used for recording patient demographics and reporting administrative and some quality data for regulatory compliance in their self-reporting of EHR adoption within the survey.
The difference in the definition of what capabilities and characteristics constitute an EHR has led to an ability to effectively compare adoption and use rates between LTPAC providers and their trading partners. The EHRs adopted by LTPAC providers have limited technological functionality when compared to the capabilities of the EHRs of their partners. While a few LTPAC facilities owned or closely associated with large IDSNs may have an MU-certified EHR, the vast majority of LTPAC providers do not have certified EHRs. Within the LTPAC market segment, the market share for EHR vendors has some regional characteristics and a degree of fragmentation, but national leaders are emerging. For NHs and SNFs, PCC is the largest provider on a national basis. For example in 2011, PCC had a 43% market share in Minnesota.57 The 2015 LeadingAge study found that PCC had an 18% market share in New York.58 As the leading EHR in-use in the LTPAC segment, PCC only added DSM in mid-2015. Within the PCC EHR, functionality is read-only and scan (the EHR does not consume or parse the data into the EHR). Other national NH and SNF vendors have indicated that they are moving towards including DSM capability in their EHR. This means that DSM is positioned to evolve as the principal bidirectional transport mechanism between NHs and SNFs and their trading partners using MU-certified EHRs.
Health Home versus Long-Term Care
HHAs have a different group of EHR vendors than NH and SNF providers. Based upon the site visits and interviews, HHAs appear more likely to be using an HHA HIT or EHR module from a certified EHR vendor than a NH or SNF using a certified EHR. This is likely due to either the HHA being owned by a hospital system or having a close hospital system affiliation. Non-certified EHRs for HHAs have similar constraints on interoperability as non-certified EHRs in the NH and SNF market segment relative to electronic data re-use, but interviews indicated an easier integration of the data. This is partially due to the nature of the services provided and the characteristics of the workflow. For example, visiting nurses will input data and notes onsite during the patient encounter. Based upon the site visits in Minnesota and Pennsylvania, there appeared near universal adoption of mobile technologies such as tablets or portable computers during patient encounters and the use of cellular systems to transmit that information to centralized systems. This supports the bidirectional exchange with both certified and non-certified EHR systems and potentially eHIE from remote locations.
Methods of Exchange
Based on our discussions with stakeholders from selected regional and state eHIEs, there currently are four potential methods and two potentially innovative solutions to data exchange for LTPAC providers and their trading partners. These are summarized in Table 1. Appendix B provides a further description of the technologies and their implications for LTPAC providers.
| TABLE 1. Exchange Alternatives for LTPAC Providers | ||
|---|---|---|
| Technology | LTPAC Provider Benefit | LTPAC Provider Issues |
| Provider Portal |
|
|
| eHIE Portal |
|
|
| DSM |
|
|
| Query-Based Exchange |
|
|
| Transform* |
|
|
| LAND/SEE* |
|
|
| FHIR |
|
|
| *Discussed in "Innovative Solutions" section. | ||
The alternative exchange solutions available to LTPAC providers have been shaped by the characteristics of competition between health care systems, technology functionality, costs, and workflow. In many regions Epic Systems Corp. is the dominant EHR vendor and providers look to the EpicCare Everywhere solution as the exchange transport solution as opposed to a public HIE. In addition, owing to competitive factors, many providers do not publish their data to public HIEs but rely instead upon their internal or private HIEs for exchange.
Aside from private vendor and HIE network considerations, there is evidence that portals are the preferred method of exchange. In Central Pennsylvania, even with a relatively mature HIE organization and high participation rates (94%) of hospitals in the region, 82% of the 122,000 patient records accessed during April 2015, was through the portal. Also, DSM does not appear to be a popular solution. While KeyHIE does not support DSM, Geisinger offers the service and indicated that for the month of March 2015; only 54 direct messages were sent to LTPAC providers. The apparent explanation is that the portal solution that Geisinger offers, EpicCare Link, contains the same information and is easier to use than DSM.
Based upon the site visits, the experience in Minnesota parallels that of Pennsylvania. The principal means of data access is through provider portals. There is very limited exchange through public eHIEs, and the current focus is to develop community exchange solutions primarily using DSM At this time, there are no technological alternatives available within the state except private HIEs and portal solutions, and planners anticipate being proactive in addressing the constraints of DSM. The the leading LTPAC EHR vendors, have either recently included or are in the process of introducing DSM within their EHR products.
For bidirectional exchange, national LTPAC chains are supporting DSM. They cite the number of markets they are in and the cost of developing individual interfaces with each HIE as being prohibitive. They are relying upon national LTPAC vendors and their Healthcare Information Services Providers (HISPs) to support DSM with the acute care EHR vendors and their respective HISPs.
In sum, there is little evidence of bidirectional information exchange and re-use among LTPAC providers. While the industry sites a high penetration of EHRs, their functionality is often limited to administrative data capture and reporting for regulatory compliance purposes and they are not certified as part of the MU of certified EHRs. View-only portals (principally from providers) are the dominant means of exchange and scanned PDF files are the principal means of data input. In the near term, our stakeholder interview and site visit results suggest that DSM is the technology that LTPAC providers plan to use for bidirectional exchange. In order to support future use of DSM for exchange, workflow issues (described below) created by the need to log out of one's email server and into Direct to receive messages will need to be addressed.
Innovative Solutions
There are alternative solutions and pathways that support LTPAC HIE. For example the KeyHIE Transform tool is based upon using the CMS MDS and OASIS data sets and converting them into a standards-based consumable CCD format which can be exchanged via DSM. Developed under federal grants, Transform has been commercialized and implemented by 27 companies encompassing 41 care locations as of September 30, 2015. There will be more than 100 care locations using Transform based upon planned funding from ONC Advanced Interoperability awards.59
A similar tool, Local Adopter for Network Distribution (LAND)/SEE is under development by researchers in Massachusetts. LAND/SEE refers to the system architecture designed to support the IMPACT (Improving Massachusetts Post-Acute Care Transfer) initiative which is part of an ONC funded grant to improve care transitions. There are two solutions, LAND, which is designed for providers with an EHR, and Surrogate EHR Environment (SEE), which is designed for providers who do not have and EHR and are using DSM. The data sets supported are standards-based. LAND works by creating a text document that can be consumed by an EHR. The SEE solution is based upon software linked to a Direct mailbox which creates a CCD from received documents that can be viewed and copied. The copied document can have content added but not edited. This more complete record can then be converted back into a CCD and transmitted via DSM. The LAND/SEE project has been targeted to be implemented at a pilot site in Worchester.
The development of both private and public application protocol interface solutions, application program interface (API) solutions and standardized data formats such as Fast Healthcare Interoperability Resources (FHIR) have the potential to bring simplified and lower cost solutions to data exchange. FHIR is currently a Health Level Seven (HL-7) draft standard available for trial-use. FHIR is a health care information exchange standard that makes use of an HL7-defined set of "resources" to support information sharing by a variety of means, including documents, messages, applications and RESTful interfaces.60 Initiatives such as SMART on FHIR and DSM on FHIR have the promise of supporting the exchange of well-defined modular pieces of information as opposed to the complexity and technical challenges associated with the exchange of a full C-CDA document. This could resolve, at effective price points, some of the technical barriers to interoperability while providing the necessary information to support transitions in care.
Findings: Assessing the Impact of Ehie Between Ltpac Providers and Their Exchange Partners
This section seeks to answer the following research question:
-
How has the creation, transmission, and receipt of eHIE (including interoperable exchange) at times of transitions in care and during instances of shared care impacted the clinical workflow in the LTPAC settings and that of their clinical trading partners (i.e., physicians, hospitals, and pharmacies/pharmacists)?
Limited bidirectional exchange is occurring nationally and in the sites selected. As a result, several research questions around long-term impact of eHIE on patient outcomes and costs cannot be answered due to minimal interoperable exchange nationally. As described in "Implementing eHIE Between LTPAC Providers and Exchange Partners," most eHIE occurring via view-only portals; volume of this type of exchange is unknown.
Below we discuss the intermediate effect or impact to workflow on LTPAC facilities and their organizations that results from implementing eHIE as well as a comprehensive approach to assessing the quantitative impact of eHIE and the challenges to conducting a comprehensive quantitative evaluation on impact.
Workflow
As mentioned before, many of the methods LTPAC providers use today to exchange information with other providers (e.g., phone, paper, and fax) are labor intensive and inefficient. While shifting to eHIE may reduce the amount of time required to collect and share necessary information,61 efforts to switch from current work processes to eHIE can be quite difficult for both post-acute and acute care providers in practice.
The challenges of adopting EHRs and implementing HIE generally are well documented for acute and primary care providers. Previous research has documented workflow barriers resulting from EHRs that lack processes for easily documenting and retrieving patient status (opt-in/opt-out) and separate, multiple log-ins (external to internal EHR log-in) to access information housed in an HIE.62 In other words, in order to access information housed in an HIE, providers often have to exit their own EHR and log into a separate solution which stores the desired health information. There was little in the literature documenting how the shift to new technology impacted the workflow of LTPAC providers specifically. Only one report from a Stratis Health study made observations on the impact of technology use in both NFs and their hospital partner,63 but there is no reason to think that the barriers encountered by acute and primary care providers do not also apply to them as well and our stakeholder interviews and site visit findings are consistent with these earlier findings.
Impact to LTPAC Provider Workflow
Overall all of the data sources confirmed that hospital portals were the primary form of data exchange, which reportedly had limited impact on the LTPAC provider's workflow. For example, respondents in our stakeholder discussions described how the prominent use of hospital portals in LTPAC facilities for gathering patient information currently minimizes workflow issues for LTPAC providers. Many suggested that as eHIE becomes more prominent, workflow breakage will likely become a more significant issue and will likely require more work-redesign attention.
However, the literature review discussed impact of eHIE on providers more broadly, and frequently did not specify the impact to LTPAC providers. The HITPAC final report (referenced above) indicated that workflow issues for both trading partners delayed implementation and eventually resulted in the discontinuation of eHIE.64 There were a few reports from some LTPAC initiatives that demonstrated that workflow issues are a top priority to LTPAC providers. Reports from early initiatives have started to identify and address the workflow challenges and potential ways to overcome them. For example, some of the ONC Challenge Grantees have been working to develop innovative and scalable solutions to improve LTPAC transitions through new workflow and clinical processes that use eHIE.65 These grants are an extension of State HIE Cooperative Agreement Programs, which funded state efforts to rapidly build capacity for data exchange. The Challenge grants are intended to encourage breakthrough innovations for eHIE that can be leveraged widely to specifically support LTPAC providers nationwide in their effort to implement eHIE.66
The majority of our findings in the area of impact to LTPAC provider workflow came from our stakeholder interviews and case study site visits and is described below.
Home Health Agencies
HHAs at each case study site were at differing levels of eHIE implementation.
Pennsylvania
In Pennsylvania, HHAs are further along in their implementation of eHIE. Many of those we spoke with have already connected to KeyHIE and have begun using it to gather patient data ahead of home visits. In addition, HHAs in Pennsylvania reportedly found great utility in Admission Discharge Transfer (ADT) alerts (described in Appendix B) and additional clinical information concerning their patients. For example, ADTs provide HHAs immediate notice when their patients have been admitted to the ER. This can prevent unnecessary home visits to patients who are under medical care elsewhere.
One HHA nurse described the process of gathering clinical information as follows: most information is gathered from KeyHIE by the intake nurse at the time of the referral. When patient information is not available in KeyHIE, the intake nurse will consult Geisinger's hospital portal, which provides valuable information about the patient's most recent acute hospital episode but not longitudinal data. The primary nurse will then review this information ahead of the home visit. After the home visit, the primary nurse will also consult KeyHIE for a history of symptoms and conditions that presented during the visit to the patient's home. Though this approach may not be as efficient as accessing needed information from a single source, as described above, home health nurses typically spend considerable time with patients and find that using these multiple methods of gathering information more efficient than gathering information via telephone and fax.
A few of the HHAs we interviewed in Pennsylvania were using Transform. They reported that transmitting information to KeyHIE using the Transform tool was also seamless; inputted OASIS data is automatically converted into a CCD and transmitted to KeyHIE. However, HHAs did express concern that the information they push is sitting in the HIE and is not being used by their trading partners because they do not know the information is there.
HHAs in Pennsylvania did not typically use DSM to communicate with trading partners due to workflow issues for both acute care and post-acute care providers. For example, home health nurses lack a consistent internet connection and are unable to share Direct mailboxes, which raises concerns that urgent messages may be missed. Trading partner resistance to eHIE is further described below.
Alerts and clinical messages from KeyHIE also provide information and insight into a patient's status that the HHA would otherwise not know or miss. For example, when a patient cared for by a HHA is admitted to an ER an ADT alert can prevent an unnecessary visit to a patient's home. Prior to the use of ADTs, a home health nurse would make an unnecessary trip and spend additional resources ascertaining the patient's status and location. However, alerts do not go to nurses in the field, but rather to the intake desk, which then notifies primary nurses of any alerts.
Minnesota
Whereas in Pennsylvania most LTPAC HIE was occurring in HHAs, in Minnesota there was much less HIE occurring in HHAs. HHAs were not at all involved in the Benedictine initiative, and Fairview's HHAs currently do not engage in electronic exchange.
At Fairview most patient information transfers are handled via fax; the HHA keeps a paper chart in addition to the EHR. The workflow when sending patients to trading partners involves many phone calls. One respondent said, "Our nurses spend a lot of time on the phone trying to get ahold of a doctor."
As in Pennsylvania, Fairview HHAs are able to utilize the read-only access to hospital portals (in this case Epic) to supplement information received at transfer. Reportedly, this dual process causes duplication of effort for HHAs. One Fairview nurse described the process of securing complete patient information: "the physician puts an order into Epic; the physician's agent has to call the home care clinician, who then enters the information into the local EHR (McKesson). It goes to HIM (health information management), they print it off, send it back to the physician for signature, and then they have to log it back into the record." Though Epic and McKesson both have certified EHR products, the McKesson product that HHAs use is not MU-certified. As a result, the two systems are not interoperable and cannot exchange health information.
Skilled Nursing Facilities
Like HHAs, NFs in each case study site were at differing levels of eHIE implementation. Within the two Minnesota initiatives there were also distinct approaches to eHIE implementation.
Pennsylvania
The SNFs in our case study were from smaller regional chains. All were still in the testing stage and had not yet implemented KeyHIE or Transform. Few facilities had begun considering how they would incorporate KeyHIE into their workflow, but indicated they would be doing so in the coming months. Due to a number of factors, we were unable to secure an interview with the national chain in the area, which according to other interviewees, may have been farther along in their implementation of eHIE.
Staff at NFs has limited experience using DSM to communicate with local hospitals. Though KeyHIE has provided all of its participating LTPAC facilities with Direct mailboxes (which if used would enable bidirectional HIE), LTPAC providers forego DSM use in favor of the hospital portal, which provides a complete set of information from the hospitals, but does not allow the NF to send information to hospital.
NFs in Pennsylvania currently obtain most or all of the needed health care information from the referring hospital's provider portal. There were two NFs (Maria Joseph and Presbyterian) who were reportedly trained in Transform, but after changes in leadership and EHRs, respectively, they discontinued use. This finding also highlights the need for ongoing commitment and engagement as well as greater institutionalization, otherwise progress toward eHIE between partners can be stalled or reversed with leadership turnover.
Minnesota
The two initiatives studied in Minnesota took distinct approaches and were at different stages in their ability exchanging health information electronically. In the case of the Benedictine-Allina initiative, the two participating facilities have modified their EHRs such that CCD exchange is enabled. When a patient is discharged from Allina owned St. Francis Hospital to Benedictine's St. Gertrude's Health and Rehabilitation Center, the hospital first calls St. Gertrude's and provides a medical record number. At that point, the admission person can enter the NF's EHR (MatrixCare) and query for a CCD. If Benedictine's MatrixCare product determines that the patient matches a record at the participating hospital, the EHR will respond with the availability of documents. At that time a person can click on it and show a CCD, which can be attached to the record as a PDF.
Though the process itself is simple, there are a few issues that disrupt workflow. In order for McKesson to show a hospital patient's CCD, the hospital must have first secured and uploaded the patient's consent. Many interviewees said the hospitals find this process cumbersome, which means that despite being able to determine that a patient has been seen at both St. Gertrude's and St. Francis, often a patient's CCD is not made available in MatrixCare because patient consent has not been received. One nurse said "It's a 10:1 ratio of 'patient match not found' versus having a CCD."
