
U.S. Department of Health and Human Services
Federal Programs for Persons with Disabilities
Brian O. Burwell, Bonnie Preston, and Sarah Bailey
Mathematica Policy Research, Inc.
January 1990
PDF Version: http://aspe.hhs.gov/daltcp/reports/task2es.pdf (143 PDF pages)
The paper was written as part of contract #HHS-100-88-0047 between U.S. Department of Health and Human Services (HHS), Office of Social Services Policy (now the Office of Disability, Aging and Long-Term Care Policy (DALTCP) and Mathematica Policy Research, Inc. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the office at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. The e-mail address is: webmaster.DALTCP@hhs.gov. The DALTCP Project Officer was Michele Adler.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
- CHAPTER 1. INTRODUCTION
- CHAPTER 2. THE SOCIAL SECURITY DISABILITY INSURANCE (DI) PROGRAM
- 2.1 Overview and Purpose
- 2.2 Authorization, History, and Funding
- 2.3 Definition of Disability
- 2.4 Administrative Structure
- 2.5 Eligibility for Benefits
- 2.6 Benefit Levels
- 2.7 Cost of Living Adjustments (COLAs)
- 2.8 Recent Program History and Legislative Changes
- 2.9 Program Interactions
- 2.10 Special Program Issues
- 2.11 Program Data
- CHAPTER 3. THE SUPPLEMENTAL SECURITY INCOME (SSI) PROGRAM
- 3.1 Overview and Purpose
- 3.2 Authorization, History and Funding
- 3.3 Definition of Disability
- 3.4 Administrative Structure
- 3.5 Eligibility for Benefits
- 3.6 SSI Benefits
- 3.7 Recent Program History and Legislative Changes
- 3.8 Program Interactions
- 3.9 Special Program Issues
- 3.10 Program Data
- CHAPTER 4. DISABILITY PROGRAMS OF THE DEPARTMENT OF VETERANS AFFAIRS
- 4.1 Disability Compensation Program
- 4.2 Disability Pension Program
- CHAPTER 5. FEDERAL CIVIL SERVICE PROGRAMS
- 5.1 Federal Employees Compensation Program
- 5.2 Federal Civil Service Disability Program
- CHAPTER 6. BLACK LUNG PROGRAM
- 6.1 Overview and Purpose
- 6.2 Authorization, History and Funding
- 6.3 Definition of Disability
- 6.4 Administrative Structure
- 6.5 Eligibility
- 6.6 Services/Benefit Provided
- 6.7 Program Interactions
- 6.8 Program Data
- CHAPTER 7. MEDICARE COVERAGE OF PERSONS WITH DISABILITIES
- 7.1 Overview and Purpose
- 7.2 Authorization, History and Funding
- 7.3 Definition of Disability
- 7.4 Administrative Structure
- 7.5 Eligibility
- 7.6 Services Provided Under Medicare
- 7.7 Recent Program History and Legislative Changes
- 7.8 Program Interactions
- 7.9 Special Issues
- 7.10 Program Data
- CHAPTER 8. MEDICAID COVERAGE OF PERSONS WITH DISABILITIES
- 8.1 Overview and Purpose
- 8.2 Authorization, History and Funding
- 8.3 Definition of Disability
- 8.4 Administrative Structure
- 8.5 Eligibility
- 8.6 Medicaid Services
- 8.7 Recent Legislative Changes
- 8.8 Program Interactions
- 8.9 Special Issues
- 8.10 Program Data
- CHAPTER 9. DEPARTMENT OF VETERANS AFFAIRS HEALTH SERVICES PROGRAMS
- 9.1 Overview and Purpose
- 9.2 Authorization, History, and Funding
- 9.3 Administrative Structure
- 9.4 Eligibility
- 9.5 Services Provided
- 9.6 Program Interactions
- 9.7 Program Data
- CHAPTER 10. CHAMPUS PROGRAM FOR THE HANDICAPPED
- 10.1 Overview and Purpose
- 10.2 Authorization, History and Funding
- 10.3 Definition of Disability
- 10.4 Administrative Structure
- 10.5 Eligibility
- 10.6 Services/Benefits Provided
- 10.7 Program Interactions
- 10.8 Program Data
- CHAPTER 11. SOCIAL SERVICES BLOCK GRANT
- 11.1 Overview and Purpose
- 11.2 Authorization, History and Funding
- 11.3 Definition of Disability
- 11.4 Administrative Structure
- 11.5 Eligibility
- 11.6 Services/Benefits Provided
- 11.7 Program Data
- CHAPTER 12. ADMINISTRATION ON DEVELOPMENTAL DISABILITIES PROGRAMS
- 12.1 Overview and Purpose
- 12.2 Authorization, History and Funding
- 12.3 Definition of Disability
- 12.4 Administrative Structure
- 12.5 Eligibility
- 12.6 Services/Benefits Provided
- 12.7 Program Data
- CHAPTER 13. MATERNAL AND CHILD HEALTH BLOCK GRANT: PROGRAMS FOR CHILDREN WITH SPECIAL HEALTH CARE NEEDS
- 13.1 Overview and Purpose
- 13.2 Authorization, History and Funding
- 13.3 Administrative Structure
- 13.4 Eligibility
- 13.5 Services/Benefits Provided
- 13.6 Program Data
- CHAPTER 14. ALCOHOL, DRUG ABUSE AND MENTAL HEALTH SERVICES BLOCK GRANT
- 14.1 Overview and Purpose
- 14.2 Authorization, History and Funding
- 14.3 Definition of Disability
- 14.4 Administrative Structure
- 14.5 Eligibility
- 14.6 Services/Benefits Provided
- 14.7 Special Issues
- CHAPTER 15. CHILD WELFARE SERVICES
- 15.1 Title IV-B Child Welfare Services
- 15.2 Title IV-E Foster Care and Title IV-E Adoption Assistance
- CHAPTER 16. DEPARTMENT OF EDUCATION PROGRAMS
- 16.1 State Grants for Special Education Programs
- 16.2 Program for Handicapped Children in State-Operated Programs
- 16.3 Preschool Incentive Grants Program/Preschool Grants Program
- 16.4 Handicapped Infants and Toddlers Program
- 16.5 Basic Vocational Rehabilitation Services
- LIST OF EXHIBITS
- EXHIBIT 2-1: Disability Determinations and Appeals, FY 1988
- EXHIBIT 2-2: Beneficiaries, Payments and Average Benefits in the DI Program: January 1989
- EXHIBIT 2-3: Disabled Workers and Dependents Receiving Monthly SSDI Cash Benefits: 1980-1988
- EXHIBIT 2-4: SSDI Disabled Workers by Age and Sex
- EXHIBIT 2-5: Adult Disabled Children Receiving Monthly SSDI Cash Benefits: 1980-1987
- EXHIBIT 3-1: Deeming of Income from Spouse to Spouse in Determining Eligibility for SSI Benefits
- EXHIBIT 3-2: Deeming of Income for Parents to a Disabled Child in Determining Eligibility for SSI Benefits
- EXHIBIT 3-3: Federal SSI Benefit Standards for Individuals and Couples Living Independently: 1980 to 1989
- EXHIBIT 3-4: Average Monthly State Supplementation Payment to Disabled SSI/SSP Recipients: December 1987
- EXHIBIT 3-5: Number of Disabled Persons Receiving SSI/SSP Benefits, Total Federal/State Payments to Disabled Persons and Average Monthly Benefit Levels: January 1989
- EXHIBIT 3-6: Number of Disabled Persons Receiving Federally-Administered SSI/SSP Payments 1980-1988
- EXHIBIT 3-7: SSI Disabled Recipients by Age Cohort
- EXHIBIT 4-1: VA Disability Compensation Program: Average Annual Benefit Level by Percent Disability, 1987
- EXHIBIT 4-2: VA Disability Compensation Program: Average Annual Benefit Level 1980-1987
- EXHIBIT 4-3: VA Disability Compensation Program: Class of Dependent, 1987
- EXHIBIT 4-4: Number of Persons Receiving Benefits Under the Veterans Administration Disability Compensation Program 1980 to 1987
- EXHIBIT 4-5: Annual Payments Made Under the Veterans Administration Disability Compensation Program 1980 to 1990
- EXHIBIT 4-6: VA Disability Pension Program: Average Annual Expenditure per Case FY 1980-FY 1987
- EXHIBIT 4-7: Veterans Receiving Benefits Under the Disability Pension Program 1980 to 1987
- EXHIBIT 4-8: Annual Payments Made under the Veterans Administration Disability Pension Program 1980 to 1990
- EXHIBIT 5-1: Number of Cases Filed Per Year Under the Federal Employees Compensation Program 1984 to 1988
- EXHIBIT 5-2: Annual Benefits Paid Under the Federal Employees Compensation Program: 1982 to 1989
- EXHIBIT 5-3: Number of Beneficiaries Receiving Disability Payments under the Federal Civil Service Disability Program 1980 to 1987
- EXHIBIT 5-4: Annual Benefits Paid under the Federal Civil Service Disability Program: 1980 to 1986
- EXHIBIT 6-1: Number of Persons Receiving Black Lung Benefits from the Social Security Administration and Department of Labor
- EXHIBIT 6-2: Annual Payments for Black Lung Benefits Made by the Social Security Administration and Department of Labor 1980 to 1988
- EXHIBIT 7-1: Estimated Medicare Disabled Enrollees, Users, Costs per Recipient, and Program Expenditures Under Part A and Part B: FY 1989
- EXHIBIT 7-2: Medicare Disabled Enrollees: 1980 to 1989
- EXHIBIT 7-3: Distribution of Medicare Disabled Population: 1987
- EXHIBIT 8-1: Federal Medical Assistance Percentages: FY 1989
- EXHIBIT 8-2: Medicaid Coverage Options for Disabled Individuals
- EXHIBIT 8-3: Distribution of Medicaid Expenditures for the Disabled: 1987
- EXHIBIT 8-4: Medicaid Disabled Recipients: 1980 - 1987
- EXHIBIT 8-5: Medicaid Disabled Recipients by Institutional Status and Cash Assistance Status FY 1980 - 1987
- EXHIBIT 11-1: Annual Funding of the Social Services Block Grant 1980 to 1990
- EXHIBIT 12-1: Annual Funding of the Administration on Developmental Disabilities Basic State Grant Program: 1980 to 1989
- EXHIBIT 13-1: Annual Federal Funding of the Maternal and Child Health Block Grant
- EXHIBIT 14-1: Annual Funding of the Alcohol, Drug Abuse and Mental Health Services Block Grant: 1982 to 1989
- EXHIBIT 16-1: Number of Children Enrolled in Special Education Program 1980 to 1987
- EXHIBIT 16-2: Annual Federal Funding for Special Education Programs 1980 to 1987
- EXHIBIT 16-3: Number of Handicapped Children in State-Operated Educational Programs 1980 to 1987
- EXHIBIT 16-4: Annual Federal Funding for Handicapped Children in State-Operated Educational Programs: 1980 to 1987
- EXHIBIT 16-5: Number of Children Served in Preschool Incentive Grant Programs 1980 to 1987
- EXHIBIT 16-6: Annual Federal Funding for Preschool Incentive Grant Programs 1980 to 1987
- EXHIBIT 16-7: Annual Number of Clients Served by State Vocational Rehabilitation Programs: 1980 to 1987
- EXHIBIT 16-8: Annual Federal Funding for State Vocational Rehabilitation Programs 1982 to 1990
PREFACE
This report was prepared under Contract No. HHS-88-0047 to the Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. The overall purpose of the project, Disability Profiles and Policy Analyses, was to produce a series of analytical reports and policy analyses of the working-age disabled population using data from the 1984 Panel of the Survey of Income and Program Participation (SIPP). This report, Federal Programs for Persons with Disabilities, constitutes one report of the series, and is intended to serve as a compendium of the major Federal assistance programs for persons with disabilities.
The Federal project officer was Michele Adler of the Office of the Assistant Secretary for Planning and Evaluation (ASPE), Office of Social Services Policy, Division on Disability, Aging and Long-Term Care. This report was prepared by SysteMetrics/McGraw-Hill under subcontract to Mathematica Policy Research, which was the prime contractor. The Project Director at Mathematica Policy Research was Pat Doyle, Ph.D.
The authors would like to thank Michele Adler and Lowell Ayre of ASPE, and Pat Doyle and Craig Thornton of Mathematica Policy Research, for their comments on previous drafts of this report. Administrative support at SysteMetrics/McGraw-Hill was provided by Kipp Gabriel. The statements contained in the report are solely those of the authors and do not necessarily reflect the views or policies of the Department of Health and Human Services. The authors assume sole responsibility for the accuracy of the information contained in the report. The authors confess to instances of outright plagiarism of other government publications which also describe the various disability programs presented in this report, particularly when it was felt that no improvements in presentation were possible.
CHAPTER 1. INTRODUCTION
Federal assistance to persons with disabilities is provided through a wide variety of programs throughout the Federal government. Indeed, the development of Federal policies concerning the provision of assistance to persons with disabilities is hampered by the fact that there are a bewildering array of Federal programs which provide financial assistance, health insurance coverage and direct supportive services to people who have various types of disabling conditions. These programs often interact, or overlap, with regard to eligibility rules, services provided, and benefit levels in complex, not to mention confusing, ways.
The purpose of this report is to provide an overview of some of the major Federal programs which provide assistance to persons with disabling conditions. The report is by no means a complete compendium of Federal assistance programs. There are many other Federal programs, not included here, which provide financial assistance or services to disabled people. The report focuses on the larger Federal programs, in terms of persons served and annual expenditure levels, with a particular focus on the four major sources of cash assistance and health insurance coverage: Social Security Disability Insurance (SSDI), the Supplemental Security Income (SSI) program, Medicare and Medicaid.
In the report, we focus on programs, or components of programs, which provide assistance to persons with disabilities who are under the age of 65. Many persons with disabling conditions have conditions which are strongly associated with the aging process, and many Federal programs are designed to provide assistance to persons who develop disabling conditions during their later stages of life. This report makes a distinction between Federal programs which provide assistance to persons under age 65 with disabilities, and to persons with disabilities over the age of 65, whenever the data are available to make such a distinction. For example, in our descriptions of Medicare and Medicaid, we have focused on the components of these programs which provide health insurance coverage for persons under the age of 65 only.
The program descriptions included in this report also focus only on those programs which involve the direct expenditure of resources from the Federal budget. We have not included descriptions of legislation and programs which are designed to protect the legal and civil rights of persons with disabilities with regard to education, housing, transportation, access, civil liberties and protection from victimization. The report also does not include descriptions of Federal tax expenditures for persons with disabilities relating to various provisions of the Internal Revenue code. These expenditures include such provisions as the exclusion of Social Security and Medicare benefits from Federal income tax, exclusion of workmen's compensation benefits paid to disabled coal miners, and special tax credits for persons with disabilities.
The report is divided into three major sections. The first section describes programs which provide direct financial assistance to persons who are not able to support themselves through work as a result of a disabling condition. The second section describes programs which provide health insurance and direct medical care to persons who are disabled, and because they are not in the work force, do not have access to employer-sponsored health care benefits. The third section describes some of the major Federal programs which finance direct supportive services to persons with disabilities.
We have tried to make all of the program descriptions comparable in format and structure, although this was sometimes difficult due to the fundamental differences between disability insurance programs and direct services programs, entitlement versus discretionary programs, and so on. One key feature we have tried to focus on is how each program defines the concept of "disability" and what eligibility rules and administrative procedures are established in each program to determine whether an applicant for benefits meets that program's operational definition of "disabled." In our review of these programs, it has become clear to us that the concepts of "disabled" and "not disabled" are not ones that are easily operationalized in the development of equitable and judicious program policies which, on the one hand, assist persons with disabling conditions to live productive and independent lives, but which, on the other hand, do not reinforce cultural barriers which have historically excluded, and continue to exclude, persons with disabling conditions from participating in the mainstream of business, sports, recreation, family life, entertainment, transportation, and educational opportunities available to persons without disabling conditions.
The Federal programs described in this report provided over $85 billion in cash assistance, medical care, and direct services to persons with disabilities under the age of 65 in FY 1989, constituting about 7.7% of total Federal outlays for the year. It is hoped that this report will provide readers with some understanding of how these resources are being spent, who is being served, and how these various Federal programs contribute, or fail to contribute, to a comprehensive Federal policy towards non-elderly persons with disabling conditions.
CHAPTER 2. THE SOCIAL SECURITY DISABILITY INSURANCE (DI) PROGRAM
2.1 Overview and Purpose
The Social Security Disability Insurance (DI) program provides monthly cash benefits to insured disabled workers under age 65 and their dependents. Like the Old-Age and Survivors Insurance Program (OASI), the purpose of the DI program is to replace income lost when a wage-earner is no longer able to work. It is the primary social insurance program in the United States for protecting workers from the potential loss of income due to a mental or physical disability that results in an inability to work. In FY 1989, an estimated $23.6 billion in cash benefits were paid to 4.1 million disabled workers and their dependents under the DI program.
2.2 Authorization, History, and Funding
The Disability Insurance (DI) was originally authorized under Title II of the Social Security Act in 1956. Initially, benefits were provided only to disabled workers age 50 and older. Benefits for dependents of disabled workers were added under the 1958 Social Security Amendments, and benefits were extended to disabled workers under age 50 under the 1960 amendments.
DI program benefits and administrative costs are financed primarily by a portion of the Federal Insurance Contribution Act (FICA) payroll tax on wages covered by Social Security. In January 1989, the FICA tax paid by both the employer and employee was 7.51 percent of the first $48,000 of earnings. In 1989, 0.53 percent of the tax was allocated to the Disability Insurance Trust Fund, which is the source of payment for monthly DI benefits and for administrative expenses. In addition, the revenue derived from the taxation of disability benefits is also credited to the Trust Fund.
2.3 Definition of Disability
To be considered disabled, an applicant for DI benefits must demonstrate the inability to engage in any substantial gainful activity by reason of any medically determinable physical or mental impairment which can be expected to result in death or has lasted or can be expected to last for a continuous period of not less than 12 months.
This definition is the foundation of the Social Security disability determination process. The actual process by which Social Security determines whether an applicant meets this definition is significantly more complicated. A more detailed description of the disability determination process is provided in Section 2.5.1. This definition of disability is the same for the DI program and for disability benefits provided under the Supplemental Security Income (SSI) program.
2.4 Administrative Structure
Unlike the OASI program, which is administered entirely by Federal employees of the Social Security Administration (SSA), the DI program is administered both by SSA and by State Disability Determination Services (DDDs), which are responsible for determining which applications should be awarded benefits. DDSs make disability determinations based on uniform regulations promulgated by SSA. The costs of making disability determinations for DI applicants are born entirely by the Federal government, but the personnel making the determinations are State employees.
To apply for DI benefits, a disabled worker must file an application at one of the Social Security Administration's more than 1,300 field offices. If a disabled worker is incapable of filing an application in person, then an application may be filed by phone or by mail, or if necessary, a Social Security worker will come to the disabled workers home. In processing a claim for benefits, an SSA claims representative first determines whether the applicant meets the "nondisability" eligibility requirements, primarily whether the claimant has achieved insured status. If the claimant has insured status, then the application is sent to the State Disability Determination Service (DDS), where the claim is evaluated and the determination of disability is made.
A multi-layered administrative structure has been developed by SSA for dealing with appeals of denied disability claims. If a disabled worker's claim for DI benefits is denied by the State Disability Determination Services (DDS) agency, he or she may request a reconsideration of the claim within 60 days of denial. The reconsideration is also conducted by the State DDS agency, but by different personnel from those who made the initial determination. If the application is again denied, then the claimant is allowed a hearing before an administrative law judge (ALJ). If the claim is denied by the administrative law judge, then the claimant has 60 days to request a review by the Appeals Council. The Appeals Council may review, affirm, modify or reverse the decision of the ALJ, or it may remand it to the AW for further development. After a decision by the Appeals Council, a claimant may seek further review of his or her claim only by a filing a civil action within 60 days in a United States district court.
2.5 Eligibility for Benefits
2.5.1 Eligibility for disabled workers' benefits
To be eligible for disabled workers' benefits, a worker must: (1) have achieved insured status; and (2) be determined disabled according to criteria established by the Social Security Administration. There is a 5-month waiting period between the time that a claimant is determined entitled to benefits and the time in which benefits begin.
(1) Insured status
As an insurance program, benefits under the DI program are only available to disabled persons who have previously worked, and to their dependents. A person builds disability protection through work in employment covered under Social Security. "Insured status" needed to qualify for disability benefits differs somewhat from that needed to qualify for retirement and survivors' (OASI) benefits. To achieve insured status for disability benefits, a person must:
- Have at least one quarter of coverage for each calendar year after the year in which he or she attained the age of 21 (e.g. a person of age 53 must have earned at least 32 quarters of coverage); AND
- Have no fewer than 20 quarters of coverage during the 40-quarter period prior to the first month in which his or her disability is determined to have begun; OR
- If determined disabled prior to age 31, have earned coverage for at least half of all quarters occurring after he or she turned age 21 and prior to the quarter in which he or she were first disabled. A minimum of six (6) quarters of coverage is required.
For persons who are determined to be blind, only the first condition listed above (A) is required to achieve insured status; neither the second nor third conditions apply.
To be credited with a quarter of coverage, workers must earn a minimum amount of covered earnings. Since 1978, the crediting of quarters of coverage has been on an annual rather than a quarterly basis. In 1989, one quarter of coverage is earned for each $500 of covered earnings, up to a maximum of four quarters of coverage per year. The amount of annual earnings needed to earn a quarter of coverage is updated annually based on increases in average wages.
(2) Determination of disability
The essential problem in disability is that it is not possible to construct a set of medical and vocational standards that will distinguish perfectly between those who are able to work and those who are not able to work.
--1979 Advisory Council on Social Security
The statutory definition of disability used in both the Social Security Disability Insurance (DI) program and the Supplemental Security Income (SSI) program is intentionally stringent and has been left largely unchanged since the enactment of the DI program in 1956. In order to be considered disabled, an applicant for DI or SSI disability benefits must demonstrate the inability to engage in any substantial gainful activity by reason of any medically determinable physical or mental impairment which be expected to result in death or has lasted or can be expected to last for a continuous period of not less than 12 months. This definition is the cornerstone of the SSA disability determination process. Only persons who are totally disabled, whose disability is expected to be long-term, and who are unable to work at any substantial level, are eligible for disability benefits. Short-term, temporary disabilities, no matter how severe, are not covered under the DI or SSI programs.
The administrative structure for conducting disability determinations involves a joint partnership between SSA and State agencies. State agencies, generally known as disability determination services (DDSs) are responsible for determining which applicants should be awarded benefits. However, DDSs make disability determinations based on uniform regulations prescribed by SSA. although DDSs are staffed by State employees, the States are fully reimbursed by the Federal government for all administrative costs of conducting disability determinations. There is no State flexibility in the conduct of disability determinations; in theory anyway, the disability determination process should be administered uniformly across all fifty States.
If a person wishes to file for DI or SSI disability benefits, they must first file an application at one of SSA's more than 1,300 field offices. For DI, an SSA claims representative first determines whether the applicant has insured status, and meets other nondisability criteria for benefits. If insured, initial disability determinations are then conducted in a five-step sequential evaluation process, as described below:
Step One: Is the claimant engaging in substantial gainful activity (SGA)?
The first step in the disability determination process is generally conducted by SSA field office staff. This involves a determination of whether the applicant is currently working at a level of substantial gainful activity. In 1988, regulations defined SGA as monthly earnings of over $300 for persons with disabilities and over $700 for persons who are blind.1 If a person is earning more than the SGA limit, this is considered to be evidence that he or she is capable of work, regardless of other evidence of physical or mental disability. In such cases, the applicant is found not to be disabled, and medical and vocational factors are not evaluated.
Step Two: Does the claimant have a severe impairment?
If a claimant is not working, or working at the SGA level, then the application is forwarded to the State DDS. At the DDS, a team consisting of a disability examiner and a physician is assigned to the case. The team gathers medical and vocational evidence concerning the applicant's disability from available records. If the medical evidence of record is incomplete or conflicting, then the disability examiner may set up a medical examination and/or specialized tests, at no cost to the applicant. After obtaining sufficient medical evidence, the DDS team then determines whether the applicant's impairment (or combination of impairments) is severe, and if the impairment is expected to result in death or is expected to last for at least 12 months. If the applicant's impairment is found not to be severe, or if the impairment is not expected to result in death or to last for at least 12 months, then the applicant is determined not to be disabled for purposes of receiving DI or SSI benefits.
Step Three: Is the impairment so severe as to meet or equal the requirements of the medical listing in the regulations?
Those applicants whose claims are not denied at the first two steps of the disability determination process, have their conditions compared with those described in the Listing of Impairments, a document promulgated in regulations by SSA. The Listing of Impairments includes over 300 medical conditions--described in terms of specific signs, symptoms, and laboratory findings--which are disabling on medical grounds alone. If the claimant's condition is determined to meet or equal in severity the medical conditions included in the Listing of Impairments, then the claimant is determined to be unable to perform substantial gainful activity, and is awarded benefits. Those whose conditions fall short of the severity described in the Listing of Impairments are evaluated further, as described in Step Four.
Step Four: Does the claimant have the functional capacity to do past relevant work?
For claimants whose impairments do not meet or equal the severity level described in the Listing of Impairments, the DDS team then determines whether claimants are functionally able to do their former jobs. At this step, a claimant's residual functional capacity (RFC) is assessed. This assessment must take into account the claimant's alleged symptoms, especially pain. In this assessment process, a program medical consultant determines whether the claimant is capable of performing his or her past work. If so, the applicant is found not disabled.
Step Five: Can the claimant do other types of work?
If the claimant is determined not able to do his or her former job, then a determination is made whether there are other jobs in the national economy that he or she could perform. At this point, the applicant's disability is assessed in conjunction with her or her age, education, and vocational experience. A determination is made whether the applicant's skills can be transferred to other types of work in the national economy. Persons who are determined unable to perform their previous jobs, or other work in the national economy, or determined disabled, and are awarded DI benefits.
Although the disability determination process has been structured to apply reliable, consistent, and uniform criteria in determining whether someone is or is not capable of working. it is widely recognized that it is extremely difficult to develop criteria for determining the ability to work that can be uniformly applied to every individual case. As stated in the 1988 Report of the Disability Advisory Council:
"One reason that claims for disability benefits are so difficult to adjudicate is that medical conditions are not the sole cause of work incapacity. Work incapacity is not the direct result of physical or mental impairments alone, but rather is attributable to a variety of additional factors--psychological, economic, environmental and, perhaps most importantly, motivational. Incontrovertible evidence for this can be found in the many people with severe disabilities who work and never apply for benefits under the DI or SSI programs."
2.5.2 Eligibility of dependents and other disabled persons
Certain dependents of disabled workers are eligible for auxiliary benefits under the DI program. Spouses are eligible for benefits if: (1) they are 60 years of age or older, or (2) they have one or more entitled children under age 16 in their care. A divorced spouse is eligible if he or she is 62 years of age or older and was married to the disabled worker for at least 10 years. Unmarried dependent children of disabled workers who are under age 18 are also eligible for monthly benefits. In June 1989, there were 276,000 dependent spouses and 972,000 dependent children of disabled workers receiving auxiliary benefits under the DI program.
In addition to disabled workers and their dependents, certain disabled persons who would otherwise not be eligible for OASDI benefits are made eligible as a result of their disability. These persons include:
Disabled widows and widowers between the ages of 50 and 59. Generally, surviving spouses of deceased Social Security beneficiaries are not eligible for survivor benefits until they reach age 60. Surviving spouses who are determined disabled are eligible for survivor benefits beginning at age 50.
Adult disabled children. Generally, childhood benefits cease once a dependent child reaches age 18. However, disabled children of retired, disabled or deceased Social Security beneficiaries, who were disabled prior to age 22, are eligible for OASDI benefits as long as they remain disabled, even though they themselves have not achieved insured status. The majority of these persons are persons with developmental disabilities such as mental retardation, autism, and cerebral palsy. Cash benefits for these persons may begin at age 18, without a five-month waiting period, and may continue as long as the person remains a dependent adult.
It is important to note that monthly cash benefits for disabled widows and widowers, and for adult disabled children are paid either from the OASI trust fund or the DI trust fund depending upon the status of the insured beneficiary to whom the adult disabled child or widow(er) is related. For example, benefits for adult disabled children of disabled workers are paid from the DI trust fund while benefits for adult disabled children of OASI beneficiaries are paid from the OASI trust fund.
2.5.3 Continuing Disability Reviews
The Social Security Act requires that every person receiving DI benefits undergo a periodic review of their continuing eligibility for benefits. The process for conducting a continuing disability review is somewhat different from the process for determining initial eligibility. In determining continuing eligibility for benefits, a medical improvement review standard is used. The medical improvement review standard was adopted in the 1984 amendments to the Social Security Act. Under this standard, once an individual is determined eligible for disability benefits, substantial evidence must show that medical improvement related to his or her ability to work has occurred and that the person is able to work before disability benefits can be terminated.
The frequency of continuing disability reviews depends upon the type of case. At the initial eligibility process, some persons are determined eligible for disability benefits but are identified as having a disability which is likely to improve. These cases are generally scheduled to be reviewed within 18 months of the initial determination. Cases which are more severe, but in which disability is not expected to be permanent, are scheduled for review every 3 years. Cases in which the disability is expected to be permanent are reviewed every 5 to 7 years.
Like the initial eligibility determination process, the continuing review process involves an orderly sequential evaluation process to determine whether an individual is still disabled and incapable of work. The continuing review process is similar to the initial determination process, but includes additional steps to determine if medical improvement has occurred, and if so, if that improvement has reached the point where the individual is now capable of performing his or her former job or other jobs in the national economy. If the individual is assessed as capable of doing work, then the DDS team will determine that the beneficiary's disability has ceased, and benefits are discontinued.
2.5.4 Termination of DI benefits
Cash benefits to disabled workers are generally terminated for one of two reasons: (1) the worker is determined by a continuing disability review to be no longer disabled; or (2) the worker reaches age 65.
A continuing disability review may find that a DI beneficiary is no longer disabled if either there has been a medical improvement in his or her condition that permits the beneficiary to participate in substantial gainful activity, or the beneficiary is participating in substantial gainful activity, regardless of his or her continuing medical condition. However, as an incentive to DI beneficiaries to attempt work without fear of losing benefits, the program provides for a nine- month "trial work period." Under this provision, most DI beneficiaries may work and earn any amount of income for up to 9 months without losing their DI cash benefits. A month of trial work is defined as any month in which earnings are more than $75; earnings of less than $75 per month are not counted as a trial work period.2 After an individual completes the 9-month trial work period, work performed during the trial work period can be considered in determining the beneficiary's ability to engage in substantial gainful activity (SGA) if the individual has worked for one or more month at the SGA level.
The trial work period only applies to beneficiaries who work while still disabled, not to beneficiaries who have medically recovered from their disabilities. Thus, DI benefits can be terminated at any time that a determination is made that a medical improvement in the beneficiary's condition permits him or her to participate in work, regardless of whether the beneficiary is in a trial work period or not.
Once a disabled worker reaches the age of 65, a disabled worker is automatically transferred to the OASI program, and he or she starts receiving retirement benefits. At transition to the OASI program, monthly benefits generally remain the same.
DI benefits can be withheld at any time from disabled workers who refuse to participate, without good cause, in a vocational rehabilitation program to which he or she has been referred.
2.6 Benefit Levels
Monthly benefits paid to disabled workers are related to the past earnings of the insured worker. Disability benefits are computed in much the same manner as benefits paid to retired workers, and are based on the insured worker's Primary Insurance Amount (PIA). The PIA is based on an individual's taxable earnings averaged over his or her working lifetime. In June 1989, the average monthly benefit paid to disabled workers was $530.
Benefits to dependents and survivors of disabled workers are paid on the same basis as benefits paid to families of retired workers. Dependents of disabled workers receive benefits equal to 50% of the disabled worker's PIA. Disabled widows or widowers receive benefits equal to 71.5% of the insured worker's PIA. In June 1989, the average monthly benefit paid to dependent spouses was $137; the average benefit paid to dependent children was $151.
There is a limit on the total amount of monthly benefits that may be paid to a disabled worker and his or her dependents. The purpose of this provision is to ensure that no family is considerably better off financially after a worker becomes disabled than it was while he or she was working. The limitation of family benefits for disabled-worker families is somewhat more stringent than for retired-worker families.
2.7 Cost of Living Adjustments (COLAs)
Under current law, DI benefits, like all Social Security and Federal SSI benefits, are automatically increased annually to adjust for increases in the cost of living. Cost of Living Adjustments (COLAs) are based on increases in the cost of living as measured by the Bureau of Labor Statistics' Consumer Price Index (CPI). A COLA is provided in any year in which there is a measurable (0.1 percent) increase in consumer prices. If there is a year of price deflation and no COLA is provided, then a 2-year change in the CPI of at least 0.1 percent is needed before a COLA is provided.
The annual COLA is reflected in DI checks mailed in January of each year. The COLA is based on the CPI increase from the third quarter of the base year through the third quarter of the year in which the benefit increase becomes effective. Thus, the COLA provided in January 1989 DI checks reflected changes in the CPI between the third quarter of 1987 and the third quarter of 1988. In addition, the COLA is based on the CPI in which the housing component is measured on a rental equivalence basis.
If the assets of the combined OASI and DI trust funds fall below a certain reserve ratio (20 percent) and wages increase at a rate lower than inflation, the automatic benefit increase will be based on wage growth rather than inflation.
2.8 Recent Program History and Legislative Changes
The most important legislative changes to the DI program in recent years occurred under the Social Security Disability Benefits Reforms Act of 1984 (Public Law 98-460). This Act was enacted largely out of Congressional concerns over the implementation of continuing disability reviews in the early 1980s which led to the termination of benefits for thousands of DI beneficiaries, and the perceived need to assure more accurate, consistent, and uniform disability decisions in the DI program. Among the provisions of the Act were:
Medical improvement standard
The Act established a medical improvement standard which specified the conditions under which disability benefits can be terminated and the evidence required in making a determination that a beneficiary is no longer disabled.
Evaluation of pain
The Act required the Secretary of HHS to conduct a study concerning the evaluation of subjective pain in disability determinations. This study was completed in 1986 and basically supported the existing treatment of subjective pain in the DDS process.
Moratorium on mental impairment reviews
A moratorium was placed on all continuing disability reviews of cases involving mental impairment until the Listing of Impairments was revised and updated to reflect current professional knowledge on the diagnosis, treatment, and evaluation of mental impairments. The revised criteria were published in 1985.
Continuation of benefits during appeals
The Act mandated the continuation of DI benefits for beneficiaries whose benefits are terminated in accordance with a finding by the continuing disability review process that the beneficiary is no longer disabled, if the beneficiary elects to appeal the decision, and at the election of the beneficiary. If the administrative law judge (ALJ) affirms the decision of the continuing disability review, then the benefits paid during the appeal process must be repaid.
The Disability Benefits Reform Act of 1984 also made various other changes to the manner in which disability determinations are initially made and continuously reviewed, and also included provisions requiring greater public dissemination of SSA procedures for conducting disability determinations.
More recently, the Budget Reconciliation Act of 1987 (Public Law 100-203) lengthened the extended period of eligibility (from 15 months to 36 months) during which a disabled beneficiary can return to work and not lose their entitlement to benefits. If the disabled beneficiary stops work during this period, then DI benefits are immediately reinstated without the beneficiary having to file a new application (at least until the next continuing disability review decision is made).
2.9 Program Interactions
2.9.1 Offsets for other public disability benefits
When a disabled worker is receiving disability benefits from more than one Federal, State or local government program, including worker's compensation, DI benefits to the worker and his family are reduced by the amount, if any, that the combined benefits from all sources exceed 80 percent of his average current earnings before he became disabled. Needs-tested benefits program (such as SSI), Veteran's Administration disability benefits, and benefits based on public employment covered by Social Security are not subject to this provision. Neither does the offset provision apply if a State worker's compensation law provides for an offset against Social Security disability benefits, provided that the State law was enacted prior to 1981.
There is no offset of DI benefits for workers who also receive private disability insurance payments. Conversely, however, most private disability insurance programs are structured to adjust benefits in accordance with the level of benefits received from DI and other public programs.
2.9.2 Eligibility for Medicare
Disabled workers receiving DI benefits are eligible for coverage under the Hospital Insurance (HI) component of Medicare, also referred to as Medicare Part A. However, there is a 24-month waiting period between the month in which the disabled worker becomes entitled to DI benefits and the month in which the worker becomes eligible for Medicare. Since there is a 5-month waiting period for DI benefits, an individual may have to wait 29 months from the onset of their disability until Medicare coverage begins. Once a disabled beneficiary becomes eligible for the HI (Part A) component of Medicare, he or she is also eligible for the Supplementary Medical Insurance (SMI) program, or Part B, which covers physician and ancillary services. As with other Medicare beneficiaries, participation in Medicare Part B is voluntary, and requires the payment of a Part B premium, which in 1989 is set at $31.90 per month.
If a disabled worker loses entitlement to DI benefits because his or her impairment ceases, Medicare eligibility is generally terminated at the end of the month following the month in which DI benefits are terminated. There are provisions in the law which extend Medicare benefits to disabled workers who attempt to return to work under a "trial work" program or whose DI benefits cease due to earnings which exceed the SGA level. For these beneficiaries, Medicare coverage is extended for not less than 39 months after the end of the trial work period, and possibly longer. It is often argued that the threatened loss of health insurance coverage is more of a work disincentive for disabled workers than the threatened loss of cash benefits, since health care expenses are more unpredictable. For those beneficiaries who have completed the two-year waiting period and who come back onto the DI rolls after a period of work, there is no additional two-year waiting period for Medicare coverage.
Disabled widows and widowers and adult disabled children who receive either DI or OASI benefits are also eligible for Medicare coverage after the mandatory two-year waiting period.
Persons who receive DI benefits as dependents or survivors of disabled workers (who are not themselves disabled) are not eligible for Medicare coverage. Thus, a disabled worker who can no longer work may receive health insurance coverage from Medicare after a two-year waiting period, but may have no health insurance coverage for his or her dependent family members.
2.10 Special Program Issues
2.10.1 Variation in allowance rates across States
State DDSs are required to apply uniform regulatory criteria in making disability determinations. However, data show wide variation in allowance rates for new DI claims across the 50 States and the District of Columbia. In FY 1986, the national average allowance rate was 39 percent for initial determinations, but this rate varied from 28.3 percent to 52.6 percent across States. While these variations in allowance rates suggest that States are not making disability determinations in a uniform manner, it is also known that differences in allowance rates are also related, in some part, to differences in filing rates. For example, the number of applications for DI benefits is related to local economic and workforce conditions. Areas of high unemployment, with high numbers of poorly educated and low-skilled workers, have more applications for DI benefits per thousand population than areas where economic conditions are better. Workers with marginal impairments obviously have more opportunities to find other kinds of work in areas where workers are in high demand than in areas where there is greater competition for jobs. In addition, some States require applicants for welfare benefits (e.g. AFDC benefits) to first apply for DI or SSI disability benefits.
Nonetheless, developing a disability determination system that exhibits nationwide uniformity in the application of disability criteria is an ongoing objective of the Social Security Administration. A number of initiatives have been implemented in recent years to increase uniformity in the review process. Many other initiatives have been recommended, but because the disability determination process always retains a subjective component, it is difficult to achieve national uniformity. One recommendation for achieving increased uniformity has been Federalize the review process entirely, so that Federal, rather than State, agencies conduct disability reviews. However, there are legitimate arguments for maintaining a decentralized system, including the desire to link the disability determination process with State vocational rehabilitation programs.
2.10.2 Disability determinations appeals process
As previously discussed, SSA has established a multi-layered system for handling appeals of denied disability claims and terminations of DI benefits. There is still some controversy concerning the equity and uniformity of this system. Although all levels of the disability determination system are required to apply the same criteria and standards in making determinations, it does not appear that all levels of the system apply the same criteria uniformly. For example, of denied initial applications which were appealed to the administrative law judge level in 1987, 57% of denials were reversed by ALJ dispositions.3 Of terminated continuing disability reviews, 51% of appealed decisions were reversed.
Exhibit 2-1 shows the number of cases allowed at appeal at various levels of appeal for both initial applications and continuing disability reviews in 1988. For initial applications, 36% were initially allowed, while 64% were denied. However, after all levels of appeal had been exhausted, some 49% of initial applications were eventually allowed. For continuing disability reviews, 88% of current cases were continued, and 12% terminated. Subsequent appeals of terminated cases eventually led to a reversal of 21% of cases initially terminated. In all, after all levels of appeal are considered, about 9% of DI beneficiaries undergoing a continuing disability review are eventually terminated. In 1988, DDSs conducted 290,942 continuing disability reviews, about 8.3 percent of the active disability caseload.
2.10.3 Vocational rehabilitation of disabled workers
The Social Security Administration also administers a program which reimburses States for 100% of the cost for reasonable and necessary vocational services for DI beneficiaries if the services result in savings and is successful. A successful rehabilitation is defined by law as the completion o a continuous 9-month period of employment at the SGA level.
| EXHIBIT 2-1: Disability Determinations and Appeals, FY 1988 |
 |
| SOURCE: U.S. House of Representatives, Background Material and Data on Programs Within the Jurisdication of the Committee on Ways and Means, 1989 Edition. |
The present VR reimbursement program was enacted as part of the Omnibus Budget Reconciliation Act of 1981. This legislation changed SSA's VR program from a grant program to one in which States VR agencies are reimbursed only for successful rehabilitations. Under the old grant program, known as the Beneficiary Rehabilitation Program, SSA provided State VR agencies with a lump sum advance. Several studies questioned the cost effectiveness of this program, and in 1981 it was replaced with the current program. In 1988, SSA reimbursed State VR agencies $16 million from the Disability Trust Fund for the costs of successfully rehabilitation DI beneficiaries.
Under guidelines developed by SSA, State DDS workers refer persons awarded disability benefits to State Vocational Rehabilitation (VR) Agencies. Under these guidelines, only those beneficiaries who are considered good candidates for rehabilitation, and who could potentially benefit from State VR services, are referred. If referred, a DI beneficiary may lose his or her benefits for refusing rehabilitation services without good cause.
A recent GAO study of the rehabilitation of DI beneficiaries found that State VR programs have very little effect on rehabilitating disabled workers in the DI program.4 In a ten-State study, GAO found that about 12 percent of DI beneficiaries were evaluated by State VR agencies. Only 1 percent of the beneficiaries had been removed from the DI rolls after three years as a result of working, and only about one-third of these had been served by a State VR agency. Thus, only about 3 DI beneficiaries in 1,000 had returned to work and been removed from the DI rolls as a result of State VR efforts. In the study, State VR counselors indicated that many DI beneficiaries do not participate in rehabilitation programs because of their fear of losing cash benefits and Medicare coverage. Many felt that more disabled workers would try to work if they could continue to keep their Medicare coverage and if their cash benefits were continued on a sliding scale basis.
2.10.4 Work incentives in the DI program
Less than 1 percent of disabled workers leave the DI rolls because they return to work. In recognition of the fact that beneficiaries will be more likely to return to work if their cash benefits and health insurance coverage are not jeopardized by their work efforts, a number of work incentive provisions have been built into the DI program. These provisions, as previously discussed, include:
- Entitlement to DI benefits is never terminated during the trial work period due to earnings as long as the person remains disabled (does not medically recover), regardless of the amount of earnings;
- The extended period of eligibility (EPE) permits the prompt reinstatement of DI benefits to persons who stop performing SGA within the 36 consecutive-month period immediately following the trial work period, provided they remain disabled. During the extended period of eligibility, a new application or a new disability determination is not required before DI benefits are reinstated;
- There is no 5-month waiting period for DI benefits for a worker who becomes reentitled to benefits within 5 years of a prior period of disability.
- For disabled workers who return to work, certain impairment-related work expenses can be deducted in determining whether the worker is engaging in substantial gainful activity;
- For persons who medically recover while participating in a State VR program, cash benefits are continued until their rehabilitation program is completed; and
- Medicare benefits are extended for beneficiaries who return to work, plus Medicare coverage is automatically reinstated for beneficiaries who return to the DI rolls after a period of work, without a 24-month waiting period.
Despite these work incentives, many believe that the program does not go far enough in encouraging DI beneficiaries to return to work. For example, the Disability Advisory Council noted that the SGA level has not increased since 1980, and recommended that it be adjusted annually to reflect average wage growth. The Council also recommended that the monthly earnings amount that counts toward the trial work period be raised from the current level of $75. The Council also noted that adequate evaluations of the various work incentives in the DI program, and of possible alternative incentives, have not been conducted.
2.11 Program Data
2.11.1 Current DI recipients expenditures and benefit levels
Exhibit 2-2 presents the number of disabled workers and dependents receiving DI benefits in June 1989, the total amount of cash benefits paid, and the average benefit amount for each beneficiary. In January 1989, there were approximately 2.8 million disabled workers receiving $1.5 billion in cash benefits, and 1.2 million dependents of disabled workers receiving $184 million in cash benefits.
| EXHIBIT 2-2: Beneficiaries, Payments and Average Benefits in the DI Program: January 1989 | |||
| Beneficiaries | Total Payments (in thousands) | Average Benefit | |
| Disabled Workers | 2,857,231 | $1,514,209 | $529.96 |
| Wives and Husbands | 276,105 | 37,938 | 134.40 |
| Children | 971,930 | 146,663 | 150.90 |
| 4,105,266 | $1,698,809 | ||
| SOURCE: Social Security Bulletin, August 1989. Children include about 36,000 children over age 18 eligible for benefits as adult disabled children. | |||
2.11.2 Recent Trends in the DI Program
As shown in Exhibit 2-3, the number of disabled workers receiving DI benefits declined by 10.2% between 1980 and 1983, from about 2.9 million to about 2.6 million. Since 1983, the number of disabled workers has again increased to about 2.9 million beneficiaries in June 1989.
The number of dependents of disabled workers receiving DI benefits has declined from about 1.8 million in 1980 to about 1.2 million in June 1989.
| EXHIBIT 2-3: Disabled Workers and Dependents Receiving Monthly SSDI Cash Benefits: 1980-1988 | ||
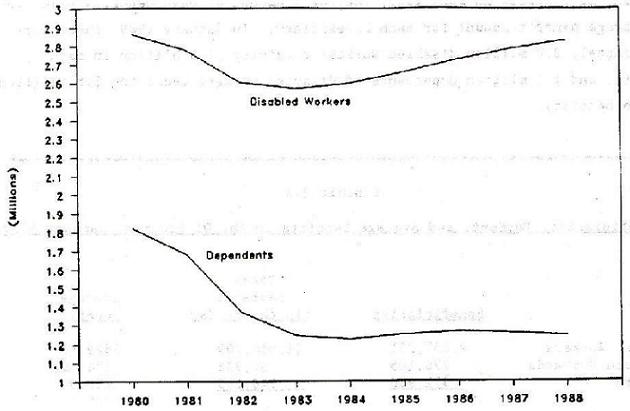 | ||
| Disabled Workers | Dependents | |
| 1980 | 2,861,253 | 1,820,919 |
| 1981 | 2,776,519 | 1,679,755 |
| 1982 | 2,603,713 | 1,369,752 |
| 1983 | 2,568,966 | 1,243,964 |
| 1984 | 2,596,535 | 1,225,269 |
| 1985 | 2,656,500 | 1,250,669 |
| 1986 | 2,727,386 | 1,265,893 |
| 1987 | 2,785,885 | 1,258,839 |
| 1988 | 2,830,284 | 1,244,016 |
| SOURCE: Social Security Bulletin, Annual Statistical Supplement, 1988. Data are monthly beneficiaries in December of each year. | ||
The application rate for DI benefits (number of applications per 1,000 insured workers) has been gradually declining, while the percentage of applications awarded has been increasing gradually. This may reflect an increased awareness among potential applicants of the likelihood of receiving an award. In 1988, 1,017,900 application were filed and 409,490 new awards approved, for an overall approval rate of 40 percent. The number of awards per 1,000 insured workers declined from 4.0 in 1980 to 3.0 in 1983, but then increased to 3.6 in 1988.
2.11.3 Characteristics of DI Beneficiaries
Approximately two-thirds of disabled workers are men. However, the proportion of female beneficiaries has been increasing gradually, reflecting the growing participation of women in the workforce.
As shown in Exhibit 2-4, the majority of disabled worker beneficiaries are between the ages of 55 and 64. However, the median age of disabled workers has been declining in recent years. In 1988, the median age of disabled workers was 52.4 years.
Mental, psychoneurotic and personality disorders are the major disabling condition of disabled workers granted new awards, accounting for 22 percent of all disabling conditions among new awards. This is twice the rate among new awards in 1982, when mental, psychoneurotic and personality disorders accounted for 11 percent of disabling conditions among new awards. Neoplasms (16 percent), diseases of the circulatory system (18 percent) and skeletal-muscular conditions (14 percent) accounted for almost half of disabling conditions among new awardees in 1988.
| EXHIBIT 2-4: SSDI Disabled Workers by Age and Sex | ||
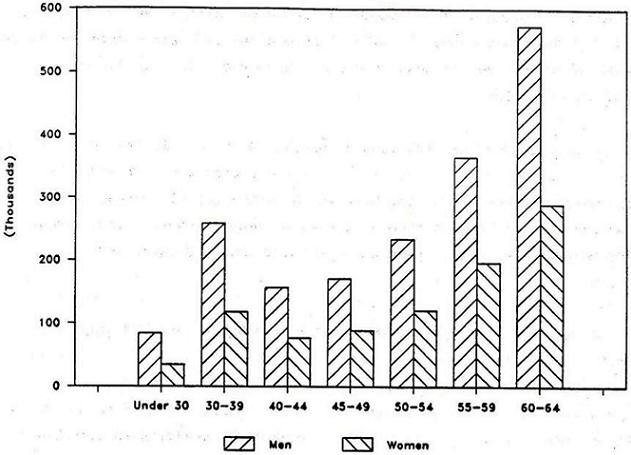 | ||
| Men | Women | |
| 1,845,600 | 928,600 | |
| Under 30 | 84,500 | 34,900 |
| 30-39 | 258,900 | 118,600 |
| 40-44 | 157,100 | 77,000 |
| 45-49 | 171,100 | 89,300 |
| 50-54 | 234,500 | 121,100 |
| 55-59 | 365,700 | 197,300 |
| 60-64 | 573,800 | 290,400 |
| SOURCE: Social Security Bulletin, Annual Statistical Supplement, 1988. Data are for December 1987 based on 1 percent sample. | ||
Additional data on the characteristics of disabled workers are available from the New Beneficiary Survey (NBS) conducted in 1982.5 The survey sample consisted of a nationally representative sample of persons who were newly awarded benefits between July 1980 and June 1981. With regard to financial status, DI beneficiaries who were married were significantly better off than unmarried beneficiaries. Overall, 66 percent of new DI beneficiaries were married, but this percentage differed greatly by sex. Among male beneficiaries, 74 percent were married, compared to only 49 percent of female beneficiaries. Median monthly household income for married men in 1982 was $1,230 and for married women, $1,360. This contrasted sharply with the average median household income for unmarried men, which was $490, and for unmarried women, which was $460.
The primary reason that families of married DI beneficiaries are better off financially than unmarried beneficiaries is the presence of earnings from the disabled worker's spouse. Social Security benefits (of all types, not just disabled workers benefits) accounted for 43 percent of total income for married disabled workers, but for 65 percent of total income for unmarried beneficiaries.
2.11.4 Adult disabled children and disabled-widows and widowers
In addition to disabled workers who receive cash benefits exclusively under the DI program, there were an additional 561,276 adult disabled children and 104,991 disabled widows and widowers receiving OASDI benefits in December 1987. Most of these persons receive their cash benefits from the OASI trust fund, not the DI trust fund, since they are eligible as children or spouses of retired or deceased beneficiaries. Over half of all adult disabled children, about 299,000, also received SSI benefits in 1987.
Adult disabled children are one of the fastest growing benefit populations in the Social Security program. The number of beneficiaries increased by 25% between 1980 and 1987, from 450,169 to 561,276 (Exhibit 2-5). Total cash benefits paid to adult disabled children in 1987 were just under $2.0 billion.
On the other hand, the number of disabled widows and widowers receiving OASDI benefits declined from 127,580 in 1980 to 104,991 in 1987. Total cash payments to disabled widows and widowers in 1987 were approximately $415 million.
| EXHIBIT 2-5: Adult Disabled Children Receiving Monthly SSDI Cash Benefits: 1980-1987 | |
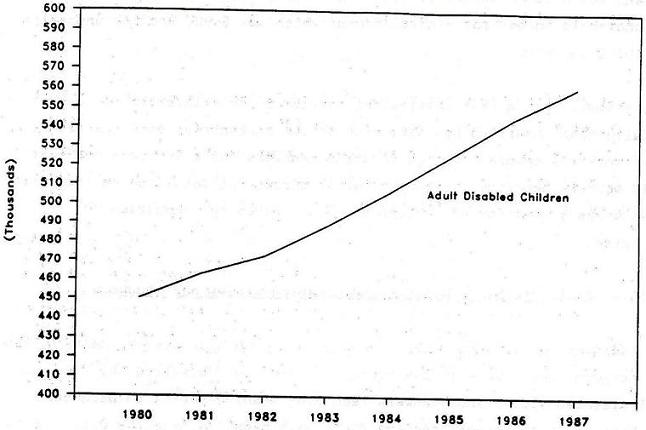 | |
| Adult Disabled Children | |
| 1980 | 450,169 |
| 1981 | 463,021 |
| 1982 | 472,408 |
| 1983 | 488,372 |
| 1984 | 506,373 |
| 1985 | 525,842 |
| 1986 | 545,387 |
| 1987 | 561,276 |
| SOURCE: Social Security Bulletin, Annual Statistical Supplement, 1988. Data are monthly beneficiaries in December of each year. | |
2.11.5 Total outlays of the DI trust fund
Total outlays from the DI trust fund were $22.5 billion in 1988. This included $21.7 billion in benefit payments to disabled workers and their dependents, approximately $16 million in payments for the vocational rehabilitation of DI beneficiaries, and $737 million in administrative expenses.
Total outlays from the DI trust fund are projected to increase at annual compound rate of 6.6 percent between 1988 and 1994, rising to $32.8 billion. Like the OASI trust fund, the DI trust fund is expected to generate significant surpluses through the first part of the 21st century, after which outlays will start to exceed surpluses indefinitely.
CHAPTER 3. THE SUPPLEMENTAL SECURITY INCOME (SSI) PROGRAM
3.1 Overview and Purpose
The Supplemental Security Income (SSI) program provides monthly cash benefits to aged, blind and disabled persons who meet financial criteria. In contrast to the Social Security program (OASDI), SSI applicants do not have to achieve insured status to be eligible for benefits (i.e., they do not have to have worked) but they do have to be poor. The purpose of the program is to provide needy aged, blind and disabled persons with financial assistance for basic living needs. At their option, States may supplement Federal SSI benefits through State Supplementation Programs (SSP). In FY 1989, approximately 4.5 million persons, including over 3.1 million blind and disabled persons, received cash assistance under the SSI/SSP program.
3.2 Authorization, History and Funding
The SSI program was authorized under Title XVI of the Social Security Act in the 1972 amendments (Public Law 92-603) to the Act, and was first implemented in 1974. The SSI program replaced a previous program of Federal grants to States for old-age assistance, aid to the blind, and aid to the permanently and totally disabled. Enactment of the SSI program served to establish uniform, nationwide eligibility requirements for Federal SSI benefits across all States, while leaving States the flexibility to supplement Federal benefits at their discretion. Enactment of SSI also extended Federal cash assistance to disabled children under the age of 18 for the first time. Although the SSI program has undergone numerous refinements and modifications since its enactment, the basic structure of the program has not changed since 1974.
Unlike the OASDI program, SSI is not financed through a self-contained financing structure or trust fund. Payments to SSI recipients are drawn from Federal tax revenues. Estimated Federal outlays under the SSI program were about $11.8 billion in FY 1989, of which 77 percent, or $9.1 billion, went to disabled SSI recipients.
3.3 Definition of Disability
The definition of disability employed in determining the eligibility of persons under the age of 65 for SSI benefits is exactly the same definition (and process) used in determining the eligibility of disabled workers for DI benefits: the inability to engage in any substantial gainful activity by reason of any medically determinable physical or mental impairment which can be expected to result in death or has lasted or can be expected to last for a continuous period of not less than 12 months. A more detailed explanation of this definition, including how the definition is operationalized in determining the eligibility of program applicants, was provided in Chapter 2 of this report.
However, the SSI program covers a beneficiary population that is generally not covered in the SSDI program: disabled children. The definition of disability initially developed for the SSDI program, and then adopted for the SSI program, focuses on determining whether an applicant is incapable of work. Consequently, the disability determination process has had to be modified in determining the eligibility of SSI children. The process attempts to assess whether child applicants have impairments which are of comparable severity to that of adults who are determined disabled. Generally, this is done by assessing the impact of a child's impairment on expected age-related activities such as participation in school, in play and in other normal daily activities. Like the process for determining disability among adults, the process for determining the eligibility of disabled children is an imprecise one, and remains controversial.
3.4 Administrative Structure
The administration of SSI benefits for disabled persons is conducted in much the same manner as the administration of SSDI benefits. Social Security Administration staff determine whether program applicants meet the financial criteria for SSI benefits, while State Disability Determination Services (DDSs) determine whether applicants meet the disability criteria. For those applicants who are denied benefits on the basis of not meeting the disability requirements, a multi-layered administrative structure has been established to handle appeals. This structure, as well as the prevalence and outcomes of appealed claims, is also discussed in some detail in Chapter 2.
A unique feature of the SSI program, however, is the State supplementation of Federal benefits. Most States elect to raise the benefit levels provided by the Federal SSI program with additional benefits provided through State general revenues. Since benefits provided through State supplementation programs are financed with 100% State funds, States have wide discretion over who is eligible to receive supplemental benefits, and how much. All but seven States currently provide some supplemental benefits to the Federal SSI program.
In addition to deciding whether to supplement Federal SSI benefits, States can choose to administer State supplementation payments directly, or to contract with the Social Security Administration to administer their supplementation payments. Under Federal administration, the State is responsible for program benefit costs only; the Federal government assumes responsibility for administrative costs. Despite this fact, of the 43 States which supplement Federal SSI benefits, only 17 and the District of Columbia have opted for Federal administration of State supplementation payments. In States where State supplementation payments are Federally-administered, the amount of the supplementary payment is added to the monthly SSI payment and the total benefit is paid in one check. When a State elects to administer State supplementation payments directly, the applicant must make a separate application at a State welfare office, and, if eligible, receives two separate checks monthly.
3.5 Eligibility-for Benefits
To qualify for SSI payments, disabled persons under age 65 must: (1) be determined disabled according to criteria established by the Social Security Administration; and (2) be determined financially needy in regard to both income and assets. The disability determination process was discussed in some detail in Chapter 2 and will not be discussed further in this chapter.6 Unlike the SSDI, the determination of financial need is unique to the SSI program, however, and involves the application of both income criteria and asset criteria.
3.5.1 Federal SSI benefit standards
In 1989, the Federal SSI benefit standard for an individual was $368 per month and $553 for a couple. In determining eligibility for SSI benefits, an individual's or couple's "countable" income is compared to these benefit standards. If an individual's or couple's countable income exceeds the Federal SSI benefit standard, then they are not eligible for SSI benefits. If countable income falls below the benefit standard, then the SSI payment amount is set equal to the difference between the Federal benefit standard and countable income (assuming the applicant also meets the asset criteria). For example, if a disabled individual's countable income in 1989 is $300, then the SSI payment amount would be $68 (the Federal benefit standard of $368 minus countable income of $300). SSI benefit standards are adjusted each year to reflect increases in the cost of living. The increase is computed in the same manner in which cost of living adjustments (COLAs) are computed for all Social Security beneficiaries (see Section 2.7).
3.5.2 Income disregards
In computing countable income for SSI benefits, certain income is "disregarded." Thus, certain applicants with gross incomes above the Federal benefit standard may end up having countable incomes below the standard, and thereby qualify for benefits. Income disregards include:
-
The first $20 of monthly income from any source, earned or unearned.
-
In addition, the first $65 of monthly earned income.
-
In addition, one-half of all remaining earnings.
-
Impairment-related work expenses for the disabled. For example, if a disabled person must use public transportation to get to work because he or she cannot drive, then those expenses would be deducted from his or her gross income.
-
For disabled and blind individuals, the cost of an approved plan for achieving self-support (PASS) is also disregarded. The plan may involve setting aside income (or resources) to achieve a work goal such as education, vocational training or starting a business. The individual must have a feasible work goal, a specific savings plan, and must provide for a clearly identifiable accounting for the funds which are set aside. Any person may help a disabled SSI applicant with developing a PASS and any SSI beneficiary can have a PASS. A PASS is often needed when a disabled SSI recipient begins to work, and earnings begin to rise, in order to remain eligible for SSI benefits.
-
Generally, any financial assistance paid by State or local governments based on financial need is disregarded. For example, the value of Food Stamps, housing subsidies, or low-income energy assistance is not included as countable income.
-
Any in-kind support and maintenance provided by a private nonprofit organization is disregarded, as long as the State determines that the assistance is provided on the basis of need. For example, the value of in-kind support provided to persons with mental retardation residing in group homes operated by non-profit agencies is not included as countable income.
3.5.3 Reduced benefit standard for in-kind support and maintenance
When an SSI applicant or recipient is receiving in-kind support and maintenance from another person, then the Federal SSI benefit standard is reduced by one-third. Since the purpose of the SSI program is to provide financial assistance with basic living needs (food, clothing, shelter), this assistance is reduced when other sources of assistance are available. For example, if a 33-year-old woman with chronic mental illness is living in her sister's household, and does not contribute to room and board costs, then the maximum SSI payment she may receive is two-thirds the standard benefit level. In 1989, instead of receiving $368 per month from SSI (assuming she has no other income), she would receive $245.34.
Similarly, when an SSI recipient receives in-kind support from other persons, even though they may not live in the same household, then the recipient may also be subject to the one-third reduction rule. For example, if a disabled man lives in his own apartment, but his son pays his rent, then his SSI benefit standard is reduced by one-third. In no case can the SSI benefit be reduced by more than one-third, plus $20. The benefit may be reduced by less than one-third if the SSI applicant/recipient can prove that the actual value of in-kind support received is less one-third the Federal benefit standard. Benefits are not reduced for other types of in-kind support, such as gifts, transportation, medical expenses, etc. Of the approximately 3 million disabled SSI beneficiaries receiving payments in January 1989, about 5.8% received reduced benefits under this "one-third reduction rule" because they lived in another person's household or received in-kind support from other persons.
3.5.4 Resource Standards
In addition to income criteria, financial need under SSI is also determined by resource criteria. In 1989, SSI recipients were required to hold countable assets of less than $2,000, or in the case of a couple, less than $3,000. Persons with countable assets in excess of these limits are not eligible for SSI benefits, regardless of income. Neither is there any provision for reducing benefit levels by the amount by which applicants exceed the resource standards. If an individual has $2,001 in countable assets, he or she simply is not eligible.
As with income, certain resources are not counted when determining whether an applicant qualifies for SSI. These exemptions include:
- A personal residence of any value;
- up to $2,000 equity value in household goods and personal effects;
- the first $4,500 of the current market wholesale value of a car, but 100% of the market value of any car used for medical treatment or employment or which has been modified for use by a handicapped person;
- Any assets or property essential to the self-support of disabled persons; and
- Cash value of life insurance policies with face values of $1,500 or less, or up to $1,500 in separately identifiable funds for burial expenses;
3.5.5 Deeming of Income and Resources
In the case of a disabled SSI applicant who is married, or in the case of a disabled child applicant, the income and resources of ineligible spouses and parents are taken into account in determining the eligibility of the applicant. This process is called "deeming." Income and resources from ineligible spouses and parents are deemed available to the applicant because it is reasonable to expect spouses and parents to help in meeting an applicant's basic living needs. The rules for deeming income and resources from spouse to spouse and parent to child can get quite complicated, and this section will only provide a general discussion.