Both of these issues are mitigated by accessing the Epic portal. For example, one NF nurse mused that when privacy concerns prevented transmission from the hospital of the CCD, the nurse just logs into the Epic portal. Information from the hospital portal is also used to supplement the information provided in the CCD to get a more complete picture of a patient's condition. In total, between the CCD and Epic portal, admissions nurses spend about 15 minutes collecting all of the information needed from a patient's record. This process was common in many of the LTPAC nurses we interviewed. St. Gertrude's gets over half of its patients from St. Francis Hospital Transfers, the only hospital with which it has a server to server connection. Transfers with hospitals other than Allina are still largely done by fax; Benedictine has reduced the amount of paper transfers as a result of their effort to connect with Allina, but still receives some paper transfers from other hospitals.
The NFs participating in the Fairview-Ebenezer initiative had not yet initiated exchange, but had participated in test cases of HIE as part of their Health Information Technology for Post-Acute Care (HITPAC) project, the goal of which was to observe workflow. Prior to receiving this grant, the NFs were reportedly sending patients who were transferred to the hospital with a 100 page hard document, which they learned the hospital was not reviewing because it was too cumbersome.
The project team determined that the Interventions to Reduce Acute Care Transfers (e-INTERACT) form provided the targeted information that hospitals said they needed for an incoming patient. This form was sent via DSM to hospitals as part of the pilot. However, shortly after the pilot was completed, the hospital discontinued participation in exchange because the workflow changes were deemed problematic. Because LTPAC facilities did not have interoperable EHRS, the HITPAC project used a separate product to exchange the e-INTERACT form. This product sends DSM notifications to hospital Outlook accounts to alert of messages in their DSM account; receivers then have to exit Outlook, and log into DSM to view the message. Because of the way it was set up at the time, it did not allow distribution lists, so a single person on the mailbox would receive the notifications.
Fairview and Ebenezer anticipate similar workflow barriers for the SIM Model Testing67 activities, and said that getting hospitals and the acute care hospitals' EHR vendors on board will be critical to success.
Impact and Evaluation
Past Evaluations of eHIE Initiatives
Overall, the peer-reviewed and other literature on the potential impacts and outcomes were on eHIE generally, not eHIE with LTPAC providers more specifically. Similarly, the majority of these HIE efforts targeted for stakeholder discussions had limited to no evaluation component, as required by grant funding or that could be conducted with relatively little resources. There was great interest in evaluation research--both formative and process oriented as well as summative or outcome oriented.
In the Pennsylvania case study, KeyHIE was the subject of an evaluation through two grants, both of which are now complete (see "Funding" section for details on those grants): Geisinger's Keystone Beacon award from ONC and their HIE grant from AHRQ. Abt's evaluation targeted all providers participating in KeyHIE, not just the LTPAC providers. Abt Associates was the lead evaluator for both grants, though Geisinger staff was involved with obtaining secondary data and coordinating qualitative data collection for case studies. The Abt evaluation team was Abt and Geisinger were unable to conduct an analysis of claims data as originally planned due to challenges described in more detail below (see section "Limitations to Conducting a Comprehensive Quantitative Evaluation on Impact") but were able to conduct the following analyses:
-
A Qualitative Case Study on HHAs. A paper describing the results of those case studies is forthcoming.
-
A Patient Survey Analysis. The results of the surveys indicated that patients are relatively comfortable with giving case managers access to their health data and allowing their physician to share their information with other physicians as needed but are less comfortable with hospitals making available their health information more broadly. The surveys also revealed patients' misconceptions about the extent to which their health information is available to ERs and hospitals and general concerns about identity theft.
-
An Analysis of ICD-9 Codes. The analysis concluded that the ICD-9 codes from the problem lists in KeyHIE cannot be used as a substitute for the final diagnosis seen on a patient's bill.
In addition to contracting with Abt Associates to conduct the evaluation activities described above, KeyHIE also recently committed to conducting a new study of KeyHIE as part of a new grant from HRSA bring 50 or more LTPAC providers onto KeyHIE and expand use of KeyHIE's three tools: KeyHIE Transform, MyKeyCare and DSM. As part of that grant, KeyHIE has agreed to measure 30-day hospital readmissions and all-cause ER visits (no projections on reductions).
In the Minnesota case study, the State Health Access Data Assistance Center (SHADAC) is the state evaluator for Minnesota's SIM grant. As part of its evaluation, SHADAC is charged with evaluating the SIM-funded development and implementation grants awarded through the e-Health Grants Program, including the Fairview-Ebenezer initiative's 12-month development grant. The goals of the SHADAC evaluation include documenting what is going on, what did not go as planned, and implementation barriers and facilitators. The evaluation will focus more on coordination and transitions, and less on issues like the type of technology use, the transport, and the ability to parse. The evaluation includes both quantitative and qualitative methods. Quantitative data sources that the SHADAC evaluation team plans to use for its evaluation of the e-Health grants include a state-fielded EHR survey and a continuum of accountability matrix, which is a self-report mostly made up of process measures (e,g., "Are you able to do exchange with X-type of providers?" and "Can you use exchange for X, Y, Z functions?"). Respondents rate themselves from a beginner to more advanced. On the qualitative side, SHADAC is conducting interviews with both development and implementation e-Health grantees (e.g., Fairview-Ebenezer, Otter Tail County Public Health, Winona Health, etc.).
Prior to the SIM evaluation, Stratis Health conducted an evaluation of the HITPAC project involving Fairview and Ebenezer. The Stratis evaluation included two surveys. The first survey was an assessment of participants as they completed exchange tests and, in some cases, as they went live with exchange; the purpose of this assessment was to understand participants' experience receiving exchange. As part of this assessment HITPAC participants developed five use case scenarios (realistic examples of typical scenarios during care transitions). The purpose of the second survey in the Stratis evaluation was to understand the extent to which participants found eHIE valuable. The Stratis evaluation identified three major barriers to widespread adoption of eHIE: (1) lack of understanding about the value of interoperability; (2) lag in adoption and optimization of EHRs among SNFs; and (3) the lack of technology solutions for exchanging in eHIE.
To date, an evaluation of the Benedictine-Allina initiative is not underway or planned.
Quantitative Evaluation Plan
Unfortunately, quantitative analysis of eHIE in LTPAC is fraught with problems because of the immature state of systems in even the more advanced areas, the fragmentation of systems and technology used across types of providers, and the very local character of exchange solutions. Much of the evaluation methodology for HIE that has been discussed in the literature is hypothetical and applicable only when more robust systems are in place for public exchange--for example, envisioning use of data from HIOs for public and disease monitoring purposes.68 In this section, we discuss major limitations to a comprehensive quantitative evaluation of eHIE based on project findings.
The Urban Institute team conducted case studies and site visits to learn about the following initiatives to enable eHIE with LTPAC providers: KeyHIE in the Northcentral/Northeast region of Pennsylvania, the Fairview Health Services/Ebenezer senior services initiative in Minneapolis, and the Allina Health/BHS initiate, also in Minneapolis. Previous memoranda summarized the eHIE in these markets, particularly as those activities pertain to the involvement of LTPAC providers.69 Specifically, these memoranda summarized key findings from the site visits, efforts to prepare for and implement HIE between LTPAC providers and their partners, and any relevant evaluations underway or completed in these markets. This section summarizes findings from these analyses relating to the feasibility of conducting the comprehensive quantitative evaluation described in the prior section.
A Path Forward for Evaluating eHIE Involving LTPAC Providers
In light of what we have learned about the reality of LTPAC providers and HIE, the following describes a feasible approach to address the research questions of interest, relying on the incentives and opportunities presented by IDSNs and ACOs, and the use of interoperable HIT tools among LTPAC providers (e.g., the Transform tool).
An overarching lesson was that having a relatively advanced HIE infrastructure is a necessary, but not sufficient condition for integrating exchange with LTPAC providers into the system. At a minimum, evaluating outcomes of exchange including LTPAC requires the ability to identify locations or organizations where LTPAC providers have been integrated into exchange beginning at some identifiable event defining an "intervention" period for a pre/post design. In practice, it is relatively simple to define the event, such as initiation of a program. However, given that implementation is a process that can take substantial time to complete, the intervention period during which change may reasonably be expected can be more difficult to clearly delineate. Thus, it may important consider stages of implementation, early operation, and maturity in evaluation design. In order to implement the stronger difference-in-difference design, the challenge is finding a credible comparison group not exposed to the intervention to examine over the same time periods.
The move toward ACOs under the ACA comes from the need to contain costs in Medicare, but interest and implementation of the model extends to Medicaid programs and predates the ACA. ACOs are networks of physicians and other providers that are held accountable for the cost and quality of the full continuum of care delivered to a group of patients. The ACA authorized Medicare to contract with ACOs with the aim of achieving the "triple aim" of improving quality of care, improving population health, and reducing costs. Similar to the IDSNs of the 1990s, the premise is that ACOs will accomplish these aims by coordinating care, managing chronic disease, and aligning financial incentives for hospitals and physicians. In theory, ACOs can improve quality and lower costs using several methods, including disease management programs, improved care coordination, alignment of incentives for physicians and hospitals via shared savings, use of non-physician providers, and the formation of PCMHs.70 Over the past five years, both the number of participating ACOs and the number of participation options for them have grown dramatically, while potentially generating $400 million in savings for Medicare.71
ACOs are increasingly turning their attention to post-acute providers to better manage cost and quality across the care continuum. A recent descriptive analysis of the structural and functional provider relationships finds that ACOs are expanding their partnerships and developing relationships with LTPAC providers. For example, more than half of Pioneer ACOs have core or structural partnerships72 with HHAs, more than 40 with hospice facilities, and more than 20% with NFs.73 ACOs are also using functional relationships74 to extend the care continuum beyond what can be achieved with care partners alone, particularly for urgent care and post-acute care providers.75
An evaluation of eHIE among ACOS/IDSNs and partnership/acquired LTPAC providers would aim to address the following research questions:
-
Prior to forming a partnership with an ACO/IDSN, what type of EHR systems were LTPAC providers using? Were they electronically exchanging health information with other providers? What type(s) of information were they exchanging and how?
-
How did LTPAC provider's EHR system and technology change after forming a partnership?
-
Once the partnership started, what type of information was exchanged within the system? Outside the system? What technology is being used to exchange this information?
-
How did patient outcomes, utilization, and costs change after the partnership was formed?
-
There are a number of advantages to evaluating HIE between LTPAC providers and their exchange partners within an ACO, or similar model of care (e.g., integrated delivery network [IDN]) setting. First, as previously mentioned, this is priority policy area in the Medicare program and findings from this evaluation would complement prior and ongoing evaluations of the ACO model. Second, it would likely be easier to obtain data by partnering with a single ACO or IDN as opposed to partnering with an HIE that represents multiple organizations. As shown with the prior Abt evaluation, providers participating in KeyHIE declined to provide access to their data for research purposes out of concern that they would be handing over key information to a major competitor. It might also be easier to access CMS claims data because an ACO-focused evaluation would directly benefit the Medicare program. Finally, our case studies and prior research76 indicate that a key advantage of private HIEs within IDNs and ACOs is that eHIE, particularly with LTPAC providers, is more robust within these private organization than in state-sponsored HIEs.
-
The major drawbacks of this approach, however, are that this type of evaluation would be limited and not provide an overall assessment of HIE within a region or market. The organizations that ACOs or IDNs connect are sometimes restricted based on strategic and proprietary interests. For example, hospitals may choose to connect with the ambulatory care and post-acute care providers with whom they would like to more closely affiliate, regardless of existing referral patterns in the market. This complicates overall participation in HIE, data re-use, and ultimately care coordination.
Given what was learned in Pennsylvania and Minnesota, a first step in an evaluation would be an evaluability analysis of candidate sites, using interviews with relevant informants within proposed ACOs/IDNs and focusing on such critical issues as willingness to participate in an evaluation, data availability and access, existence of comparisons, and volume of exchange with LTPAC providers occurring. Having identified the most promising site or sites, we would use a mixed methods approach to address the research questions listed above. We would conduct a survey of LTPAC providers within the selected "treatment" ACO/IDN, and ideally, comparison group providers. This survey would assess the technology used, the regularity and frequency of use, the primary objectives of use, the motivations to engage in exchange, implementation challenges, and the benefits realized. To complement the survey and fill in any potential gaps in understanding of the exchange environment in which the LTPAC providers are operating, we would conduct additional targeted case study interviews with key decision makers within the ACO/IDN across the care continuum. Finally, we would conduct quantitative data analysis with the best available data, which would depend on the location and organizations selected.
Analyses could draw on claims data, EHR and other clinical data, and measures developed from the survey data. Claims data could provide direct measures of patient encounters (e.g., readmission rates) and some treatments and medications. Claims data are accessible from government entities (states, CMS) and from private payers, and increasingly, states and other stakeholders are working to establish all-payer claims databases (APCDs). Based on the experience of a recent ACO evaluation, as a federal contractor, we anticipate that CMS would be willing to approve a data use request for research identifiable Medicare claims and enrollment data from the Chronic Conditions Warehouse (CCW) and ACO-specific data that contains identifying information for participating providers and aligned beneficiaries and their corresponding ACOs.77 A critical issue for the value of the latter information is the ability to identify ACOs that have integrated LTPAC facilities into their networks.
While claims data is currently the main data source used to calculate outcome measures, it might be feasible to use clinical data from EHRs. Much of the information in claims data is now being captured by EHRs and is available at the system level. A notable limitation of EHR data, in contrast to claims, is that comparable data may not be available for potential comparison groups. In addition, the possibility of data sharing arrangements would need to be explored early on.
We would attempt to find a comparison group that consists of similar fee-for-service (FFS) Medicare beneficiaries in markets not served by an ACO and who do not receive care from an ACO/IDN. Alternatively, comparisons might be feasible between IDNs or ACOs in locations where there is a distinct difference in LTPAC participation across networks.
Examples of Potential Settings
Pennsylvania
The Geisinger Health System is one example of an ACO-like model that has incorporated LTPAC providers and continues to do so. In contrast to Abt's evaluation of KeyHIE as a whole, we would only assess eHIE among LTPAC providers and their partners within the Geisinger system.
Results from our site visit suggest that in a departure from its traditional business strategy, Geisinger is increasingly becoming interested in purchasing LTPAC providers. Initially, Geisinger focused mostly on acquiring HHAs. For example, in 2014, Geisinger acquired Sun Home Health and Hospice.78 Several respondents indicated that after completing the acquisition of these HHA sites, Geisinger has focused on the NF sector. One interviewee indicated that Geisinger is trying to develop a "SNFist model" where providers can make decisions at the NF site instead of taking the patients back to the hospital.
From an evaluation and policy perspective, a unique aspect of Geisinger is their development of the Transform tool. Geisinger's 2010 Beacon Community grant provided funding for LTPAC provider outreach and the development of the Transform tool. The KeyHIE Transform tool takes MDS and OASIS data and converts the clinically meaningful information to a CCD. This CCD can be exchanged using KeyHIE so that the all participating providers could access the CCD. The Transform tool is inexpensive relative to the cost of interfacing with an exchange, which appeals to LTPAC providers who may otherwise not be willing to participate in information exchange. The Transform tool was launched in 2013 and provides a unique opportunity for a quasi-experimental design evaluation, with the "pre" period being before 2013 and the "post" period including 2013 and later years. A key question to address in an evaluation would be whether LTPAC providers acquired by Geisinger use the Transform tool and/or whether their EHRs were integrated into Geisinger's system. Another key issue to address is the extent to which Geisinger is working with LTPAC providers that they did not acquire, and the extent to which these providers use Transform.
Minnesota
The Benedictine-Allina project also represents an example of an ACO-like model that has incorporated LTPAC providers. Allina Health is a non-profit health care system based in Minneapolis that owns or operates 14 hospitals and more than 90 clinics throughout Minnesota and Western Wisconsin. Allina Health is participating in the Medicare ACO program. The BHS is one of the largest senior care organizations in the United States, with 36 NFs, 25 ALFs, and one HHA.
We would propose to evaluate the March 2013 e-Health Connectivity Grant as a policy intervention. In 2013, Benedictine received $375,000 from the State of Minnesota to develop MatrixCare software so that it can exchange CCDs with Allina's Epic system peer-to-peer. This new software was launched in December 2013, creating a "post-intervention" period of 2014 and later.
Colorado
Colorado represents a number of potential evaluation opportunities, from the perspective of delivery system reforms involving both Medicare and Medicaid, HIE infrastructure, and data. Colorado also still is largely a FFS state, although its SIM plan includes transitioning to capitation over the next several years.
Colorado's Medicaid Accountable Care Collaborative (ACC), launched in 2011, draws on seven Regional Care Collaborative Organizations (RCCOs) state-wide that develop networks of providers. The RCCOs are responsible for connecting beneficiaries with needed clinical and other services and fostering communications between providers to improve care coordination. The ACC did not initially enroll dually eligible beneficiaries, but it expanded membership to include them in 2014 under the state's Financial Alignment Initiative demonstration.79 The focus will be on improving chronic disease management and transitions between hospitals, rehabilitation hospitals, NFs and community residence.
Physician Health Partners, a medical management company based in Denver, became a Medicare Pioneer ACO in 2012 in partnership with the Primary Physician Partners and South Metro Primary Care. The ACO serves about 30,000 Medicare beneficiaries in the seven-county metro area, and in 2014 began participating in the Medicare Shared Savings Program.
The state has a large and well-established regional HIO, the CORHIO, which in 2011 received a challenge grant from the ONC to increase connections with LTPAC facilities including post-acute rehabilitation hospitals, NHs, assisted living centers, home health care agencies and hospice. As of June, the CORHIO network included 48 hospitals, more than 2,600 providers, 131 long-term care facilities, 39 behavioral health centers, four large medical laboratories, EMS providers, the Colorado Springs Military Health System, and the state health department.
CORHIO provides bidirectional exchange with provider EHRs, but most LTPAC providers are using secure, web-based query access to a community health record system from which they can have real-time access to patient information and the ability to generate CCDs, regardless of whether they have an interoperable EHR. In 2015, CORHIO received a new ONC grant to support implementation of the Transform tool, which would allow LTPAC providers with or without EHRs to translate information from MDS and OASIS assessments and share them through the HIO. Thus, two possible evaluation points are defined by the initial 2011 challenge grant to increase connections with LTPAC providers and the 2015 grant to implement Transform.
The state also has an APCD, administered by the non-profit Center for Improving Value in Health Care (CIVHC). The APCD was established by the legislature in 2010, and as of January 2015, its data warehouse reported health insurance claims from Medicare, Medicaid, and the 20 largest health plans for individual, large group fully-insured, small group and some self-insured lives, as well as Medicaid and Medicare. The claims represent more than 3.5 million unique covered lives and 65% of the insured population in Colorado. Medicare claims for 2009-2011 and 2013 data for commercial payers and Medicaid is currently available through the Data Release Review Process and will be available on the data website in 2015.80 Unlike Minnesota, Colorado allows release of APCD data at varying levels of detail and specificity for research under a CMS-like review process requiring "that the intended use supports reaching the Colorado Triple Aim of better health, better care, and lower costs."
Setting Strengths and Limitations
It is important to consider several factors while conducting an evaluability assessment of the proposed sites. Table 2 uses the three settings described above to illustrate the type of questions to be addressed in selecting an evaluation site or sites. This table provides cross-setting information on several factors, including existing contacts, the availability specific settings and interventions, and the relative ease of access to quantitative data.
Each site has a specific setting and intervention to evaluate. We would evaluate the launch of the KeyHIE Transform Tool in 2013 in Pennsylvania, the 2013 e-Health Connectivity grant in Minnesota, and the 2011 and/or 2015 HITECH grants in Colorado. However, the magnitude of these interventions is likely to vary across settings. For example, the Transform Tool has a more global focus, with the ability to be used by more providers, relative to the smaller e-Health Connectivity grant intervention. Similarly, Colorado's new grant to implement Transform has a broader application than the earlier grant. In contrast to Pennsylvania, however, it might be easier to find a valid comparison group in Minnesota and Colorado, where there is a relatively high prevalence of similar health care systems in the region, compared with Pennsylvania, where Geisinger is one of the most unique and advanced IDNs in the nation. Colorado is likely the best site in terms of claims data access due to the availability of APCD data to researchers.
| TABLE 2. Cross-Setting Comparisons | |||
|---|---|---|---|
| Pennsylvania | Minnesota | Colorado | |
| Contacts from site visits? | Yes | Yes | No |
| Specific setting to evaluate? | Geisinger | BHS-Allina Health | Physician Health Partners and other potential options |
| Intervention for evaluation? | 2010 Beacon Community grant to develop its Transform tool to convert MDS and OASIS data into a CCD (launched in 2013) | March 2013 e-Health Connectivity grant for exchange and use of CCDs between BHS (long-term care system) and Allina (hospital system), via MatrixCare and EpicCare software (launched December 2013). | 2011 HITECH grant to expand LTPAC access 2015 HITECH grant to implement Transform tool |
| Comparison group feasibility? | Challenging, due to Geisinger's uniqueness | Relatively easy, due to high prevalence of IDNs in Minneapolis region | Relatively easy, due to multiple regional networks in operation. |
| Medicare ACO program? [could improve likelihood of CMS approval for claims data] | Medicare Shared Savings Plan ACO (Keystone ACO) | Pioneer ACO (Allina) | Pioneer ACO (Physician Health Partners) |
| APCD? | No | Yes, but not accessible to evaluation except for state contractors | Yes |
General Limitations
There are some general limitations that apply to all settings as well. First, small sample sizes could hinder evaluation efforts at each of the potential sites, especially given the limited post-implementation period of the interventions considered and the relatively low prevalence of NH residence, hospitalizations and post-acute care. About 20% of all Medicare enrollees use hospitals in a year; about 5-6% use SNFs, Part A Home Health, and Part B Home Health, respectively, not adjusting for enrollees using more than one type of post-acute care; and 3% of those age 65 or older reside in NHs.81 Similarly, the interventions to be evaluated are not discrete, that is, implementation was likely phased-in over a relatively long period of time. Second, sample selection could bias any potential estimates since these interventions were not randomly assigned, and each site could also suffer from omitted variable biases as multiple policy interventions and changes to the health care were occurring during the same analysis period. Third, research organizations in any of these settings will likely need to obtain multiple IRB and data use agreement approvals, thus creating substantial time costs in obtaining data. Finally, across all settings, it will likely be very challenging, if not impossible, to directly obtain data from providers (e.g., EHR data) due to privacy and security concerns. However, researchers could potentially obtain aggregated EHR data for sites that cooperate.
Conclusion: Issues to Consider
Awareness is growing that LTPAC providers play a critical role in care coordination and related payment and delivery system reforms intended to improve quality and reduce costs. Examples include ACOs and other new payment and care delivery models (e.g., PCMHs and health homes), Medicare's hospital readmission policy hospital, and post-acute care bundling. eHIE between LTPAC providers and their exchange partners is a promising and important strategy for achieving the ultimate aims of these reform namely improved health system performance.
This study found that progress is being made but increased focus on the importance of LTPAC providers in the care continuum has not yet translated into robust, bidirectional exchange involving LTPAC providers and key trading partners like hospitals and medical groups. Rather, participation of LTPAC providers in eHIE efforts is still in its infancy and generally does not involve the robust, bidirectional exchange initially envisioned in early stages of ARRA HITECH.
As our research shows, there are many challenges to further progress in the area of eHIE between LTPAC providers and their exchange partners. Some major barriers include: lack of funding to support adoption and use of certified HIT that supports interoperable HIE by LTPAC providers; lack of strong enough incentives for critical exchange partners (i.e., hospitals, medical groups, IDSNs) to engage in eHIE with LTPAC providers; competing demands for both LTPAC providers and their exchange partners; limited capacity on the part of many LTPAC providers to use HIT solutions and limited technical assistance to this sector to support and increase their ability to use technology solutions; competitive and proprietary concerns by providers and vendors; provider concerns and misconceptions related to federal and state privacy and security laws, and, a host of significant eHIE technological challenges, some of which disrupt workflow and discourage use. Consequently, as described through this report, eHIE efforts are often opportunistic and very local solutions.
Despite these challenges, our stakeholder interviews and review of the gray literature identified 12 regions around the country where LTPAC providers are involved in the planning or implementation of eHIE and have started to engage in eHIE with key exchange partners. Progress was made with previous funding, and as these existing federal funding opportunities end, new federal funding opportunities are beginning (e.g., ACOs, SIM grants, ONC HIE grants). These provide new opportunities and incentives that are influencing eHIE initiatives and the states and providers that choose to participate in them. For example, the presence of ACOs in many local markets across the United States is prompting some ACOs and key portions of them (e.g., hospitals) to reach out to LTPAC providers and conversely LTPAC providers in those communities to develop eHIE capacity as a way to ensure that referrals from local hospitals continue in the future. The IMPACT Act also has the potential to accelerate LTPAC provider involvement in HIE through its new requirements to standardize and make interoperable post-acute care assessment data.
Where LTPAC providers are participating in eHIE, they currently are often are limited to view-only access to clinical documents, DSM, and partial solutions (e.g., Transform, LAND/SEE). While providing an immediate solution, they have limits, and potentially reduce incentives for adopting more functional, interoperable HIT systems. A potential wildcard in predicting LTPAC provider involvement in eHIE initiatives going forward is the technology used to engage in eHIE. Policymakers, providers, and HIOs are continually trying to anticipate how the technology for enabling exchange with LTPAC providers will evolve and whether there will be a feasible, affordable technology solution in the shorter run and which technologies will be successful longer term. The availability of new technology solutions depends on the HIT/EHR and HIE vendor communities and whether they decide to move into the LTPAC space more aggressively. Findings from the literature review, stakeholder discussions, and case studies suggest that the technology continues to rapidly evolve and those interested in advancing LTPAC involvement in eHIE initiatives should not wait for a so-called "silver bullet" that will produce seamless exchange between LTPAC providers and their exchange partners.
Our findings suggest that the likely migratory path going forward will involve DSM, view-only portals through hospitals and HIE, and, due to considerable regional variation, smaller implementation efforts and assessment of their impacts (i.e., test of specific use cases). The current lack of certified HIT/EHR adoption in the LTPAC market segment constrains bidirectional exchange capability. Certified technology that support more robust forms of exchange are less likely to be adopted by enough LTPAC providers in the near term. Starting small and making incremental changes to EHR and eHIE capacity in the LTPAC setting would facilitate the availability of critical pieces of information needed to care for patients across providers (e.g., medication lists). Given these realities, DSM, view portals, and specific use cases can provide a cost-effective intermediary path forward for data exchange with LTPAC providers. Other new innovative technologies, such as Transform Tool are beginning to take hold and spread, and LAND/SEE is in early stages of implementation after years of planning and development. Even newer and more innovative applications like FHIR are promising but more long-term solutions.
These "pockets of progress" involving LTPAC providers in eHIE across the United States offer rich opportunities for research and learning. Maturation of HIT efforts in some regions, combined with new policy and market dynamics, are beginning to convince at least some LTPAC providers, hospitals, medical groups, and other providers of the value in eHIE efforts and are facilitating more interest in more innovative and robust eHIE approaches. Additionally, new technological solutions offer better opportunities for more robust eHIE involving a wider swath of LTPAC providers.
The time is ripe for targeted research about planning, implementation and impact, particularly what works and does not work and why in eHIE initiatives involving LTPAC providers. Our stakeholder interviews, literature review, and comparative case studies suggest that specific regions have a favorable environment, capable IDSNs, HIOs, and promising technological solutions from which we can learn much about implementation and impact. The Urban Institute team describes one promising approach to conducting a targeted quantitative impact evaluation using ACOs or IDSNs, approaches that could be used in the longer term, as well as potential strengths and limits to various research opportunities and approaches in this arena. The results of such an evaluation as well as other evaluations already underway will help to identify promising approaches to eHIE involving LTPAC providers across the country, provide sound evidence about their ongoing implementation experience, lessons learned, and short and longer term impacts.
Appendix A: Literature Review Bibliography
Abramson, E.L., S. McGinnis, J. Moore, and R. Kaushal. 2014. A statewide assessment of electronic health record adoption and health information exchange among nursing homes. Health Services Research, 49(1 PART 2): 361-72 (accessed November 24, 2014).
Abramson, Erika, L., Michael Silver, and Rainu Kaushal. 2014. Meaningful use status and participation in health information exchange among New York state hospitals: A longitudinal assessment. Joint Commission Journal on Quality and Patient Safety, 40(10): 452-60, http://search.ebscohost.com/login.aspx?direct=true&db=rzh&AN=2012750210&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Alexander, G.L., M. Alwan, L. Batshon, S.M. Bloom, R.D. Brennan Jr., J.F. Derr, M. Dougherty, et al. 2011. Building on a national health information technology strategic plan for long-term and post-acute care: Comments by the long term post acute care health information technology collaborative. Journal of Gerontological Nursing, 37(7): 23-5, http://proxygw.wrlc.org/login?url=http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=medl&AN=21667892; http://ck8gh5qu6z.search.serialssolutions.com/?url_ver=Z39.88-2004&rft_val_fmt=info:ofi/fmt:kev:mtx:journal&rfr_id=info:sid/Ovid:medl&rft.genre=article&rft_id=info:doi/10.3928%2F00989134-20110602-01&rft_id=info:pmid/21667892&rft.issn=&rft.volume=37&rft.issue=7&rft.spage=23&rft.pages=23-5&rft.date=2011&rft.jtitle=Journal+of+Gerontological+Nursing&rft.atitle=Building+on+a+national+health+information+technology+strategic+plan+for+long-term+and+post-acute+care%3A+comments+by+the+Long+Term+Post+Acute+Care+Health+Information+Technology+Collaborative.&rft.aulast=Alexander.
American Physical Therapy Association. 2012. Letter to HIT Policy Committee from Paul Rockar. http://www.healthit.gov/sites/default/files/private/commentsltpac_mu080112rockar.pdf (accessed November 25, 2014).
Arizona Strategic Enterprise Technology. 2012. New electronic health record designed for long-term care providers. https://aset.az.gov/sites/default/files/private/Arizona_HIE_Environmental_Scan_Long_Term_Care.pdf (accessed December 17, 2014).
Babalola, E.O., R.R. Baier, S. Gravenstein, L. Capizzo, A. Zimmerman, and R. Gardner. 2014. Building a health information technology infrastructure in long-term care. Annals of Long-Term Care, 22(6): 43-7.
Blavin, Frederic, Arnav Shah, Nicole Cafarella Lallemand, Kelly J. Devers, and Christal Ramos. 2014. How local context affects providers' adoption and use of interoperable health information technology: Case study evidence from four communities in 2013 (Round Two). Issue Brief, Urban Institute. http://www.urban.org/UploadedPDF/413251-How-Local-Context-Affects-Providers-Adoption-and-Use-of-Interoperable-HIT-2013.pdf (accessed June 25, 2014).
Bhuyan, Soumitra S., He Zhu, Aastha Chandak, Jungyoon Kim, and Jim P. Stimpson. 2014. Do service innovations influence the adoption of electronic health records in long-term care organizations? Results from the U.S. national survey of residential care facilities. International Journal of Medical Informatics, 83(12): 975-982, doi:10.1016/j.ijmedinf.2014.09.007, http://search.ebscohost.com/login.aspx?direct=true&db=edselp&AN=S1386505614001877&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Bryne, Colene, and Michelle Dougherty. 2013. Long-term and post-acute care providers engaged in health information exchange: Final report. Office of the Assistant Secretary for Planning and Evaluation. https://aspe.hhs.gov/report/long-term-and-post-acute-care-providers-engaged-health-information-exchange-final-report.
Caffrey, C., and E. Park-Lee. 2013. Use of electronic health records in residential care communities. Data Brief, National Center for Health Statistics. http://www.cdc.gov/nchs/data/databriefs/db128.htm.
Caillouet, L. Philip. 2012. Health information exchange--A public policy challenge for healthcare professionals and administrators. International Journal of Business and Public Administration, 9(2) (Spring2012): 28-41, http://search.ebscohost.com/login.aspx?direct=true&db=buh&AN=80132669&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Campion, Thomas R. Jr., Alison M. Edwards, Stephen B. Johnson, and Rainu Kaushal. 2013. Health information exchange system usage patterns in three communities: Practice sites, users, patients, and data. International Journal of Medical Informatics, 82(9): 810-20, http://search.ebscohost.com/login.aspx?direct=true&db=rzh&AN=2012312925&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Campion,Thomas R. Jr., Joshua R. Vest, Jessica S. Ancker, and Rainu Kaushal. 2013. Patient encounters and care transitions in one community supported by automated query-based health information exchange. AMIA Annual Symposium Proceedings, AMIA Symposium. 175-84, http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=24551330&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Cannoy, Sherrie Drye, and Pamela E. Carter. 2011. Information politics in health information exchange networks. Journal of Information Privacy and Security (Ivy League Publishing), 7(2): 65-90. International Security and Counter Terrorism Reference Center, EBSCOhost.
CIO Consortium and Nurse Executive Council. 2013. Electronic health record (EHR) solutions LTPAC providers need today. White Paper, American Health Care Association. http://www.ahcancal.org/facility_operations/hit/Documents/2013-06-12%20CIOC-NEC_EHR_WhitePaper_FINAL.pdf.
Colorado Regional Health Information Organization. 2012. Facilitating health information organization. http://www.corhio.org/about.aspx.
Decker, S.L., E.W. Jamoom, and J.E. Sisk. 2012. Physicians in nonprimary care and small practices and those age 55 and older lag in adopting electronic health record systems. Health Affairs, 31(5): 1108-1114.
DeSalvo, Karen, Seth Pazinski, Matthew Swain, and Gretchen Wyatt. 2014. From the national coordinator for health IT: The federal strategy for collecting, sharing, and using electronic health information. Health Affairs Blog, http://healthaffairs.org/blog.