In considering the amount of income available to an applicant from an ineligible spouse, all of the income exclusions which are applied to the applicant are also applied to the ineligible spouse. Deductions from income are also allowed for each dependent child living in the household. Once these income deductions and exclusions are applied, the remaining income of the ineligible spouse is combined with the income of the eligible spouse and applied to the Federal SSI benefit standard for a couple. Exhibit 3-1 provides an example of how the deeming of income from spouse to spouse would work in the SSI program.
| EXHIBIT 3-1: Deeming of Income from Spouse to Spouse in Determining Eligibility for SSI Benefits |
| Marty, a disabled individual, lives with his ineligible spouse, Rebekah, and their two children, Jennifer and Kristin. Marty receives $230 in SSDI benefits monthly, and Rebekah has monthly earned income of $1,000. After application of the $20 income disregard, Martys countable income is $210 per month. In deeming income from Rebekah to Marty, allocations are first made for the needs of the two children. The allocation amount is one-half the Federal SSI benefit standard ($184 in 1989) for each child. This leaves Rebekah with with $632 in monthly earned income. From this amount, the $65 earned income disregard is first deducted, and then one-half of all remaining earnings, leaving Rebekah with a countable monthly income of $283.50. This amount is then combined with Martys countable income of $210 for a total countable income for the couple of $493.50. This amount is then subtracted from the Federal SSI benefit standard for a couple ($553 in 1989) to determine the monthly SSI payment amount for which they are eligible: $59.50. |
The deeming of income from parents to disabled children works somewhat differently, as shown in Exhibit 3-2. Deeming rules from parent to child are more liberal than deeming rules from spouse to spouse. As shown in the example provided, a disabled child living in a family of four with a total annual income of over $25,000 (about twice the Federal poverty level) can still qualify for SSI benefits (assuming SSI resource standards can also be met). Although the SSI benefit level may be modest, an important consideration is that receipt of SSI benefits automatically qualifies disabled children for health insurance coverage under Medicaid (except in a very few States). The benefits provided to families with disabled children under Medicaid may far exceed the cash assistance which they receive through SSI. Of the 289,000 blind and disabled children receiving SSI benefits in 1987, only about 8 percent receive reduced benefits due to the deeming of parental income. This suggests that the participation of non-poor families with disabled children in the SSI program is considerably less than it could be.
| EXHIBIT 3-2: Deeming of Income for Parents to a Disabled Child in Determining Eligibility for SSI Benefits |
| Ervin and Joyce Scott live with their severely disabled children, Joshua, and their non-disabled child, Brendan. Ervin and Joyce both work, and have a combined monthly income of $2,100. In deeming the income available to Joshua from his parents, an allocation is first made for Brendan of $184, half the Federal benefit standard. The $20 income disregard is then applied, plus the $65 earned income disregard, reducing available income from the parents to $1,831, which is then reduced by half, leaving $915.50. This amount is then reduced by the Federal benefit standard for a couple ($553 in 1989), leaving $362.50 deemed available to Joshua. Since Joshua is also entitled to his own $20 income disregard, his countable income is $342.50. His monthly SSI benefit payment is then applied the Federal SSI benefit standard ($368 in 1989) to determine his monthly benefit: $25.50. Note that while the deeming of parental income left Joshua with countable income sufficient to reduce his SSI benefit level to a relatively modest amount of $25.50 per month, his eligibility for SSI benefits automatically renders Joshua eligible for health insurance coverage under Medicaid in most States (see Chapter 10). Joshuas eligibility for Medicaid may help to reduce out-of-pocket health care expenses for the Scott family significantly. |
3.5.6 Residents of Public Institutions Not Eligible
Persons in public institutions that are not certified for Medicaid payments are not eligible for SSI benefits. These persons include residents of State mental hospitals, prisoners, and residents of publicly-operated nursing homes not certified for Medicaid reimbursement. Exceptions to this rule are persons in publicly-operated community residences serving no more than 16 persons (e.g. group homes for the chronically mentally ill which are publicly operated) and SSI recipients who are receiving temporary medical or psychiatric care (less than 3 months) in a public institution.
3.5.7 Termination of SSI benefits
SSI benefits for the disabled are generally terminated for one of two reasons: (1) the recipient is found by a continuing disability review to no longer be disabled; or (2) the recipient's countable income or assets, upon financial redetermination, are found to exceed SSI/SSP standards. Financial redeterminations are scheduled periodically, and the length of time between redeterminations depends upon the likelihood that the recipient's situation may change in a manner that affects his or her benefit amount. Recipients are also required to report any changes in their financial or household status that may affect their eligibility or payment amount.
Disabled SSI beneficiaries who have been medically determined to be drug addicts or alcoholics may also lose their eligibility for benefits if they refuse to undergo available appropriate treatment or if they fail to comply with the requirements of such treatment.
3.6 SSI Benefits
Persons eligible for SSI benefits receive monthly cash payments. The amount of the benefit depends primarily on two factors: (1) the beneficiary's countable income; and (2) the amount of State supplementation for which the beneficiary may qualify (see below). For persons with no countable income, the Federal SSI payment amount is equal to the Federal benefit standard. Federal SSI benefit standards are indexed to the Consumer Price Index (CPI) in the same manner as Social Security benefits. Federal SSI benefit standards since 1980 for individuals and couples living in their own household are presented in Exhibit 3-3. For individuals and couples with countable income greater than zero, the SSI payment amount equals the difference between countable income and the Federal benefit standard. For example, in 1989, if a disabled individual had countable income of $150 per month, the Federal benefit amount would equal $218 ($368 minus $150). The average Federal monthly benefit in January 1989 for a disabled individual, excluding State supplementation, was $257.83.
| EXHIBIT 3-3: Federal SSI Benefit Standards for Individuals and Couples Living Independently: 1980 to 1989 | ||
| Period | Individuals | Couples |
| July 1980-June 1981 | $238.00 | $357.00 |
| July 1981-June 1982 | 264.70 | 397.00 |
| July 1982-June 1983 | 284.30 | 426.40 |
| July 1983-December 1983 | 304.30 | 456.40 |
| January 1984-December 1984 | 314.00 | 472.00 |
| January 1985-December 1985 | 325.00 | 488.00 |
| January 1986-December 1986 | 336.00 | 504.00 |
| January 1987-December 1987 | 340.00 | 510.00 |
| January 1988-December 1988 | 354.00 | 532.00 |
| January 1989-December 1989 | 368.00 | 553.00 |
3.6.1 Reduced benefits in Medicaid-certified institutions
As previously discussed, SSI benefits are reduced by one-third when a recipient is receiving in-kind support and maintenance in another person's household. Similarly, SSI benefits are reduced when recipients are receiving care in Medicaid-certified institutions such as nursing homes. Because Medicaid payments to the providers of such institutions include the costs of providing room and board, a lower SSI benefit standard is used. This lower benefit standard, called the Personal Needs Allowance (PNA), is $30 per month, and is intended to take care of small personal expenses for institutionalized persons. Of the approximately 2.8 million SSI disabled recipients receiving benefits in December 1987, 4.6 percent received reduced benefits as recipients of Medicaid-covered institutional care. Many persons who receive SSI benefits prior to entering a nursing home lose their benefits upon nursing home admission because their countable income exceeds this lower benefit standard o $30 per month.
3.6.2 State Supplementation of Federal SSI benefits
States, at their option, may provide supplementary payments to Federal SSI benefits and all but seven States do so. The seven States which do not supplement SSI are Arkansas, Georgia, Kansas, Mississippi, Tennessee, Texas and West Virginia. With regard to eligibility criteria for State supplementation payments, States have broad flexibility with regard to establishing "groups" of persons eligible for supplementation (as long as they are aged, blind, or disabled). Two dimensions that are frequently used by States in establishing eligible groups are: (a) living arrangement; and (b) functioning level. For example, many States establish eligibility categories by different levels of residential care (i.e. various types of board-and-care homes) related to the amount of care and supervision provided by the residential care provider. Further, many States establish different payment levels related to individualized assessments of the recipient's functioning level and service needs.
States which elect to contract with the Social Security Administration to administer their supplementation programs must use Federal eligibility criteria in all aspects, except that they may establish additional income disregards. In other words, States with Federally-administered supplements must determine "countable income" in the same manner used in determining eligibility for Federal SSI benefits and they must also use Federal resource standards in the same way. States which administer their own supplementation programs do not have to follow Federal SSI rules, since the Federal government is not contributing to the cost of the program in any way. Eighteen States and the District of Columbia presently contract with SSA to administer their supplementation programs, while 25 States administer their own programs. Since 1974, six States have shifted from Federal to State administration.
A State supplementation program effectively raises the Federal SSI benefit standard to some higher level. In determining eligibility for benefits in Federally-administered programs, SSA first determines whether an applicant is eligible for Federal SSI benefits, and then whether the applicant may also be eligible for State supplementation. In cases in which the applicants countable income is higher than the Federal benefit standard, but lower than the State supplementation standard, the applicant may be eligible for State supplementation payments only. In State-administered supplementation programs, applicants must make separate applications for Federal and State benefits.
State supplementation standards vary both within States (e.g., by eligibility category) and across States. Although States retain flexibility with regard to the amount of State supplementation they elect to provide to specific groups of recipients, under Federal law, States are required to pass-through all Federal increases in SSI benefits to State supplementation recipients. In other words, States cannot offset a Federal cost-of-living increase in SSI benefits with a reduction in State supplementation payments. States are not required, however, to index their own supplementation benefit levels. Average State supplementation payments made to disabled individuals in December 1987, by State, is presented in Exhibit 3-4.
3.7 Recent Program History and Legislative Changes
The provisions of the Social Security Disability Benefits Reform Act of 1984 relating to the conduct of continuing disability reviews, as described in Chapter 2, apply to SSI disabled recipients as well as to recipients of SSDI. With regard to the SSI program, the most important legislative change made to the program affecting disabled persons in recent years has been the initial demonstration and then permanent enactment of the Section 1619 program. Under the section 1619 program, which was made permanent under the SSI Disability Amendments of 1986 (Public Law 99-643), disabled SSI recipients continue to receive benefits even though they are working at the substantial gainful activity (SGA)- level and as long as there is not a medical improvement in their disabling condition.
| EXHIBIT 3-4: Average Monthly State Supplementation Payment to Disabled SSI/SSP Recipients: December 1987 | |
| Federally-Administered State Supplementation | |
| California | $221.39 |
| Delaware | $134.81 |
| Dist. of Columbia | $24.37 |
| Hawaii | $38.91 |
| Iowa | $142.45 |
| Louisiana | $22.58 |
| Maine | $30.93 |
| Maryland | $30.56 |
| Massachusetts | $80.06 |
| Michigan | $50.94 |
| Montana | $79.01 |
| New Jersey | $49.89 |
| New York | $78.38 |
| Ohio | $29.80 |
| Pennsylvania | $40.01 |
| Rhode Island | $58.40 |
| Vermont | $75.54 |
| Washington | $33.63 |
| Wisconsin | $112.55 |
| State-Administered Supplementation | |
| Alabama | $59.82 |
| Alaska | NA |
| Arizona | $66.64 |
| Colorado | $57.97 |
| Connecticut | $249.53 |
| Florida | $93.01 |
| Idaho | $129.79 |
| Illinois | $50.77 |
| Indiana | NA |
| Kentucky | $130.05 |
| Maryland1 | |
| Minnesota | $161.36 |
| Missouri | $35.05 |
| Nebraska | $56.68 |
| New Hampshire | NA |
| New Mexico | NA |
| North Carolina | $332.90 |
| North Dakota | NA |
| Oklahoma | $55.74 |
| Oregon | $33.49 |
| South Carolina | $142.43 |
| South Dakota | NA |
| Utah | NA |
| Virginia | NA |
| Wyoming | $20.00 |
SOURCE: Social Security Bulletin, Annual Statistical Supplement, 1988.
| |
Prior to section 1619, disabled SSI recipients who returned to work could have their SSI benefits terminated on the basis of evidence that they were capable of working at the SGA level of $300 per month. This provision no longer applies to disabled SSI recipients who return to work.7 Under Section 1619, as the earnings of disabled SSI recipients increase, SSI cash benefits are gradually reduced under the income disregard formula until their countable earnings reach the SSI benefit standard, or what is known as the "breakeven point." Since SSI eligibility rules include provisions for earned income disregards (the first $65 of monthly earned income plus one-half of remaining earned income), these disregards are used in determining the continuing benefit levels of disabled recipients who return to work. In a State with no supplementation program, the "break even" point under the section 1619 program was $821 per month in 1989. People who receive special SSI benefits under this provision also retain their eligibility for Medicaid benefits, and can even retain Medicaid eligibility once their income exceeds the "break even" point under other special program provisions. States have the option of using a similar methodology in determining continuing eligibility for supplementation payments of section 1619 participants.
Another recent change in the SSI program was an increase in resource standards. From 1974, when SSI was first implemented, and 1985, the SSI resource standard stayed at $1,500 per month for an individual and $2,250 per month for a couple. Under the Deficit Reduction Act of 1984 (P.L. 98-369), SSI resource standards were increased $100 per year for an individual and $150 per year for a couple, beginning in 1985 and continuing through 1989. Thus, by 1989, resource standards had increased to $2,000 for an individual and $3,000 for a couple, but there is no current provision for increasing resource standards any further.
3.8 Program Interactions
3.8.1 Eligibility for Medicaid
The most important program interaction for disabled persons receiving SSI is their eligibility for health insurance coverage under Medicaid. Most, but not all, disabled SSI recipients are automatically eligible for Medicaid immediately upon receipt of SSI benefits. Unlike the link between SSDI and Medicare, there is no waiting period for Medicaid coverage.
State Medicaid programs have three options with regard to extending eligibility for Medicaid to SSI recipients. Under the "Section 1634" option, SSI recipients are automatically enrolled in Medicaid, without having to make a separate application. Thirty States have elected this option. Under the second option, SSI recipients are automatically eligible for Medicaid, but they must make a separate application to the State agency which administers the Medicaid program. Six States (Alaska, Idaho, Kansas, Mississippi, Nevada and Oregon) have elected this option.
Under the third and most restrictive option, referred to as the Section "209(b)" option, States may impose more restrictive eligibility criteria for Medicaid than are used in determining eligibility for SSI, as long as the criteria were used in the State Medicaid program prior to 1972 (when the SSI program was enacted). States may impose more restrictive criteria in determining disability, and/or more restrictive income and assets criteria. For example, in two States (Missouri and New Hampshire) SSI disabled children under age 18 are not eligible for Medicaid at all. Fourteen States (Connecticut, Hawaii, Illinois, Indiana, Minnesota, Missouri, Nebraska, New Hampshire, North Carolina, North Dakota, Ohio, Oklahoma, Utah, and Virginia) have elected the 209(b) option. Analyses have shown that the latter two options definitely reduce Medicaid enrollment of SSI disabled recipients compared to States which elect the 1634 option.8
Certain SSI disabled recipients are protected from losing their eligibility for Medicaid due to increases in income from Social Security benefits. This includes disabled SSI recipients who become eligible for DI benefits as adult disabled children, and persons who become eligible for Social Security widow's or widower's benefits at age 60. These provisions ensure that disabled SSI recipients do not lose health insurance coverage simply due to increases in income from Social Security benefits, particularly given the two-year waiting period for Medicare coverage required for DI beneficiaries.
A more detailed discussion of Medicaid coverage of persons with disabilities is provided in Chapter 8.
3.8.2 Eligibility for Food Stamps
Unlike SSI, eligibility for food stamps is determined on a household, not an individual, basis. For households which are comprised entirely of SSI recipients (i.e. disabled SSI individuals and couples living independently), eligibility for food stamps is generally automatic. In households where disabled SSI recipients live with other household members, the household is allowed to take additional deductions from income (e.g., for medical expenses) in determining eligibility for food stamps.
Because food stamp benefits are reduced by $0.30 for every $1.00 increase in recipient income, States lose Federal food stamp benefits (which are entirely Federally-funded) when they raise their State supplementation payments (which are entirely State-funded). For this reason, two States (California and Wisconsin) have elected to "cash out" their food stamp program, and to increase their State supplementation payment for SSI recipients in lieu of food stamps. In these two States, disabled SSI/SSP recipients are not eligible for food stamps; they instead receive comparable cash benefits through an increase in State supplementation payments.
3.8.3 Eligibility for AFDC
A disabled SSI recipient who lives in a household which is applying for AFDC benefits is not counted as part of the AFDC unit in determining eligibility for AFDC benefits. For example, an SSI disabled child living in a single-parent family is not taken into account in the determination of AFDC benefit levels for that household. At the same time, the disabled child's income and assets (including SSI income) are ignored in determining the AFDC benefit.
3.9 Special Program Issues
All of the issues related to the determination of disability by State Disability Determination Services (DDS) agencies, as discussed in Section 2.9, are also relevant to the SSI disabled population. Furthermore, the section 1619 program, discussed in Section 3.7, is now the major work incentive in the SSI program for disabled beneficiaries. Other program issues are discussed below.
3.9.1 SSI Participation Rates
Various studies have shown that many elderly persons over age 65 do not apply for SSI benefits, even though they would be eligible for benefits if they did apply. Separate studies have indicated that only about 50% of potentially eligible elderly SSI recipients actually participate in the program.9, 10 Many of these "non-participants" are persons with incomes that are close to Federal or State supplementation benefit standards, who, although eligible, would receive only a small monthly SSI benefit if they applied.
SSI participation rates for the disabled are more difficult to estimate, because disabled SSI beneficiaries must meet disability criteria as well as financial criteria. Survey data, which are generally used to estimate SSI participation rates among the elderly, can provide only rough estimates of the number of disabled persons who would pass the relatively strict definition of disability applied by SSA and DDSs. Thus, it is not known whether SSI participation rates among the disabled are similar to that among the elderly population.
Low participation rates among one sub-group of disabled persons is known: the disabled homeless. It is well known that a relatively large percentage (up to 30%) of homeless persons living in emergency shelters are chronically mentally ill, including many former residents of public mental hospitals. It is also known that relatively few of these homeless persons with chronic mental illness receive SSI benefits. There are many reasons for low SSI participation among this population, a major one being the difficulty which chronically mentally ill persons have in negotiating the SSI bureaucratic process, and the unavailability of persons to help them through the process. Consequently, the Social Security Administration has participated in a number of initiatives to increase SSI participation among the homeless, including the development of SSA outreach stations at the shelters themselves, the award of "immediate payments" to persons in need of emergency assistance, and the development of prerelease programs between SSA and public mental hospitals, in which SSI eligibility is determined while the patient is being prepared for discharge, so that payments can be initiated as soon as the patient is released from the hospital.
3.9.2 Representative Payees
The policy of the Social Security Administration is that every SSI beneficiary has the right to manage his or her own cash benefit payments. However, where there is evidence that the SSI beneficiary is not capable of managing benefits in his or her own best interests, SSI payments can be made to a representative payee. In general, all payments for SSI disabled children under age 18 are made to representative payees (usually parents). Also, persons with the disabilities of alcoholism or drug addiction are required to have representative payees. In December 1987, there were about 277,000 SSI children and 792,000 SSI disabled adults (about 31% of disabled adult beneficiaries) with representative payees. Representative payees are required to apply SSI payments solely for the beneficiary's current and foreseeable needs, and must make periodic account to SSA on how benefits were used.
3.10 Program Data
3.10.1 Current disabled SSI recipients, expenditures, and benefit levels
Exhibit 3-5 presents information on the number of disabled persons receiving Federal SSI benefits and/or State supplementation payments. In January 1989, over 2.7 million disabled persons received Federal SSI benefits. Of these, almost 1.4 million (50%) also received a State supplement to their Federal benefit. An additional 221,000 disabled persons had countable incomes in excess of the Federal benefit standard, and were eligible for a State supplement only. Thus, almost 3.0 million persons with disabilities received monthly SSI/SSP benefits in January of 1989. Persons eligible for SSI benefits on the basis of disability account for about two-thirds of the total SSI population.
Total Federal SSI payments to disabled persons in January 1989 equalled $706.9 million in January 1989, and State supplementation payments totalled $165.3 million, for a total of $872.2 million in monthly cash benefits to persons with disabilities. It is interesting to note that of the $165.3 million in State supplementation payments made to disabled persons in January 1989, $67.6 million (40.9%) was made in the State of California alone. This is partly due to the high State benefit standard used in California, and also partly due to the fact that SSI recipients in California receive their food stamp allotments in their State supplementation payment through a "cash out" demonstration program.
| EXHIBIT 3-5: Number of Disabled Persons Receiving SSI/SSP Benefits, Total Federal/State Payments to Disabled Persons and Average Monthly Benefit Levels: January 1989 | |
| Disabled Beneficiaries | |
| Federal SSI | 2,741,571 |
| Federal SSI and State Supplementation | 1,377,764 |
| State Supplementation only | 220,984 |
| Total SSI/SSP recipients | 2,962,501 |
| Total Payments | |
| Federal SSI | $706.9 million |
| State supplementation | 165.3 million |
| Total payments | $872.2 million |
| Average Monthly Benefits | |
| Federal SSI | $257.83 |
| State supplementation | $103.37 |
| SOURCES: Social Security Bulletin, Annual Statistical Supplements: 1980-1988. Excludes persons eligible for SSI/SSP on the basis of blindness. Includes persons receiving State-administered State supplementation payments. | |
The average monthly Federal SSI benefit in January 1989 was $257.83, and for those disabled persons eligible for State supplementation, the average State supplementation payment was $103.37.
3.10.2 Recent Trends
As shown in Exhibit 3-6, the number of SSI disabled recipients has been increasing at a fairly consistent rate since 1982. The annual compound rate of growth (ACRG) between 1982 and 1988 was 4.9%, and in this time period, the average number of disabled persons receiving SSI payments increased by about 123,600 each year.
Total Federal SSI payments for persons with disabilities increased from $3.9 billion in 1980 to $9.0 billion in 1988, an average annual compound rate of growth of 11.1%. Annual State supplementation payments for the disabled increased from $1.1 billion to $2.0 billion over the same time period. Disabled SSI recipients receive 77% of all Federal SSI benefits and 63% of all State supplementation payments.
3.10.3 Characteristics of Disabled SSI Recipients
Whereas almost two-thirds of disabled workers receiving Social Security Disability Insurance (DI) benefits are men, 58.4% of all disabled SSI beneficiaries are women. This is, no doubt, partly attributable to the fact that receipt of DI benefits is contingent upon prior participation in Social Security-covered employment, while receipt of SSI benefits is not.
| EXHIBIT 3-6: Number of Disabled Persons Receiving Federally-Administered SSI/SSP Payments 1980-1988 | ||||
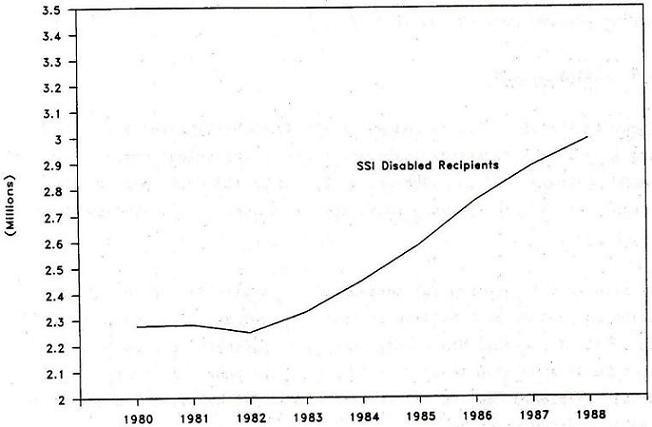 | ||||
| Total Disabled | 21 | 22-64 | Over 65 | |
| 1980 | 2,276,130 | 221,711 | 1,659,419 | 398,000 |
| 1981 | 2,280,525 | 222,987 | 1,639,538 | 418,000 |
| 1982 | 2,251,013 | 221,953 | 1,591,060 | 438,000 |
| 1983 | 2,329,596 | 220,258 | 1,643,338 | 466,000 |
| 1984 | 2,449,947 | 240,741 | 1,725,206 | 484,000 |
| 1985 | 2,586,741 | 257,065 | 1,825,676 | 504,000 |
| 1986 | 2,755,401 | 271,748 | 1,962,653 | 521,000 |
| 1987 | 2,888,852 | 280,407 | 2,071,245 | 537,200 |
| 1988 | 2,992,506 | 290,031 | 2,152,475 | 550,000 |
As shown in Exhibit 3-7, SSI recipients also tend to be younger than DI recipients. This is partly due to the fact that receipt of SSI benefits does not require prior participation in the workforce, as well as the fact that SSI recipients are more likely to be persons who have been disabled since childhood (persons with mental retardation) or who became disabled in early adulthood (persons with schizophrenia and other chronic mental illnesses). In December 1987, there were approximately 280,000 disabled children receiving SSI benefits, accounting for about 9 percent of all disabled recipients.
In contrast to the Social Security program, persons who initially receive SSI benefits as "disabled" do not get re-classified as "aged" upon their 65th birthday by the Social Security Administration. About 19% of all disabled SSI recipients are over the age of 65. There are few disabled recipients over the age of 75, however, because: (1) the SSI program was initially implemented in 1974, so that disabled persons who were age 64 in 1974 would only be 79 years of age in 1989; and (2) many disabled recipients lose their benefits when they are admitted to nursing homes, due to the lower SSI benefit standard applied in Medicaid-certified institutions.
| EXHIBIT 3-7: SSI Disabled Recipients by Age Cohort | |
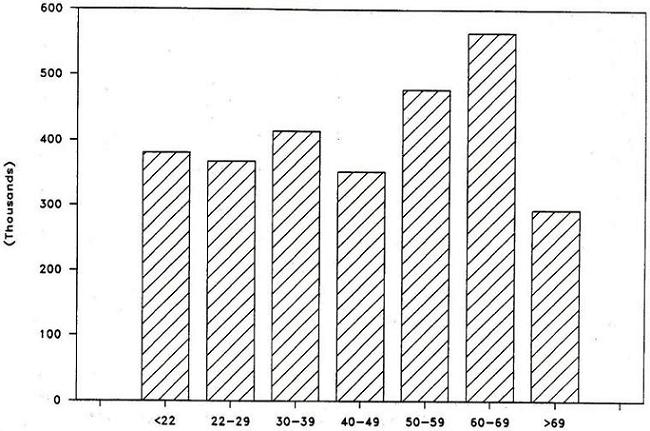 | |
| 22 | 380,473 |
| 22-29 | 366,907 |
| 30-39 | 413,091 |
| 40-49 | 351,512 |
| 50-59 | 477,236 |
| 60-69 | 564,472 |
| >69 | 292,499 |
| Total | 2,846,190 |
In recent years, the Social Security Administration has attempted to collect aggregate statistics on the primary disabling conditions of disabled SSI recipients. By December 1987, diagnosis data had been obtained for about 77% of disabled recipients under the age of 65. These data indicate that approximately half of disabled SSI recipients under age 65 have a primary disabling condition related to their mental, rather than physical, functioning. Approximately 27% of all recipients have a primary disabling condition of mental retardation and approximately 24% have mental disorders other than mental retardation. Among SSI disabled children, mental retardation is the primary disabling condition of 42.5% of all recipients.
Additional data on the characteristics of disabled SSI recipients between the ages of 18 and 64 are available from the Survey of Income and Program Participation (SIPP) conducted in 1984.11 These data indicate that 34% of disabled recipients in this age group were black, a much higher proportion than in the general population. Additionally, while only 19% were currently married, less than one in four lived alone. Approximately 50% of recipients between 18 and 64 still lived as dependent children in their parents' households. These data suggest that many adult disabled SSI recipients are persons with mental retardation or mental illness who still live with their natural parents.
3.10.4 Participation in the section 1619 program
Of the 2.1 million disabled adults between the ages of 18 and 64 receiving SSI benefits in September 1988, 33,155 (1.6%) were receiving special SSI benefits and/or Medicaid coverage under the section 1619 program. Section 1619 participants are persons who would otherwise not be eligible for benefits due to the fact that they have either started to earn income or have returned to work. Compared to disabled SSI recipients not participating in the 1619 program, 1619 participants are more likely to be: (a) younger; (b) white; (c) male; (d) have a diagnosis of mental retardation or mental illness; and (e) be receiving Social Security benefits.
3.10.5 Other income sources of disabled SSI recipients
Just over half of all SSI disabled recipients receive income from sources other than SSI. Approximately 37% receive Social Security benefits. These are persons whose Social Security benefits fall below Federal or State SSI benefit standards, and therefore receive SSI payments to bring their total cash assistance levels up to these standards. Note that not all of these persons are necessarily disabled workers receiving DI benefits. Some may be persons eligible for DI payments as adult disabled children, or persons receiving Social Security survivors' benefits as minor children, widows, or widowers.
Only about 5 percent of SSI disabled recipients have earned income. Another 10 percent have unearned income other than Social Security benefits. Just under half of all disabled recipients have no source of income other than SSI.
3.10.6 Termination of SSI benefits
In a recently-published longitudinal study of SSI recipients who were initially awarded SSI benefits during the period of October-December 1981, it was found that 41.7 percent of disabled recipients had become ineligible for benefits over a four-year follow-up period.12 The most frequent reason for the termination of SSI benefits was an increase in income due to receipt of Social Security benefits. Many persons had their SSI benefits terminated within the first six months, because there is a six-month waiting period required under the SSDI program between the established date of disability onset and the start of disability payments. Thus, many disabled SSDI applicants receive SSI payments during this waiting period until their SSDI benefits begin. Approximately 9 percent of new SSI awardees died within the four-year follow-up period, while the remaining 17 percent of recipients left for a variety of other reasons such as excess income from other sources, admission to a public institution or Medicaid-certified facility, leaving the country, excess resources, cessation of disability, or failure to provide needed documentation at eligibility redeterminations.
CHAPTER 4. DISABILITY PROGRAMS OF THE DEPARTMENT OF VETERANS AFFAIRS
The Department of Veterans Affairs administers a system of benefits for veterans and their dependents.13 The Veterans Benefits Administration administers two main assistance programs for veterans with disabilities: (1) the Disability Compensation Program; and (2) the Disability Pension Program. The Disability Compensation Program provides benefits to veterans who suffer from disabling injuries or diseases incurred or aggravated while in military service (not necessarily during active combat). The Disability Pension Program provides benefits to veterans who are permanently and totally disabled, who have served during a designated wartime period, and who meet specific income and net worth criteria. It is a needs-based program for veterans whose disabilities are not related to military service. Estimated FY 1989 payments under the Disability Compensation Program were $8.5 billion, while estimated payments under the Disability Pension Program were $2.6 billion.
In addition to these two main compensation/pension programs for disabled veterans, the VA administers a variety of smaller programs offering vocational rehabilitation, employment services, housing assistance, and prosthetic and sensory aids to disabled veterans. Only the two major programs, the Disability Pension Program and the Disability Compensation Program, are described in this chapter.
4.1 Disability Compensation Program
4.1.1 Overview and Purpose
The purpose of the Disability Compensation Program is to provide financial assistance to veterans with service-connected disabilities.
4.1.2 Authorization, History and Funding
This 100% Federally funded program is authorized under Title 38 United States Code, 107, Chapters 11, 13, 51, 53, 55, and 61. Actual FY 1988 program expenditures were $8.68 billion; estimated FY 1989 program expenditures are $8.50 billion, and estimated FY 1990 expenditures are $8.89 billion.
4.1.3 Definition of Disability
In the Disability Compensation Program, disability is defined as a partial or total impairment by injury or disease incurred or aggravated during military service. A VA rating board employs criteria developed by the VA to rate the extent of a disability.
4.1.4 Administrative Structure
The program is administered by the Compensation and Pension Service of the Veterans Benefits Administration of the Department of Veterans Affairs through 58 regional offices in each State, the District of Columbia, Puerto Rico, and the Republic of the Philippines. Each regional office has one or more rating boards, each composed of a physician and two nonmedical rating specialists, that determine eligibility for benefits.