Dhopeshwarkar, Rina V., Lisa M. Kern, Heather C. O'Donnell, Alison M. Edwards, and Rainu Kaushal. 2012. Health care consumers' preferences around health information exchange. Annals of Family Medicine, 10(5): 428-34, http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=22966106&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Dougherty, Michelle, Margaret Williams, Michael Millenson, and Jennie Harvell. 2013. EHR payment incentives for providers ineligible for payment incentives and other funding study. HHS Office of the Assistant Secretary for Planning and Evaluation. https://aspe.hhs.gov/basic-report/ehr-payment-incentives-providers-ineligible-payment-incentives-and-other-funding-study (accessed November 25, 2014).
Dullabh, Prashila, and Lauren Hovey. 2013. Large scale health information exchange: Implementation experiences from five states. Studies in Health Technology and Informatics, 192(10): 613-7, http://search.ebscohost.com/login.aspx?direct=true&db=rzh&AN=2012354014&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Dullabh, P., J. Milstein, C. Nye, A. Moiduddin, L. Virost, E. Babalola, A. Mahmud, and A. Jha. 2012. Evaluation of the state health information exchange cooperative agreement program: Early findings from a review of twenty-seven states. Program Evaluation, NORC at the University of Chicago. http://www.healthit.gov/sites/default/files/private/pdf/state-health-info-exchange-coop-program-evaluation.pdf.
Filipova, Anna A. 2013. Electronic health records use and barriers and benefits to use in skilled nursing facilities. Computers, Informatics, Nursing, 31(7): 305-18, http://search.ebscohost.com/login.aspx?direct=true&db=cmedm&AN=23774447&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Golden, Roblyn, and Gayle Shier. 2012. What does "care transitions" really mean? Generations, 36(4) (Winter2012): 6-12, http://search.ebscohost.com/login.aspx?direct=true&db=aph&AN=85406844&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Goldwater, Jason, and Yael Harris. 2011. Using technology to enhance the aging experience: A market analysis of existing technologies. Ageing International, 36(1): 5-28, http://search.ebscohost.com/login.aspx?direct=true&db=aph&AN=58527060&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Guise, J.M., C. Chang, M. Viswanathan, S. Glick, J. Treadwell, C. Umscheid, E. Whitlock, R. Fu, E. Berliner, R. Paynter, J. Anderson, M. Motu'apuaka, and T. Trikalinos. 2014. Systematic reviews of complex multicomponent health care interventions. Systematic Review, HHS Agency for Healthcare Research and Quality. http://www.effectivehealthcare.ahrq.gov/ehc/products/578/1878/health-care-interventions-review-report-140303.pdf.
Hamann, D.J., and K.C. Bezboruah. 2013. Utilization of technology by long-term care providers: Comparisons between for-profit and nonprofit institutions. Journal of Aging and Health, 25(4): 535-54, http://jah.sagepub.com.proxygw.wrlc.org/content/25/4/535.full.pdf.
Hassol, Andrea, Laura Goodman, Jim Younkin, Mary Honicker, Kimberly Chaundy, and James M. Walker. 2014. Survey of state health information exchanges regarding inclusion of continuity of care documents for long-term post-acute care (LTPAC) patient assessment. Perspectives in Health Information Management, 1-9, http://search.ebscohost.com/login.aspx?direct=true&db=rzh&AN=2012755452&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Health Information Technology Learning Center. Ohio's health information exchange survey for patient centered medical homes. 2013. Ohio Patient-centered Primary Care Collaborative. http://www.odh.ohio.gov/~/media/ODH/ASSETS/Files/chss/PCMH/Ohios%20PCMH%20HIE%20Survey%20Results%20073013.ashx.
Health Information Technology Research Center. Care coordination tool for transition to long-term and post-acute. http://www.healthit.gov/sites/default/files/private/nlc_ltpac_carecoordinationtool.pdf (accessed November 25, 2014).
Health Management Associates. 2014. Colorado regional health information organization (CORHIO) program evaluation. Final Report.
HealthTech Solutions. 2014. State health information exchange cooperative agreement. Evaluation Report, Maine Office of MaineCare Services. http://www.maine.gov/hit/steering/documents/maineoscevaluationreportfinal416.pdf.
HIMSS Health Information Exchange Committee. 2011. Integrating the HIE into the EHR workflow. http://himss.files.cms-plus.com/2011-08-08-IntegratingtheHIEintotheEHRWorkflow.pdf.
HIMSS Interoperability and HIE Business Case Workgroup. 2014. The business case of interoperability and health information exchange. Common Practices Survey. http://himss.files.cms-plus.com/2014-08-28-BusinessCaseforInteroperabilityandHIE.pdf (accessed December 9, 2014).
Hogin, Emily, and Jodi Daniel. 2011. The many meaningful uses of health information technology. Health IT Buzz blog, HealthIT.gov. http://www.healthit.gov/buzz-blog/meaningful-use/meaningful-health-information-technology/ (accessed November 25, 2014).
Howe, Dottie. Smooth transitions of care through CliniSync: Electronic communications fosters better care, lower costs for patients. Ohio Health Information Partnership Health Information in a Heartbeat. http://himss.files.cms-plus.com/2011-08-08-IntegratingtheHIEintotheEHRWorkflow.pdf.
Hustey, Fredric M., and Robert M. Palmer. 2012. Original study: Implementing an internet-based communication network for use during skilled nursing facility to emergency department care transitions: Challenges and opportunities for improvement. Journal of the American Medical Directors Association, 13: 249-53, http://search.ebscohost.com/login.aspx?direct=true&db=edselp&AN=S1525861010002331&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Kentucky Cabinet for Health and Family Services. 2014. Kentucky strategic and operational plan for health information exchange. http://khie.ky.gov/inc/Documents/SOP%20Plan%20Update%20Draft%20June%2014%20FINAL%20Edition.pdf.
Kern, Lisa M., Adam B. Wilcox, Jason Shapiro, Kahyun Yoon-Flannery, Erika Abramson, Yolanda Barrón, and Rainu Kaushal. 2011. Community-based health information technology alliances: Potential predictors of early sustainability. American Journal of Managed Care, 17(4): 290-5, http://search.ebscohost.com/login.aspx?direct=true&db=aph&AN=64458887&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
LaVecchia Ragone, Gina. 2014. Hospitals, LTC facilities connect in Illinois. Long-Term Living: For the Continuing Care Professional, 63(2): 14-5, http://search.ebscohost.com/login.aspx?direct=true&db=aph&AN=95346512&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Mertz, Kory and William Russell. 2013. Improving transitions of care in LTPAC: An update from the theme 2 Challenge Grant awardees. HealthIT.gov. http://www.healthit.gov/sites/default/files/private/challengegrantslessonslearnedltpac_paper.pdf (accessed November 25, 2014).
MacTaggart, Patricia and Jane Hyatt Thorpe. 2013. Long-term care and health information technology: Opportunities and responsibilities for long-term and post-acute care providers. Perspectives in Health Information Management, 10(Fall): 1e. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3797552/.
Morris, Genevieve, Scott Afzal, Mrinal Bhasker, and David Finney. 2012. HIE driven subscription and notification services: Market assessment and policy considerations. HealthIT.gov. http://www.healthit.gov/sites/default/files/private/hie_subscription_notification_final.pdf.
Murphy, Kyle. 2014. ONC targets non-meaningful users with 2015 edition criteria. EHR Intelligence. http://ehrintelligence.com/2014/05/15/onc-targets-non-meaningful-users-with-2015-edition-criteria/.
National eHealth Collaborative. 2013. Trust framework for health information exchange. National HIE Governance Forum, HealthIT.gov. http://www.healthit.gov/sites/default/files/private/trustframeworkfinal.pdf.
No author. 2012. New electronic health record designed for long-term care providers. Annals of Long Term Care, 20(10): 38. http://www.annalsoflongtermcare.com/article/technology-and-product-spotlight.
No author. 2012. The shared task. Long-Term Living: For the Continuing Care Professional, 92(6): 50-51.
Office of the National Coordinator for Health Information Technology. 2014. A ten-year vision to achieve interoperable health IT infrastructure. Concept Paper, HealthIT.gov. http://www.healthit.gov/sites/default/files/private/ONC10yearInteroperabilityConceptPaper.pdf (accessed December 9, 2014).
Office of the National Coordinator for Health Information Technology. 2014. Federal health IT strategic plan. Strategic Plan, HealthIT.gov. http://www.healthit.gov/sites/default/files/private/federal-healthIT-strategic-plan-2014.pdf (accessed December 9, 2014).
Office of the National Coordinator for Health Information Technology. 2013. Health IT in long-term and post-acute care. Policy Brief, HealthIT.gov. http://www.healthit.gov/sites/default/files/private/pdf/HIT_LTPAC_IssueBrief031513.pdf (accessed November 25, 2014).
Ouslander, J.G., A. Bonner, L. Herndon, and J. Shutes. 2014. The interventions to reduce acute care transfers (INTERACT) quality improvement program: An overview for medical directors and primary care clinicians in long term care. Journal of the American Medical Directors Association, 15(3): 162-70.
Palena Hall, Liz. Electronic health record (EHR) incentive program improves EHR adoption and LTPAC. Health IT Buzz blog, HealthIT.gov. http://www.healthit.gov/buzz-blog/ehr-case-studies/long-term-post-acute-care-ltpac-related-ehr-adoption/ (accessed November 25, 2014).
Palena Hall, Liz. Identifying and addressing long-term and post-acute care (LTPAC) priorities. 2012. Health IT Buzz blog, HealthIT.gov. http://www.healthit.gov/buzz-blog/electronic-health-and-medical-records/longterm-postacute-care-ltpac-priorities/ (accessed November 25, 2014).
Park, Hae K., Laurence G. Branch, Tatjana Bulat, Bavna B. Vyas, and Cynthia P. Roever. 2013. Influence of a transitional care clinic on subsequent 30-day hospitalizations and emergency department visits in individuals discharged from a skilled nursing facility. Journal of the American Geriatrics Society, 61(1): 137-42, http://search.ebscohost.com/login.aspx?direct=true&db=aph&AN=84740630&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Park, Hae K. 2012. Care transitions from skilled nursing facilities to the community. Annals of Long Term Care, 20(11): 36-9, http://search.ebscohost.com/login.aspx?direct=true&db=rzh&AN=2011886236&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Pillemer, Karl, Rhoda H. Meador, Jeanne A. Teresi, Emily K. Chen, Charles R. Henderson Jr., Mark S. Lachs, Gabriel Boratgis, Stephanie Silver, and Joseph P. Eimicke. 2012. Effects of electronic health information technology implementation on nursing home resident outcomes. Journal of Aging and Health, 24(1): 92-112, http://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=2011-30549-005&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Platts-Mills, T.F., K. Biese, M. LaMantia, Z. Zamora, L.N. Patel, B. McCall, F. Egbulefu, J. Busby-Whitehead, C.B. Cairns, and J.S. Kizer. 2012. Nursing home revenue source and information availability during the emergency department evaluation of nursing home residents. Journal of the American Medical Directors Association, 13(4): 332-6 (accessed November 24, 2014).
RTI International. 2012. Long-term and post-acute care (LTPAC) roundtable summary report of findings. HealthIT.gov. http://www.healthit.gov/sites/default/files/private/pdf/LTPACroundtablesummary.pdf (accessed November 25, 2014).
Rudin, Robert S., Aneesa Motala, Caroline L. Goldzweig, and Paul G. Shekelle. 2014. Usage and effect of health information exchange: A systematic review. Annals of Internal Medicine, 161(11): 803-11, doi:10.7326/M14-0877.
Ruggiano, Nicole, Ellen L. Brown, Vagelis Hristidis, and Timothy F. Page. 2013. Adding home health care to the discussion on health information technology policy. Home Health Care Services Quarterly, 32(3): 149-162.
Stratis Health. 2014. HITPAC updated. Final Summary Report.
Stratis Health. 2014. Health information technology for post-acute care (HITPAC). Project Brief. http://www.stratishealth.org/documents/project-brief-HITPAC-2014.pdf (accessed December 11, 2014).
Stratis Health. 2014. Understanding and improving medication reconciliation between hospitals and nursing homes. White Paper. http://www.stratishealth.org/documents/Stratis-Health-medication-reconciliation-white-paper-2014.pdf.
Tabar, Pamela. 2013. The power of partnerships. Long-Term Living: For the Continuing Care Professional, 62(6): 10-13. http://www.ltlmagazine.com/article/power-partnerships.
Tabar, Pamela, C.Y. Lu, M. Johantgen, E.S. Muncert, S.A. Bickford, B.L. Guzic, B.R. Demuth, A.R. Bapat, and J.B. Roberts. 2011. Take the trauma out of IT initiatives. Long-Term Living: For The Continuing Care Professional, 61(10): 18, http://search.ebscohost.com/login.aspx?direct=true&db=edb&AN=84364657&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Wolf, Larry. 2014. Seeking your feedback: Voluntary EHR certification behavioral health long-term post-acute care settings. Health IT Buzz blog, HealthIT.gov. http://www.healthit.gov/buzz-blog/federal-advisory-committees/seeking-feedback-voluntary-ehr-certification-behavioral-health-longterm-postacute-care-settings/ (accessed November 25/2014).
Wolf, Larry. 2014. Update to HITSC: Final HITPC recommendations on health IT certification for LTPAC and BH settings. Health IT Policy Committee Presentation, HealthIT.gov. http://www.healthit.gov/FACAS/sites/faca/files/HITSC_CAWG_VoluntaryCert_Materials_2014-07-16.pdf (accessed November 25, 2014).
Wolf, Larry, Jennie Harvell, and Ashish K. Jha. 2012. Hospitals ineligible for federal meaningful-use incentives have dismally low rates of adoption of electronic health records. Health Affairs, 31(3): 505-13, http://search.ebscohost.com/login.aspx?direct=true&db=aph&AN=74054544&site=eds-live&scope=site&authtype=ip,uid&custid=s8987071.
Younkin, Jim. 2012. HIE implementation connects long-term and post-acute care facilities. Health IT Buzz blog, HealthIT.gov. http://www.healthit.gov/buzz-blog/beacon-community-program/hie-implementation-longterm-postacute-care-facilities/ (accessed November 25, 2014).
Zamora, Z., B. McCall, L. Patel, et al. 2012. Implementation of a web-based system to improve the transitional care of older adults. Journal of Nursing Care Quality, 27(2): 182-9 (accessed November 24, 2014).
Appendix B: Technology
The technology challenges facing LTPAC providers and their trading partners mirror the interoperability issues that face the overall health care industry. However, there their manifestation and possible solutions are somewhat unique to this segment. Key technology factors and trends are discussed below.
Private Health Information Exchanges and Vendor Health Information Exchanges
Private HIEs can have several organizing structures including ACOs, IDNs, and vendor networks. These approaches are more focused exchange to support the internal needs of organizations than public HIEs. The high penetration of Epic Systems Corporation and their software solutions including their health exchange product, EpicCare Everywhere, has resulted in this being a common means of exchange. Care Everywhere supports exchange that meets MU Requirements such as interoperable exchange between non-affiliated providers. For exchange between two Epic customers, Care Everywhere breaks the standard CCD and users proprietary data structures. When exchanging data with an EHR with others vendors, Epic uses standards-based approaches.
A second issue is that Epic does not support DSM and unlike most large EHR vendors does not act as a Health Information Service Provider (HISP). This means that providers who are Epic customers must go to third party vendors to for DSM services that most integrated within the Epic system. This provides additional complexity and costs for HISP to HISP interfaces, as providers select different HISP vendors and solutions. Each HISP to HISP solution and interfaces with HIEs must be individually developed.
Our interviews and site visits indicated concerns about the interoperability and dominance of Epic. In Minnesota to the extent that exchange was occurring between IDSNs, this exchange occurred through Care Everywhere between Epic customers. The concern is that this a barrier to exchange that supports continuity of care. This also makes the use of a provider portal, in this case EpicCare Link, the optimal solution for both the hospital system and the LTPAC provider.
Electronic Health Record
As non-eligible providers under MU, LTPAC providers are moving on a parallel but different path than most of their trading partners. Based upon the interviews in the project most LTPAC providers see the primary goal of exchange is the reporting of administrative data as opposed to the exchange of clinical data. The EHR vendors to the LTPAC market have responded to their customer's needs and have not focused on exchange functionality within their software solutions.
PCC, the largest vendor to LTPAC facilities and the common choice among national chains, has only recently supported for DSM and is alone among the LTPAC providers in integrating DSM with an EHR. However, this solution provides the ability to receive a CCD but not consume it or parse that data into the EHR. This is not that different than using a provider portal and printing and scanning the relevant portions into the local EHR as a document.