4.1.5 Eligibility
Veterans are eligible for disability compensation if the disability was incurred or aggravated while on active duty. Unlike the VA Disability Pension Program, there are no income eligibility requirements and compensation is made for partial, as well as total, disability. The degree of disability is based on a Schedule for Rating Disabilities, which ranges from 0 to 100%. The severity of a disability is determined by using this rating schedule, which lists medical conditions and criteria for assigning each claimant a percentage disability rating. This rating is intended to represent an average earnings loss the veteran would experience in civilian occupations because of the disability. The rating is determined by a regional VA rating board based on the veteran's ability to function at work and at home. If a veteran has several impairments, each are rated separately and combined to determine an overall rating, taking into account the effects of multiple impairments.
4.1.6 Benefits Levels
Monthly cash payments are made to veterans awarded benefits under the Disability Compensation Program. Benefit levels are related to the percentage of disability determined by the VA rating board, which are assigned in increments of 10 percent (see Exhibit 4-1). The average annual benefit level for service-disabled veterans for FY 1987 was $3,808. For veterans determined to be 30% disabled or more, compensation is increased if they have dependents, if they are housebound, or if they require an aide and attendants allowance for in-home care. In 1987, the average annual compensation level for veterans determined to be 30% disabled or more was $7,416. For veterans determined to be less than 30% disabled, the average annual compensation was $1,032 (see Exhibit 4-2). There are limits on the amount veterans can receive based on the percentage of disability. In 1988, the maximum compensation for a veteran determined to be 100% disabled with no dependents was $14,068.
| EXHIBIT 4-1: VA Disability Compensation Program: Average Annual Benefit Level by Percent Disability, 1987 | ||||||||||
| *0% | 10% | 20% | 30% | 40% | 50% | 60% | 70% | 80% | 90% | 100% |
| $804 | $828 | $1,548 | $2,604 | $3,756 | $5,304 | $9,444 | $11,160 | $13,032 | $14,604 | $19,536 |
| SOURCE: Veterans Administration Annual Reports, 1980-1987. * Statutory award. | ||||||||||
| EXHIBIT 4-2: VA Disability Compensation Program: Average Annual Benefit Level 1980-1987 | ||||||||
| 1980 | 1981 | 1982 | 1983 | 1984 | 1985 | 1986 | 1987 | |
| 30% disabled | $723 | $809 | $870 | $927 | $957 | $984 | $1,020 | $1032 |
| > 30% disabled | $5,124 | $5,790 | $6,426 | $6,818 | $6,997 | $7,176 | $7,332 | $7,416 |
| SOURCE: Veterans Administration Annual Reports, 1980-1987. | ||||||||
4.1.7 Program Interactions
Benefits received from the Disability Compensation Program are not reduced or otherwise affected by benefits received from other programs.
4.1.8 Program Data
In FY 1987 there were 2,212,303 veterans receiving benefits under the Disability Compensation Program, over three times the number of veterans receiving nonservice-connected disability payments under the Disability Pension Program. Of these veterans, 65% were under 65 years old and 35% were 65 or older. Fifty-seven percent were determined to be less than 30% disabled while 43% were determined to be 30% or more disabled. For veterans with disability ratings of 30% or more and who had one or more dependents, the majority had a spouse only (see Exhibit 4-3). Exhibit 4-4 and Exhibit 4-5 show trends in the number of veterans receiving disability compensation benefits and total annual payments under the Disability Compensation Program from 1980 onward.
| EXHIBIT 4-3: VA Disability Compensation Program: Class of Dependent, 1987 | |
| Veterans 30% or more disabled with: | |
| Spouse only | 67.8% |
| Spouse, child or children | 26.7% |
| Spouse, child or children, and parent or parents | 0.3% |
| Spouse, parent or parents | 0.2% |
| Child or children only | 4.5% |
| Child or children, and parent or parents | 0.1% |
| Parent or parents only | 0.5% |
| SOURCE: Veterans Administration Annual Reports, 1980-1987. | |
4.2 Disability Pension Program
4.2.1 Overview and Purpose
The purpose of the Disability Pension Program is to provide financial assistance to veterans who have nonservice-connected disabilities, who served during a designated wartime period, and who meet income and net worth criteria.
| EXHIBIT 4-4: Number of Persons Receiving Benefits Under the Veterans Administration Disability Compensation Program 1980 to 1987 |
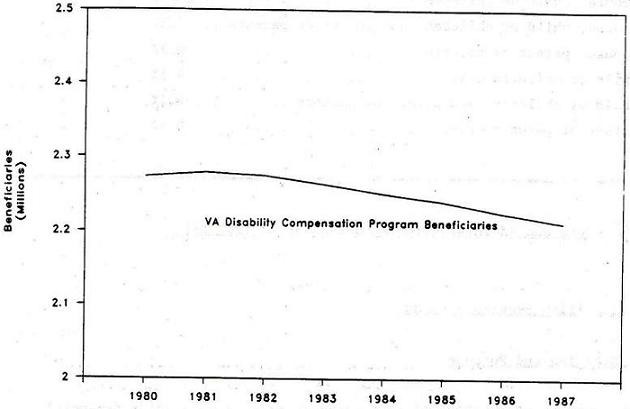 |
| EXHIBIT 4-5: Annual Payments Made Under the Veterans Administration Disability Compensation Program 1980 to 1990 |
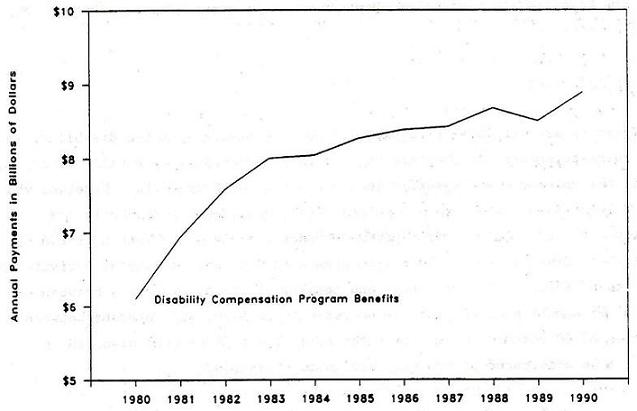 |
| 1989 and 1990 data are estimated. |
4.2.2 Authorization, History and Funding
The program is authorized under Title 38 United States Code, Chapters 15, 51, 53, 55, and 61; 92 Stat. 2508. The program is 100% Federally funded through allocations to the VA. Actual FY 1988 program expenditures were $2.50 billion. Estimated FY 1989 expenditures are $2.55 billion, and estimated FY 1990 expenditures are $2.64 billion.
4.2.3 Definition of Disability
Disability is defined as an injury or disease sustained outside of military service rendering a veteran permanently and totally impaired. Impairment is determined based on the veteran's ability to function at work and at home.
4.2.4 Administrative Structure
The program is administered by the Compensation and Pension Service, Veterans Benefits Administration, Department of Veterans Affairs, through 58 regional offices.
4.2.5 Eligibility
Veterans are eligible for disability pension benefits if the disability is nonservice-connected, if the veteran is either permanently or totally disabled, and if the veteran meets specific income and net worth criteria. Veterans who are at least 65 years of age are automatically considered permanently and totally disabled. In contrast, veterans under the age of 55 must be rated as 100-percent disabled and be unable to engage in substantial gainful activity in order to be defined as permanently and totally disabled. Veterans between the ages of 55 and 59 must be rated as 60-percent disabled, and veterans between the ages of 60 through 64 must be rated as at least 50-percent disabled in order to be considered permanently and totally disabled.
To establish eligibility for a pension, a veteran must file a claim with the VA regional office. If the veteran is under 65, the regional office then refers the veteran to a VA hospital for a medical examination evaluating the disability to see if it is permanent and total. The results of the medical examination are reviewed by a regional VA rating board which certifies that the veteran is permanently and totally disabled. The regional office may then grant the veteran a disability pension. The process takes approximately 120 days from the time the application is filed with the VA regional office to the time the veteran begins receiving payments.
4.2.6 Benefits Levels
The average annual expenditure per case for nonservice-disabled veterans for FY 1987 was $3,865 (see Exhibit 4-6). The amount of the pension is related to the veteran's income level and their beneficiary class including whether it is the veteran or a spouse receiving the pension, the number of dependents, and whether or not the beneficiary is housebound and/or requiring an aid and attendants allowance for in-home care. There are limits on the amount the beneficiary can receive. For example in 1987, the maximum a veteran living alone could receive was $5,963 per year and the maximum for a veteran with one dependent was $7,811 per year.
| EXHIBIT 4-6: VA Disability Pension Program: Average Annual Expenditure per Case FY 1980-FY 1987 | |||||||
| FY1980 | FY1981 | FY1982 | FY1983 | FY1984 | FY1985 | FY1986 | FY1987 |
| $2,428 | $2,726 | $2,982 | $3,193 | $3,416 | $3,581 | $3,755 | $3,865 |
| SOURCE: Veterans Administration Annual Reports, 1980-1987. | |||||||
4.2.7 Program Interactions
The veteran's nonservice-connected pension may be reduced if the veteran receives other benefits such as Social Security or workers' compensation which raise the beneficiary's income level. Since the pension is means-tested, additional income from these programs may place the veteran in a higher income category which may reduce the level of benefits he receives, or disqualify him from the program.
| EXHIBIT 4-7: Veterans Receiving Benefits Under the Disability Pension Program 1980 to 1987 |
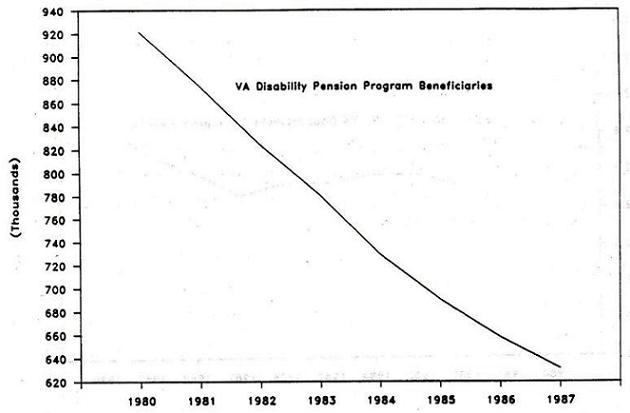 |
4.2.8 Program Data
In FY 1987 there were 631,306 nonservice-connected pension cases. Of these veterans, 39% were less than 65 years of age and 61% were 65 or older. Exhibit 4-7 and Exhibit 4-8 present recent trends in the number of veterans receiving disability pension program benefits and annual payments under the Disability Pension Program from 1980 onward. Estimated payments in FY 1989 under the Disability Pension Program totalled $2.5 billion.
| EXHIBIT 4-8: Annual Payments Made under the Veterans Administration Disability Pension Program 1980 to 1990 |
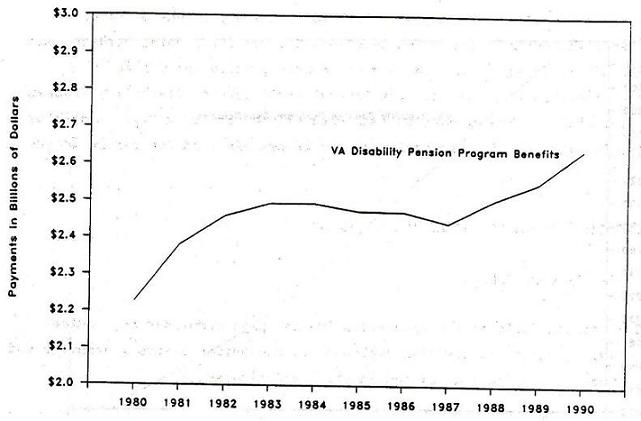 |
| 1989 and 1990 data are estimated. |
CHAPTER 5. FEDERAL CIVIL SERVICE PROGRAMS
Since civilian employees of the Federal government do not participate in the Social Security program, they are not eligible for Social Security Disability Insurance (DI) if they become disabled. Consequently, a separate system of disability compensation has been established for administering disability claims of Federal government employees. In general, the Federal Employees Compensation Program, administered by the Department of Labor, serves as a workmen's compensation insurance program for Federal workers, and pays short-term benefits for job-related injuries, while the Office of Personnel Management administers the Federal Civil Service Disability Program, which operates like the DI program, and generally covers long-term disability benefits for Federal civilian employees who become disabled and can no longer work.
5.1 Federal Employees' Compensation Program
5.1.1 Overview and Purpose
The Federal Employees' Compensation Program pays compensation, medical, and survivor benefits to civilian employees of the United States government and to their dependents for job-related injuries and diseases.
5.1.2 Authorization, History and Funding
This program is authorized under the Federal Employees, Compensation Act of 1966. An estimated $1.24 billion will be spent on Federal workman's compensation benefits in 1989 and $1.14 billion was spent in 1988.
5.1.3 Definition of Disability
The program compensates for job-related injuries rendering an individual completely or partially disabled. Covered injuries include traumatic injuries, which occur at a specific place and time, and nontraumatic injuries, which are occupational diseases or illnesses occurring over a longer period than one workday. Covered injuries do not include those caused by willful misconduct, by intent to injure oneself or another, or by employee intoxication.
5.1.4 Administrative Structure
The program is administered by the Department of Labor, Office of Workers' Compensation Programs (OWCP) through 13 district offices located across the United States.
5.1.5 Eligibility
To be eligible for Federal workman's compensation an individual must 1) be a civilian employed by the United States government 2) sustain a job-related injury or disease and 3) report the injury within the time limit for the particular injury.
Reports of a traumatic injury must be filed within 30 days of the injury and reports of an occupational disease must be filed within 30 days of the employee's realization that the disease or illness was caused or aggravated by their work conditions. Claims for compensation must be filed within 3 years of the date of injury although OWCP may cover claims submitted later if the injury was documented in a written notice or by the employing agency.
5.1.6 Services/Benefits Provided
Employees with traumatic injuries receive their regular salary for up to 45 calendar days after the day of injury. Following this, compensation payments begin after a three-day waiting period that is not covered unless the disability is permanent or lasts more than 14 additional days.
The formula for the monthly, nontaxable compensation benefit is as follows: two-thirds of the employee pay rate if the individual has no dependents and three-fourths of the employee pay rate if the individual has one or more dependents. Dependents include spouse, children, children for whom the individual is paying child support, and dependent parents. An ex-spouse does not qualify as a dependent. The maximum annual rate is set at three-fourths of the highest rate of basic pay for GS-15 which is $56,250 per year. There is no limit on the number of years an individual can receive compensation but the OWCP will often require a yearly medical examination for individuals receiving extended disability compensation.
If a disabled individual can return to work at a lower pay rate, the individual can receive compensation for the loss of earning capacity resulting from the injury. The compensation is equal to two-thirds or three-fourths (depending on whether or not they have dependents) of the difference between what they were earning before and after the injury.
5.1.7 Programs Interactions
Individuals cannot simultaneously receive disability compensation from OWCP and the Federal civil service disability program administered through the Office of Personnel Management (OPM), they must elect one or the other. However, if an individual chooses OPM disability compensation, OWCP will still cover the costs of medical treatment for a job-related injury. Individuals must choose between OWCP coverage and Veterans Administration coverage when the injury was originally service-connected and later aggravated on the job. However payments for non-service-connected disability or for a pension are allowed concurrently with benefits from OWCP both to the individual and his/her dependents. For OWCP benefits received after September 1974, compensation may be received concurrently with military retirement or retainer pay. An employee may receive Social Security Administration (SSA) payment and OWCP benefits concurrently as long as his/her total benefit does not exceed 80% of the employee's average earnings before he became disabled. If this maximum benefit level is reached, the individual's SSA benefits will be reduced to the maximum allowable compensation.
5.1.8 Program Data
In FY 1987, 156,410 Federal employees' compensation cases were filed and in FY 1988, 169,418 cases were filed. Exhibit 5-1 and Exhibit 5-2 present the annual number of cases filed from 1984 to 1988 under the program and annual payments made from 1982 to 1989. In FY 1989, an estimated $1.2 billion in disability compensation payments were made under the Federal Employees Compensation Program.
| EXHIBIT 5-1: Number of Cases Filed Per Year Under the Federal Employees Compensation Program 1984 to 1988 |
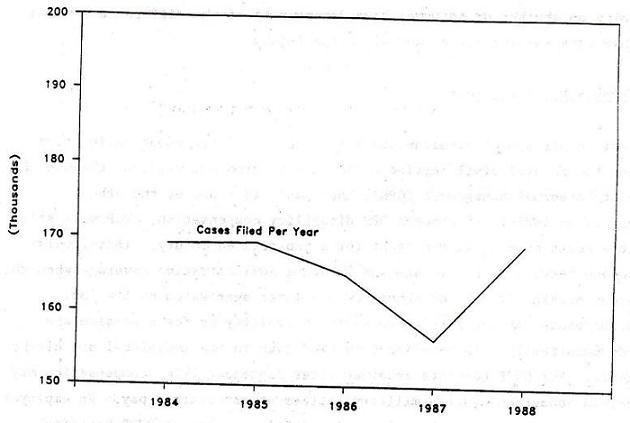 |
| EXHIBIT 5-2: Annual Benefits Paid Under the Federal Employees Compensation Program: 1982 to 1989 |
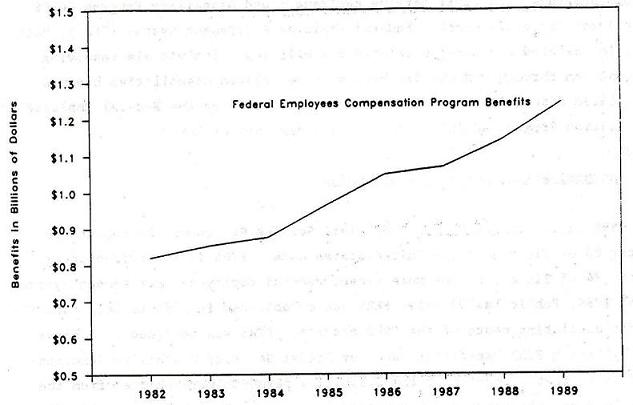 |
| 1989 data are estimated. |
5.2 Federal Civil Service-Disability Program
5.2.1 Overview and Purpose
The Office of Personnel Management (OPM) administers two programs which provide monthly cash benefits to disabled employees of the U.S. government. The two programs, the Civil Service Retirement and Disability Program (CSRS) and the more recently enacted Federal Employee Retirement System (FERS), both cover job-related and non-job-related disabilities. Individuals receiving compensation through OPM usually have non-job-related disabilities because job-related disabilities are covered more generously by the Federal Employee's Compensation Program administered by the Department of Labor.
5.2.2 Authorization, History, and Funding
CSRS is authorized by the 1969 Civil Service Retirement Amendments to Chapter 83 of Title 5 of the United States Code. FERS is authorized under Chapter 84 of Title 5 by the more recent Federal Employees' Retirement System Act of 1986, Public Law 99-335. FERS was established in 1986 to help curb the rapidly escalating costs of the CSRS program. FERS was designed to achieve this by having FERS benefits reduced by Social Security Disability Insurance benefits so that a portion of the disability payments were shifted from the Civil Service Retirement and Disability Fund to the Social Security Disability Trust Fund. In 1986, $3.55 billion in benefits was administered to OPM disability beneficiaries.
5.2.3 Definition of Disability
The OPM definition of disability is an employee who is "unable to render useful and efficient service because of disease or injury (1) in the employee's current position or (2) in a vacant position in the same agency at the same grade or pay level for which the individual is qualified for reassignment (5 CFR Ch.1, 831.502)."
5.2.4 Administrative Structure
OPM administers both the CSRS and FERS programs. Disability applications are sent to OPM by either the employee or his or her department or agency and OPM makes the determination of eligibility.
5.2.5 Eligibility
To be eligible for disability benefits through either the CSRS or FERS programs, a disabled individual must be a civilian employee of the U.S. government. Government employees with at least five years of service as of January 1, 1987 had the option to switch from CSRS to FERS between July 1 and December 31, 1987, but newer employees only have FERS as an option. To receive CSRS benefits an employee must have completed at least 5 years of service and to receive FERS benefits an employee must have completed at least 1.5 years of service and have earned Social Security work credit hours.
The procedure for applying for CSRS and FERS benefits is the same. An applicant for disability retirement must submit an application to OPM before leaving their job or within one year after leaving. Exceptions are made for employees found to be incompetent who are allowed to file up until a year after they have been restored to competency or a fiduciary is appointed, whichever is earlier.
A department or agency files for the employee when the employee is institutionalized or has no family or guardian, and the department or agency concludes that cause for unacceptable performance or conduct, or attendance is due to disease or injury. Before the employee is removed from service, the agency must notify the employee in writing that the agency is submitting a' disability retirement application for the employee to OPM and that the employee may review the application and submit one himself, in addition, if he desires.
OPM determines whether or not a claim will be granted based on documentation of various conditions of disability. To be classified as disabled, an individual must provide documentation of a medical condition which causes a deficiency in their job performance, conduct, or attendance. The condition must be expected to last at least a year and the agency must not be able to accommodate the individual's medical condition nor reassign them to a vacant position at the same grade or pay level.
Each disability annuitant under 60 years of age must be reexamined annually, unless OPM determines their disability is permanent. When a disability annuitant is found to have recovered, their annuity will be discontinued beginning one year from the date of the examination or the day of reemployment, whichever is first. Even if a disability annuitant has not been found to have recovered, if their income from wages and/or self-employment exceeds 80% of their earning capacity comparable to the rate of pay at the time of their retirement, payment of the annuity terminates 180 days after the end of the calendar year in which earning capacity was restored or upon reemployment to a position where their earning capacity is restored.
5.2.6 Services/Benefits Provided
Computation of the annuity was changed under the FERS program from the method used under CSRS. As was noted earlier, this is one of the main differences between the disability programs. Under the CSRS, annuity is based on the number of years of service and the employee's average pay, which is the largest rate of pay calculated by averaging the employee's basic pay rate over any three consecutive years of service. The resulting annuity is a percentage of the employee's average pay, from 1.5 to 2.0%, depending on the number of years of service.
Under FERS, annuity is based solely on the employees average pay and does not take into account years of service. The annuity is 60% of the employee's average pay for the twelve months after the annuity begins or is restored, and 40% of the employee's average pay after that.
5.2.7 Program Interactions
Individuals cannot receive disability compensation from the Federal Employees' Compensation Programs and the OPM disability programs at the same time, they must elect one or the other. Under FERS, but not CSRS, the annuity is reduced by 100% of the annuitant's Social Security disability insurance benefit for periods of concurrent coverage during the first year of FERS coverage and by 60% of the disability insurance for any time thereafter.
5.2.8 Program Data
In FY 1985, there were 332,000 disability annuitants; in FY 1986, there were 326,000 annuitants; and in FY 1987, there were 318,000 annuitants. The data for the total number of disability annuitants is for annuitants from both the CSRS and FERS programs. Since FERS is a relatively new program, there has not been much activity as yet under FERS and most annuitants are covered by the CSRS program. Exhibit 5-3 and Exhibit 5-4 present the annual number of cases receiving benefits under both programs from 1980 onward, and annual payments made under the program through FY 1986, the most recent year for which payment data are available. Disability payments made in FY 1986 under both programs totalled $3.5 billion.
| EXHIBIT 5-3: Number of Beneficiaries Receiving Disability Payments under the Federal Civil Service Disability Program 1980 to 1987 |
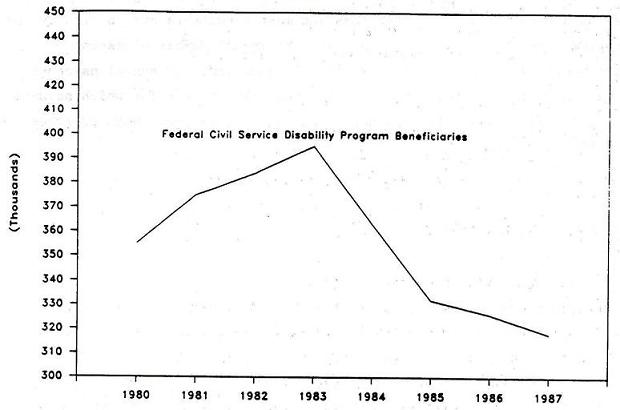 |
| EXHIBIT 5-4: Annual Benefits Paid under the Federal Civil Service Disability Program: 1980 to 1986 |
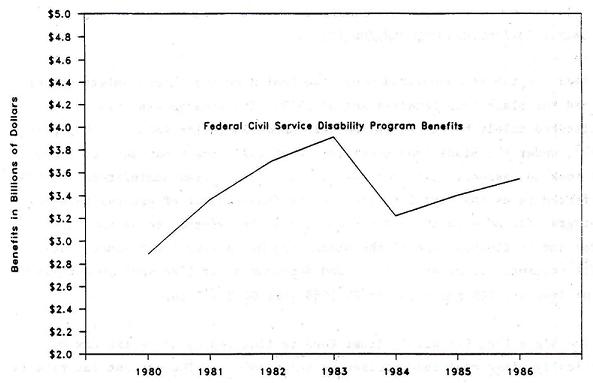 |
CHAPTER 6. BLACK LUNG PROGRAM
6.1 Overview and Purpose
The Black Lung program pays monthly cash benefits to coal miners who are totally disabled as a result of pneuomoconiosis, to widows of miners who died from Black Lung disease, and to their dependents.14
6.2 Authorization, History and Funding
This program is authorized under the Coal Mine Health and Safety Act of 1969 and the Black Lung Benefits Act of 1972. The program was originally administered solely by the Social Security Administration (SSA) but beginning in 1973, under the Black Lung Benefits Act of 1972, the Department of Labor (DOL) took on responsibility for new claims. The program administered by SSA is referred to as the Part B program and is financed out of general revenues. The program for more recent and current claims is referred to as the Part C program and is financed out of the Black Lung Disability Trust Fund. Total SSA benefit payments for miners, widows and dependents for 1988 were an estimated $904 million and DOL payments for FY 1988 were $602 million.
The Black Lung Disability Trust Fund is financed by an excise tax on domestically mined coal sold or used by the producer. The current tax rate is the lesser of: (1) $1.10 per ton of coal from underground mines plus $0.55 per ton of coal from surface mines; or (2) 4.4 percent of the total price for which the coal is sold. However, since its establishment in 1978, the Trust Fund has always operated at a deficit. Total revenue from the excise tax, plus interest and fines, was about $4.7 billion through 1988, while benefit payments and administrative expenses totalled about $6.6 billion, leaving a cumulative deficit of about $3 billion through 1988. Under current law, this deficit must be repaid from future Trust Fund revenues.
6.3 Definition of Disability
Three general conditions must be met for a claim to be approved for black lung benefits: (1) the miner must have (or, if deceased, have had) pneumoconiosis; (2) the miner must be totally disabled by the disease (or must have been totally disabled at the time of death); and (3) the pneumoconiosis must have arisen out of coal mine employment.
6.4 Administrative Structure
Two government agencies administer the Black Lung Program depending on when claims were initiated in a given case. The Department of Labor is responsible for all claims made by miners and their dependents, payable after July 1, 1973. The Social Security Administration handles claims payable before this date and survivor claims from these miners' relatives filed by December 31, 1973 or within six months of the miner's death.
Application for black lung benefits can be filed at any Social Security office. Expect with respect to surviving children, no benefits can be paid for months before the application is filed.
6.5 Eligibility
To be eligible for black lung benefits, an applicant must provide documentation that he or she was employed as a coal miner, has a medical diagnosis of pneumoconiosis, and is totally disabled by the disease. Total disability is defined as an inability to engage in comparable and gainful work by reason of pneumoconiosis which can be expected to result in death or which has lasted or can be expected to last for a continuous period of not less than 12 months.
The definition of "comparable and gainful" work in the Black Lung program is less restrictive than the definition of "substantial gainful activity" employed in the SSDI and SSI programs since comparable and gainful work is defined as work "in the immediate area of residence requiring skills and abilities comparable to those of any work in a mine or mines in which the miner was previously engaged with some regulatory and over a substantial period of time." Thus, unlike disabled persons applying for SSDI or SSI, black lung applicants must only demonstrate an inability to perform comparable work in the immediate area of residence.
The 1972 amendments to the original legislation expanded coverage to surface as well as underground coal miners. Widows and dependents of miners with black lung disease can also qualify for benefits.
6.6 Services/Benefit Provided
The basic monthly benefit rate for disabled miners or their widows is 37.5% of the monthly pay rate to Federal employees in grade GS-2. Effective January 1989, the basic benefit rate was $358.90 per month, and the maximum payment rate per family $717.80. The basic rate is adjusted for the number of qualified dependents according to the following formula: a 50% increase for one dependent, 75% for two dependents, and 100% increase for 3 or more dependents. The program has no income requirements, but the benefit level is offset for earnings above a certain threshold. In 1988 the benefit level for eligible miners was offset one dollar for every one dollar of annual taxable income over $6,021. For beneficiaries aged 65 to 69 years, the benefit offset rate was one dollar for every two dollars of annual taxable income above $8,400 and for beneficiaries 70 years or older, there was no offset.
Since Black Lung payments are tied indirectly to Federal employee pay scales, increases are automatically payable when Federal salaries are increased.
6.7 Program Interactions
Black lung benefits are not taxed by the Federal government, although States may do so.
Benefits are reduced (excluding benefits to widows and children) due to excess earnings in the same manner as Social Security benefits. In 1989, benefits for persons under age 65 are reduced $1 for each $2 in annual earnings in excess of $6,480; for persons aged 65-69 benefits are reduced for earnings in excess of $8,880. Black lung benefits are not reduced due to receipt of Social Security Disability insurance benefits or Supplemental Security Income (SSI) benefits.
Under Part B (benefits for claims made prior to July 1, 1973), benefits are reduced for payments received under State workers' compensation, unemployment compensation, or disability insurance laws, if such payments are for death or disability due to pneumoconiosis. Under Part C, benefits are reduced for State or Federal workers, compensation, but not for unemployment or disability insurance.
6.8 Program Data
In 1988, almost 400,000 individuals were paid black lung benefits. Approximately, 243,000 miners, survivors and dependents received benefits under the Part B program administered by the Social Security Administration, while 149,000 persons received benefits under Part C administered by the Department of Labor. Surviving miners comprise only about 29 percent of total beneficiaries, while widows, surviving children, and dependents comprise 71 percent of the beneficiary population. Exhibit 6-1 presents the total number of Part B and Part C recipients of black lung benefits from 1980 to 1988.
Exhibit 6-2 presents total payments made under the Part B and Part C programs from 1980 to 1988. Total payments have declined slightly from $1.8 billion in 1980 to about $1.5 billion in 1988; benefit payments are expected to continue to decline in the future.
| EXHIBIT 6-1: Number of Persons Receiving Black Lung Benefits from the Social Security Administration (SSA) and Department of Labor (DOL) |
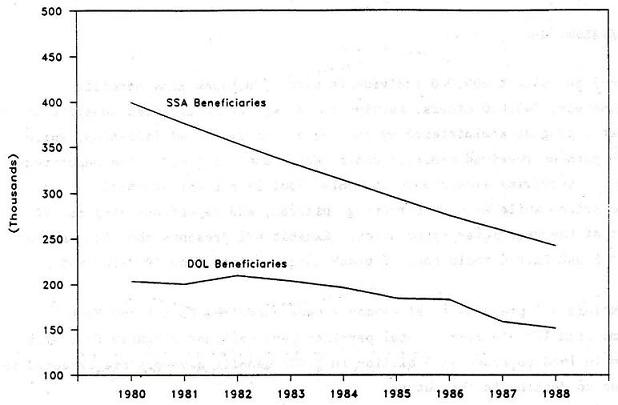 |
| SSA beneficiaries are persons with claims filed prior to July 1, 1973; DOL beneficiaries are persons with claims filed subsequent to June 30, 1973. Beneficiaries include miners, survivors, and dependents. |
| EXHIBIT 6-2: Annual Payments for Black Lung Benefits Made by the Social Security Administration (SSA) and Department of Labor (DOL) 1980 to 1988 |
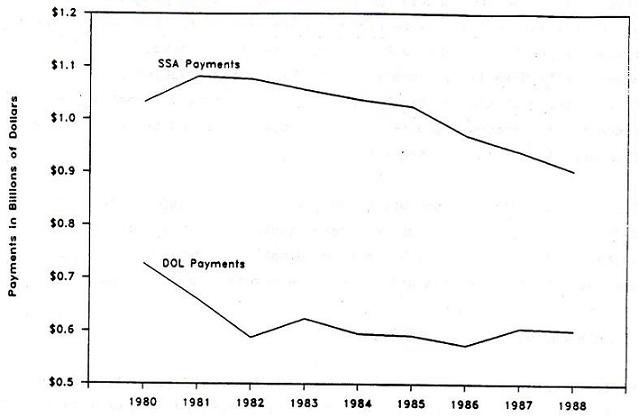 |
| SSA beneficiaries are persons with claims filed prior to July 1, 1973; DOL beneficiaries are persons with claims filed subsequent to June 30, 1973. Beneficiaries include miners, survivors, and dependents. |
CHAPTER 7. MEDICARE COVERAGE OF PERSONS WITH DISABILITIES
7.1 Overview and Purpose
Medicare is a Federally financed health insurance program for elderly and disabled persons who are insured under the Social Security program. The purpose of Medicare is to provide health insurance coverage for Social Security beneficiaries who have reached age 65 or who have left the workforce as a consequence of a disability. Medicare eligibility for disabled persons under age 65 is closely linked to eligibility for Social Security Disability Insurance (DI), although there is a two-year waiting period between award of DI benefits and eligibility for Medicare.