There is no indication that LTPAC facilities or their EHR vendors are considering the development of an interface solution with public HIEs. The cost, "one-off" nature of the interfaces, programming challenges make this approach infeasible. This means that query-based exchange is not a viable option.
Potential Solutions
There are several solutions to the constraints shaping data exchange and re-use by LTPAC providers and their trading partners. This first of these is the KeyHIE Transform tool developed under a Beacon Grant and being commercialized by Vorro Health. This elegant but simple solution converts the CMS MDS and OASIS into a CCD that can be exchanged and consumed by an EHR. This solution is being sold to and offered by public HIEs, not to LTPAC providers. The number of HIEs who have adopted Transform is not publicly available, but the interviews undertaken indicated that more than six are currently offering the service.
An alternative solution to using an exchange network is peer-to-peer solutions. Within Minnesota, under a state grant, Allina Health (an IDSN) and Benedictine (a LTPAC provider) developed a server to server solution that allowed for the bidirectional exchange and consumption of a CCD. This was between an Epic EHR and the MDI Achieve, a LTPAC EHR developed by MatrixDirect. Although the project achieved all of its goals and objectives, the exchange ended. The reasons cited were a concern about liabilities associated with externally sourced data and an absence of funding to continue software development.
The development of API solutions and standardized data formats such as FHIR (Fast Health Interoperability Resource) have the potential to bring a simplified and lower cost solution to data exchange. The development of exchangeable content as defined Resources provides a foundation for technical and semantic interoperability. Initiatives such as SMART on FHIR and DIRECT on FHIR are demonstrating how EHRs can be extended and accessible. The ability to exchange well-defined modular pieces of information as opposed to the complexity of exchange required under a C-CDA could provide a resolution to technological barriers to interoperability while providing the necessary information to support transitions in care.
Appendix C: Quantitative Evaluation Plan
Introduction
In this report, we outline a plan for quantitative analyses to assess how the growing, but still relatively rare, participation of LTPAC providers in electronic exchange of health information affects utilization, cost, and quality of care outcomes. Specifically, we consider methods and data to better understand how new care delivery and payment systems are resulting in greater integration of LTPAC providers into HIE arrangements and how outcomes differ in areas where exchange is occurring relative to those where it is not. Our plan is informed by the literature review and conceptual framework model developed as part of this project, stakeholder interviews, and what we learned in site visits to two states.
Background
Awareness is growing that LTPAC providers play a critical role in care coordination and related payment and delivery system reforms intended to improve quality and reduce costs. These reforms include ACOs, hospital and post-acute care bundling, various integrated care delivery models, and Medicare's hospital readmission policy.82 eHIE between LTPAC providers and other providers is a promising and important strategy for achieving the goals of improving care coordination and quality, and reducing the cost of care.
Despite the increased focus on the importance of LTPAC in the care continuum, results from this project indicate that integration of these providers into electronic data exchange is still in its infancy. Exchange that is occurring generally is not the robust, bidirectional exchange typically envisioned in earlier studies regarding the potential for improvements in care delivery and outcomes.83
The basic findings are the following:
-
Lack of funding and the business case for LTPAC providers to participate in robust exchange has led to use of ad hoc and often very local solutions.
-
Even in markets where relatively robust exchange is occurring for acute care providers, including hospitals, laboratories, and outpatient care in clinics and physician offices, LTPAC providers most often are limited to view-only access to clinical documents and partial solutions that may reduce incentives for adopting more functional, interoperable EHR systems.
The ARRA of 2009 established HITECH, to accelerate the digitization of the American health care system through greater adoption and the MU of EHRs and the electronic exchange of health information.84 HITECH created three successive stages of MU regulations designed to ensure that providers use EHRs in ways most likely to improve the quality and efficiency of care and, through the EHR Incentive Programs, provided incentives and financial resources for a subset of largely acute care providers to purchase or upgrade EHRs to achieve MU.85 Certain Medicaid providers may also be eligible for EHR incentives under that program.86
SNFs, HHAs, and other post-acute care and long-term care providers, including NFs, have to date been ineligible for financial assistance under either Medicare or Medicaid EHR incentive program and technical assistance under HITECH. These providers are a critical component of the care continuum, especially for key outcomes of current policy aims such as reducing avoidable hospital readmissions, but lag behind in their adoption of certified EHRs and ability to engage in HIE. At the same time, HITECH's Stage 2 MU requirements and other factors such as readmission penalties have increased interest among eligible hospitals and other providers in electronic data exchange with LTPAC partners and other HITECH ineligible providers. Final rules have not been issued for Stage 3 MU. Specific public integrated care programs such as Integrated Care for Dual Eligible Individuals demonstrations and the Medicaid Health Home option are designed to manage and coordinate care across all providers, including LTPAC providers, facilitated where feasible by HIT. In Medicaid Health Homes, however, even such basic tools as timely notifications of hospital admissions and discharges have proved to be an obstacle, even between eligible providers.87 Accelerating interoperable HIE and data use across the care continuum will require special attention to LTPAC providers and other non-eligible providers and strategies to help them catch up and address their unique barriers.
The IMPACT Act of 2014 is one policy development that has the potential to accelerate LTPAC provider involvement in HIE through its new requirements for LTPAC reporting. The act further specifies that specific data elements within each patient assessment instrument be standardized and interoperable to allow for exchange and use of data among LTPAC providers and with other providers. The IMPACT Act requires that CMS standardize post-acute care patient assessment data, including data with regard to specified patient assessment instrument categories and quality measures. In addition, the IMPACT Act intends for data comparability to allow for cross-setting quality comparison in settings including SNFs, HHAs, IRFs, and LTCHs, and, importantly, it conveys the inclusion of patient-centeredness in its references and requirements related to capturing patient preferences and goals.88 The IMPACT Act also requires that standardized post-acute care assessment data elements be made interoperable so as to support the exchange of such data among post-acute care and other providers in order to support access to longitudinal information and coordinated care. The provisions in the IMPACT Act will drive data standardization in post-acute care settings and will support the use of interoperable HIT systems within the LTPAC and interoperable HIE with and by this sector. Because most NFs and HHAs provide both post-acute and long-term care, these requirements have the further potential to enhance eHIE for long-term services and supports as well as post-acute care.
Analytic Plan Roadmap
The purpose of this quantitative analysis plan is to outline and discuss methods for assessing the impact of eHIE participation by LTPAC providers on key outcomes. Considerations fundamental to any such assessment are understanding the degree to which LTPAC providers are engaged in HIE and the types of data they are able to transmit and access.
The plan is informed by key questions that ASPE seeks to address, such as what is the measurable impact of eHIE on the quality, continuity, and cost of care for LTPAC providers and their trading partners. We also draw on the conceptual framework developed in this project and the information and insights about data quality, availability, and related issues (e.g., data use agreements) gathered through stakeholder interviews and site visits in Pennsylvania and Minnesota.
To provide context, we first briefly describe a generic comprehensive approach to a quantitative impact analysis of LTPAC involvement in electronic heath information exchange. We then summarize the key lessons learned and limitations revealed based on insights gathered from the prior project work in locations in Pennsylvania and Minnesota, particularly with respect to the necessity of taking into account the unique characteristics of localities. Given this context, we provide examples of feasible evaluation analyses that could be conducted in Pennsylvania, Minnesota, or other potential markets where an identifiable "intervention" relating to enhanced LTPAC provider participation in electronic data sharing has occurred. We also summarize the pros and cons of each as an illustration of the type of information that should feed into selection of evaluation sites and discuss parameters that would affect evaluation costs.
Comprehensive Approach to Quantitative Impact Analysis
In the abstract, a comprehensive plan for evaluation of eHIE among LTPAC providers would require the following information to identify evaluation targets and factors that may affect outcomes:
-
In what geographic areas, markets, or types of care delivery organizations is electronic exchange of health information occurring?
- What technologies are being used, and what types of information are LTPAC providers and their trading partners creating and transmitting? Different types of eHIE could range from view-only portals and ADT alerts to true interoperable eHIE--defined as the sharing information seamlessly, moving discrete data that can be inserted into another system's database and pulled into its EHR fields.89
- What is the volume and regularity of exchanges per LTPAC admission and discharge?
- What percent of total admissions and discharges do the electronic transmissions represent?
- To what extent is exchanged information timely and comprehensive with respect to patient care across the care continuum?
Assessment of the impact of the areas, markets, or systems identified would then aim to answer the following questions:
-
What is the measureable impact of eHIE on the quality, continuity, and cost of care for: (1) the LTPAC providers; and (2) their trading partners?
- How has eHIE affected specific utilization outcomes of interest, such as 30-day post-hospital discharge readmission rates and hospital admission rates from the ER?
- How has exchange affected costs for each party of interest (e.g., insurer, organized delivery system, hospital, and LTPAC provider)?
- Has exchange affected total Medicare expenditures and resource utilization?
- Do effects differ when assessed from the episode of care (e.g., hospitalization to post-acute to discharge destination) perspective rather than the event (e.g., LTPAC admission) perspective?
To address the first group of questions, we would ideally analyze the types of information LTPAC providers and their trading partners are exchanging. There are two potential points of collection for these data: (1) network servers for public HIOs; and (2) servers supporting private HIEs, such as those of IDSNs and ACOs. Most public HIO participation agreements do not allow the HIO to capture specific information about the nature and type of most clinical data transmitted, however. Thus, network logs would only provide metadata, including the volume of information exchanged and the source and receiver of the information. Such metadata nevertheless could be useful in providing descriptive statistics indicating the geographic range and volume of data exchanged, as well as information about important network nodes and areas where exchange happens less than might be optimal. For private HIEs, more robust data could be available, and these organizations may be willing to share information. For example, during the Pennsylvania site visit, Geisinger was willing to share the number of DSMs that they sent from their EHR system to LTPAC providers during the most recent 30 days, although this would not provide insights on the type of information being transmitted. Data from such a private network could provide richer information, particularly if examined in conjunction with EHR logs.
To address the second group of questions related to the effects of eHIE on patient and provider outcomes, we would examine claims experience of individuals and data on provider characteristics, such as data from the Certification and Survey Provider Enhanced Reports (CASPER)90 and Medicare Cost Reports.91 The strongest evaluation design would be examination of outcomes before and after an identifiable policy or system change (pre/post analysis) for a group of affected participants (or providers) relative to a comparison group not affected by the change (difference-in-difference analysis). In the absence of an actual controlled experiment, we would estimate multivariate regression models comparing patient outcomes, costs, and other outcomes in situations where electronic exchange is occurring to the same outcomes in areas or for providers where electronic exchange is not occurring. Similarly, we could compare regions with robust HIE with similar regions where LTPAC providers lag behind. We would use a propensity score reweighting method, or other method if appropriate, to match the treatment group (i.e., patients in LTPAC facilities that electronically exchange information) with a comparison group based on observable provider, area, and patient characteristics (e.g., socio-demographics and health status) that are available in the given data source. Under this approach, impact assessments would be made based on adjusted comparisons between the experiences of the treatment group and comparison group during the years when exchange occurred.
Lessons Learned from This Project
Unfortunately, quantitative analysis of eHIE in LTPAC is fraught with problems because of the immature state of systems in even the more advanced areas, the fragmentation of systems and technology used across types of providers, and the very local character of exchange solutions. Much of the evaluation methodology for HIE that has been discussed in the literature is hypothetical and applicable only when more robust systems are in place for public exchange--for example, envisioning use of data from HIOs for public and disease monitoring purposes.92 In this section, we discuss major limitations to a comprehensive quantitative evaluation of eHIE based on project findings.
The Urban Institute team conducted case studies and site visits to learn about the following initiatives to enable eHIE with LTPAC providers: KeyHIE in the Northcentral/Northeast region of Pennsylvania, the Fairview Health Services/Ebenezer senior services initiative in Minneapolis, and the Allina Health/BHS initiate, also in Minneapolis. Previous memoranda summarized the eHIE in these markets, particularly as those activities pertain to the involvement of LTPAC providers.93 Specifically, these memoranda summarized key findings from the site visits, efforts to prepare for and implement HIE between LTPAC providers and their partners, and any relevant evaluations underway or completed in these markets. This section summarizes findings from these analyses relating to the feasibility of conducting the comprehensive quantitative evaluation described in the prior section.
Lack of Bidirectional HIE
From a real world perspective with systems as they now stand, a focus on specific use cases of particular policy interest, such as transmission of and access to real-time notifications of hospital admissions, discharges, or transfers, represents an evaluation opportunity: how often and how reliably is transmission to relevant providers occurring and how often do those providers access and act on the information? In turn, the volume and reliability of timely notifications would be hypothesized to affect patient outcomes of interest, such as readmissions. The results of our site visit and qualitative analyses indicate, however, that even among systems further along the planning and early implementation process we selected for examination, obtaining the data underlying such evaluations may be feasible in practice only within integrated systems of affiliated partners, if at all, because of privacy issues and unwillingness of competing organizations participating in an HIO to publish data to the exchange. Even in places where there is a reasonable infrastructure for exchange and a reasonable level of participation, the bulk of exchange occurs among acute care providers--largely hospitals, clinics, and physician offices.
For the country as a whole, the best available information suggests that LTPAC providers lag behind other key providers both in the adoption of EHRs capable of exchange and in the process of the bidirectional electronic exchange of health information.94 Results of our case studies indicate that also is true in the two markets we examined. In both markets, LTPAC providers are generally not involved in robust interoperable HIE with their partners:
-
One of the most commonly found exchange technologies among LTPAC providers in both markets were view-only hospital portals, which are uni-directional and do not capture encounters outside of the hospital or system.
-
Historically, staff at LTPAC facilities in both markets have used a variety of mechanisms, including telephone calls, and faxes to obtain critical patient information. However, using eHIE to gather information, particularly in home health settings, may require use of new technologies such as portable devices, tablets or notebook computers, to capture data during the patient encounter. Moreover, new data formats such as the Transform tool developed by KeyHIE and transport methods, such as Direct, which operate using the new technologies, have been introduced in LTPAC facilities.
-
KeyHIE, a relatively mature HIO covering 53 counties in Northcentral and Northeast Pennsylvania, reports that in April 2015, 82% of its user transactions were through a portal, with only 18% of access being query-based through an EHR. None of the query-based exchange occurred among LTPAC providers, and LTPAC EHRs do not support query-based exchange.
-
Sixty-one long-term care facilities have participation agreements with KeyHIE, but only 18 (11%) are publishing to the exchange. Among the 28 HHAs with participation agreements, only nine (32%) are publishing data. In contrast, 90% of hospitals and 64% of physician practices with participation agreements with KeyHIE are publishing or sharing electronic health data.
-
In 2007, the Minnesota state legislature passed a law stating that "January 1, 2015, all hospitals and health care providers must have in place an interoperable EHR within their hospital system or clinical practice setting." This legislation has contributed to the state's high EHR adoption rate, even among NHs, which are excluded from the mandate.95 However, the definition of EHR in the mandate does not mean a certified EHR that supports data exchange or meets requirements under MU. According to a recent report of Minnesota clinics on the adoption and use of EHRs and HIE, only 10% of NFs and 4% of HHAs in Minnesota currently exchange electronic data using their EHRs.96
-
The Minnesota site visit focused on two initiatives to promote exchange with LTPAC providers in the Minneapolis region: the Fairview-Ebenezer project and the Benedictine-Allina project. One major factor shaping this market is the dominance of Epic EHR systems; the Fairview and Allina health systems both use Epic with the EpicCare Everywhere, an exchange tool used to share patient records with other providers.
Data Access Barriers
There are a number of data challenges in terms of quality, comparability, timeliness, reporting for dual eligibles, and use of data from managed care providers. These challenges depend on the type of data and region under study and also the maturity of the structures and processes in the selected sites.
For the Medicare population, who are dominant users of post-acute care, CMS data are an obvious source for analysis of utilization and cost outcomes and can be used to construct some quality of care measures for both participating providers and any comparison providers. For Medicare FFS beneficiaries, Medicare claims and drug data include most acute and post-acute utilization and spending for beneficiaries, including dual eligibles, and MDS files provide NH utilization for all payers, including Medicaid. These data are available in a uniform format, with a lag of about two years. Medicare claims and beneficiary data and MDS files currently are available through 2013, and data files for 2014 are expected by the end of 2015. Medicare files include a reasonably accurate indicator of Medicaid enrollment. They do not include information on Medicaid financed NF or home health use or cost, but Medicare is the primary payer for most post-acute care for beneficiaries using these providers. Medicare files also are not a reliable source of comprehensive data for beneficiaries enrolled in managed care plans for whom encounter data would be required.97
Medicaid data are effectively not available unless obtained directly from states or providers because of lags in availability. Historically, reporting of eligibility, managed care plan encounters, and claims data to CMS though the Medicaid Statistical Information System (MSIS) has been neither complete nor of uniform quality across states and years. The more analytically friendly, cleaned and processed versions of MSIS data--Medicaid Analytic Extract (MAX) files--produced by a CMS contractor at present are available through 2012 for only 35 states, and their future is uncertain. States are in the process of switching from MSIS to a new reporting system called Transformed MSIS (T-MSIS). At least three states, Colorado, Rhode Island, and North Carolina have stopped submitting MSIS data. The T-MSIS, which ultimately is intended to provide timelier, research-friendly files as part of the CMS Integrated Data Repository. At this point, however, it is still in the development stage, so that both availability and comparability with MAX data for earlier years to examine change over time is in question.