There are two major components to Medicare: (1) the hospital insurance (Part A) program; and 2) the supplementary insurance (Part B) program. In 1989, there were approximately 3.2 million disabled persons under age 65 covered under Medicare Part A and 2.9 million covered under Part B.
7.2 Authorization, History and Funding
Medicare was originally enacted on July 30, 1965 as Title XVIII of the Social Security Act. Originally, the program only covered persons aged 65 and over. Under 1972 amendments to the Act (P.L. 92-603) coverage was extended to persons entitled to Social Security benefits because of their disability and to certain individuals with end-stage renal disease. Various other legislative changes have been made to the Medicare program in recent years.15
There are separate financing mechanisms for the two components of Medicare, and separate Trust Funds have been established for each component. The Hospital Insurance Trust Fund (Part A) is financed primarily through the Social Security payroll (FICA) tax on Social Security-covered employment. Employers and employees make equal contributions. In 1989, the tax rate for the HI Trust Fund was 1.45 percent of earnings up to $48,000 per employee. The taxable earnings base will continue to increase each year in accordance with increases in average earnings.
The Supplemental Medical Insurance (SMI) Trust Fund (Part B) is voluntary and is financed partly from premiums paid by Part B enrollees and partly from general revenues. Premium income originally financed half of the Part B Trust Fund, but has since declined to the point of financing about 25 percent of total Part B Trust Fund contributions. In 1989, the monthly premium for all Part B enrollees was $31.90. This premium is usually deducted from an enrollee's monthly Social Security benefits.
7.3 Definition of Disability
Since eligibility for Medicare as a disabled enrollee under age 65 is linked to receipt of SSDI benefits, the definition of disability employed in determining eligibility for Medicare benefits is exactly the same definition employed in determining eligibility for SSDI benefits (see Chapter 2).
There is one exception. Insured Social Security beneficiaries, or dependents of insured beneficiaries, are eligible for Medicare if they are medically determined to have end-stage renal disease. End-stage renal disease is defined as "that stage of kidney impairment that appears irreversible and permanent and requires a regular course of dialysis or kidney transplantation to maintain life." In the case of a dialysis patient, coverage begins in the third month after the month in which a course of renal dialysis is initiated (although the three-month waiting period can be waived if the individual participates in a self-care training program). For transplant patients, coverage can begin as early as the month in which the patient is hospitalized for transplantation, and continues until the 36th month after the transplant, if it is successful.
7.4 Administrative Structure
Responsibility for administration of the Medicare program rests with the Health Care Financing Administration (HCFA) within the Department of Health and Human Services. The Social Security Administration also plays a role in the administration of Medicare, primarily in the enrollment of beneficiaries and the maintenance of beneficiary rolls. For SSDI beneficiaries, enrollment in Medicare is automatic once the 24-month waiting period is reached.
HCFA contracts with fiscal intermediaries, which are usually insurance companies, to process and pay Medicare claims, and to perform other administrative and operational tasks for the program. HCFA also contracts with Peer Review Organizations (PROs), which include physician reviewers, to determine whether the health care services paid for by Medicare are reasonable and medically necessary, are furnished effectively in the most economical setting, and meet professional quality standards.
7.5 Eligibility
In addition to persons with end-stage renal disease, there are three major categories of disabled social security beneficiaries who receive Medicare benefits prior to age 65:
- Disabled workers;
- Disabled widows and widowers eligible for early benefits between the ages of 50 and 65; and
- Adult disabled children.
Persons in all three categories must undergo a 24-month waiting period between the first award of social security benefits and entitlement to Medicare benefits. Medicare coverage begins on the first day of the 25th month of entitlement to social security benefits. Since there is a 5-month waiting period between the date of disability onset and the award of social security disability benefits, some disabled persons are not be entitled to Medicare coverage until the 30th month of their disability. Because persons receiving social security benefits as adult disabled children ate not eligible for these benefits until the age of 18, Medicare coverage of adult disabled children cannot begin until at least age 20.
7.5.1 Termination of Medicare benefits
If a disabled Medicare enrollee loses entitlement to DI benefits, because the enrollee's impairment has improved or ceased, then Medicare coverage terminates at the end of the month following the month in which he or she is notified of the termination of disability status. However, if an enrollee's DI benefits cease due to an increase in earnings, Medicare coverage can continue for up to 4 years, as long as the disability continues, as explained further below.
7.5.2 Work incentive provisions under Medicare
Since the threatened loss of health insurance benefits is considered a strong work disincentive, perhaps more so than the threatened loss of cash assistance benefits, there are a number of provisions in the social security program to continue Medicare coverage for disabled social security beneficiaries who attempt to work.
First, Medicare coverage continues throughout a beneficiary's "trial work" period. The trial work period is a period of up to nine months (not necessarily consecutive) in which disabled beneficiaries can earn more than $75 per month without losing entitlement to their social security benefits. Further, Medicare coverage is extended for at least 39 months after completion of the trial work period, as long as the beneficiary is still determined disabled (4 years after the start of the trial work period). In other words, as long as a disabled beneficiary has no medical improvement in his or her condition, and remains disabled, then he or she can still receive Medicare coverage for at least 39 months after their cash benefits are terminated due to their ability to earn income on their own. Finally, if a disabled beneficiary attempts work and temporarily loses his or her entitlement to cash benefits, but then is forced to leave work and reapply for social security benefits, then the two-year waiting period for Medicare coverage is waived, as is the 5-month waiting period for DI benefits.
7.6 Services Provided Under Medicare
Benefits provided under Medicare are administered under two separate components: (1) the Hospital Insurance program (Part A); and (2) the supplementary insurance program (Part B). Persons eligible for Part A coverage are also eligible for Part B coverage, which requires payment of a monthly premium, and participation is voluntary.
7.6.1 Benefits Provided Under Part A
Disabled persons under age 65 are covered for the following health care expenses under Medicare Part A:
-
Inpatient hospital care. Medicare covers all reasonable charges for a medically-necessary in-patient acute-care hospital stay prescribed by a physician. Medicare provides full coverage of inpatient hospital care for the first 0 days per spell of illness, minus a deductible (which in 1989, was $560).16 From the 61st to the 90th day of a spell of illness, Medicare provides partial hospital coverage; the beneficiary is liable for coinsurance of one-fourth the deductible amount per day of coverage (e.g. $140 per day in 1989), above which Medicare pays the balance. A beneficiary is also eligible for a lifetime reserve of 60 days of inpatient hospital coverage for use in any benefit period in which more than 90 days of hospital care has been utilized. The coinsurance amount for these additional 60 days of coverage is half the deductible ($280 in 1989). Medicare does not cover convenience items, such as telephones or television rentals, or luxuries such as a private room or private duty nursing.
-
Skilled nursing facility (SNF) care. Medicare will pay for up to 100 days per spell of illness in a nursing home which is certified by Medicare as a skilled nursing facility (SNF). Most nursing homes are not Medicare-certified because they do not provide skilled nursing care. To qualify for SNF coverage, the Medicare beneficiary must require continuous (not intermittent) and skilled (not custodial) nursing care prescribed by a physician. A SNF stay is also not covered unless the patient spent at least three consecutive days in a hospital for a related condition within 30 days of nursing home admission. Medicare provides full payment for covered stays for the first 20 days of SNF care. For days 21 to 100, there is A Coinsurance requirement equal to one-eighth the hospital deductible. In 1989, the coinsurance requirement would have been $70 per day.
-
Home health care. Medicare covers an unlimited number of medically necessary home health visits by nurses, therapists and other health care professionals under both Part A and Part B. To be eligible for services, a beneficiary must: (a) require skilled nursing care, physical therapy, or speech therapy; (b) be in need of "intermittent" care, as opposed to continuous care (c) have that need certified by a physician under a home care plan; (d) be confined to the home; and (e) receive services from a Medicare-certified home health agency. A patient who needs full-time skilled nursing care over an extended period of time would not qualify for home health benefits under the "interrmittent" requirement.
-
Hospice care. Medicare provides coverage for a broader service benefit package for terminally ill beneficiaries with life expectancies of six months or less. In accepting the hospice service benefit package, enrollees must waive the right to traditional Medicare curative treatments. There are small coinsurance requirements for drugs and in-home respite care services. Medicare pays certified hospice care providers a prospective payment amount for various categories of hospice care, subject to an annual "cost cap" for each hospice.
-
Inpatient psychiatric care. Medicare coverage for inpatient psychiatric care is generally the same as coverage of inpatient medical care, except that benefits are limited to 190 days of care in the beneficiary's lifetime. If a beneficiary is an inpatient in a psychiatric hospital at the time he or she becomes eligible for Medicare coverage, certain restrictions apply.
7.6.2 Benefits Provided Under Part B
Of the 3.2 million disabled persons receiving Medicare benefits under Part A, about 2.9 million (93%) are also covered under Part B. For Part B services, Medicare pays 80% of reasonable charges after an annual deductible of $75. The monthly premium for Part B services in 1989 was $31.90 per month. Medicare services provided under Part B include:
-
Physician's services. Medicare covers medical and surgical services provided by physicians, as well as ancillary services provided in a doctor's office. Routine services, such as routine physical examinations and eye and ear exams, are not covered. Limitations also apply to services provided by dentists, podiatrists, chiropractors, and the treatment of mental illness.
Most physicians agree to accept Medicare's approved charges for physician services as payment in full. This is called "accepting assignment" For services provided by these physicians, enrollees must only pay the 20% coinsurance amount on approved charges. Other physicians, however, do not accept assignment, and charge more than the Medicare approved charge. For services provided by these physicians, enrollees must pay the 20% coinsurance amount of the approved charge, plus any additional charges above the Medicare approved charge.
-
Other medical and health services. Part B covered services also include laboratory and other diagnostic tests, home health services, X-ray and other radiation therapy services, hospital outpatient services, home dialysis equipment and supplies, prosthetic devices, immunosuppressive drugs, physical and speech therapy, and ambulance services.
7.7 Recent Program History and Legislative Changes
In efforts to slow the growth of Medicare program expenditures, while maintaining the scope and quality of Medicare benefits for enrollees, myriad legislative changes are made to the Medicare program each year. The Medicare Catastrophic Coverage Act of 1988 provided for the greatest expansion of Medicare benefits since the program was originally enacted in 1965, but political resistance to the financing structure of the bill led to its repeal in 1989. This report will not attempt to describe all the recent changes which have been made to the Medicare program, but a recent change which specifically affects disabled Medicare enrollees under age 65 is described below.
7.7.1 Medicare as secondary payer for certain disabled Medicare enrollees
Under the Omnibus Budget Reconciliation Act of 1986, effective January 1987, Medicare became the secondary payer for disabled Medicare enrollees who are covered by a "large group health care plan." A large group health care plan is defined as an employer with 100 or more employees. This provision also applies to dependents of employees covered by a large group plan. Thus, for example, if an employee receives full family coverage under his group plan and his working spouse becomes disabled and subsequently entitled to Medicare benefits, Medicare becomes the secondary payer for all health care services which are covered both by the employer group plan and by Medicare. This provision does not apply to elderly Medicare enrollees who are also covered by a private health insurance plan.
This provision shifted some health care costs from the Medicare program to private health insurance plans for disabled enrollees covered by more than one plan. Note that it may be financially beneficial for a disabled Medicare enrollee to maintain coverage under a group health plan if employee contributions to the group plan are less than Medicare Part B premiums, and/or if the group plan provides broader coverage with fewer deductibles and copayments requirements than Medicare.
7.8 Program Interactions
7.8.1 Social Security Disability Insurance
Enrollment in Medicare by persons under age 65 is predicated upon entitlement to social security disability (DI) benefits, with the exception of persons with end-stage renal disease, who can become eligible for Medicare without receiving social security. Changes in policies regarding the eligibility of disabled persons under age 65 for DI benefits therefore impact enrollment and expenditures in the Medicare program.
7.8.2 Interaction of Medicare and Medicaid Among the Disabled
Approximately 25-30% of all disabled Medicare enrollees under age 65 are also covered by Medicaid. A disabled social security beneficiary entitled to Medicare benefits may also be entitled to full or partial Medicaid benefits through a variety of eligibility pathways, as follows:
-
DI recipients whose social security benefits fall below Federal and/or State SSI benefit standards, and who therefore also receive monthly SSI cash payments, are generally eligible for Medicaid by virtue of their receipt of SSI.
-
DI recipients with incomes above SSI benefit standards may nonetheless qualify for Medicaid under a higher "medically needy" income level in the 36 States (including the District of Columbia) which have medically needy programs.
-
DI recipients with incomes above SSI benefit standards may qualify for Medicaid under a State Medicaid option to extend eligibility to all elderly and disabled persons with incomes below the poverty threshold. As of July 1989, three States (New Jersey, Florida and the District of Columbia) had elected this option. New Jersey and Florida have set their Medicaid eligibility levels at 100% of the poverty level, while Florida has set its level at 90% of poverty. Two other States (Alaska and California) already have SSI/SSP benefit standards above the poverty level due to their State supplementation of SSI.
-
Disabled Medicare enrollees with substantial out-of-pocket expenses for medical care services not covered by Medicare (including Medicare premiums, deductibles and coinsurance requirements) may qualify for medical assistance under Medicaid "spend-down" provisions. Under spend-down, out-of-pocket medical costs are deducted from applicants' incomes until their incomes are lowered to the medically needy threshold. These spend-down provisions apply both in States which have medically needy programs and in States which have elected the so-called Section 209(b) option.
Thus, through these various Medicaid eligibility provisions, some disabled Medicare enrollees may be permanent enrollees in Medicaid (e.g. if they also receive SSI cash assistance) or they may receive medical assistance through Medicaid on a more temporary basis (e.g. if they have substantial health care expenses not covered by Medicare over a short time period). Also, since there is a 24-month waiting period between intitial receipt of DI benefits and entitlement to Medicare, some DI beneficiaries receive Medicaid coverage during the 24-month waiting period. One recent study indicated that about 14 percent of DI beneficiaries had Medicaid coverage during the last six months of the Medicare waiting period.17
Under a provision of the Medicare Catastrophic Coverage Act that was not repealed, disabled Medicare enrollees with incomes below the poverty level (and who are otherwise not eligible for Medicaid) will be universally entitled to limited Medicaid benefits. The Act mandates that effective January 1989 all State Medicaid programs must pay the Medicare Part B premiums, coinsurance and deductibles for all elderly and disabled Medicare enrollees with incomes up to 85% of the poverty threshold (and resources at or below twice the standard used in the SSI program). This mandate will be expanded to include all elderly and disabled persons with incomes up to 100% of poverty by January 1992. For these disabled Medicare enrollees, Medicaid benefits will be limited to payment of Medicare premiums, deductibles and coinsurance requirements; they will not be eligible for other services covered by the State Medicaid plan. This provision also applies to deductibles and coinsurance requirements for outpatient prescription drugs, when that coverage is phased into the Medicare program in January 1991.
Medicaid is always the payer of last resort, so that Medicare provides first payer coverage for all services covered by both programs.
7.8.3 Interaction with other Federal payers
If a disabled person is eligible for health care benefits from both Medicare and from the Veterans' Administration (VA), the VA is generally the first payer. Any service that is authorized by the VA and for which the provider bills the VA directly, the provider must accept the VA's payment as payment in full, and Medicare cannot be billed for any supplementary charges. However, if the provider does not accept the VA's authorization, and the bill is submitted to the VA directly by the disabled veteran, Medicare will pay the difference between the VA payment and the Medicare approved charge, to the extent that the VA payment is less than the Medicare payment would be. Medicare may also pay for services if the disabled veteran chooses to bill Medicare instead of the VA.
For disabled persons who are eligible for health care benefits under both Medicare and CHAMPUS (Civilian Health and Medical Program of the Uniformed Services), Medicare is the primary payer and CHAMPUS generally supplements Medicare by paying the Medicare deductibles and coinsurance amounts, plus any benefits that may be covered by CHAMPUS but not Medicare.
Prior to 1983, Federal employees who were covered both by the Federal Employees Health Benefits Program and by Medicare (due to non-federal work), Medicare was the primary payer. Beginning in 1983, Federal workers began paying the Medicare (HI) payroll tax and, accordingly, becoming eligible for Medicare based on Federal quarters of employment. However, the Federal government health benefits program is now considered an employer group health plan, and for disabled Medicare enrollees who are still covered under the plan, Medicare is now the secondary payer, as discussed in Section 7.7.
7.9 Special Issues
7.9.1 Should the two-year waiting period for Medicare coverage be eliminated or reduced?
The most debated issue in regard to Medicare's coverage of the disabled is undoubtedly the proposed elimination of the two-year waiting period. When Medicare coverage was extended to DI beneficiaries in 1973, the two-year waiting period was enacted primarily to limit program costs. There was an assumption that many disabled workers retain private health insurance coverage after the onset of their disability, and that without a waiting period for Medicare coverage, many of these private health insurance costs would be shifted to Medicare.
In a recent study by the Social Security Administration, it was estimated that elimination of the two-year waiting period for Medicare coverage would result in significantly increased costs to the Medicare trust fund.18 Assuming that Medicare would be the primary payer during the two-year waiting period, the study estimated that the average 10-year cost per disabled beneficiary would increase by 45 percent if the waiting period were eliminated. Thirty percent of the estimated increase was attributable to persons who die within the first two years of their entitlement to SSDI benefits.
A related issue is the degree to which SSDI beneficiaries are covered by some other health insurance plan during their waiting period for Medicare coverage. In a 1982 survey of new disabled-worker beneficiaries who had been receiving DI benefits for at least 18 months, 73 percent of those in the 18-24 month period reported some form of health insurance coverage. About 54 percent reported some private or other coverage, 14 percent reported Medicaid coverage, and about 12 percent reported coverage under CHAMPUS. Twenty-seven percent reported no health insurance coverage.19 Older DI beneficiaries in the two-year waiting period were more likely to have health insurance than younger beneficiaries. The cost of eliminating the two-year waiting period would be much lower if Medicare was not the primary payer during this interval, although concurrent legislation would have to be enacted to prevent private employers and other insurers from reducing their coverage provisions in response to expanded Medicare coverage.
Another proposal has been to eliminate the two-year waiting period for only certain DI beneficiaries with high health care costs, for example, persons with AIDS. This proposal has been opposed by those who believe that such a policy would not be equitable to other DI beneficiaries with equally severe medical conditions and high medical care costs.
7.9.2 Medicare and AIDs
The 24-month waiting period for Medicare coverage is particularly relevant to the issue of health insurance coverage for persons with AIDs. Many persons with AIDs are persons who have achieved insured status under the Social Security program, who become eligible for DI benefits after contracting AIDs and are unable to continue working, but who are left without adequate health insurance coverage while waiting for their entitlement to Medicare. The Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA) required that employers provide employees with the option of purchasing health insurance coverage after leaving their jobs if the employee pays the full group premium, but under present law, this option is only available for up to 18 months after leaving employment. Moreover, the cost of paying the full premium cost of group insurance may be beyond the ability of many persons with AIDs if they are unemployed and relying on DI benefits as their sole source of income. Consequently, many persons with AIDs are incurring catastrophic health care costs related to the care of their illness and becoming eligible for Medicaid after their resources are depleted. Many persons with AIDs also die within the 24-month waiting period without gaining entitlement to Medicare coverage at all.
7.10 Program Data
7.10.1 Current Medicare disabled enrollees, expenditures, and costs.
Estimated FY 1989 data on Medicare disabled enrollees, expenditures, and costs per recipient are presented in Exhibit 7-1. In 1989, the average monthly number of Medicare disabled beneficiaries enrolled in Part A was 3,153,000. Of these, approximately 2,922,000 (93%) were also enrolled in Part B. Disabled Medicare enrollees under age 65 account for about 10% of the total Medicare population. Since Part A mainly provides coverage of inpatient hospital care, only about 25% of Part A disabled enrollees actually used a Part A-covered service, whereas 78% of Part B enrollees had at least one paid claim for a Part B service.
Average annual expenditures per disabled enrollee under Part A was about $1,994, about 15% higher than the average cost per Medicare enrollee over the age of 65, which was $1,727. This is not surprising given that Medicare enrollees under age 65 are, by definition, functionally impaired, whereas most Medicare enrollees over the age of 65 are not. Average Medicare payments under Part B for disabled enrollees were about $1,426, about 20% higher than average Part B payments for aged enrollees. Estimated total expenditures for the Medicare disabled in 1989 were $10.5 billion, about 11% of total Medicare program outlays.
| EXHIBIT 7-1: Estimated Medicare Disabled Enrollees, Users, Costs per Recipient, and Program Expenditures Under Part A and Part B: FY 1989 | ||||
| Enrollees | Users | Costs per Enrollee | Expenditures | |
| Part A | 3,153,000 | 25% | $1,994 | $6.3 billion |
| Part B | 2,922,000 | 78% | $1,426 | $4.2 billion |
| SOURCE: Background Materials and Data on Programs Within the Jurisdiction of the Committee on Ways and Means, 1989 Edition. | ||||
7.10.2 Recent Trends among the Medicare Disabled Population
As would be expected, trends in the Medicare disabled population reflect trends in the SSDI population. The number of Medicare disabled enrollees from 1980 through 1989 is presented in Exhibit 7-2. Reflecting the decline in the number of disabled persons receiving SSDI benefits in the early 1980s, the number of Medicare disabled enrollees also declined slightly, but in recent years the disabled Medicare population has been growing at about an average annual rate of about 2.0 percent, or about 60,000 enrollees per year.
Medicare expenditures for disabled enrollees increased at an average annual compound rate of growth of 10.7% between 1980 and 1987, increasing from $4.5 billion to $9.1 billion. Expenditure data presented in Exhibit 7-2 for FY 1988 and 1989 are estimated, and are subject to revision.
7.10.3 Characteristics of Medicare Disabled Enrollees
The characteristics of the Medicare disabled population are similar to those of the SSDI population (see Section 2.9.3), with the exception that dependents of SSDI disabled workers are not eligible for Medicare benefits, and the Medicare disabled population includes a relatively small number of persons with end-stage renal disease who do not receive SSDI benefits.
Exhibit 7-3 shows the distribution of the Medicare disabled population by major population category. Of approximately 3 million Medicare disabled enrollees in 1987, 79.3% were disabled workers, 16.7% were adult disabled children, 2.5% were disabled widows or widowers, and 1.6% were persons with end-stage renal disease not otherwise eligible for Medicare benefits.20 Almost half (46%) of the Medicare disabled are between the ages of 55 and 64.
| EXHIBIT 7-2: Medicare Disabled Enrollees: 1980 to 1989 | ||||
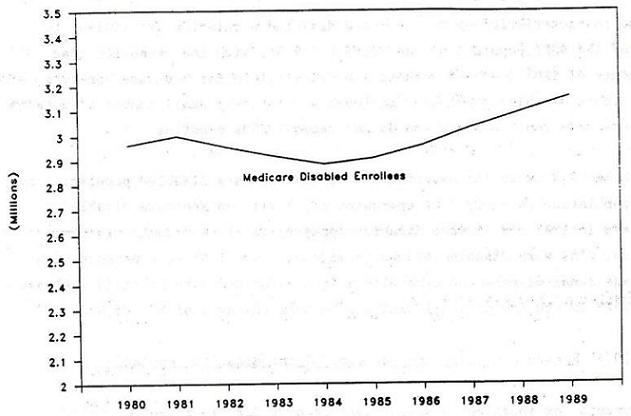 | ||||
| Recipients | Percent Increase | Expenditures (thousands) | Percent Increase | |
| 1980 | 2,963,000 | -- | $4,478,000 | -- |
| 1981 | 2,999,000 | 1.2% | $5,315,000 | 18.7% |
| 1982 | 2,954,000 | -1.5% | $6,172,000 | 16.1% |
| 1983 | 2,918,000 | -1.2% | $6,711,000 | 8.7% |
| 1984 | 2,884,000 | -1.2% | $6,680,000 | -0.5% |
| 1985 | 2,907,000 | 0.8% | $7,495,000 | 12.2% |
| 1986 | 2,959,000 | 1.8% | $8,123,000 | 8.4% |
| 1987 | 3,031,000 | 2.4% | $9,128,000 | 12.4% |
| 1988 | 3,091,000 (est) | 2.0% | $9,460,000 (est) | 3.6% |
| 1989 | 3,153,000 (est) | 2.0% | $10,500,000 (est) | 11.0% |
7.10.4 Medicare utilization patterns of the disabled population
Payments for inpatient hospital care account for 57 percent of total Medicare expenditures for the disabled. Payments to physicians account for 24 percent of expenditures, and outpatient hospital expenditures (including dialysis treatment for end-stage renal disease patients) account for 14 percent. Other Medicare-covered services account for the remaining 5 percent of expenditures. The utilization patterns of the disabled Medicare population are similar to those of the elderly population, except that the disabled are lower utilizers of nursing home and home health services, and higher utilizers of hospital outpatient services.
Persons with end-stage renal disease (ESRD) are a unique sub-group within the total Medicare disabled population. The 126,980 ESRD patients who received Medicare benefits in 1987 represented just 4.1% of the Medicare disabled, but they accounted for $2.5 billion of the $9.1 billion (27.8%) in Medicare expenditures for the disabled in that year. Average Medicare reimbursements per ESRD beneficiary were $19,956 in 1987. The number of ESRD patients more than doubled between 1980 and 1987. In 1987, 8,967 ESRD patients received kidney transplants; Medicare now pays for over 90% of the kidney transplants performed in the United States.
| EXHIBIT 7-3: Distribution of Medicare Disabled Population: 1987 |
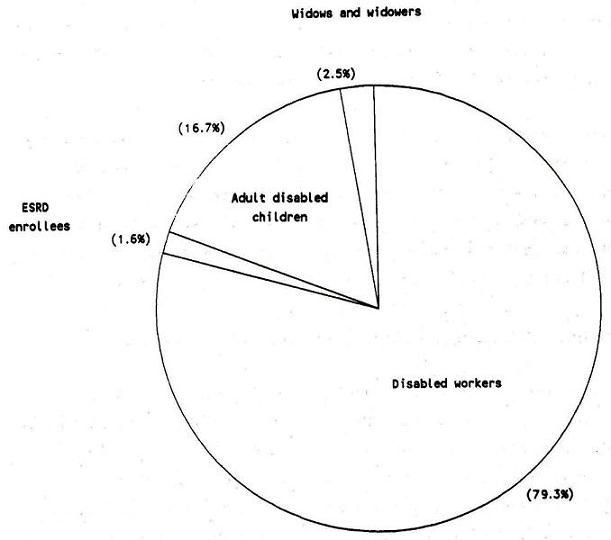 |
CHAPTER 8. MEDICAID COVERAGE OF PERSONS WITH DISABILITIES
8.1 Overview and Purpose
Medicaid is a joint Federal and State entitlement program that provides medical assistance to persons and families with low incomes. Unlike Medicare, which is a Federally-administered program with uniform eligibility rules and benefits nationwide, individual States design and administer their own Medicaid programs within broad Federal guidelines. As a result, there is considerable variation across States with regard to who is eligible to receive medical assistance under Medicaid and with regard the services that are covered by each State Medicaid program.
Another important distinction between Medicare and Medicaid is that Medicaid is a means-tested program designed to provide assistance to persons who are financially needy, while Medicare is a social insurance program based on participation in the workforce. The Medicaid program is extremely complex, and this chapter can only provide a broad overview of how persons with disabilities may receive medical assistance through the program.
In 1989, approximately 24.7 million persons received Medicaid-funded services under the program.21 Of these, about 3.6 million (15%) were eligible for Medicaid on the basis of their disability. However, persons with disabilities account for a much larger proportion of total program expenditures. Approximately $16.5 billion of the estimated $45.1 billion in 1987 Medicaid spending, about 36% of total program expenditures, were payments for services provided to persons with disabilities.
8.2 Authorization, History and Funding
The Medicaid program was originally enacted under Title XIX of the Social Security Amendments of 1965, the same legislation which established the Medicare program. Medicaid was a modification and expansion of several preexisting programs which provided medical payments for certain groups of needy individuals.
Since 1965, the Medicaid program has undergone many legislative changes, particularly in recent years. Eligibility for Medicaid coverage was initially closely linked to eligibility for cash assistance under the Aid to Families with Dependent Children (AFDC) program and the Supplemental Security Income (SSI) program. Although Medicaid eligibility retains strong ties to these two programs, there has been a gradual loosening of these ties to expand Medicaid coverage to other poor persons who do not necessarily receive cash assistance through SSI or AFDC. Another major development in the Medicaid program is that although it was originally enacted, like Medicare, as a health insurance program for acute health care needs, it has now become the nation's primary program or financing long term care services to elderly and disabled individuals. Payments for long term care services account for about half of all Medicaid program spending.
The Medicaid program is jointly financed by the Federal government and by the States. The Federal government's share of State Medicaid payments is known as the Federal Medical Assistance Percentage (FMAP). The FMAP is recalculated annually and is related to State per capita income, such that poorer States receive a higher FMAP than wealthier States. FMAP rates for FY 1989 are presented in Exhibit 8-1. In 1987, the Federal government paid 55.6% of all paid Medicaid claims to service vendors. The Federal government also pays for 50 percent of all State Medicaid administrative costs, although higher rates are applicable for specific administrative activities.
The non-Federal portion of State Medicaid payments can be financed entirely through State funds, or, alternatively States may require local governments to participate in Medicaid program financing. In 1986, fourteen States required some local funding of Medicaid program costs.
| EXHIBIT 8-1: Federal Medical Assistance Percentages: FY 1989 | |||
| Alabama | 73.10 | Missouri | 59.96 |
| Alaska | 50.00 | Montana | 70.62 |
| Arizona | 62.04 | Nebraska | 60.37 |
| Arkansas | 74.14 | Nevada | 50.00 |
| California | 50.00 | New Hampshire | 50.00 |
| Colorado | 50.00 | New Jersey | 50.00 |
| Connecticut | 50.00 | New Mexico | 71.54 |
| Delaware | 52.60 | New York | 50.00 |
| Dist. of Columbia | 50.00 | North Carolina | 68.01 |
| Florida | 55.18 | North Dakota | 66.53 |
| Georgia | 62.78 | Ohio | 58.98 |
| Hawaii | 53.99 | Oklahoma | 66.06 |
| Idaho | 72.71 | Oregon | 62.44 |
| Illinois | 50.00 | Pennsylvania | 57.42 |
| Indiana | 63.71 | Rhode Island | 55.88 |
| Iowa | 62.95 | South Carolina | 73.08 |
| Kansas | 54.93 | South Dakota | 71.02 |
| Kentucky | 72.89 | Tennessee | 70.17 |
| Louisiana | 71.07 | Texas | 59.04 |
| Maine | 66.68 | Utah | 73.86 |
| Maryland | 50.00 | Vermont | 63.92 |
| Massachusetts | 50.00 | Virginia | 51.20 |
| Michigan | 54.75 | Washington | 53.06 |
| Minnesota | 53.07 | West Virginia | 76.14 |
| Mississippi | 79.80 | Wisconsin | 59.31 |
| Wyoming | 62.61 | ||
8.3 Definition of Disability
The definition of disability used in determining eligibility for Medicaid is the same definition employed by the Social Security Administration in determining eligibility for SSDI, SSI and Medicare. Most disabled persons receiving Medicaid coverage do so on the basis of their receipt of cash assistance under the SSI program, and have therefore been determined disabled by their State Disability Determination Service (DDS). Disabled persons who do not receive SSI cash assistance due to excess income and/or resources, but who nonetheless may be eligible for Medicaid coverage under other eligibility provisions must also be determined disabled by the same process.22
Three State Medicaid programs, however, employ more restrictive disability criteria in determining eligibility for Medicaid than are used in determining eligibility for SSI. These States--Indiana, Missouri, and New Hampshire--are allowed to do so under the so-called "Section 209(b)" Medicaid program option. Indiana and New Hampshire require that a disability be "permanent and total" and Missouri and New Hampshire do not extend Medicaid coverage to children under age 18, even though they may be receiving SSI benefits as disabled children.
One definition of disability relates to that definition used to determine who is eligible for coverage under the Medicaid program. As in Medicare, however, other definitions of disability or impairment are often used in determining whether Medicaid enrollees are eligible to receive specific types of services. State Medicaid programs may use functional criteria for coverage of nursing home services, home health services, personal care services, home and community-based waiver services, and other Medicaid-covered services. Thus, two levels of disability criteria are applied--one in determining eligibility for the Medicaid program in general, and one used in determining eligibility for specific covered services.
8.4 Administrative Structure
Each State designates a single agency to administer its Medicaid program under the general oversight of the Health Care Financing Administration (HCFA) in the Department of Health and Human Services. The responsibilities of the single State agency include: eligibility determinations, certification of Medicaid providers, payment of Medicaid claims, review and inspection of facilities providing care, as well as maintaining the overall integrity and administration of the Medicaid program.
Congress and HCFA also play important roles in the administration of the Medicaid program. Although individual States have a good deal of flexibility in the design and operation of their Medicaid programs, the Federal government still establishes the broader parameters of Medicaid program policy. Federal law determines which groups of persons States must and may cover, at their option, as well as what services States must and may provide to Medicaid beneficiaries.23 The Federal government, through law and regulation, provides broad definitions of Medicaid-covered services, and also minimum standards for Medicaid providers and the services they provide. HCFA conducts various monitoring activities of State Medicaid programs to ensure that they are administering the program in compliance with Federal law and regulations.
8.5 Eligibility
Medicaid eligibility policy is extremely complex and varies from State to State. Persons with comparable disabilities and in equal financial circumstances can be eligible for Medicaid in one State but not in another. While this section cannot possibly provide a detailed explanation of Medicaid eligibility policy, and its various pertubations from State to State, it will attempt to provide an overview of how persons with disabilities can become eligible for medical assistance under various State Medicaid program options.
In all cases, persons who receive Medicaid coverage must meet both categorical and financial eligibility criteria. Categorical criteria refer to the various groups of persons who are potentially eligible for Medicaid, while financial criteria refer to the level of financial need which is used in determining eligibility. Since disabled persons (defined as persons who pass the DDS disability determination process) are a mandated categorical group, disabled persons of any age are potentially eligible for Medicaid if they meet the State's financial eligibility criteria.
8.5.1 SSI eligibility links to Medicaid
Most disabled persons are eligible for Medicaid by virtue of their receipt of cash assistance from SSI and/or optional State supplementation (SSP). Almost four of five (79%) disabled persons on Medicaid receive SSI/SSP cash assistance. As discussed in Chapter 3, however, a disabled person's eligibility for SSI/SSP is related to the income level at which States set their optional supplementation standards. Thus, eligibility for Medicaid is, in part, related to the characteristics of each State's optional supplementation program.
| EXHIBIT 8-2: Medicaid Coverage Options for Disabled Individuals | ||||||||
| 1634 State | 209(b) State | SeparateState Application | SSI/SSP Standard (1989) | Medically NeedyProgram | Medically Needy Income Levelfor Individual(1989) | Separate Income Level forthe Disabled | TEFRA Option for DisabledChildren | |
| Alabama | X | $368 | ||||||
| Alaska | X | 685 | ||||||
| Arizona | X | 368 | ||||||
| Arkansas | X | 368 | X | $108 | X | |||
| California | X | 602 | X | 575 | ||||
| Colorado | X | 426 | ||||||
| Connecticut | X | 752 | X | 434 | X | |||
| Delaware | X | 368 | ||||||
| Dist. Col. | X | 383 | X | 362 | X | X | ||
| Florida | X | 368 | X | 300 | X | |||
| Georgia | X | 368 | X | 200 | X | |||
| Hawaii | X | 373 | X | 332 | X | |||
| Idaho | X | 441 | X | |||||
| Illinois | X | NA | X | 267 | ||||
| Indiana | X | 368 | ||||||
| Iowa | X | 368 | X | 450 | ||||
| Kansas | X | 368 | X | 368 | ||||
| Kentucky | X | 368 | X | 208 | ||||
| Louisiana | X | 368 | X | 100 | ||||
| Maine | X | 378 | X | 400 | X | |||
| Maryland | X | 368 | X | 359 | ||||
| Massachusetts | X | 497 | X | 469 | X | |||
| Michigan | X | 398 | X | 385 | ||||
| Minnesota | X | 403 | X | 466 | ||||
| Mississippi | X | 368 | ||||||
| Missouri | X | 368 | ||||||
| Montana | X | 368 | X | 368 | X | |||
| Nebraska | X | 406 | X | 392 | X | |||
| Nevada | X | 404 | X | |||||
| New Hampshire | X | 395 | X | 382 | ||||
| New Jersey | X | 399 | X | 350 | X | |||
| New Mexico | X | 368 | ||||||
| New York | X | 454 | X | 459 | ||||
| North Carolina | X | 368 | X | 242 | X | |||
| North Dakota | X | 368 | X | 345 | ||||
| Ohio | X | 368 | ||||||
| Oklahoma | X | 432 | X | 275 | X | |||
| Oregon | X | 370 | X | 374 | X | |||
| Pennsylvania | X | 400 | X | 392 | X | |||
| Rhode Island | X | 429 | X | 525 | X | |||
| South Carolina | X | 368 | ||||||
| South Dakota | X | 383 | X | |||||
| Tennessee | X | 368 | 167 | |||||
| Texas | X | 368 | X | 100 | ||||
| Utah | X | 377 | X | 289 | X | |||
| Vermont | X | 428 | X | 708 | X | |||
| Virginia | X | 368 | X | 250 | ||||
| Washington | X | 396 | X | 396 | X | |||
| West Virginia | X | 368 | X | 200 | X | |||
| Wisconsin | X | 471 | X | 471 | X | |||
| Wyoming | X | 388 | ||||||
Not all disabled persons who receive SSI or optional State supplementation payments are necessarily eligible for Medicaid, however. State Medicaid programs have three options with regard to extending Medicaid eligibility Medicaid to SSI recipients. Under the "Section 1634" option, SSI recipients are automatically enrolled in Medicaid, without having to make a separate application. As shown in Exhibit 8-2, thirty States have elected this option. Under the second option, SSI recipients are automatically eligible for Medicaid, but they must make a separate application to the State agency which administers the Medicaid program. Six States (Alaska, Idaho, Kansas, Mississippi, Nevada and Oregon) have elected this option.
Under the third and most restrictive option, referred to as the Section "209(b)" option, States may impose more restrictive eligibility criteria for Medicaid than are used in determining eligibility for SSI, as long as the criteria were used in the State Medicaid program prior to 1972 (when the SSI program was enacted). States may impose more restrictive criteria in determining disability, and/or more restrictive income and assets criteria. As previously discussed, three States (Indiana, Missouri, and New Hampshire) have elected to apply more restrictive definitions of disability in determining eligibility for Medicaid than are used for SSI eligibility determinations. Eleven other "209(b)" States (Connecticut, Hawaii, Illinois, Minnesota, Nebraska, North Carolina, North Dakota, Ohio, Oklahoma, Utah, and Virginia) used the same definition of disability, but employ more restrictive financial criteria than SSI in determining Medicaid eligibility.
8.5.2 Medicaid eligibility of persons not receiving SSI/SSP
For disabled persons who do not receive SSI or optional State supplementation payments, there are a number of Medicaid program options which extend eligibility to the "non-cash" disabled. Approximately 20% of all categorically-related disabled persons receiving Medicaid do not receive SSI cash assistance and are eligible for Medicaid under these other program options. The most common eligibility provisions under which these disabled persons qualify for Medicaid are:
Medically Needy Programs. Thirty-six (36) States extend Medicaid coverage to certain "medically needy" individuals whose income and/or resources exceed the levels established for SSI/SSP cash assistance, but who nonetheless require medical assistance. States which have elected to cover the medically needy establish income and resource standards for these recipients which are different from those used in determining eligibility for SSI. However, by Federal law, the medically needy income standard cannot exceed 133% of the State AFDC income standard for a similarly sized family. Further, individuals with incomes above the medically needy standard may reduce his or her income to the requisite level through eligible deductions for medical care. This process is called "spending-down." For example, if an individual's countable income is $500, and the State's medically needy income standard is $400, the individual would be required to incur $100 in medical care costs (i.e. the spend-down) prior to establishing eligibility for Medicaid. Once a medically needy applicant meets his or her spend-down obligation (the difference between the medically needy income standard and the person's monthly countable income), he or she becomes eligible for Medicaid for the remainder the eligibility period.24
Special Income Levels for the Institutionalized. The SSI benefit standard for persons in Medicaid-certified institutions is just $30, so States may extend Medicaid eligibility to persons in institutions with incomes which do not exceed a special income level. This income level, established by the State, cannot exceed 300% of the Federal SSI benefit level. In 1989, the maximum level was $1,104 (3 x $368) per month. For persons with incomes up to the special income level, this provision works like a medically needy spend-down for the institutionalized: recipients must contribute all income in excess of the SSI personal needs allowance of $30 per month towards the cost of their care, after which Medicaid pays the balance of the bill (up to the Medicaid-approved rate). States which do not have a medically needy program use this provision to provide medical assistance to persons in nursing homes who have some income, but not sufficient income to pay for their own nursing home care. Many persons who receive SSI cash assistance prior to nursing home admission lose their eligibility for SSI upon admission (because their income exceeds the SSI institutional benefit standard of $30 per month) but remain eligible for Medicaid as "non-cash" recipients under this provision.
Higher Income Levels for the Aped and Disabled. Under the Omnibus Budget Reconciliation Act of 1986, States were authorized to establish Medicaid eligibility income levels for the aged and disabled up to 100 percent of the Federal poverty level, effective July 1, 1987. This provision marked the first time that States could establish Medicaid eligibility levels that were not tied to benefit standards used in their SSI/SSP or AFDC programs. As of July 1989, two States and the District of Columbia had elected to establish higher Medicaid eligibility levels for the aged and disabled under this option: the District of Columbia and New Jersey had established their income levels at 100 percent of the poverty level, while Florida had set its income level at 90 percent of the poverty level.
Optional Coverage of Noninstitutionalized Disabled Children. This provision allows States to extend Medicaid eligibility to certain disabled children who would otherwise not be eligible for Medicaid due to the deeming of parental income and resources.25 Under a Medicaid program modification enacted in 1982, States may waive Medicaid deeming rules for disabled children who meet the following conditions:
- the child would be eligible for Medicaid if institutionalized;
- the child meets the State's Level of Care criteria for hospital care, nursing home care, or ICF-MR (Intermediate Care Facility for the Mentally Retarded) care;
- the child can be appropriately cared for outside of an institutional setting; and
- the estimated cost of care at home is no more than the estimated cost of institutional care.
This provision essentially allows States to extend Medicaid eligibility to all disabled children, regardless of family income status, as long as their disabilities are severe enough to qualify for institutional placement. As of July 1989, 19 States and the District of Columbia had elected to use this option to extend Medicaid eligibility to certain disabled children.
Expanded Eligibility Options under the Section 2176 Home and Community-Based Care Medicaid Waiver Program. Under the Omnibus Budget Reconciliation Act of 1981, States were authorized to apply for special Medicaid waivers to provide coverage of home and community-based services not otherwise included in the State Medicaid plan for persons at risk of institutional placement. Although the major provision of these waivers is an expansion in Medicaid service benefits, not an expansion in Medicaid eligibility, States may also apply special Medicaid eligibility provisions in their Section 2176 Medicaid waiver programs. These eligibility provisions include: (1) waiving Medicaid deeming rules for persons who are otherwise eligible for waiver services; and (2) applying the institutional "special income level" in determining the financial eligibility of waiver applicants. Thus, certain disabled persons living in non-institutional settings may become eligible for Medicaid under these special waiver program options if they would have been eligible for Medicaid upon entering an institution. Not only are these persons eligible for the benefit package provided for under the regular State Medicaid plan, but they are also eligible for the supplemental home and community-based "waiver" services provided under this Medicaid program option.
Section 1619 Recipients. Under the provisions of Section 1619(a) and 1619(b) of the Social Security Act, disabled SSI recipients who enter the work force are eligible for continued SSI benefits and Medicaid eligibility status as long as there is not a medical improvement in their disabling condition. Under Section 1619(a), disabled persons with earnings can continue to receive SSI benefits as long as their countable earnings fall below the so-called "breakeven point." Disabled recipients with earnings above this level can continue to be eligible for Medicaid benefits even after they no longer receive SSI benefits. In December 1987, there were 15,632 former SSI recipients receiving special Medicaid benefits under Section 1619(b).
Thus, there are a number of Medicaid program options through which disabled persons who are not eligible for SSI cash assistance can nonetheless qualify for Medicaid coverage as "non-cash" recipients. There are a number of other relatively minor program provisions which extend Medicaid eligibility to certain disabled persons not receiving SSI benefits, but they apply to relatively few persons. For example, disabled SSI recipients who lose their benefits because they become eligible for SSDI benefits as Adult Disabled Children (and their SSDI benefits exceed the SSI benefit standard) retain their eligibility for Medicaid benefits despite losing SSI.
A new Medicaid provision also extends limited Medicaid benefits to certain disabled persons who are not otherwise eligible for Medicaid coverage. Under a provision of the Medicare Catastrophic Coverage Act of 1988 which was not subsequently repealed, States are required to pay Medicare Part B premiums, deductibles and coinsurance for disabled Medicare enrollees whose incomes are at or below the Federal poverty level and whose resources are at or below twice the SSI resource standard (in 1989, the SSI resource standard was $2,000 for an individual). This provision applies to disabled Medicare enrollees under age 65 whose incomes and/or resources are too high to qualify them for Medicaid coverage, but who are still living at or below the poverty level. The provision is being phased in gradually: effective January 1989, States were required to implement "buy-in" coverage for disabled Medicare enrollees with incomes at or below 85 percent of poverty. This limit will be gradually raised to 100 percent of the poverty level between 1989 and 1992.
In 1989, it is estimated that there were about 3.2 million disabled Medicare beneficiaries, of which about 25-30% were already enrolled in the Medicaid program. It is difficult to estimate how many of the remaining 2.2 million disabled Medicare enrollees who are not currently eligible for Medicaid qualify for these "buy-in" benefits. Note that these persons are not eligible for the full Medicaid benefit package; Medicaid only pays for their Medicare Part B premiums, deductibles, and coinsurance.
8.6 Medicaid Services
As in Medicaid eligibility, in which there are both mandatory and optional groups of Medicaid beneficiaries, there are also both mandatory and optional services which States can provide in their Medicaid benefit packages. Further, States have considerable flexibility in regard to the amount, scope and duration of the Medicaid benefits they elect to provide. For example, a State may place limits on the number of inpatient hospital days it will cover over a certain period, or a limit on the number of physician visits it will pay per beneficiary. However, all services must be equal in amount, duration and scope to all beneficiaries within an eligibility group, they must be available on a statewide basis, and Medicaid beneficiaries must be allowed freedom-of-choice in selecting from whom they obtain Medicaid-funded services.
Mandatory services which all States must provide include:
- inpatient hospital services;
- outpatient hospital services;
- rural health clinic services
- other laboratory and X-ray services;
- skilled nursing facility (SNF) services;
- early and periodic screening, diagnosis, and treatment (EPSDT) services for individuals under age 21;
- physician services;
- home health services for persons requiring skilled nursing care; and
- nurse-midwife services (in States where nurse midwives are authorized to practice under State law).
In addition to these mandatory services, States may offer Medicaid coverage for a broad array of optional services in their State plans. These services include:
- podiatrists' services
- optometrists' services
- chiropractors' services
- other practitioner services
- private duty nursing
- clinic services
- dental services
- physical therapy
- speech, hearing, and language therapies
- prescribed drugs
- dentures
- prosthetic devices
- eyeglasses
- diagnostic services
- screening services
- preventive services
- rehabilitative services
- services for persons age 65 and over in mental institutions
- intermediate care facility (ICF) services
- intermediate care facility for the mentally retarded (ICF-MR) services
- inpatient psychiatric services for persons under age 22
- Christian Science nurses
- Christian Science sanitoria
- SNF services for persons under age 21
- emergency hospital services
- personal care services
- transportation services
- case management services, and
- hospice services
With regard to the amount, duration and scope of both optional and mandatory services, States have the option of offering a more restrictive benefit package for the medically needy than they offer for the categorically needy. Thus, disabled Medicaid beneficiaries who qualify under one of the "non-cash" eligibility options may not be entitled to the same set of Medicaid services as an SSI cash recipient. Of the 35 States which had medically needy programs in 1986, 27 States offered the same benefit package for mandatory Medicaid services to the medically needy as they did to the categorically needy, and 23 offered the same benefit package for optional services.
Providers who agree to participate in the Medicaid program are required to accept Medicaid reimbursements as "payment in full" for the services they provide. Unlike Medicare providers, they cannot bill Medicaid recipients for additional charges above and beyond the amount they are reimbursed by Medicaid. However, States can impose "nominal" copayments for certain Medicaid services, as a utilization control measure. In general, copayments cannot exceed $3.00 per service per month. States cannot impose copayments on services provided to children or for pregnancy-related services.
8.7 Recent Legislative Changes
The Medicaid program has been subject to considerable legislative change during the 1980s, and it is not possible to summarize all of the changes in this brief program description. Many of the changes did not affect persons with disabling conditions at all. However, some of the changes which did apply to the Medicaid disabled population are summarized below:
The Section 1619 program. Initially enacted on a demonstration basis in 1981, and eventually made permanent in 1987, Section 1619 ensured that any disabled person receiving SSI benefits could enter the workforce and not be in danger of losing health insurance benefits under Medicaid as long as there was no improvement in his or her medical condition.
Medicaid Home and Community-Based Care Waiver Program. Enacted in 1981, the Medicaid waiver program provides alternative home and community-based services to aged and disabled persons who might otherwise only be able to access Medicaid-funded long term care services by entering an institution.
TEFRA Section 134 Option for Disabled Children. Sometimes referred to as the "Katie Beckett" option after the disabled child whose case initially led to this policy change, this option, enacted in 1982, allows States to waive Medicaid deeming rules for certain disabled children living at home who would otherwise only be eligible for Medicaid in an institutional setting (see Section 8.5.2).
Optional income levels for the aged and disabled. OBRA 1986 allowed States to establish Medicaid eligibility income levels for the aged and disabled that are separate from income levels used in establishing eligibility for SSI/SSP benefits. Under this option, income levels for SSI-related applicants can be set anywhere up to the Federal poverty level for a comparably-sized household.
Mandated Medicaid buy-in for disabled Medicare enrollees living below the poverty level. The Medicare Catastrophic Coverage Act of 1988 mandated that State Medicaid programs pay for ("buy-in") the Medicare premiums, deductibles, and coinsurance for all Medicare disabled enrollees living at or below the poverty threshold. This provision is being phased in between 1989 and 1992.
Protection of income and resources of spouses of institutionalized Medicaid recipients. The Medicare Catastrophic Coverage Act also provided increased protection for the non-institutionalized spouses of Medicaid recipients in nursing homes and other institutional settings. Prior to enactment of this provision, non-institutionalized spouses could be left destitute if all of the couple's income and assets were held in the name of the institutionalized spouse.
Mandated preadmission screening of mentally ill and mentally retarded persons for nursing home placement. OBRA 1987 mandated that all States implement nursing home preadmission screening programs to identify nursing home applicants with a primary medical diagnosis of mental illness or mental retardation. Persons with such a diagnosis, who do not need the level of care provided in a nursing home, are to be diverted elsewhere. Current residents of nursing homes who are mentally ill or mentally retarded must also be given the choice of alternative placement in the community.
8.8 Program Interactions
8.8.1 Medicaid and SSI
Medicaid eligibility for persons with disabilities is closely tied to eligibility for SSI cash assistance, as previously discussed. Except in so-called "Section 209(b)" States, disabled persons who receive SSI benefits are automatically eligible for Medicaid coverage. In some States, disabled SSI beneficiaries are automatically enrolled in Medicaid; in others they must make a separate application (see Section 8.5).
8.8.2 Medicaid and SSDI
SSDI beneficiaries are not necessarily eligible for Medicaid, but many SSDI beneficiaries nonetheless are. Some are eligible because they receive both SSDI and SSI. Others only receive SSDI, but qualify for Medicaid coverage as "non-cash" recipients under medically needy programs or other Medicaid program options.
8.8.3 Medicaid and Medicare
Persons who receive both SSDI and SSI benefits as disabled are generally eligible for both Medicaid and Medicare coverage (unless they are in the two-year waiting period for Medicare). These persons are often referred to as "dual enrollees." When persons are covered by both Medicare and Medicaid, Medicare is always the first payer; Medicaid covers the premiums, deductibles and coinsurance amounts for services covered under both programs (e.g. inpatient hospital care). However, the Medicaid benefit package in most States is much broader than the Medicare benefit package, and therefore Medicaid is often the first and only payer of other covered services, such as nursing home care and prescription drugs.
8.8.4 Coordination with other payment sources
Medicaid is almost always the payer of last resort. Medicaid applicants are required to disclose any insurance coverage or other potential third party payment source at the time of their application, and all State Medicaid programs are required to have a system for pursuing third party claims. These systems may include data exchanges with workers' compensation boards or State motor vehicle accident report files. States must also have systems for collecting medical support payments from absent parents.
8.8.5 Medicaid and the Indian Health Service
An exception to the rule of Medicaid being the payer of last resort occurs in the case of Native Americans who receive services through the Indian Health Services (IHS), and who are also eligible for Medicaid. In the case of services provided in IHS facilities to Medicaid-eligible Native Americans, IHS bills Medicaid directly, and Federal matching funds for services provided in IHS facilities are reimbursable at a matching rate of 100 percent.
8.9 Special Issues
This section discusses Medicaid policy issues which specifically relate to the coverage of persons who are categorically eligible as disabled.
8.9.1 Variations in access to Medicaid coverage across States
The flexibility offered States in designing their own Medicaid eligibility and service coverage policies has led to wide variation across States in providing access to Medicaid-covered services for low income persons with disabilities. Some States have relatively broad coverage of persons with disabilities, others relatively restrictive coverage. A disabled person in one State may have health insurance coverage under Medicaid, while a disabled person in the same financial circumstances may be left without any health insurance coverage at all. Some of the factors which lead to variations in coverage across States include:
- The method by which States elect to extend Medicaid coverage for persons receiving SSI/SSP cash assistance, including the Section 209(b) option to impose more restrictive criteria than are used in SSI;
- Variations in benefit standards used for optional State supplementation programs;
- Whether a State has elected to have a medically needy program, and, if so, the income and asset levels used in determining Medicaid eligibility for the medically needy;
- Only a few States have elected to use a higher income level in determining Medicaid eligibility for SSI-related recipients, as authorized in OBRA 1986, than is used in determining eligibility for SSI/SSP; and
- States vary in the degree to which they have used Medicaid home and community-based care waivers and the 1982 TEFRA option to extend Medicaid eligibility to disabled persons in the community who would otherwise only be able to access Medicaid coverage through institutionalization.
Although State flexibility in Medicaid eligibility and service coverage policy has always been a key component of the Medicaid program, there is also concern about inequities across States in the degree to which low-income persons are provided health insurance coverage under Medicaid. To address access inequities, there are those who believe that the Federal government should mandate more uniform Medicaid eligibility policies nationwide.
8.9.2 Bias Towards Institutional Coverage
The Medicaid program has long been criticized for having an inherent bias towards institutional coverage for elderly and disabled persons with long term care needs. In most States, Medicaid-eligible persons with severe disabilities, who may require continuous care and supervision, can more easily access the services they need in institutional settings, such as nursing homes and ICFs-MR, than in community-based settings. A number of Medicaid policy changes in recent years have attempted to counter this bias in Medicaid service coverage policy, such as the 1982 TEFRA option for disabled children, and the Section 2176 Medicaid home and community-based waiver program. However, coverage of non-medical home and community-based services for persons with long term care needs is still highly restricted under Medicaid. There is considerable momentum to provide States the option of coveraging a broad array of non-institutional home and community-based services under Medicaid without restrictions. At the same time, there is concern about the fiscal impact this policy change would have on Medicaid program expenditures, given that most disabled persons with long-term care needs do not live in institutional settings.
8.9.3 Exclusion of Long-Term Care Coverage for Disabled Persons with Chronic Mental Illness
Although Medicaid provides institutional long term care coverage for all other persons under age 65 with severe disabilities, the program generally excludes institutional coverage for disabled persons with chronic mental illness. While the enactment of the ICF-MR (Intermediate Care Facility for the Mentally Retarded) benefit in 1971 allowed States to receive Federal Financial Participation (FFP) under Medicaid for the costs of operating their public institutions for the mentally retarded (provided the institutions met Federal certification standards), a similar option has never been enacted to include public institutions for the mentally ill in the Medicaid program. Thus, State mental hospitals and other residential facilities which serve the chronically mentally ill are generally not financed by the Medicaid program. In fact, if any Medicaid-certified facility, such as a nursing home, is found to serve a population in which more than 50% of the residents have a primary diagnosis of mental illness, the facility is classified as an Institution for Mental Diseases (IMD) and loses eligibility for Medicaid reimbursement.
Under the provisions of OBRA 1987, States are also required to establish preadmission screening programs designed to prevent the inappropriate placement of persons with mental illness in nursing homes. Under this law, States are also required to offer mentally ill persons currently in nursing homes the opportunity to live in an alternative residential environment more appropriate to their needs.
8.9.4 Medicaid and AIDS
Medicaid is an important source of health insurance coverage for persons with AIDS. Both the total health care costs of treating persons with AIDS, and the percentage of those costs paid by Medicaid are difficult to estimate. The office of the Actuary at HCFA estimates that Medicaid will pay for about half of all health costs for AIDS patients in 1991. However, there are indications that many private insurers are implementing underwriting policies to limit their exposure to the costs of treating persons with AIDS by screening out persons with AIDS or persons infected with the AIDS virus at the time of application for health insurance coverage and by imposing restrictions on coverage of AIDS-related cases. It is also important to remember that persons with AIDS who become disabled and thereby eligible for Social Security disability insurance are not eligible for Medicare coverage until two years after their initial receipt of disability benefits. Consequently, many persons with AIDS who become disabled and unable to work are left without any health insurance coverage whatsoever, and may qualify for Medicaid after spending down their available income and assets.
AIDS patients can qualify for Medicaid coverage in one of three ways. First, some persons who develop AIDS, particularly IV drug-users, may already be receiving cash assistance through SSI or AFDC prior to contracting AIDS, and are therefore already eligible for Medicaid. Second, some AIDS victims may become impoverished as a result of their disease, and qualify for SSI cash assistance after their diagnosis. Third, other persons with AIDS may continue to be able to work, or may continue to have income which disqualifies them for SSI benefits, but have high medical expenses which cause them to become eligible for Medicaid under the medically needy "spend down" provisions.
Under a special ruling, AIDS victims who apply for SSI benefits can begin to receive benefits, and therefore Medicaid, under a "presumptive eligibility" process which expedites their eligibility for benefits. Persons with a medically confirmed diagnosis of AIDS can automatically begin receiving SSI and Medicaid under this process while the formal determination of their disabled status is being made. This special provision does not apply to persons with AIDS-related complex (ARC) who do not have the more narrowly defined diagnosis of AIDS.
It is recognized that the costs of treating persons with AIDS will not affect all State Medicaid programs equally. The two States with by far the largest numbers of persons with AIDS are California and New York. These States are not only grappling with the problem of covering the potential costs of caring for AIDS patients in their Medicaid populations, but also the most appropriate service approaches to providing care. Many AIDS patients are being inappropriately treated in inpatient hospital settings for extended periods of time. Alternative service approaches, such as specialized nursing homes, hospice programs, and home and community-based waiver programs, are currently under development in several States.
8.10 Program Data
8.10.1 Current Medicaid disabled recipients, expenditures, and costs per recipient
In 1989, there were approximately 3,471,000 persons eligible for Medicaid on the basis of disability who received at least one Medicaid-funded service.26 Another 95,000 Medicaid recipients were eligible on the basis of blindness. Together, these two populations accounted for about 14 percent of the 24.7 million Medicaid recipients in 1989.
In terms of expenditures, the Medicaid disabled population account for a much larger share of program spending. In 1987, Medicaid payments made for services provided to the disabled totalled $16.5 billion, about 36 percent of the $45.1 billion in total Medicaid program expenditures for that year. Of this total, the Federal government paid about $9.2 billion (56 percent), while the State share of Medicaid costs for the disabled totalled $7.3 billion (44 percent).
In 1987, the average annual cost per Medicaid disabled recipient was $4,986, the highest of any major eligibility group in Medicaid.
8.10.2 Distribution of Medicaid expenditures for the disabled
Exhibit 8-3 presents the distribution of Medicaid expenditures for the disabled in FY 1987. Almost half (46.3%) of all Medicaid spending for the disabled was for institutional long term care services, either in ICF-MR certified facilities or in nursing homes. ICF-MR care alone accounted for 31.5 percent of total Medicaid spending for the disabled, although the 149,000 recipients of ICF-MR care represented only about 4.5 percent of the entire Medicaid disabled population. In 1987, the average annual cost per recipient of ICF-MR care was $37,630. Another 229,000 disabled Medicaid recipients received care in ICF-certified and SNF-certified facilities in 1987, at a cost of about $2.4 billion.
Disabled persons on Medicaid are high users of prescription drugs. In 1987, about 78% of all Medicaid disabled recipients had at least one claim for prescription drugs, and among users, the average annual cost of prescription drug use per disabled recipient was $449.
| EXHIBIT 8-3: Distribution of Medicaid Expenditures for the Disabled: 1987 | |
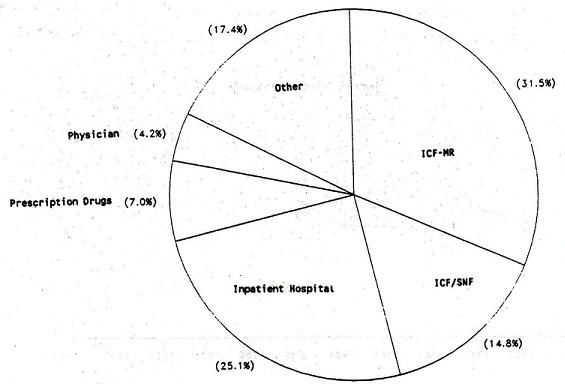 | |
| Service | Expenditures (millions) |
| ICF-MR | $5,188 |
| ICF/SNF | 2,430 |
| Inpatient Hospital | 4,123 |
| Prescription Drugs | 1,148 |
| Physician | 696 |
| Other | 2,865 |
| Total | $16,450 |
8.10.3 Recent Trends Among the Medicaid Disabled Population
Exhibit 8-4 shows the growth of the Medicaid disabled population between 1980 and 1989 (data for 1988 and 1989 are estimated). Reflecting tends in the SSI program (see Chapter 3), there was little or no growth in the number of recipients in the early 1980s, but since 1984, there has been continuous growth in the number of recipients at a rate of about 5 percent per year.