Findings from the case studies provide additional insight into data access in Pennsylvania and Minnesota, and particularly to barriers encountered by earlier evaluation efforts.
Pennsylvania
In 2010, Abt Associates joined Geisinger as an internal evaluator on two projects, both of which are now finished: Geisinger's Keystone Beacon award from ONC and a HIE grant from the Agency for Healthcare Research and Quality (AHRQ). Both projects aimed to address key questions such as who uses KeyHIE and to what extent can KeyHIE's impact on quality and outcomes be measured using the available data.
Abt's initial evaluation design included both quantitative and qualitative methods. Similar to our ideal quantitative evaluation framework, the Abt evaluation team planned to conduct a difference-in-difference analysis, where the data sources they sought for included:
-
KeyHIE's transactional data, including information on admissions, discharges, and transfers; searches used by clinicians to find a specific patient's health information; documents and data downloaded by clinicians; and documents viewed by clinicians.
-
Claims or billing data to study the utilization of services (e.g., ER use) and readmissions.
However, the Abt evaluation team faced significant challenges in collecting the quantitative data needed to conduct their evaluation. Most of the providers participating in KeyHIE declined to give Abt access to their data for research purposes, perhaps out of concern that they would be handing over their data to a major competitor (Geisinger) who would be able to study patient flows and readmission patterns. The Abt evaluation team, like the other Beacon grant evaluators, was also unsuccessful in obtaining Medicare claims data from CMS because the evaluation would not directly benefit the Medicare program.
Without Medicare claims data, the Abt evaluation team was unable to conduct the difference-in-difference analysis originally planned. And with limited permission to access KeyHIE transaction data and billing data from only a handful of participating providers, the Abt evaluation team was unable to complete a descriptive quantitative analysis.
Minnesota
Data access barriers appear less severe in in Minnesota. SHADAC is the state evaluator for Minnesota's CMS SIM grant. As part of its evaluation, SHADAC is charged with evaluating the SIM-funded development and implementation grants awarded through the e-Health Grants Program, including the Fairview-Ebenezer initiative's 12-month development grant. Of the 12 collaboratives awarded a first round e-Health grant, seven include LTPAC providers.
The goals of the SHADAC quantitative and qualitative evaluation include documenting what is going on, what did not go as planned, and implementation barriers and facilitators. The evaluation also focuses on coordination and transitions outcomes (i.e., improved care transitions, quality of care, and costs) and process measures related to being able to exchange health information and use of technology.
Quantitative data sources that the SHADAC evaluation team plans to use for its evaluation of the e-Health grants include a state-fielded EHR survey and a continuum of accountability matrix. Grantees completed the matrix as part of their grant application so the SHADAC evaluation team will be able to assess change over time. Some grantees completed the matrix as a collaborative, and others as an organization.98
SHADAC is going to try to obtain data for its evaluation from the state's APCD, but those data likely will be used to assess the Medicaid ACOs, not the e-Health grants. At present, access to the APCD data are by law limited to staff at the Minnesota Department of Health (MDH) or organizations working under contract with MDH to conduct research on its behalf.99 The theoretical benefits of APCDs, which are in place in about 14 states, are that the data are likely to be available in a more timely fashion than through Medicare, but their value for external evaluation research relies on the availability of data with identifiers for providers and patients that allow tracking over time. In February 2015, a workgroup recommended that the legislature authorize MDH to release public use files, but provider and patient identifiers would not be included.
Revised Quantitative Evaluation Approaches
In light of what we have learned about the reality of LTPAC providers and HIE, the following describes a feasible approach to address the research questions of interest, relying on the incentives and opportunities presented by IDSNs and ACOs, and the use of interoperable HIT tools among LTPAC providers (e.g., the Transform tool).
An overarching lesson was that having a relatively advanced HIE infrastructure is a necessary, but not sufficient condition for integrating exchange with LTPAC providers into the system. At a minimum, evaluating outcomes of exchange including LTPAC requires the ability to identify locations or organizations where LTPAC providers have been integrated into exchange beginning at some identifiable event defining an "intervention" period for a pre/post design. In practice, it is relatively simple to define the event, such as initiation of a program. However, given that implementation is a process that can take substantial time to complete, the intervention period during which change may reasonably be expected can be more difficult to clearly delineate. Thus, it may important consider stages of implementation, early operation, and maturity in evaluation design. In order to implement the stronger difference-in-difference design, the challenge is finding a credible comparison group not exposed to the intervention to examine over the same time periods.
The move toward ACOs under the ACA comes from the need to contain costs in Medicare, but interest and implementation of the model extends to Medicaid programs and predates the ACA. ACOs are networks of physicians and other providers that are held accountable for the cost and quality of the full continuum of care delivered to a group of patients. The ACA authorized Medicare to contract with ACOs with the aim of achieving the "triple aim" of improving quality of care, improving population health, and reducing costs. Similar to the IDSNs of the 1990s, the premise is that ACOs will accomplish these aims by coordinating care, managing chronic disease, and aligning financial incentives for hospitals and physicians. In theory, ACOs can improve quality and lower costs using several methods, including disease management programs, improved care coordination, alignment of incentives for physicians and hospitals via shared savings, use of non-physician providers, and the formation of PCMHs.100 Over the past five years, both the number of participating ACOs and the number of participation options for them have grown dramatically, while potentially generating $400 million in savings for Medicare.101
ACOs are increasingly turning their attention to post-acute providers to better manage cost and quality across the care continuum. A recent descriptive analysis of the structural and functional provider relationships finds that ACOs are expanding their partnerships and developing relationships with LTPAC providers. For example, more than half of Pioneer ACOs have core or structural partnerships102 with HHAs, more than 40 with hospice facilities, and more than 20% with NFs.103 ACOs are also using functional relationships104 to extend the care continuum beyond what can be achieved with care partners alone, particularly for urgent care and post-acute care providers.105
An evaluation of eHIE among ACOS/IDSNs and partnership/acquired LTPAC providers would aim to address the following research questions:
-
Prior to forming a partnership with an ACO/IDSN, what type of EHR systems were LTPAC providers using? Were they electronically exchanging health information with other providers? What type(s) of information were they exchanging and how?
-
How did LTPAC provider's EHR system and technology change after forming a partnership?
-
Once the partnership started, what type of information was exchanged within the system? Outside the system? What technology is being used to exchange this information?
-
How did patient outcomes, utilization, and costs change after the partnership was formed?
There are a number of advantages to evaluating HIE between LTPAC providers and their exchange partners within an ACO, or similar model of care (e.g., IDSN) setting. First, as previously mentioned, this is priority policy area in the Medicare program and findings from this evaluation would complement prior and ongoing evaluations of the ACO model. Second, it would likely be easier to obtain data by partnering with a single ACO or IDSN as opposed to partnering with an HIE that represents multiple organizations. As shown with the prior Abt evaluation, providers participating in KeyHIE declined to provide access to their data for research purposes out of concern that they would be handing over key information to a major competitor. It might also be easier to access CMS claims data because an ACO-focused evaluation would directly benefit the Medicare program. Finally, our case studies and prior research106 indicate that a key advantage of private HIEs within IDSNs and ACOs is that eHIE, particularly with LTPAC providers, is more robust within these private organizations than in state-sponsored HIEs.
The major drawbacks of this approach, however, are that this type of evaluation would be limited and not provide an overall assessment of HIE within a region or market. The organizations that ACOs or IDSNs connect are sometimes restricted based on strategic and proprietary interests. For example, hospitals may choose to connect with the ambulatory care and post-acute care providers with whom they would like to more closely affiliate, regardless of existing referral patterns in the market. This complicates overall participation in HIE, data re-use, and ultimately care coordination.
Methods
Given what was learned in Pennsylvania and Minnesota, a first step in an evaluation would be an evaluability analysis of candidate sites, using interviews with relevant informants within proposed ACOs/IDSNs and focusing on such critical issues as willingness to participate in an evaluation, data availability and access, existence of comparisons, and volume of exchange with LTPAC providers occurring. Having identified the most promising site or sites, we would use a mixed methods approach to address the research questions listed above. We would conduct a survey of LTPAC providers within the selected "treatment" ACO/IDSN, and ideally, comparison group providers. This survey would assess the technology used, the regularity and frequency of use, the primary objectives of use, the motivations to engage in exchange, implementation challenges, and the benefits realized. To complement the survey and fill in any potential gaps in understanding of the exchange environment in which the LTPAC providers are operating, we would conduct additional targeted case study interviews with key decision makers within the ACO/IDSN across the care continuum. Finally, we would conduct quantitative data analysis with the best available data, which would depend on the location and organizations selected.
Analyses could draw on claims data, EHR and other clinical data, and measures developed from the survey data. Claims data could provide direct measures of patient encounters (e.g., readmission rates) and some treatments and medications. Claims data are accessible from government entities (states, CMS) and from private payers, and increasingly, states and other stakeholders are working to to establish APCDs. Based on the experience of a recent ACO evaluation, as a federal contractor, we anticipate that CMS would be willing to approve a data use request for research identifiable Medicare claims and enrollment data from the CCW and ACO-specific data that contains identifying information for participating providers and aligned beneficiaries and their corresponding ACOs.107 A critical issue for the value of the latter information is the ability to identify ACOs that have integrated LTPAC facilities into their networks.
While claims data is currently the main data source used to calculate outcome measures, it might be feasible to use clinical data from EHRs. Much of the information in claims data is now being captured by EHRs and is available at the system level. A notable limitation of EHR data, in contrast to claims, is that comparable data may not be available for potential comparison groups. In addition, the possibility of data sharing arrangements would need to be explored early on.
We would attempt to find a comparison group that consists of similar FFS Medicare beneficiaries in markets not served by an ACO and who do not receive care from an ACO/IDSN. Alternatively, comparisons might be feasible between IDSNs or ACOs in locations where there is a distinct difference in LTPAC participation across networks.
Examples of Potential Settings
Pennsylvania
The Geisinger Health System is one example of an ACO-like model that has incorporated LTPAC providers and continues to do so. In contrast to Abt's evaluation of KeyHIE as a whole, we would only assess eHIE among LTPAC providers and their partners within the Geisinger system.
Results from our site visit suggest that in a departure from its traditional business strategy, Geisinger is increasingly becoming interested in purchasing LTPAC providers. Initially, Geisinger focused mostly on acquiring HHAs. For example, in 2014, Geisinger acquired Sun Home Health and Hospice.108 Several respondents indicated that after completing the acquisition of these HHA sites, Geisinger has focused on the NF sector. One interviewee indicated that Geisinger is trying to develop a "SNFist model" where providers can make decisions at the NF site instead of taking the patients back to the hospital.
From an evaluation and policy perspective, a unique aspect of Geisinger is their development of the Transform tool. Geisinger's 2010 Beacon Community grant provided funding for LTPAC provider outreach and the development of the Transform tool. The KeyHIE Transform tool takes MDS and OASIS data and converts the clinically meaningful information to a CCD. This CCD can be exchanged using KeyHIE so that the all participating providers could access the CCD. The Transform tool is inexpensive relative to the cost of interfacing with an exchange, which appeals to LTPAC providers who may otherwise not be willing to participate in information exchange. The Transform tool was launched in 2013 and provides a unique opportunity for a quasi-experimental design evaluation, with the "pre" period being before 2013 and the "post" period including 2013 and later years. A key question to address in an evaluation would be whether LTPAC providers acquired by Geisinger use the Transform tool and/or whether their EHRs were integrated into Geisinger's system. Another key issue to address is the extent to which Geisinger is working with LTPAC providers that they did not acquire, and the extent to which these providers use Transform.
Minnesota
The Benedictine-Allina project also represents an example of an ACO-like model that has incorporated LTPAC providers. Allina Health is a non-profit health care system based in Minneapolis that owns or operates 14 hospitals and more than 90 clinics throughout Minnesota and Western Wisconsin. Allina Health is participating in the Medicare ACO program. The BHS is one of the largest senior care organizations in the United States, with 36 NFs, 25 ALFs, and one HHA.
We would propose to evaluate the March 2013 e-Health Connectivity Grant as a policy intervention. In 2013, Benedictine received $375,000 from the state of Minnesota to develop MatrixCare software so that it can exchange CCDs with Allina's Epic system peer-to-peer. This new software was launched in December 2013, creating a "post-intervention" period of 2014 and later.
Colorado
Colorado represents a number of potential evaluation opportunities, from the perspective of delivery system reforms involving both Medicare and Medicaid, HIE infrastructure, and data. Colorado also still is largely a FFS state, although its SIM plan includes transitioning to capitation over the next several years.
Colorado's Medicaid ACC, launched in 2011, draws on seven RCCOs state-wide that develop networks of providers. The RCCOs are responsible for connecting beneficiaries with needed clinical and other services and fostering communications between providers to improve care coordination. The ACC did not initially enroll dually eligible beneficiaries, but it expanded membership to include them in 2014 under the state's Financial Alignment Initiative demonstration.109 The focus will be on improving chronic disease management and transitions between hospitals, rehabilitation hospitals, NFs and community residence.
Physician Health Partners, a medical management company based in Denver, became a Medicare Pioneer ACO in 2012 in partnership with the Primary Physician Partners and South Metro Primary Care. The ACO serves about 30,000 Medicare beneficiaries in the seven-county metro area, and in 2014 began participating in the Medicare Shared Savings Program.
The state has a large and well-established regional HIO, the CORHIO, which in 2011 received a challenge grant from the ONC to increase connections with LTPAC facilities including post-acute rehabilitation hospitals, NHs, assisted living centers, home health care agencies and hospice. As of June, the CORHIO network included 48 hospitals, more than 2,600 providers, 131 long-term care facilities, 39 behavioral health centers, four large medical laboratories, EMS providers, the Colorado Springs Military Health System, and the state health department.
CORHIO provides bidirectional exchange with provider EHRs, but most LTPAC providers are using secure, web-based query access to a community health record system from which they can have real-time access to patient information and the ability to generate CCDs, regardless of whether they have an interoperable EHR. In 2015, CORHIO received a new ONC grant to support implementation of the Transform tool, which would allow LTPAC providers with or without EHRs to translate information from MDS and OASIS assessments and share them through the HIO. Thus, two possible evaluation points are defined by the initial 2011 challenge grant to increase connections with LTPAC providers and the 2015 grant to implement Transform.
The state also has an APCD, administered by the non-profit CIVHC. The APCD was established by the legislature in 2010, and as of January 2015, its data warehouse reported health insurance claims from Medicare, Medicaid, and the 20 largest health plans for individual, large group fully-insured, small group and some self-insured lives, as well as Medicaid and Medicare. The claims represent more than 3.5 million unique covered lives and 65% of the insured population in Colorado. Medicare claims for 2009-2011 and 2013 data for commercial payers and Medicaid is currently available through the Data Release Review Process and will be available on the data website in 2015.110 Unlike Minnesota, Colorado allows release of APCD data at varying levels of detail and specificity for research under a CMS-like review process requiring "that the intended use supports reaching the Colorado Triple Aim of better health, better care, and lower costs."
Setting Strengths and Limitations
It is important to consider several factors while conducting an evaluability assessment of the proposed sites. Table C-1 uses the three settings described above to illustrate the type of questions to be addressed in selecting an evaluation site or sites. This table provides cross-setting information on several factors, including existing contacts, the availability specific settings and interventions, and the relative ease of access to quantitative data.
Each site has a specific setting and intervention to evaluate. We would evaluate the launch of the KeyHIE Transform Tool in 2013 in Pennsylvania, the 2013 e-Health Connectivity grant in Minnesota, and the 2011 and/or 2015 HITECH grants in Colorado. However, the magnitude of these interventions is likely to vary across settings. For example, the Transform Tool has a more global focus, with the ability to be used by more providers, relative to the smaller e-Health Connectivity grant intervention. Similarly, Colorado's new grant to implement Transform has a broader application than the earlier grant. In contrast to Pennsylvania, however, it might be easier to find a valid comparison group in Minnesota and Colorado, where there is a relatively high prevalence of similar health care systems in the region, compared with Pennsylvania, where Geisinger is one of the most unique and advanced IDSNs in the nation. Colorado is likely the best site in terms of claims data access due to the availability of APCD data to researchers.
| TABLE C-1. Cross-Setting Comparisons | |||
|---|---|---|---|
| Pennsylvania | Minnesota | Colorado | |
| Contacts from site visits? | Yes | Yes | No |
| Specific setting to evaluate? | Geisinger | BHS-Allina Health | Physician Health Partners and other potential options |
| Intervention for evaluation? | 2010 Beacon Community grant to develop its Transform tool to convert MDS and OASIS data into a CCD (launched in 2013) | March 2013 e-Health Connectivity grant for exchange and use of CCDs between BHS (long-term care system) and Allina (hospital system), via MatrixCare and EpicCare software (launched December 2013). | 2011 HITECH grant to expand LTPAC access 2015 HITECH grant to implement Transform tool |
| Comparison group feasibility? | Challenging, due to Geisinger's uniqueness | Relatively easy, due to high prevalence of IDSNs in Minneapolis region | Relatively easy, due to multiple regional networks in operation. |
| Medicare ACO program? [could improve likelihood of CMS approval for claims data] | Medicare Shared Savings Plan ACO (Keystone ACO) | Pioneer ACO (Allina) | Pioneer ACO (Physician Health Partners) |
| APCD? | No | Yes, but not accessible to evaluation except for state contractors | Yes |
General Limitations
There are some general limitations that apply to all settings as well. First, small sample sizes could hinder evaluation efforts at each of the potential sites, especially given the limited post-implementation period of the interventions considered and the relatively low prevalence of NH residence, hospitalizations and post-acute care. About 20% of all Medicare enrollees use hospitals in a year; about 5-6% use SNFs, Part A Home Health, and Part B Home Health, respectively, not adjusting for enrollees using more than one type of post-acute care; and 3% of those age 65 or older reside in NHs.111 Similarly, the interventions to be evaluated are not discrete, that is, implementation was likely phased-in over a relatively long period of time. Second, sample selection could bias any potential estimates since these interventions were not randomly assigned, and each site could also suffer from omitted variable biases as multiple policy interventions and changes to the health care were occurring during the same analysis period. Third, research organizations in any of these settings will likely need to obtain multiple IRB and data use agreement approvals, thus creating substantial time costs in obtaining data. Finally, across all settings, it will likely be very challenging, if not impossible, to directly obtain data from providers (e.g., EHR data) due to privacy and security concerns. However, researchers could potentially obtain aggregated EHR data for sites that cooperate.
Cost Considerations
The costs associated with any given evaluation would depend on the size (e.g., number of providers, number of patients), and the type of data to be used. Any cost estimate would need to include the cost of data acquisition, such as the cost of an LTPAC provider survey; the cost of identifying, requesting, and, if applicable, negotiating for claims and other data. If a comparison group design is selected, additional survey and data collection costs would need to be factored in. Costs of developing analytic files and conducting analyses could vary significantly depending on the source and type of data. For example, standard format Medicare and assessment files, which are widely used and familiar to researchers, likely would be less expensive to process than data from other sources, which might require considerable interaction with the organization providing the data to specify the data needed and understand its format or to oversee work done within the organization.
The Urban Institute has experience working with contractors with the capability of doing provider surveys. Overall costs depend on various factors, including the number of providers (sample size), the length of the instrument, financial incentives or other methods to increase response rates, etc.
The cost of CMS data depends on the method of access. The Virtual Research Data Center is priced based on an access fee of $40,000 per year for a single user ($25,000 for federal contractors), and a one-time project fee that is data specific and depends on the cohort extracted. No additional charges are incurred for adding years of data to a cohort, but changes in the cohort that require additional extracting generate charges. Projects requiring more than 500 GB of space also have to pay $2,000 for each additional 500 GB block of space. The costs of data obtained from the CCW depend on whether the CCW is asked to extract data for a cohort (versus having the requester provide a "finder" file of beneficiary identifiers, in which case there is no extract charge) and the complexity of the algorithm for extraction. Charges for Medicare data are based on the size of the cohort, the number of services for which files are requested and the number of years of data. For example, for a cohort of 1 million or fewer beneficiaries, inpatient, outpatient, SNF, and durable medical equipment files are $2,000 per year, Carrier claims are $4,000 per year, and Part D Event data are $5,000 per year. There is no charge for beneficiary files if service files are requested.
Summary and Conclusions
This report outlined a feasible structure for evaluations to assess the impact of LTPAC involvement in eHIE on outcomes of particular interest to federal and local policymakers. For context, we first recapped the relatively undeveloped state of HIE among LTPAC providers; reasons for lagging implementation and use of exchange tools, such as DSM, rather than widespread use of certified interoperable EHRs and bidirectional exchange; and current policy changes and initiatives that may accelerate HIE. Chief among those are the IMPACT Act--which requires new levels of reporting by LTPAC providers and specifies that data be standardized and interoperable to support HIE--and a new ONC focus on grants to reach providers such as LTPAC providers who were ineligible for previous incentive programs.
Fundamental needs for such an evaluation are the following:
-
The ability to examine outcomes before and after an identifiable policy or system change (pre/post analysis).
-
Ideally, the ability to identify a comparison group not affected by the change and analyze outcomes over the same time period (difference-in-difference analysis).
-
Access to claims data (pre and post) to assess outcomes.
-
Information about provider characteristics and the volume and types of eHIE happening (e.g., the volume and regularity of exchanges per admission or discharge).
Based on what we learned from earlier project activities, particularly with regard to the state of LTPAC eHIE involvement and data access in our two site visit states, we concluded by outlining a high-level approach for evaluations based on identifying appropriate ACOs or IDSNs and comparing outcomes for their members using LTPAC services. We provided three examples of ACO/IDSNs in Pennsylvania, Minnesota, and Colorado where such evaluations would be possible. There are, of course, other possibilities among provider partners in Accelerating Change and Transformation in Organizations and Networks (ACTION III),112 states originally considered in the early stages of this project, as well as in additional potential in other states that, like Colorado, received new ONC grants to implement the Transform tool (Delaware and Illinois), or where Transform is already being implemented, including Pennsylvania's KeyHIE.
Identifying appropriate comparisons remains a challenge in any of the settings, but focusing on a discrete set of LTPAC partners in selected ACOs/IDSNs provides a more manageable structure than, for example, starting with LTPAC providers and identifying the multiple hospitals and practices with whom they interact. A simplifying approach to data acquisition would be to focus on Medicare FFS beneficiaries, for whom CMS claims and beneficiary information would represent all spending except Medicaid financed long-term care for beneficiaries who are eligible for both programs. However, partnerships with ACOs/IDSNs may hold the potential for both claims data and analysis of the volume and nature of data exchanges if data access and privacy issues can be addressed.
Notes
-
Devers, K., N. Lallemand, G. Ozanich, et al. 2015.Health information exchange in long-term and post-acute care settings: Conceptual framework. Commissioned by the Assistant Secretary for Planning and Evaluation. Freedman, V., and B. Spillman. 2014. Disability and care needs among older americans. Milbank Quarterly, 92(3): 509-41, doi:10.1111/1468-0009.12076. Stefanacci, R.G., and B.S. Spivack. 2014. Long-term care regulatory and practice changes: Impact on care, quality, and access. Annals of Long-Term Care, 22(11), http://www.annalsoflongtermcare.com/article/long-term-care-regulatory-and-practice-changes-impact-care-quality-and-access.
-
Government Accountability Office. 2015. Nonfederal efforts to help achieve health information interoperability. GAO-15-817, http://www.gao.gov/assets/680/672585.pdf.
-
Devers, K., N. Lallemand, G. Ozanich, et al. 2015.Health information exchange in long-term and post-acute care settings: Conceptual framework. Commissioned by the Assistant Secretary for Planning and Evaluation. Lallemand, N., A. Napoles, K. Devers, et al. 2015. Pennsylvania site visiting findings. Memorandum commissioned by the Assistant Secretary for Planning and Evaluation. Lallemand, N. , A. Napoles, K. Devers, et al. 2015. Minnesota site visit findings. Memorandum commissioned by the Assistant Secretary for Planning and Evaluation.
-
Includes both NHs and skilled nursing facilities (SNFs).
-
American Health Care Association. 2015. Trends in nursing facility characteristics. http://www.ahcancal.org/research_data/trends_statistics/Documents/Trend_PVNF_FINALRPT_March2015.pdf.
-
Administration on Aging, Administration for Community Living. 2012. A profile of Older Americans: 2012. U.S. Department of Health and Human Services. http://www.aoa.gov/Aging_Statistics/Profile/2012/docs/2012profile.pdf.
-
Grady, PA. n.d. Advancing the health of our aging population: A lead role for nursing science. Nursing Outlook, 59(4): 207-209, Science Citation Index, EBSCOhost.
-
CMS Claims Data, prepared by Health Dimensions Group 2013.
-
Centers for Medicare and Medicaid Services. Home health quality initiative. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HomeHealthQualityInits/index.html?redirect=/HomeHealthQualityInits/14_HHQIOASISUserManual.asp.
-
Morley, M., S. Bogasky, B. Gage, et al. 2014. Medicare post-acute care episodes and payment bundling. Medicare and Medicaid Research Review, 4(1), https://www.cms.gov/mmrr/downloads/mmrr2014_004_01_b02.pdf.
-
Resnick, H.E., B.B. Manard, R.I. Stone, and M. Alwan. 2009. Use of electronic information systems in nursing homes: United States, 2004. Journal of the American Medical Informatics Association, 16(2): 179-186, MEDLINE Complete, EBSCOhost.
-
Office of the Assistant Secretary for Planning and Evaluation. 2014. Electronic health information exchange in LTPAC: Preparation, implementation, and impact. Request for Task Order/Proposal/Solicitation #14-233-SOL-00365.
-
Office of the National Coordinator for Health Information Technology. 2014. A ten-year vision to achieve interoperable health IT infrastructure. Washington, DC: ONC. https://www.healthit.gov/sites/default/files/private/ONC10yearInteroperabilityConceptPaper.pdf. Office of the National Coordinator for Health Information Technology. 2014. Draft interoperability roadmap. Washington, DC. https://www.healthit.gov/policy-researchers-implementers/draft-interoperability-roadmap.
-
U.S. Department of Health and Human Services. 2015. Medicare and Medicaid programs; electronic health record incentive program--modifications to meaningful use in 2015 Through 2017. Proposed Rule, 42 CFR Part 495, 80(72), Part III, http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/Modifications_MU_Rule.pdf. For the 2015-2017 new rule released October 6, 2015, see https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2015-Fact-sheets-items/2015-10-06.html and https://s3.amazonaws.com/public-inspection.federalregister.gov/2015-25595.pdf.
-
Decker, S.L., E.W. Jamoom, and J.E. Sisk. 2012. Physicians in nonprimary care and small practices and those age 55 and older lag in adopting electronic health record systems. Health Affairs, 31(5): 1108-1114.
-
Yin, R.K. 1999. Enhancing the quality of case studies in health services research. Health Services Research, 34(5 Pt 2): 1209-1224.
-
Flood, A.B., M. Fennell, K.J. Devers. 2012. Health reforms as examples of multilevel interventions in cancer care. JNCI Monographs, (44): 80-85, doi:10.1093/jncimonographs/lgs012.
-
Minnesota Department of Health. 2015. Understanding the Minnesota interoperable electronic health record mandate. http://www.health.state.mn.us/e-health/hitimp/2015mandateguidance.pdf.
-
Office of the National Coordinator for Health Information Technology. 2015. Health information exchange challenge grant program. HealthIT.gov. http://www.healthit.gov/providers-professionals/health-information-exchange-challenge-grant-program.
-
Hogin, E., and J. Daniel. 2011. The many meaningful uses of health information technology. Health IT Buzz blog, HealthIT.gov. http://www.healthit.gov/buzz-blog/meaningful-use/meaningful-health-information-technology/.
-
The of the National Coordinator for Health Information Technology. n.d. Beacon community program. HealthIT.gov. http://www.healthit.gov/policy-researchers-implementers/beacon-community-program.
-
Stratis Health. 2014. HITPAC updated. Final Summary Report.
-
Bryne, C., and M. Dougherty. 2013. Long-term and post-acute care providers engaged in health information exchange: Final report. Office of the Assistant Secretary for Planning and Evaluation. Available at https://aspe.hhs.gov/report/long-term-and-post-acute-care-providers-engaged-health-information-exchange-final-report. Harvell, J., M. Harr, E. Palena Hall, et al. 2012. Implementing health information exchange in the long-term and post-acute care community. Presentation, AHIMA Foundation. http://campus.ahima.org/audio/2012/RB121212.pdf.
-
Stratis Health. 2013. Environmental scan of adoption and use of electronic health records and health information exchange in Minnesota skilled nursing facilities. Centers for Medicare and Medicaid Services, Special Innovation Project. http://www.stratishealth.org/documents/MN_Environmental_Scan_HITPAC.pdf.
-
Centers for Medicare and Medicaid Services. 2013. CMS initiative to reduce avoidable hospitalizations among nursing facility residents. Fact Sheet. http://innovation.cms.gov/initiatives/rahnfr/.
-
Centers for Medicare and Medicaid Services. 2015. State innovation models initiative: Model test awards round two. CMS.gov. http://cmswnmgteam.polldaddy.com/s/was-this-helpful?iframe=http%3A%2F%2Finnovation.cms.gov%2Finitiatives%2FState-Innovations-Model-Testing-Round-Two%2F&ft=1.
-
Geisinger Health System. 2010. 2010 system report. http://www.geisinger.org/pages/newsroom/includes/pdf/ar10-111714.pdf.
-
Office of the National Coordinator for Health Information Technology. 2015. 2015 edition final rule: Supporting care across the continuum. https://www.healthit.gov/sites/default/files/private/2015editioncareacrosscontinuum_10615.pdf.
-
Office of the National Coordinator for Health Information Technology. 2015. Community interoperability and health information exchange cooperative agreement program. HealthIT.gov. http://www.healthit.gov/newsroom/community-interoperability-and-health-information-exchange-cooperative-agreement-program.
-
Office of the National Coordinator for Health Information Technology. 2014. State health information exchange cooperative agreement program. HealthIT.gov. http://www.healthit.gov/policy-researchers-implementers/state-health-information-exchange.
-
Kern, L.M., A.B. Wilcox, J. Shapiro, et al. 2011. Community-based health information technology alliances: Potential predictors of early sustainability. American Journal of Managed Care, 17(4): 290-5.
-
Health Management Associates. 2014. Colorado regional health information organization (CORHIO) program evaluation. Final Report.
-
About Healthcare. About Kindred. http://www.kindredhealthcare.com/our-company/company-overview/.
-
Office of the National Coordinator for Health Information Technology. 2015. HITECH act. HealthIT.gov. http://www.healthit.gov/policy-researchers-implementers/health-it-legislation.
-
U.S. Department of Health and Human Services. 2012. Health information technology: Standards, implementation specifications, and certification criteria for electronic health record technology. Final Rule, 77 FR 54163. https://federalregister.gov/a/2012-20982.
-
Mostashari, F. 2012. Meaningful use stage 2: What it means for interoperability.Health IT Buzz blog. http://www.healthit.gov/buzz-blog/meaningful-use/meaningful-use-stage-2/.
-
Keystone Health Information Exchange. About us. http://www.keyhie.org/about_us/compliance.html.
-
Minnesota Department of Health. 2015. Understanding the Minnesota interoperable electronic health record mandate. http://www.health.state.mn.us/e-health/hitimp/2015mandateguidance.pdf.
-
Senate Finance Committee. 2014. The improving Medicare post-acute care transformation act of 2014. http://www.finance.senate.gov/imo/media/doc/IMPACT%20Summary.pdf.
-
U.S. Department of Health and Human Services Press Office. 2015. HHS proposes to improve care and safety for nursing home residents. http://www.hhs.gov/news/press/2015pres/07/20150713d.html.
-
Centers for Medicare and Medicaid Services. 2015. Medicare and Medicaid programs; reform of requirements for long-term care facilities. Proposed rule, 80 FR 55284. https://www.federalregister.gov/articles/2015/09/15/2015-23110/medicare-and-medicaid-programs-reform-of-requirements-for-long-term-care-facilities-reopening-of.
-
Adler-Milstein, J., C.M. DesRoches, M.F. Furukawa, et al. 2014. More than half of US hospitals have at least a basic EHR, but stage 2 criteria remain challenging for most. Health Affairs; 33(9): 1664-1671. doi:10.1377/hlthaff.2014.0453.
-
Furukawa, M.F., J. King, V. Patel, et al. 2014. Despite substantial progress in EHR adoption, health information exchange and patient engagement remain low in office settings. Health Affairs, doi:10.1377/hlthaff.2014.0445.
-
Zamora, Z., B. McCall, L. Patel, et al. 2012. Implementation of a web-based system to improve the transitional care of older adults. Journal of Nursing Care Quality, 27(2): 182-9.
-
Geisinger Health System. 2014. Transforming healthcare through continuous innovation. System Report. http://www.geisinger.org/pages/newsroom/includes/pdf/ar-final-2014.pdf.