Medicaid expenditures for the disabled increased from $7.5 billion in 1980 to $16.5 billion in 1987, an average annual compound rate of growth (ACRG) of 11.9 percent.
| EXHIBIT 8-4: Medicaid Disabled Recipients: 1980 - 1987 | ||||
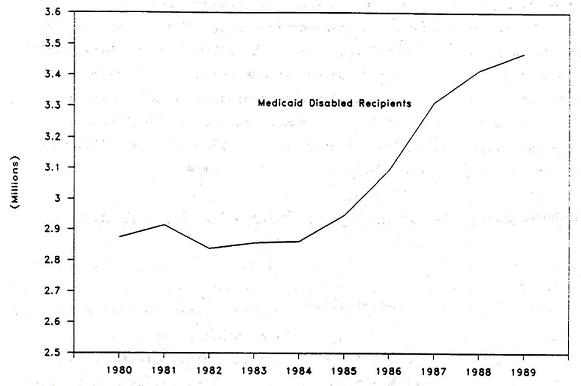 | ||||
| MedicaidDisabled Recipients | Percent Increase | MedicaidDisabled Expenditures | Percent Increase | |
| 1980 | 2,874,447 | -- | $7,493,381,996 | -- |
| 1981 | 2,914,208 | 1.4% | $9,296,838,006 | 24.1% |
| 1982 | 2,837,909 | -2.6% | $10,228,049,379 | 10.0% |
| 1983 | 2,855,936 | 0.6% | $11,176,500,351 | 9.3% |
| 1984 | 2,860,630 | 0.2% | $11,695,973,503 | 4.6% |
| 1985 | 2,947,064 | 3.0% | $13,203,217,927 | 12.9% |
| 1986 | 3,093,873 | 5.0% | $14,578,763,375 | 10.4% |
| 1987 | 3,310,066 | 7.0% | $16,442,194,549 | 12.8% |
| 1988 | 3,415,000 (est.) | 3.2% | NA | |
| 1989 | 3,471,000 (est.) | 1.6% | NA | |
8.10.4 Medicaid Disabled Recipients by Institutional Status and Cash Assistance Status
Exhibit 8-5 presents a distribution of the Medicaid disabled population by institutional status and cash assistance status in FY 1987. Almost three-fourths of the Medicaid disabled population are SSI cash recipients who do not receive institutional long term care in ICFs-MR, SNFs, or ICFs. About 12 percent of the population are institutionalized for at least part of the year.27 The number of institutionalized recipients declined between 1980 and 1987.
About 15 percent of the Medicaid disabled are non-institutionalized non-cash recipients, who are eligible for Medicaid under one of the eligibility options discussed in Section 8.5 for persons not receiving SSI cash assistance. Trends in the number of non-institutionalized non-cash recipients are an important indicator of the degree to which Medicaid is providing health insurance coverage for low-income disabled persons who for one reason or another, do not receive SSI benefits, but who nonetheless require medical assistance. As shown in Exhibit 8-5, the number of non-institutionalized non-cash recipients increased from about 345,000 in 1980 to about 475,000 in 1987, an average ACRG of 4.6 percent.
8.10.5 Age and Sex Characteristics of Medicaid Disabled Recipients
Since most Medicaid disabled recipients are also SSI disabled recipients, the age and sex characteristics of the two populations are similar (see Section 3.10.3). Approximately 10% of the Medicaid disabled population are SSI children under the age of 18. Very few disabled children not receiving SSI cash assistance participate in the Medicaid program. About 18 percent of the Medicaid disabled population is over the age of 65. Disabled recipients over age 65 are persons who were eligible for Medicaid prior to age 65, and who continue to be classified as Medicaid "disabled" instead of "aged" after passing their 65th birthday. Almost all of these persons are non-institutionalized SSI cash recipients.
As discussed in Chapter 3, about half of all SSI disabled recipients (and therefore Medicaid disabled recipients) under the age of 65 are persons with a primary diagnosis of mental retardation or mental illness. About 58% of the Medicaid disabled are women, and about 34% are black.
A recent study of the Medicaid disabled "cash" population (only those receiving SSI benefits) showed that younger disabled persons on Medicaid had higher average expenditures than older recipients, primarily because older recipients were more likely to have work histories and be also covered by Medicare, which is always the first payer.28
| EXHIBIT 8-5: Medicaid Disabled Recipients by Institutional Status and Cash Assistance Status FY 1980 - 1987 | ||||||||
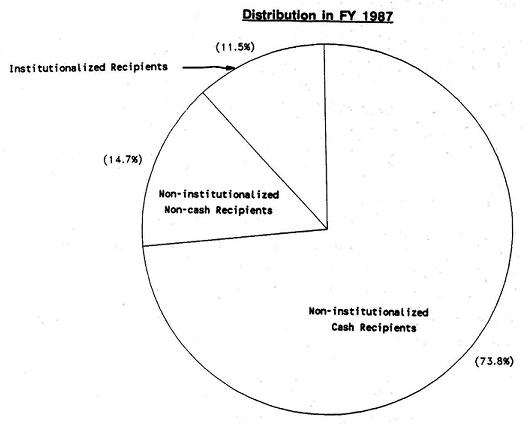 | ||||||||
| Total Medicaid Disabled | Percent Increase | Non-inst Cash | Percent Increase | Non-inst Non-cash | Percent Increase | Institutionalized | Percent Increase | |
| 1980 | 2,783,048 | 5.3% | 2,000,892 | 5.3% | 345,567 | 5.5% | 436,589 | 5.5% |
| 1981 | 2,828,533 | 1.6% | 2,029,704 | 1.4% | 355,160 | 2.8% | 443,669 | 1.6% |
| 1982 | 2,754,378 | -2.6% | 1,974,844 | -2.7% | 357,731 | 0.7% | 421,803 | -4.9% |
| 1983 | 2,779,692 | 0.9% | 1,975,210 | 0.0% | 399,659 | 11.7% | 404,823 | -4.0% |
| 1984 | 2,776,640 | -0.1% | 1,993,917 | 0.9% | 414,431 | 3.7% | 368,292 | -9.0% |
| 1985 | 2,867,539 | 3.3% | 2,080,551 | 4.3% | 412,665 | -0.4% | 374,323 | 1.6% |
| 1986 | 3,013,521 | 5.1% | 2,194,324 | 5.5% | 456,260 | 10.6% | 362,937 | -3.0% |
| 1987 | 3,225,726 | 7.0% | 2,380,731 | 8.5% | 474,932 | 4.1% | 370,063 | 2.0% |
8.10.6 Impact of Section 209(b) Option on Enrollment of Medicaid Disabled Recipients
As discussed in Section 8.5, States have various options as to how to treat SSI recipients in determining eligibility for Medicaid. Analyses indicate if States elect either of the two more restrictive options (requiring disabled SSI recipients to file a separate application for Medicaid or imposing more restrictive eligibility criteria under the Section 209(b) option), enrollment of disabled SSI recipients on Medicaid is definitively reduced. Compared to States which automatically extend Medicaid eligibility to SSI recipients without requiring a separate application, States which require a separate application have about 10% fewer SSI cash recipients on Medicaid, and States which elect the Section 209(b) option have, on average, about 35% fewer SSI cash recipients on Medicaid.29
CHAPTER 9. DEPARTMENT OF VETERANS AFFAIRS HEALTH SERVICES PROGRAMS
9.1 Overview and Purpose
The Department of Veterans Affairs (VA) operates a nationwide health care system, the goal of which is to provide quality medical care on a timely basis to all eligible veterans. The system includes 172 hospital centers, 119 nursing homes, 233 outpatient clinics, and 26 domiciliary care facilities.
9.2 Authorization, History, and Funding
The Department of Veterans Affairs was established as a separate Federal agency in 1930, consolidating benefits and services administered by three separate agencies prior to that time. The VA hospital system has grown from 54 hospitals in 1930 to its current network of 172 medical centers.
Funding allocations for medical care programs are made through annual direct appropriations to the VA. In 1988, medical care programs administered by the VA totalled $10.8 billion. This includes the cost of direct medical services, the construction and modernization of facilities, as well as medical research and training programs.
9.3 Administrative Structure
Medical care in the VA health system is administered by the Veterans Health Services and Research Administration. Most medical services provided by the VA are provided in facilities directly owned and operated by the VA, although the VA also contracts for certain types of services, such as community nursing home care. The VA also provides cost sharing for services provided in State-operated hospitals, nursing homes, and domiciliary care facilities which serve eligible veterans. The VA directly employs over 200,000 health service personnel in the management and delivery of its health services programs.
9.4 Eligibility
Public Law 99-272, enacted in 1986, established three eligibility groups among veterans for health care services (Category A, B and C). VA hospitals are required to provide care to veterans in Category A and can provide care to veterans in categories B and C on a space-available basis.
A Category A veteran is any person who meets one or more of the following criteria:
- is rated as "ser-vice-connected;"
- is retired from active duty for a disability incurred or aggravated while in military service;
- is in receipt of a VA pension;
- is eligible for Medicaid;
- is a former POW;
- is in need of care for a condition that is possibly related to exposure to dioxin or other toxic substance;
- is in need of care for a condition possibly related to exposure to radiation from nuclear tests or in the American occupation of Japan; or
- has an income below $16,466 with no dependents, or $19,759 with one dependent (with $1,055 added for each additional dependent).
Persons in Category B are veterans who are not service-connected and have incomes above $16,466 but below $21,954 (higher limits are applied to veterans with dependents). Medical care for veterans with higher incomes (Category C) is available as long as resources permit, and requires a copayment on the part of the veteran.
The same law eliminated the previous eligibility of veterans aged 65 and over to receive medical care on the basis of age alone. In FY 1987, 95% of the patients served by the VA system were in Category A, 2.5% were in Category B, and 2.5% were in Category C.
9.5 Services Provided
The VA provides a complete range of surgical, medical, rehabilitative and long term care services to eligible veterans. The system includes about 76,000 hospital beds, including 22,000 psychiatric beds, as well as approximately 12,000 nursing home beds. Services provided by the VA include many specialized services required by veterans with disabilities, including rehabilitative services, special programs for veterans with alcohol and drug dependence a spinal cord injury service, programs for post-traumatic stress problems, disorder, and a prosthetic and sensory aids services.
9.6 Program Interactions
The VA is first payer for all services provided to veterans who qualify under Category A for VA medical services. For veterans who are non-service connected (Categories B and C), VA is generally the secondary payer and attempts are made to recover the cost of care provided to veterans in Categories B and C with third party health insurance. In 1987, the VA collected about $24 million for medical care provided to health-insured nonservice-connected veterans.
9.7 Program Data
In FY 1987, VA health care system treated about 1.4 million veterans in its hospital care system, and had an average daily census of about 56,000 patients. The system served an average daily census of about 17,000 patients in its nursing home and domiciliary care facilities, and supported an additional daily census of about 25,000 in community and State-operated nursing homes and domiciliary care facilities. In total, about 2.9 million recipients received medical care services through the VA system in 1987.
Total outlays for medical programs operated by the VA have increased from $6.5 billion in 1980 to $10.8 billion in 1988. Of course, not all of these expenditures are for veterans with disabilities, and although veterans with disabilities comprise a significant portion of the VA caseload, it is not possible to disaggregate services and expenditures in the VA system to disabled and nondisabled populations.
CHAPTER 10. CHAMPUS PROGRAM FOR THE HANDICAPPED
10.1 Overview and Purpose
The Civilian Health and Medical Program of the Uniformed Services (CHAMPUS) provides health insurance coverage for eligible dependents of active service personnel. The CHAMPUS Program for the Handicapped (PFTH) provides specialized care for disabled dependents of active-duty military personnel who cannot get required care from public institutions or agencies.
10.2 Authorization, History and Funding
PFTH is authorized under the Military Medical Benefits Act Amendments of 1966 (P.L. 89-614). The program was established by Congress to provide financial assistance to active-duty military personnel's handicapped dependents, who because of residency laws, are excluded from public programs and institutions for the handicapped. Funding for this 100% Federally funded program in FY 1987 was $4,681,000.
10.3 Definition of Disability
The definition of disability used for PFTH is based on the strength and duration of a physical or mental handicap. The physical handicap must be of such severity as to preclude the individual from performing basic activities of daily living at a level expected of unimpaired individuals of the same age group and must be expected to result in death or to have lasted or be expected to last for at least 12 months. For a mental handicap, the applicant must be medically determined to be moderately or severely retarded.
10.4 Administrative Structure
The program is administered by the Department of Defense, Office of Civilian Health and Medical Program of the Uniformed Services (OCHAMPUS) through its fiscal intermediaries. Active duty members who wish to apply for benefits under the CHAMPUS Program for the Handicapped must submit a plan of management of the handicapping condition, including estimated costs, to the CHAMPUS fiscal intermediary for approval.
10.5 Eligibility
Spouses and children of active duty military personnel are eligible to receive specialized institutional care, training, or rehabilitation if moderately or severely mentally retarded or seriously physically handicapped. The program will pay for care only if the individual is ineligible for other publicly financed programs or if the available programs are unable to meet the individual's needs.
10.6 Services/Benefits Provided
Services provided include diagnosis; inpatient, outpatient, and home treatment; training, rehabilitation and special education; institutional care; payment for nutrient solutions required for special feeding at home; and the purchase and maintenance of durable equipment. The family pays a set amount of the cost of care each month based on the active-duty member's pay level. The cost-share amount ranges from $25 to $250 a month and does not increase with the number of dependents covered by the program. Beneficiaries ate eligible for up to $1,000 a month of coverage beyond the costs covered by the family's share for services and supplies provided under the program.
10.7 Program Interactions
This program is designed to finance services as a last resort if a disabled individual is ineligible for services provided by public institutions and agencies.
10.8 Program Data
In FY 1987, 2,508 individuals were assisted by the program.
CHAPTER 11. SOCIAL SERVICES BLOCK GRANT
11.1 Overview and Purpose
The Social Services Block Grant (SSBG) is the largest source of Federal funds for social services. The statute specifies five service goals for the SSBG program: 1) preventing, reducing or eliminating dependency; 2) achieving or maintaining self-sufficiency or economic self-support; 3) preventing or remedying child and adult abuse and neglect; 4) preventing or reducing inappropriate institutional care; and 5) securing admission or referral for institutional care when other types of care are not appropriate. Each State determines the types of services to be provided and the individuals to be served under the program. There is considerable variation across States with regard to how SSBG funds are targeted, and although the program has been a major source of financing for supportive services to persons with disabilities, actual data on the extent to which the program serves persons with disabilities are not available.
11.2 Authorization, History and Funding
Authorization for the Social Services Block Grant is contained in Title XX of the Social Security Act, as amended by the Omnibus Budget Reconciliation Act of 1981. The block grant consolidated Federal assistance to States for social services, child day care services and training; and increased State flexibility in the use of the funds. Federal appropriations for the SSBG rose between 1982 and 1984 but have remained essentially constant from FY 1984 to FY 1989 at $2.7 billion. The program is 100% Federally funded. Because of the flexibility the block grant has allowed the States, it is not possible to determine what proportion of total funds are expended for services to the disabled.
The territories are allocated funds based on the initial allocations made in FY 1981 when the program was established. For the remaining States, allocations are made in proportion to State population. Allocations for FY 1989 ranged from $301 million in California and $198 million in New York State to $5.6 million in the State of Wyoming.
11.3 Definition of Disability
There is no Federal statutory definition of disability in the SSBG program, and States are given complete discretion in determining the programs that will be supported with SSBG funds. State programs that serve persons with disabilities with SSBG funds can set their own criteria for determining disability.
11.4 Administrative Structure
The Social Services Block Grant Program is administered by the Department of Health and Human Services, Office of Human Development Services. Block grant funds are awarded primarily to State and territorial departments of social services, who then provide services directly through local offices and/or through contracts with private providers. In order to qualify for an allotment under the SSBG program, States must submit pre-expenditure reports that meet Federal requirements.
11.5 Eligibility
There are no Federal eligibility requirements for receipt of services under the Social Services Block Grant program. States may establish their own eligibility rules. The Office of Human Development Services reports that of the 55 States and territories reporting in 1986, at least 52 States and territories reported use of AFDC, SSI and non-income related eligibility groups for SSBG supported services. Ten States reported use of special groups including the disabled to define eligibility categories.
11.6 Services/Benefits Provided
Program funds may be used for the planning, administration or evaluation of social service programs as well as reimbursement for direct services. Services that benefit persons with disabilities include but are not limited to protective services, services for children and adults in foster care, services related to the management and maintenance of the home, day care services for adults, transportation services, employment services, information, referral and counseling services, the preparation and delivery of meals and health support services. States have broad discretion to define the social services they support under their block grant programs, provided they are directed at the program's five major goals. Many States provide a broad range of services to many target populations while others narrowly define their target population and scope of services. For example, in FY 1987 California utilized their SSBG funds to support home-based services for all of their program's target populations. The same year Montana earmarked all their SSBG funds for services to their developmentally disabled population. Out of 54 States and territories reporting to Human Development Services in 1986, 31 stated that they used some portion of their SSBG funds to support services targeted to persons with disabilities. A study of State funding of services to persons with developmental disabilities reported that in FY 1986, States spent $293 million in SSBG funds for services to the developmentally disabled.30
11.7 Program Data
There is very limited information available on the use of SSBG funds by States. Presently, States are only required to report information about the types of activities they plan to fund and the characteristics of the persons served. Under the Family Support Act of 1988, reporting requirements were strengthened, and States will be required to submit annual reports containing detailed information on services funded and individuals served.
| EXHIBIT 11-1: Annual Funding of the Social Services Block Grant 1980 to 1990 |
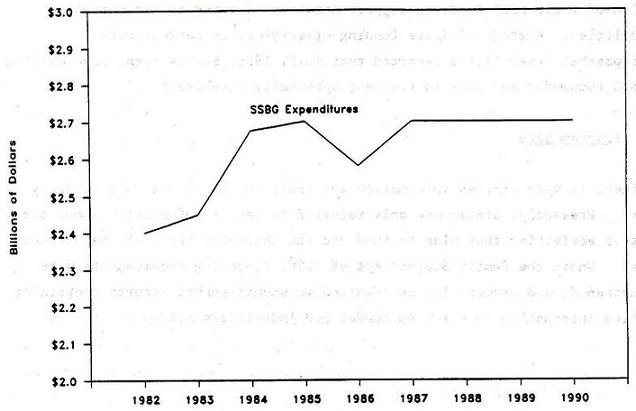 |
CHAPTER 12. ADMINISTRATION ON DEVELOPMENTAL DISABILITIES PROGRAMS
12.1 Overview and Purpose
The mission of the Administration on Developmental Disabilities is to assist States in assuring that persons with developmental disabilities are given opportunities to achieve their maximum potential through increased independence, productivity and integration into the community. The administration sponsors four grant programs that support planning and coordination of services, and the provision of an array of direct services, as well as protection and advocacy systems in each State to protect the legal and human rights of persons with developmental disabilities. The four programs are the Basic State Grant Program, the Protection and Advocacy Program, the University Affiliated Programs and Projects of National Significance.
12.2 Authorization, History and Funding
The Administration on Developmental Disabilities' Programs are authorized under the Developmental Disabilities Assistance and Bill of Rights Act Amendments of 1987 (Public Law 100-146) parts A-E. The Act evolved from the Mental Retardation Facilities Construction Act of 1963 and has been revised periodically to the current act. In FY 1989, approximately $60 million was awarded to States under the Basic State Grant Program to better plan and coordinate services for persons with developmental disabilities with an emphasis on case management, child development, community living and employment related services. Also in FY 1989, the Protection and Advocacy Program allocated $19.8 million to States to protect the rights of persons with developmental disabilities through the pursuit of legal and administrative remedies. $12.6 million was provided to support the University Affiliated Programs and almost $3 million was allocated in support of research and demonstration Projects of National Significance to increase the independence, productivity and integration into the community of persons with developmental disabilities.
The four Administration on Developmental Disabilities (ADD) grant programs have different State matching fund requirements. For the Basic State Grants, the Federal share can be no greater than 75% of the project costs, except in rural or urban poverty areas where the Federal share will not exceed 90%. The Protection and Advocacy Program is 100% Federally funded as are the University Affiliated Programs and the Projects of National Significance.
Grant funding for the two of the State grant programs is allocated among the States and territories on the basis of population, need for services, and financial need of the individual States and territories. Grant awards for these ADD grant programs have been allocated as follows:
-
Basic State Grants: Federal funding of the Basic State grant program in FY 1989 totalled just under $60 million. Annual funding levels for FY 1980 through FY 1989 are presented in Exhibit 12-1. Grants ranged from $4 million in California to $160,000 in the U.S. territories. The minimum allotment for the program when the appropriation exceeds $47 million is $300,000 per State and $160,000 per territory.
-
Protection and Advocacy Grants: In FY 1986, funding totaled $9 million. State allotments ranged from $700,000 in California, and $150,000 in Missouri, to $67,000 in the U.S. territories.
12.3 Definition of Disability
The Administration on Developmental Disabilities estimates that as of 1989, 3.9 million people in the United States had developmental disabilities. The Developmental Disabilities Assistance and Bill of Rights Act Amendments of 1987 defines developmental disability as:
"A severe, chronic disability of a person which is attributable to a mental and/or physical impairment; is manifested before the person attains age 22, is likely to continue indefinitely; reflects the person's need for a combination and sequence of special, interdisciplinary or generic care, treatment or other services which are of a lifelong or extended duration and are individually planned and coordinated; and results in substantial functional limitations in three or more of the following areas of major life activities: (1) self care; (2) receptive and expressive language; (3) learning; (4) mobility; (5) self-direction; (6) capacity for independent living.
12.4 Administrative Structure
At the Federal level, the programs are administered by the U.S. Department of Health and Human Services, Office of Human Development Services. In order to receive funding through the State grant programs, States must establish a Protection and Advocacy System for persons with developmental disabilities. Currently Protection and Advocacy Systems operate in every State. Most of the systems are operated by private non-profit organizations. Several systems are operated by State agencies such as Governors' Commissions on Human Resources and State Civil Rights Commissions. The Protection and Advocacy System in each State must have the authority to pursue legal, administrative and other remedies. For example, the system must have the authority to investigate incidents of abuse and neglect and have access to client records. The system must be independent from any agency which provides these services.
The University Affiliated Program grants are awarded to and administered by universities and satellite centers. The Projects of National Significance are awarded to and administered by State and local governments, universities and non-profit organizations.
12.5 Eligibility
Direct service provision to persons with developmental disabilities is not a priority for ADD grant programs; however some services are funded out of the activities of the grants. In cases where ADD grant monies are being used in direct service provision, there are no Federally mandated income or functional eligibility requirements for clients served. However, Federal guidelines define the population to be served under ADD programs as persons meeting the definition of developmental disabilities contained in the DD Act of 1987 (see Section 12.3).
12.6 Services/Benefits Provided
The Administration on Developmental Disabilities' grant programs support a variety of activities aimed at enhancing the independence and protecting the rights of persons with developmental disabilities. The Basic State Grant Program funds are used to support planning and administrative costs as well as the delivery of services. The main focus of the program is stimulating new programs which are responsive to the needs of developmentally disabled persons. Under the program, State DD Councils receive monies to better plan and coordinate services for persons with developmental disabilities with priority on strengthening case management, child development, community living, and employment related services. States are required to spend at least 65% of their grant for service activities within certain priority areas specified by ADD for each grant cycle. Beginning in 1986, States were required to include employment activities as a funding priority.
The Protection and Advocacy Program grants are used to assist people with developmental disabilities in obtaining appropriate education, employment, guardianship, transportation, and housing; resolving situations that are abusive and neglectful; and removing architectural barriers. Protection and Advocacy System staff offer referrals to appropriate agencies, counseling, negotiation, dispute mediation, and legal representation.
The University Affiliated Program grants support forty-seven university programs in forty-one States and the District of Columbia. The funding is used to support administrative and operating expenses related to the provision of services to the ADD community and training for personnel needed to serve people with developmental disabilities. Direct services to individuals include initial diagnosis and evaluation, and community-based services such as supportive housing and vocational training.
Projects of National Significance grants have supported demonstrations, research and evaluation projects which have expanded or otherwise improved opportunities for persons with developmental disabilities. Each year, ADD announces priorities for these projects. In FY 1988, 25 grants were awarded in the following priority areas: family support services, data collection activities, HIV/AIDS, minority populations, and elderly persons with developmental disabilities.
12.7 Program Data
-
While direct services are not a priority for use of Basic State Grants, ADD reports that approximately 57,414 persons were served in FY 1986. Services were in the areas of alternative community living arrangements, job training, health care and education.
-
In FY 1987 the Protection and Advocacy Program served an estimated 70,210 persons with needs in education, housing, financial entitlement, abuse, neglect and exploitation.
-
An estimated 57,000 individuals with developmental disabilities and their families receive direct services each year from the University Affiliated Programs. In addition, approximately 250,000 professionals, paraprofessionals, parents and volunteers receive training in these programs each year.
| EXHIBIT 12-1: Annual Funding of the Administration on Developmental Disabilities Basic State Grant Program: 1980 to 1989 |
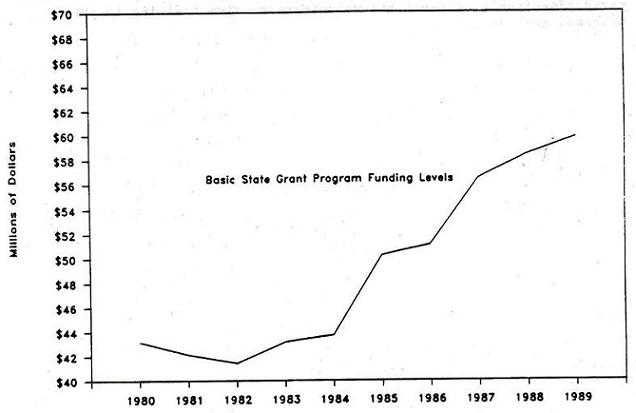 |
CHAPTER 13. MATERNAL AND CHILD HEALTH BLOCK GRANT: PROGRAMS FOR CHILDREN WITH SPECIAL HEALTH CARE NEEDS
13.1 Overview and Purpose
The objectives of the Maternal and Child Health (MCH) block grant program, funded under the Public Health Service (PHS), are to enable States to maintain and strengthen their leadership in planning, promoting, coordinating and evaluating health care for mothers and children and in providing health services for mothers and children who do not have access to adequate health care. Until 1981, the Public Health Service provided discretionary funding for services to disabled children under separate categorical funding of the Services for Crippled Children (CCS) program. Under OBRA 1981, funding for the CCS program was folded into the overall Maternal and Child Health Block Grant, so that disabled children are no longer identified as a separate categorical population. However, most States continue to use a substantial portion of their MCH block grant funds to support services for disabled children, now generally referred to as Programs for Children with Special Health Care Needs (CSHCN).
13.2 Authorization, History and Funding
The Maternal and Child Health block grant is authorized under Title V of the Social Security Act. The establishment of the block grant dates back to the Maternity and Infant Act of 1921. The current grant program was formed by the Omnibus Budget Reconciliation Act of 1981 which consolidated six programs authorized under Title V into a single block grant authority (the six programs were: the State grants-in-aid program for maternal and child health and crippled children's services, the SSI Disabled Children's program, and grant support for the prevention of lead-based paint poisoning, sudden infant death syndrome, hemophilia treatment centers, an adolescent pregnancy program and a genetic screening program). State are required to match $3 of direct or in kind expenditures for every $4 of Federal aid. Federal appropriations for the program in FY 1989 were $554.3 million, up 5% from FY 1988 appropriations of $526.6 million.
Of the allocation for the MCH grant, 15% is retained by the Department of Health and Human Services (DHHS) to fund research, training, special projects, genetic services and hemophilia projects conducted by public and private organizations. These are called Special Projects of Regional and National Significance (SPRANS grants). The remaining funds are allocated to the States and territories based on the share of funds received historically under related programs. If appropriations exceed the FY 1983 level, additional funds are allocated among the States according to proportion of persons under 21 living in poverty. In FY 1986 State allocations ranged from $37 million in California and $31 million in New York State to $16 million in Florida and $858,000 in Alaska.
13.3 Administrative Structure
The program is administered by the Bureau of Maternal and Child Health in the Department of Health and Human Services, Public Health Service, Health Resources and Services Administration. The Bureau of Maternal and Child Health (BCMH) requires each State to submit a State needs assessment. The assessment must include information on the types of services to be provided, the types of individuals to be served and the type of data the State intends to collect on the programs. The State must assure the Secretary that it will use the majority of its Title V allotment for services to mothers and children. The State agency that administers the program must coordinate its activities with the State's Medicaid program and other Federal grant programs (e.g. WIC, education, health and developmental disabilities services). States are required to submit annual reports to DHHS on programs funded under the Maternal and Child Health block grant. Grantees are primarily State health departments who then award subcontracts to local or regional health departments, migrant and community health centers or private providers.
13.4 Eligibility
Although the grant targets low income women and children, there are no Federal eligibility requirements that woman and children receiving services under the grant must meet. States have the authority to set precise eligibility requirements for the receipt of services under the block grant. However, the MCH block grant prohibits States from charging fees to low-income mothers and children and requires that when fees are charged they reflect the income, resources, and family size of the beneficiary. A number of States have sliding fee scales for beneficiaries.
There are no Federal criteria for defining children with special health care needs who are eligible for assistance under the program. The population served by CSHCN programs has changed considerably over time. The CCS programs primarily served children with crippling conditions such as polio and cerebral palsy, often in State-fun clinics and tertiary care centers. Presently, however, CSHCN programs have expanded to serve children with a wide range of chronic health conditions.31
13.5 Services/Benefits Provided
In most States, the CSHCN program plays a significant role in the care of chronically ill children. Services offered by States are diverse and extensive. Most State spend program funds on screening and treatment of handicapping conditions. They also fund a variety of ongoing support services, including case management and counseling. A few operate State-owned hospitals for handicapped children. State CSHN services are typically provided through State health agencies and physicians on a fee-for-service basis.
CSHCN programs are strongly clinic-based programs in many States, actually providing some or all of the covered services directly, rather than simply serving as a payer of services provided through other programs. However, as other sources of financing services for disabled children have grown, particularly under Medicaid, there is a general trend in CSHCN programs towards an emphasis on the development of case management systems which identify, assess and assist families with disabled children in accessing requisite medical and support services through other programs.
13.6 Program Data
According to survey data collected by the Public Health Foundation, States used approximately $98.5 million of the $496.8 million (20%) of their MCH block grant funds on Programs for Children with Special Health Care Needs. However, States also spent an addition $408.9 million of their own State funds on CSHCN programs in the same year. Exhibit 3-1 presents trends in Federal funding of the overall Maternal and Child Health block grant program from 1980 onward.
| EXHIBIT 13-1: Annual Federal Funding of the Maternal and Child Health Block Grant |
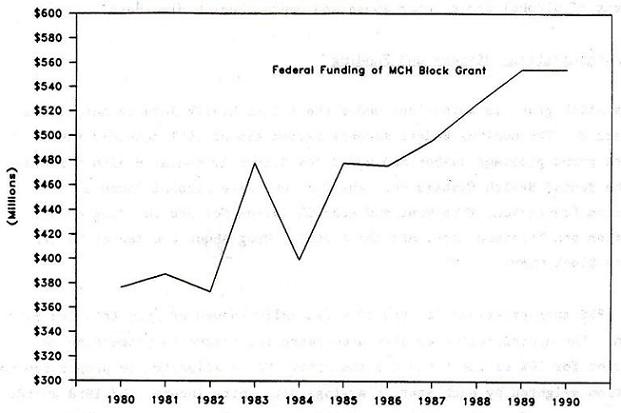 |
| Federal funding for 1983 includes $105 million from the Jobs Bill designated as being for the care of mothers and children. Prior to consolidation of categorical programs into the block grant in 1982, funding for Crippled Childrens Services comprised 27 percent of Title V funding. |
CHAPTER 14. ALCOHOL, DRUG ABUSE AND MENTAL HEALTH SERVICES BLOCK GRANT
14.1 Overview and Purpose
The Alcohol, Drug Abuse and Mental Health Services Block Grant provides funding to States for maintaining and expanding programs for the prevention and treatment of alcohol abuse, drug abuse and mental health disorders.