-
Minnesota Department of Health. 2015. Understanding the Minnesota interoperable electronic health record mandate. http://www.health.state.mn.us/e-health/hitimp/2015mandateguidance.pdf.
-
Long-Term and Post-Acute Care (LTPAC) Health Information Technology (IT) Collaborative. 2012. A roadmap for health IT in long-term and post-acute care (LTPAC). http://www.ltpachealthit.org/sites/default/files/private/LTPAC_HealthIT_Roadmap_2012-2014%28Final%29.pdf. Office of the National Coordinator for Health Information Technology. 2012. Long-term and post-acute care (LTPAC) roundtable summary report of findings." http://www.healthit.gov/sites/default/files/private/pdf/LTPACroundtablesummary.pdf.
-
Mertz, K., and W. Russell. 2013. Improving transitions of care in LTPAC: An update from the theme 2 Challenge Grant awardees. HealthIT.gov. http://www.healthit.gov/sites/default/files/private/challengegrantslessonslearnedltpac_paper.pdf.
-
Health Management Associates. 2014. Colorado regional health information organization (CORHIO) program evaluation. Final Report.
-
Hustey, F.M., and R.M. Palmer. 2012. Original study: Implementing an internet-based communication network for use during skilled nursing facility to emergency department care transitions: Challenges and opportunities for improvement. Journal of the American Medical Directors Association, 13: 249-53.
-
Bresnick, J. 2014. HIMSS: Sustainability top of mind for RECs as funding dries up. EHR Intelligence. https://ehrintelligence.com/news/himss-sustainability-top-of-mind-for-recs-as-funding-dries-up.
-
Office of the National Coordinator for Health Information Technology. Care coordination tool for transition to long-term and post-acute care. http://www.healthit.gov/sites/default/files/private/nlc_ltpac_carecoordinationtool.pdf.
-
LeadingAge. 2015. Electronic health record adoption and health information exchange among long-term and post-acute care providers: A survey of LeadingAge New York members. http://www.leadingageny.org/linkservid/2E102FA3-007E-0553-F50E1E2BB975E3DC/showMeta/0/.
-
Minnesota Department of Health. 2012. MN e-health report: Nursing homes adoption and use of EHRs and exchange of health information. http://www.health.state.mn.us/e-health/summaries/reportnursehome2011.pdf.
-
LeadingAge. 2015. Electronic health record adoption and health information exchange among long-term and post-acute care providers: A survey of LeadingAge New York members. http://www.leadingageny.org/linkservid/2E102FA3-007E-0553-F50E1E2BB975E3DC/showMeta/0/.
-
Private correspondence with Varro Health on September 25, 2015.
-
Health Level Seven Special Committee. 2015. FHIR infrastructure. http://www.hl7.org/Special/committees/fiwg/overview.cfm.
-
Stratis Health. 2014. HITPAC updated. Final Summary Report.
-
Yeager, V.A., D. Walker, E. Cole, et al. 2014. Factors related to health information exchange participation and use." Journal of Medical Systems 38(8): 78, MEDLINE Complete, EBSCOhost. Dullabh, P., J. Adler-Milstein, H. Hovey, et al. 2014. Key challenges to enabling health information exchange and how states can help. FinalReport, Office of the National Coordinator for Health Information Technology. https://www.healthit.gov/sites/default/files/private/state_hie_evaluation_stakeholder_discussions.pdf. Blavin, F.E., A. Shah, N. Cafarella Lallemand, et al. 2014. How local context affects providers' adoption and use of interoperable health information technology: Case study evidence from four communities in 2013 (Round Two). Issue Brief, Urban Institute. http://www.urban.org/UploadedPDF/413251-How-Local-Context-Affects-Providers-Adoption-and-Use-of-Interoperable-HIT-2013.pdf. Devers, K.J., A. Shah, and F. Blavin. 2014. How local context affects providers' adoption and use of interoperable health information technology: Case study evidence from four communities in 2012 (Round One). Issue Brief, Urban Institute. http://www.urban.org/research/publication/how-local-context-affects-providers-adoption-and-use-interoperable-health-information-technology.
-
Stratis Health. 2014. HITPAC updated. Final Summary Report.
-
Office of the National Coordinator for Health Information Technology. 2015. Health information exchange challenge grant program. HealthIT.gov. http://www.healthit.gov/providers-professionals/health-information-exchange-challenge-grant-program.
-
Centers for Medicare and Medicaid Services. 2015. State innovation models initiative: Model test awards round two. CMS.gov. http://cmswnmgteam.polldaddy.com/s/was-this-helpful?iframe=http%3A%2F%2Finnovation.cms.gov%2Finitiatives%2FState-Innovations-Model-Testing-Round-Two%2F&ft=1.
-
Shapiro, J.S. (2007). Evaluating public health uses of health information exchange.Journal of Biomedical Informatics, 40: S46-S49. Shapiro, J.S., F. Mostashari, G. Hripcsak, N. Soulakis, and G. Kuperman. 2011. Using health information exchange to improve public health. American Journal of Public Health, 101(4): 616-623, doi:10.2105/AJPH.2008.158980.
-
Lallemand, N., A. Napoles, K. Devers, et al. 2015. Pennsylvania site visiting findings. Memorandum commissioned by the Assistant Secretary for Planning and Evaluation. Lallemand, N., A. Napoles, K. Devers, et al. 2015. Minnesota site visit findings. Memorandum commissioned by the Assistant Secretary for Planning and Evaluation.
-
Berenson, R., and R. Burton. 2012. Health policy brief: Next steps for ACOs. Health Affairs. Burns, L., and M. Pauly. 2012. Accountable care organizations may have difficulty avoiding the failures of integrated care networks of the 1990s. Health Affairs, 31: 2407-2416.
-
Pham, H., J. Pilotte, R. Rajkumar, et al. 2015. Medicare's vision for delivery-system reform--The role of ACOs. New England Journal of Medicine, 373(11): 987-990.
-
Core partners are identified as part of the ACO in its application to CMS or share in the costs of the ACO.
-
Based upon the site visits and interviews, there is market segmentation between long-term care facilities and HHAs in terms of the types of technology adopted and their use for data exchange. HHAs appear more likely to be using a module from a certified EHR vendor than a NH or SNF. This is likely due to either the HHA being owned by a hospital system or having a close hospital system affiliation.
-
Functional relationships are those that the ACO has with providers that are not core partners that facilitate management of beneficiaries across settings. They typically include data sharing agreements and adoption of common protocols.
-
L&M Policy Research. 2015. Evaluation of CMMI accountable care organization initiatives: Pioneer ACO evaluation findings from performance years one and two. Centers for Medicare and Medicaid Services. http://innovation.cms.gov/Files/reports/PioneerACOEvalRpt2.pdf.
-
Lallemand, N., A. Napoles, K. Devers, et al. 2015. Pennsylvania site visiting findings. Memorandum commissioned by the Assistant Secretary for Planning and Evaluation. Lallemand, N., A. Napoles, K. Devers, et al. 2015. Minnesota site visit findings. Memorandum commissioned by the Assistant Secretary for Planning and Evaluation.
-
For example, see http://www.resdac.org/cms-data/files/ssp-aco-provider-level-rif/data-documentation.
-
Scicchitano, E. 2014. Geisinger, SUN home health to "integrate". Newsitem.com. http://newsitem.com/news/geisinger-sun-home-health-to-integrate-1.1669782.
-
Colorado Department of Health Care Policy and Financing. 2014. Accountable care collaborative (ACC): Medicare-Medicaid program. https://www.colorado.gov/pacific/hcpf/accountable-care-collaborative-acc-medicare-medicaid-program. Musumeci, Marybeth. 2015. Financial and administrative alignment demonstrations for dual eligible beneficiaries compared: States with memoranda of understanding approved by CMS. Kaiser Family Foundation. http://kff.org/medicaid/issue-brief/financial-and-administrative-alignment-demonstrations-for-dual-eligible-beneficiaries-compared-states-with-memoranda-of-understanding-approved-by-cms/.
-
Administration on Aging, Administration for Community Living. 2012. A profile of Older Americans: 2012. U.S. Department of Health and Human Services. http://www.aoa.gov/Aging_Statistics/Profile/2012/docs/2012profile.pdf.
-
Devers, K., N. Lallemand, G. Ozanich, et al. 2015. Health information exchange in long-term and post-acute care settings: Conceptual framework. HHS Office of the Assistant Secretary for Planning and Evaluation. Freedman, V., and B. Spillman. 2014. Disability and care needs among older americans. Milbank Quarterly, 92(3): 509-41, doi:10.1111/1468-0009.12076. Stefanacci, R.G., and B.S. Spivack. 2014. Long-term care regulatory and practice changes: Impact on care, quality, and access. Annals of Long-Term Care, 22(11), http://www.annalsoflongtermcare.com/article/long-term-care-regulatory-and-practice-changes-impact-care-quality-and-access.
-
Lallemand, N., A. Napoles, K. Devers, et al. 2015. Pennsylvania site visiting findings. Memorandum commissioned by the Assistant Secretary for Planning and Evaluation. Lallemand, N., A. Napoles, K. Devers, et al. 2015. Minnesota site visit findings. Memorandum commissioned by the Assistant Secretary for Planning and Evaluation.
-
Blumenthal, D. 2010. Launching HITECH. New England Journal of Medicine, 362(5): 382-385.
-
An introduction to the Medicaid EHR incentive program for eligible professionals. https://www.cms.gov/regulations-and-guidance/legislation/ehrincentiveprograms/downloads/ehr_medicaid_guide_remediated_2012.pdf. Eligible providers are physicians (primarily doctors of medicine and doctors of osteopathy), nurse practitioners, certified nurse-midwives, dentists, physician assistants who furnish services in a federally qualified Health Center or Rural Health Clinic that is led by a physician assistant, and in some states optometrists.
-
Spillman, B.C., E.H. Allen, and A. Spencer. 2015. Evaluation of the Medicaid health home option for beneficiaries with chronic conditions: Provider experiences with implementation, service delivery, and health information technology, final annual report: Year 3. HHS Office of the Assistant Secretary of Planning and Evaluation. https://aspe.hhs.gov/basic-report/evaluation-medicaid-health-home-option-beneficiaries-chronic-conditions-annual-report-year-three
-
Senate Finance Committee. 2014. The improving Medicare post-acute care transformation act of 2014. http://www.finance.senate.gov/imo/media/doc/IMPACT%20Summary.pdf.
-
Stratis Health. 2014. Progress in cross-setting health information exchange in Minnesota. http://www.stratishealth.org/pubs/qualityupdate/sp14/HIE.html.
-
CASPER contains information on NF, HHA, and hospice provider characteristics, as well as citations for substandard care, and quality measures and is used in production of CMS's Nursing Home and Home Health Compare. It is a compilation of all the data elements collected during the inspection survey conducted for the purpose of certification for participation in CMS programs.
-
An alternative approach would be from the provider perspective. The power of such an approach depends on the number of providers included, not the number of individuals served by those providers. See, for example, Peikes, D., S. Dale, E. Lundquist, J. Genevro, and D. Meyers. 2011. Building the evidence base for the medical home: What sample and sample size do studies need? White Paper, Mathematica Policy Research, Contract No. HHSA290200900019I TO2, AHRQ Publication No. 11-0100-EF. Rockville, MD: Agency for Healthcare Research and Quality. Because our interest is in evaluating patient outcomes in the presence and absence of health information exchange, not a particular model, we focus on an individual level.
-
Shapiro, J.S. (2007). Evaluating public health uses of health information exchange.Journal of Biomedical Informatics, 40: S46-S49. Shapiro, J.S., F. Mostashari, G. Hripcsak, N. Soulakis, and G. Kuperman. 2011. Using health information exchange to improve public health. American Journal of Public Health, 101(4): 616-623, doi:10.2105/AJPH.2008.158980.
-
Lallemand, N., A. Napoles, K. Devers, et al. 2015. Pennsylvania site visiting findings. Memorandum commissioned by the Assistant Secretary for Planning and Evaluation. Lallemand, N., A. Napoles, K. Devers, et al. 2015. Minnesota site visit findings. Memorandum commissioned by the Assistant Secretary for Planning and Evaluation.
-
Devers, K., N. Lallemand, G. Ozanich, et al. 2015. Health information exchange in long-term and post-acute care settings: Conceptual framework. HHS Office of the Assistant Secretary for Planning and Evaluation.
-
Minnesota Department of Health, Office of Health Information Technology. 2015. Understanding the Minnesota interoperable electronic health mandate. http://www.health.state.mn.us/e-health/hitimp/2015mandateguidance.pdf.
-
Minnesota Department of Health, Office of Health Information Technology. 2015. Understanding the Minnesota interoperable electronic health mandate. http://www.health.state.mn.us/e-health/hitimp/2015mandateguidance.pdf.
-
General Accounting Office. 2014. Medicare advantage: CMS should fully develop plans for encounter data and assess data quality before use. http://www.gao.gov/assets/670/665142.pdf.
-
Lallemand, N., A. Napoles, K. Devers, et al. 2015. Minnesota site visit findings. Memorandum commissioned by the Assistant Secretary for Planning and Evaluation.
-
Minnesota Department of Health. 2015. All payer claims database--Overview. http://www.health.state.mn.us/healthreform/allpayer/.
-
Berenson, R., and R. Burton. 2012. Health policy brief: Next steps for ACOs. Health Affairs. Burns, L., and M. Pauly. 2012. Accountable care organizations may have difficulty avoiding the failures of integrated care networks of the 1990s. Health Affairs, 31: 2407-2416.
-
Pham, H., J. Pilotte, R. Rajkumar, et al. 2015. Medicare's vision for delivery-system reform--The role of ACOs. New England Journal of Medicine, 373(11): 987-990.
-
Core partners are identified as part of the ACO in its application to CMS or share in the costs of the ACO.
-
Based upon the site visits and interviews, there is market segmentation between long-term care facilities and HHAs in terms of the types of technology adopted and their use for data exchange. HHAs appear more likely to be using a module from a certified EHR vendor than a NH or SNF. This is likely due to either the HHA being owned by a hospital system or having a close hospital system affiliation.
-
Functional relationships are those that the ACO has with providers that are not core partners that facilitate management of beneficiaries across settings. They typically include data sharing agreements and adoption of common protocols.
-
L&M Policy Research. 2015. Evaluation of CMMI accountable care organization initiatives: Pioneer ACO evaluation findings from performance years one and two. Centers for Medicare and Medicaid Services. http://innovation.cms.gov/Files/reports/PioneerACOEvalRpt2.pdf.
-
Lallemand, N., A. Napoles, K. Devers, et al. 2015. Pennsylvania site visiting findings. Memorandum commissioned by the Assistant Secretary for Planning and Evaluation. Lallemand, N., A. Napoles, K. Devers, et al. 2015. Minnesota site visit findings. Memorandum commissioned by the Assistant Secretary for Planning and Evaluation.
-
For see http://www.resdac.org/cms-data/files/ssp-aco-provider-level-rif/data-documentation.
-
Scicchitano, E. 2014. Geisinger, SUN home health to "integrate". Newsitem.com. http://newsitem.com/news/geisinger-sun-home-health-to-integrate-1.1669782.
-
Colorado Department of Health Care Policy and Financing. 2014. Accountable care collaborative (ACC): Medicare-Medicaid program. https://www.colorado.gov/pacific/hcpf/accountable-care-collaborative-acc-medicare-medicaid-program. Musumeci, Marybeth. 2015. Financial and administrative alignment demonstrations for dual eligible beneficiaries compared: States with memoranda of understanding approved by CMS. Kaiser Family Foundation. http://kff.org/medicaid/issue-brief/financial-and-administrative-alignment-demonstrations-for-dual-eligible-beneficiaries-compared-states-with-memoranda-of-understanding-approved-by-cms/.
-
Centers for Medicare and Medicaid Services. 2014. IMPACT Act of 2014 and cross setting measures. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Post-Acute-Care-Quality-Initiatives/IMPACT-Act-of-2014-and-Cross-Setting-Measures.html. Freedman, V.A., and B.C. Spillman. 2014. The residential continuum from home to nursing home: Size, characteristics and unmet needs of older adults. Journal of Gerontology: Social Sciences, 69(Suppl 1): S42-S50, doi:10.1093/geronb/gbu120.
-
ACTION III is a contract mechanism AHRQ uses to support field-based delivery system research. The Urban Institute is a subcontractor to multiple prime organizations on this funding vehicle. For additional information on ACTION III, see http://www.ahrq.gov/research/findings/factsheets/translating/action3/index.html.
Project Information
Electronic Health Information Exchange in Long-Term/Post-Acute Care (LTPAC): Preparation, Implementation, and Impact
This report was prepared under contract #HHSP23320100025WI between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the Urban Institute. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the ASPE Project Officers, Iara Woody and Jennie Harvell, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201; Iara.Woody@hhs.gov.