14.2 Authorization, History and Funding
The block grant is authorized under the Public Health Service Act, Title XIX, Part B. The Omnibus Budget Reconciliation Act of 1981 combined four separate grant programs authorized under the Community Mental Health Centers Act, the Mental Health Systems Act, the Comprehensive Alcohol Abuse and Alcoholism Prevention, Treatment and Rehabilitation Act and the Drug Abuse Prevention and Treatment Act into the Alcohol, Drug Abuse and Mental Health Services Block Grant.
FY 1988 appropriations for the 100% Federally funded program totalled $487 million. The appropriation is allocated among the States in proportion to population for 50% of the funds and the other 50% is allocated in proportion to population weighted by each State's average per capita income. FY 1988 awards to States ranged from $48 million in California and $40 million in New York State to $758,000 in Wyoming.
14.3 Definition of Disability
Block grant funds are meant to benefit persons with chronic mental illness, including severely mentally disturbed children, adolescents, and elderly clients and those with severe drug dependency problems.
14.4 Administrative Structure
The program is administered by the Department of Health and Human Services, Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration (ADAMHA). ADAMHA requires each grantee to submit an annual report on program activities. Participating States are also required to develop a comprehensive State plan to serve persons with chronic mental illness. Grantees are primarily State health, mental health and social services departments. These State agencies may contract for services with local substance abuse and mental health programs.
14.5 Eligibility
As is true with the other block grant programs that benefit the disabled population, States have discretion over who is served under the program. There are no Federal requirements that certain income or functional eligibility criteria be used in programs supported by ADAMHA block grant funds. However, services funded with the block grant are to be targeted to individuals with chronic mental illness, severely mentally disturbed children and adolescents, mentally ill elderly individuals and other identifiable populations which are underserved.
14.6 Services/Benefits Provided
Block grant funds may be used to support community mental health centers and the provision of services to the previously specified target populations. Spending is at the discretion of the States except that the amount allotted for mental health must be used to support community mental health centers. In addition, of the amount allotted for substance abuse, not less than 35% must be used for alcohol activities, not less than 35% for drug abuse activities and not less than 20% for prevention and early intervention activities. Beginning in 1985, States were required to set aside monies for new or expanded alcohol and drug abuse services to women, and new comprehensive community mental health services for the underserved with a special emphasis on severely disturbed children. Not more than 10% of the funding can be used to administer the grant funds.
14.7 Special Issues
In a survey of the States conducted by the Alcohol, Drug Abuse, and Mental Health Administration in 1986, many States reported an inability to serve the handicapped population. California, Minnesota, New Hampshire, New Jersey, Oregon and Wisconsin all identified a need to develop and expand services to substance abusers with physical or mental handicaps.
| EXHIBIT 14-1: Annual Funding of the Alcohol, Drug Abuse and Mental Health Services Block Grant: 1982 to 1989 |
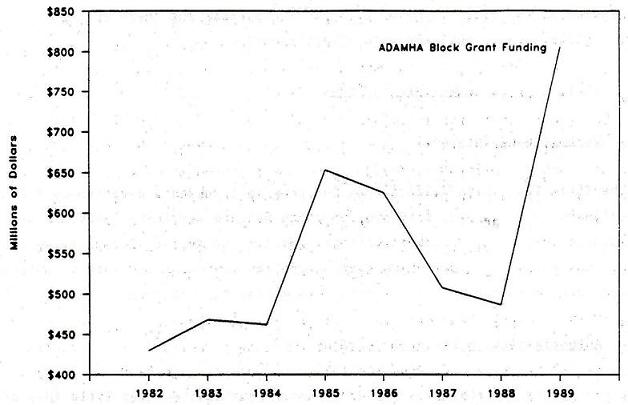 |
CHAPTER 15. CHILD WELFARE SERVICES
Child welfare services are aimed at protecting and promoting the well being of all children including handicapped, homeless, dependent or neglected children. The Department of Health and Human Services has several programs offering support for child welfare services. The four primary sources of funding for child welfare services are Title IV-B Child Welfare Services, the Title IV-E Foster Care program, the Title IV-E Adoption Assistance program, and the Title XX Social Services Block Grant program. This chapter includes a description of the Title IV-B and Title IV-E programs, and their role in providing services to children with disabilities.
15.1 Title IV-B Child Welfare Services
15.1.1 Overview and Purpose
The Title IV-B Child Welfare Services program provides discretionary funds to designated State agencies to provide child welfare services. Services are provided to children and members of their families to assist in preserving the family structure. In cases where family problems cannot be resolved, services are provided to obtain suitable adoptive homes for the children.
15.1.2 Authorization, History and Funding
State grants for child welfare services are authorized under Title IV-B of the Social Security Act. Such grants have been authorized under the Social Security Act since its enactment in 1935. Amendments to the act in recent years (1972 and 1980) have increased funding and focused the grants on supporting more Adoption assistance activities especially for hard to place children, to minimize the need for foster care placements.
Title IV-B grants are 75% Federally funded and in FY 1989, $247 million in Federal appropriations were allocated to the States and territories. States are given a base amount plus an allotment based on a formula which accounts for population under 21 years old and per capita income.
15.1.3 Administrative Structure
The Title IV-B program is administered at the Federal level by the Administration for Children Youth and Families, Office of Human Development Services within the Department of Health and Human Services. Grants are made to States that conduct an inventory of children who have been in foster care for over 6 months; implement a Statewide information system on children in foster care; and initiate a case review system that includes each child in foster care. The case review system must incorporate a 6-month review and 18-month dispositional hearing for each child; be designed to achieve placement in the least restrictive setting and in close proximity to the child's home; and provide procedural safeguards for children, parents, and foster care providers. Finally, States must implement a program designed to assist children, where possible, to return to their homes.
15.1.4 Eligibility
There are no Federal eligibility requirements for receipt of services under the State Grant Program.
15.1.5 Services/Benefits Provided
Funding is provided to States for services to support the family structure and promote family reunification such as counseling, and day care services. Funds may be used to support personnel for protective services to children; to fund licensing and standard setting for private child care agencies and institutions; to provide homemaker services; and to work toward the return of runaway children.
15.2 Title IV-E Foster Care and Title IV-E Adoption Assistance
15.2.1 Overview and Purpose
The Title IV-E Foster Care program is an entitlement program which provides open-ended matching funds to States for the maintenance payments made for AFDC-eligible children in foster care family homes or child care institutions of 25 persons or less. The Title IV-E Adoption Assistance Program is also an open-ended entitlement program which requires States to develop adoption assistance agreements with the adoptive parents of children with "special needs." Since the Adoption Assistance program is the Federal program which is primarily used to provide adoption services for children with various disabilities, the remainder of this section presents a discussion of this component of the Title IV-E program only.
15.2.2 Authorization, History and Funding
The Adoption Assistance Act of 1980 (P.L. 96-272) established Title IV-E of the Social Security Act which authorized an adoption assistance program to assist States in promoting and facilitating the adoption of children with special needs. The program is 50% Federally funded for up to $2,000 in State expenditures per adoptive placement. Estimated State claims for Adoption Assistance Services in FY 1989 are $112 million.
15.2.3 Definition of Disability
The Adoption Assistance program serves children with special needs. Children with special needs are those who have a specific factor or condition that makes it difficult to place the child in an adoptive home such as age, ethnic background, or physical, mental or emotional handicaps. States have considerable latitude in defining "special needs" eligibility criteria and individually determining whether a child is eligible.
15.2.4 Administrative Structure
The program is administered by the Administration for Children, Youth and Families, the same office within Health and Human Services that administers the Title IV-B program.
15.2.5 Eligibility
Under the Title IV-E authority, States are reimbursed for payments of nonrecurring expenses of adoption as well as ongoing expenses for all children with special needs. As was summarized previously, a child with special needs: 1) cannot or should not be returned to the home of the parents; 2) has a specific factor or condition that makes it difficult for the child to be placed in an adoptive home without providing assistance (i.e., age, ethnic background, or physical, mental or emotional handicaps); and, 3) except where it would not be in the best interest of the child, a reasonable effort must be made to place the child in an adoptive home without providing special adoption assistance. In most States, the Adoption Unit within the State Department of Social Services determines whether a child meets the special needs definition. Children aged 0-18 are covered unless the State determines that the child has a physical or mental handicap which allows continuation of payments until the age of 21.
There are no income requirements that must be meet by adoptive parents of children with special needs.
15.2.6 Services/Benefits Provided
The Adoption Assistance program provides financial assistance to assist adoptive parents with nonrecurring, or one time expenses at the time of adoption. In addition, families continue to receive ongoing assistance at a level that is negotiated between the parents and the State agency. The amount of the adoption assistance benefit cannot exceed the State foster care payment rate. In 1988, it was estimated that the average benefit per placement was $1,800 per year.
15.2.7 Program Interactions
The State will determine the amount of the adoption assistance payments through an agreement with the adoptive parents. If a child receives SSI and is eligible for adoption assistance, the child's SSI payment will be reduced by the amount of the adoption assistance payment, Children provided benefits through adoption assistance are also eligible for Medicaid.
15.2.8 Program Data
In FY 1989, an estimated 38,000 children with special needs were receiving monthly payments under the Adoption Assistance program. Total State claims for adoption assistance services in FY 1989 are estimated at $112 million, of which the Federal share was about $73 million.
There is little available data on the specific characteristics of "special needs" children provided adoption assistance under the Title IV-E program.
CHAPTER 16. DEPARTMENT OF EDUCATION PROGRAMS
The U.S. Department of Education (DOE) offers educational and vocational rehabilitation programs for individuals with disabilities through the DOE Office of Special Education and Rehabilitative Services. The educational program supports State efforts in providing special education and related services to handicapped children from birth to age twenty-one. The vocational rehabilitation programs, administered by the Rehabilitative Services Administration, is focused on post-educational opportunities for handicapped individuals. There are no age requirements for the vocational rehabilitation program, unlike the special education programs, but over 90% of the participants are age eighteen or older. In this chapter, four Federally-funded special education programs will be profiled, followed by a profile of the vocational rehabilitation program.
The largest special education grant program is authorized under Part B of the Education of the Handicapped Act (EHA-B). The goal of this program is to provide a free public education to all handicapped children ages three to twenty-one. A second program, the Program for Handicapped Children in State-Operated Programs targets children from birth to age 20 who are currently enrolled in State-operated or State-supported schools and institutions and who are not served under EHA-B.
Two other programs concentrate on early education and intervention programs. The Preschool Grants Program provides special education programs and services to handicapped children three to five years old and the Handicapped Infants and Toddlers Program provides early intervention services to handicapped children from birth through age two.
Except for the Program for Handicapped Children in State-Operated Programs, the funds for the special education programs may, and do, support some of the same populations. For example, the discretionary part of the funding for the EHA-B programs may be used for early intervention services or programs for younger children if the State so chooses. Each State has developed a unique range of special education programs depending on their particular needs and interests.
16.1 State Grants for Special Education Programs
16.1.1 Overview and Purpose
The State Grants for Special Education Programs (EHA-B) support States in providing special education and related services to handicapped children ages three through twenty-one.
16.1.2 Authorization, History and Funding
The program was originally established in 1966 by the addition of Title VI to the Elementary and Secondary Education Act. Over the years, amendments to the Act have expanded the program and committed increased funding. In 1975, the Education for All Handicapped Children's Act (P.L. 94-142), dramatically increased the Federal commitment to educating all handicapped children.
In 1988, Federal funding was $1.12 billion, in 1989 Federal funding is expected to be $1.91 billion and in 1990, Federal funding is expected to be $1.53 billion. The States are required to match the Federal funding with 94% of the program costs. In FY 1988, the State grants ranged from $123 million to California, and $92 million to Texas, to $2.8 million to Vermont. The maximum amount of funding per State is equal to the number of handicapped children aged 3 through 21 who are currently receiving special education services multiplied by 40% of the average expenditure per pupil in public schools. The number of handicapped children included is capped at 12% of the total number of children between 5 and 17 in the State. The State Educational Agency is required to channel at least 75% of its funds received from the Federal grant to local educational agencies (i.e., intermediate or local school districts).
16.1.3 Definition of Disability
The program services children in the following disability categories: mental retardation, hearing impaired, speech impaired, visually handicapped, seriously emotionally disturbed, orthopedically impaired, other health impaired, deaf-blind, multi-handicapped, or severely learning disabled.
16.1.4 Administrative Structure
The Federal program is administered by the U.S. Department of Education, Office of Special Education and Rehabilitative Services, which distributes funds to the States. The State programs are administered through State educational agencies which in turn distribute and administer funds to local educational agencies.
Each State must submit an annual program plan to be eligible for a grant. The plan must include the development and use of an individualized education program for each handicapped student, the establishment of procedural safeguards for all handicapped children and their parents, the training of personnel for special education programs, and the development of a plan to identify, locate and evaluate all handicapped children in all public and private agencies and institutions in the State. The plan must cover handicapped children ages three to twenty-one unless the State law indicates otherwise.
16.1.5 Eligibility
To receive special education services a child must be evaluated and found to be in one of the above mentioned handicapped categories. The evaluation is conducted under the auspices of a State or local educational agency depending on which agency is administering the program. The evaluation must be carried out by a multi-disciplinary team or group, including at least one specialist with knowledge in the area of suspected disability. The evaluation consists of a variety of tests and other evaluation materials and no single test may be used as the sole criterion for determining eligibility. The child must be re-evaluated at least once every three years and more frequently if necessary.
16.1.6 Services/Benefits Provided
The provision of special education for handicapped children includes classroom instruction, instruction in physical education, home instruction, and instruction in hospitals and institutions. In addition to providing direct special education, the State and local educational agencies can use grant money to provide related services which are required to help a handicapped child benefit from special education. These services include diagnostic services, occupational therapy, physical therapy, speech/language pathology, psychological services, counseling, school health services, and social work services in school.
After channeling 75% of its funds to local educational agencies, the State may use the remaining 25% of its funds for a range of State-established priorities. Up to 5% or $350,000, whichever is greater, may be used for administrative costs. Some States channel the remaining 20% to local educational agencies and some use the money to provide direct and/or support services for priority programs, such as targeting the handicapped preschool population or other underserved handicapped children.
16.1.7 Program Data
In the 1985-86 school year, 4,121,104 handicapped children aged 3 to 21 years were served under the State grants and in 1986-87, 4,166,692 children were served. This represents a 1.2% increase in the total number of handicapped children served between the 1986 and 1987 school years.
16.2 Program for Handicapped Children in State-Operated Programs
16.2.1 Overview and Purpose
The purpose of the program is to expand or improve educational services to handicapped children from birth to age 20 who are currently enrolled in State-operated or State-supported schools, programs, and institutions.
16.2.2 Authorization, History and Funding
The program is authorized under Chapter 1 of the Education Consolidation Improvement Act of 1981 (P.L. 97-35) as it amends Title 1 of the Elementary and Secondary Education Act of 1965 (P.L. 89-10). In FY 1987, $150 million was granted to the States and in FY 1986, $144 million was granted. Each State receives funds based on the number of handicapped children served in the previous year. The number of children includes 1) handicapped children currently enrolled in State-operated and State-supported institutions and 2) children who were enrolled in a State institution for at least a full school year during the school year 1971-1972 or any subsequent year and who are currently receiving their education through a local public school. If this is the case, the State agency must transfer the funds to the local educational agency currently serving the child. A State may not receive funds for the same child under this program and EHA-B.
| EXHIBIT 16-1: Number of Children Enrolled in Special Education Program 1980 to 1987 |
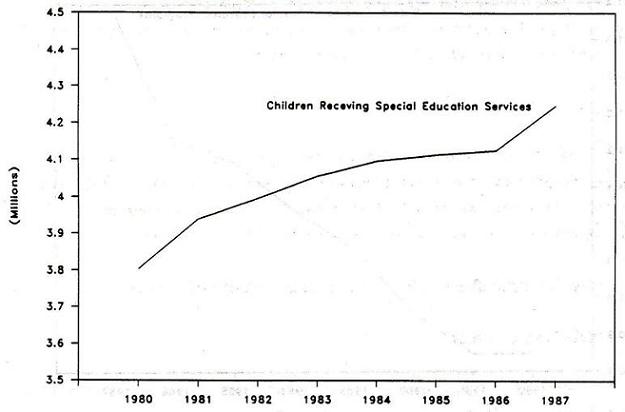 |
| EXHIBIT 16-2: Annual Federal Funding for Special Education Programs 1980 to 1987 |
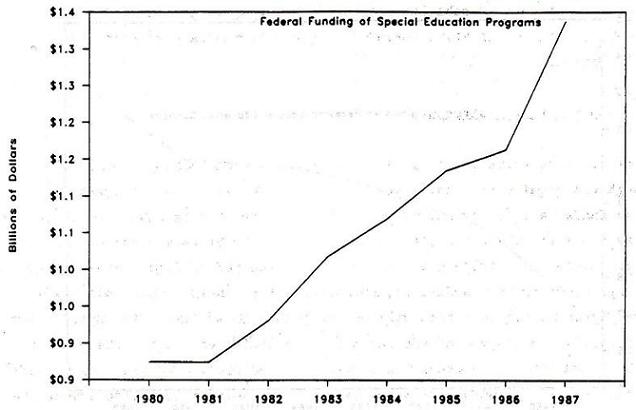 |
16.2.3 Definition of Disability
The definition of disability used in determining eligibility for handicapped children in State-operated programs is the same as that used for EHA-B programs.
16.2.4 Administrative Structure
The administrative structure of this program is the same as for EHA-B, although the requirements for State agencies differ under this program. To receive funds, a State agency operating a State-operated or State-supported institution must submit a project application to the State educational agency. The application must include the number of handicapped children to be served and their handicapping conditions, an assessment of their educational needs, and the types of services that will be provided. In addition, the application must describe how the use of the funds will be evaluated and how the project will be coordinated with other Federal, State, and local agencies. Each year, an agency receiving funds must submit an annual report to the State educational agency detailing the number of children served and the number transferring to a local educational agency during the school year.
If a handicapped child transfers from a State-operated or State-supported institution to a-school under the jurisdiction of a local educational agency, then the per capita funds for that individual are transferred with them. In order to receive such funds, a local educational agency must have submitted an application to the State educational agency detailing their program.
16.2.5 Eligibility
Handicapped children from birth to age 20 who attend State-operated or State-supported institutions are eligible to be covered by this program. As under the EHA-B program, each child must be evaluated by the State to determine eligibility (i.e., meet the definition of disability) and to assess the needs of the individual child.
16.2.6 Services/Benefits Provided
The services provided are the same as those provided under EHA-B. As under EHA-B, the States may use a portion of their funds for a range of State-established priorities. For example, some States have developed programs to ease the transition of students from State institutions to local community schools. Other States have opted to fund and develop home intervention programs for preschoolers.
16.2.7 Program Data
For the 1985-86 school year, this program served 249,140 handicapped children. For the 1986-87 school year, 254,909 children were served, compared to 4,166,692 handicapped children under the EHA-B program. The average per pupil annual allocation was $588 in FY 1987, $572 in FY 1986, $587 in FY 1985, and $593 in FY 1984.
16.3 Preschool Incentive Grants Program/Preschool Grants Program
16.3.1 Overview and Purpose
The Preschool Grants Program is designed to ensure that by 1991, all handicapped children aged 3 through 5 will have access to a free appropriate public education.
16.3.2 Authorization, History and Funding
The Preschool Incentive Grants Program first funded in 1977, was the original program targeting this handicapped population. In 1986, amendments to the 1975 Education for all Handicapped Children Act, Part B, changed both the name and purpose of the program. The new Preschool Grants Programs was developed to ensure that 100% of handicapped 3 to 5 year olds would have access to a free appropriate public education. The Federal funding level in FY 1986, the last year the program was called the Preschool Incentive Grant Program, was $28.7 million. Under the new Preschool Grant Program, the Federal funding for FY 1987 was $180 million. Of this, $80 million was for services provided to children already in the program and $100 million was for children expected to be newly identified and served by the program.
| EXHIBIT 16-3: Number of Handicapped Children in State-Operated Educational Programs 1980 to 1987 |
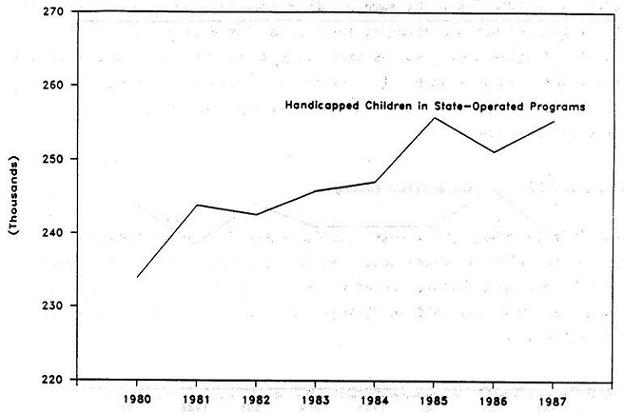 |
| EXHIBIT 16-4: Annual Federal Funding for Handicapped Children in State-Operated Educational Programs: 1980 to 1987 |
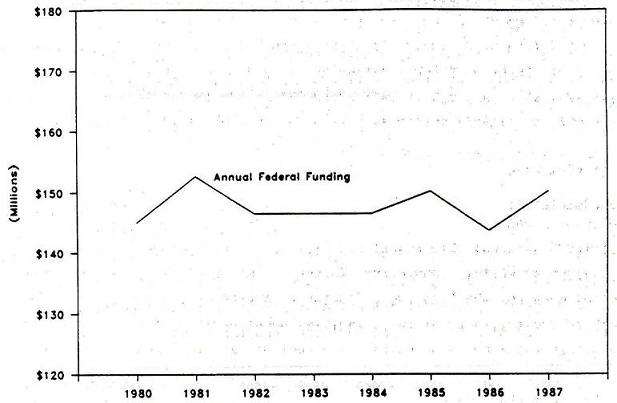 |
16.3.3 Definition of- Disability
The definition of disability used in determining eligibility for handicapped children in preschool programs is the same as that used for EHA-B programs.
16.3.4 Administrative Structure
The administrative structure of this program is the same as for EHA-B although the requirements for State agencies differ under this program. To receive funds, the State must submit an application to the Federal Secretary of Education through the State educational agency. The State must already have an approved plan for the EHA-B program and must already provide special education and related services to handicapped children aged three, four, or five.
As of FY 1988, states were required to channel 75% of their grant to local educational agencies and were limited to using 5% of the grant for administration. The State may use the other 20% for a range of State-established priorities. Before FY 1988, States had to channel at least 70% to local educational agencies.
16.3.5 Eligibility
Handicapped children ages three to five are eligible to receive services through this program. As under the EHA-B program, each child must be evaluated by the State to determine eligibility (i.e., meet the definition of disability) and to assess the needs of the individual child.
16.3.6 Services/Benefits Provided
The services provided are the same as those provided under EHA-B. In addition, the State must have a program to identify and locate new handicapped preschoolers through such activities as involvement in interagency groups, sponsoring public awareness programs, and conducting child finding activities. The States may also elect to fund other types of activities, such as providing training and technical assistance to existing programs or planning and developing a comprehensive system of service delivery for handicapped children.
16.3.7 Program Data
By 1986, the Preschool Incentive Grants Program had succeeded in getting all eligible State agencies to participate in the program which resulted in them reaching an estimated 75% of all handicapped children ages 3 through 5. However, in order to reach the goal of serving all eligible children by 1991, the Federal government sought to increase the pace of the program by committing more funds. The Federal government increased the annual per child allocation from $110 in FY 1986 under the original program to $300 in FY 1987, $400 in FY 1988, $500 in FY 1989, and $1,000 in FY 1989, where it will remain for subsequent years. Additionally, in order to promote locating and assisting all handicapped children for this age group, the Federal government committed $3,800 to the States for each newly identified handicapped child to be served for FY 1987 through FY 1989. In order to remain eligible to receive funding under the grant program, States must provide services to all 3 to 5 year old handicapped children by 1991.
16.4 Handicapped Infants and Toddlers Program
16.4.1 Overview and Purpose
The purpose of this program is to expand and improve the provision of early intervention programs for infants and young children with handicaps. The intervention programs are designed to minimize the child's potential for developmental delay so that the child will be less likely to need special education services in school and/or be institutionalized later in life.
| EXHIBIT 16-5: Number of Children Served in Preschool Incentive Grant Programs 1980 to 1987 |
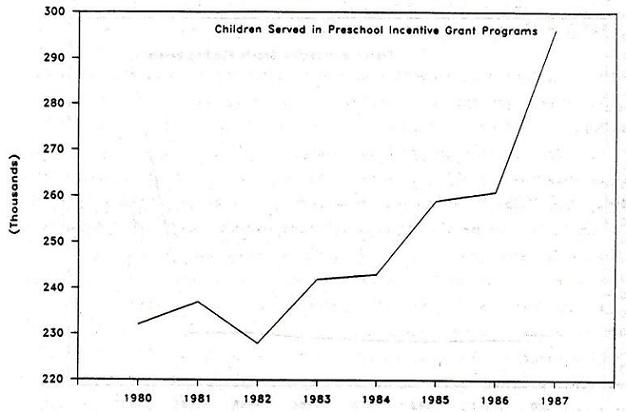 |
16.4.2 Authorization, History and Funding
This program is authorized under Part H of the 1986 Amendments of the Education for all Handicapped Children Act of 1975. In FY 1987, $50 million was awarded to the 50 States, D.C. and 7 territories with state grants ranging from $244,000 to Alaska to $5.7 million to California and in FY 1988, $75 million was awarded.
| EXHIBIT 16-6: Annual Federal Funding for Preschool Incentive Grant Programs 1980 to 1987 |
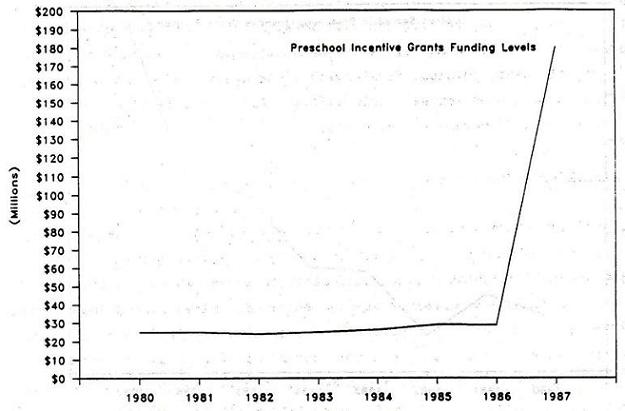 |
16.4.3 Definition of Disability
This program focuses on children with developmental delays or children who are at risk for developmental delays in one or more of the following areas: cognitive development, physical development, language and speech development, psychosocial development, or self-help skills. Each State develops its own working definition of developmental delay.
16.4.4 Administrative Structure
The administrative structure of this program is similar to that of EHA-B. The program is administered nationally by the U.S. Department of Education, Office of Special Education and Rehabilitative Services, which distributes the funds to the States. The Governor of each State designates a lead agency which administers and monitors the program. Each participating State must establish a State Interagency Coordinating Council, comprised of 15 members, which assists t e lead agency in developing a coordinated system and is responsible for submitting an annual report to the Governor and to the Federal Secretary of Education. By 1987, about one-third of the States had designated as lead agencies state Educational Agencies, another third chose the State Health Departments and the remainder chose a different agency such as Social Services, or Human Resources, or interdepartmental committees.
To receive funding, States must develop and implement a comprehensive, coordinated, interagency program of early intervention services for handicapped infants and toddlers and their families and facilitate the coordination of payment for early intervention services from Federal, State, and local government, as well as from private sources.
16.4.5 Eligibility
States are authorized to serve handicapped children from birth to age two who are experiencing delays, children who are likely to experience delays due to particular mental or physical conditions, and children who are at risk for developmental delays if early intervention services are not provided. As previously mentioned, each State may determine a definition for developmental delay.
16.4.6 Services/Benefits Provided
At a minimum, the State system must provide developmental services which: are free of charge unless the State law indicates otherwise, meet the child's physical, cognitive, psychosocial, language and speech developmental needs, meet State standards, and are provided by qualified personnel, including special educators, physical therapists, social workers, and nurses. Allowable services include family training counseling and home visits, special instruction, and speech pathology and audiology. Like the Preschool Incentive Grants Program, this program must conduct activities to identify individuals eligible for the program.
16.5 Basic Vocational Rehabilitation Services
16.5.1 Overview and Purpose
The Basic Vocational Rehabilitation Service Program supports the States in assisting physically and mentally handicapped individuals become gainfully employed. Unlike the special education programs, the vocational rehabilitation program does not use age as one of the eligibility criteria.
16.5.2 Authorization, History and Funding
The program is authorized under Title I of the the Rehabilitation Act of 1973, as amended. Vocational rehabilitation programs date back to 1920 when Congress passed the National Vocational Rehabilitation Act of 1920, authorizing the first program to help disabled civilians regain work skills. The program has been expanding ever since and most recently has been focusing on serving individuals with the most severe handicaps.
In FY 1988, Federal funding was $1.38 billion and in FY 1989, Federal funding is expected to be $1.44 billion. The State share of funds for the program is 20%. Beginning in FY 1989, the Federal share for the amount of funding above the previous year for each State decreases by 1% per year for five years. For example, in 1989 the Federal share of the increased amount of funding is 79% and in 1990 it will be 78%. This change in the Federal share applies to the development and provision of vocational rehabilitation services.
In FY 1989, an estimated $1.44 billion was allocated among the States according to a formula based on population and per capita income. California received $114 million, the largest allocation, followed by Texas with $92 million, New York with $85 million and Pennsylvania with $72 million. The minimum level of funding allowed is $4 million for States; however, there is no minimum funding level for territories.
16.5.3 Definition of Disability
The definition of disability used for this program is based on a physical or mental handicap that limits an individual's ability to be employed.
16.5.4 Administrative Structure
This program is nationally administered by the U.S. Department of Education, Office of Special Education and Rehabilitation Services, Rehabilitative Services Administration (RSA). RSA distributes funds to State agencies who develop and administer their State program.
The State administering agency must submit a State plan every 3 years which must be approved before the agency can receive Federal funds. Some States have two vocational rehabilitation agencies, one for the blind and one for people with other disabilities. In FY 1987, 27 States and territories had two such agencies. The State plan must assure the fair determination of eligibility, must provide a plan for a preliminary diagnostic study for those referred for rehabilitation, and must provide a thorough diagnostic study for those individuals found eligible for rehabilitation services. Ineligible determinations based on the finding that an individual cannot be expected to achieve a vocational goal, must be reviewed within 12 months of the determination.
If services cannot be provided to all eligible individuals who apply, then two groups of individuals should be given priority for services: those with the most severe handicaps and those public safety officers who sustained a disability in the line of duty.
There is no Federal requirement that the financial need of an individual be considered by a State when providing vocational rehabilitation services. However, a State may choose to consider the financial need of applicants for certain services and require that individuals share in the costs of services. The State may not use a financial needs test for the following services: evaluation of rehabilitation potential, counseling, guidance, referral, and placement.
The 1984 amendments to the act require States receiving basic vocational rehabilitation services funding to have a Client Assistance Program (CAP). CAP advises clients and client applicants of available services under the Rehabilitation Act and works to protect client's rights under the Act. The CAP must be administered by an agency that does not provide services under the Rehabilitation Act unless the agency had a CAP before 1984 and received Federal funding. Like the Vocational Rehabilitation Program, CAPs are supported by direct funding from the Federal Rehabilitation Services Administration (RSA). In 1987, $7.1 million in grants was awarded to CAP programs in the 50 States, D.C. and the 8 territories, based on the relative population of each State.
16.5.5 Eligibility
Eligibility is based upon "the presence of a physical or mental disability which for the individual constitutes or results in a substantial handicap to employment and a reasonable expectation that vocational rehabilitation services may benefit the individual in terms of employability" (34 CFR Ch.III, 361.31). Type of disability and State residency cannot be used in determining eligibility.
16.5.6 Services/Benefits Provided
The State is required to provide many vocational rehabilitation services including, evaluation of vocational rehabilitation potential, counseling and guidance, physical and mental restoration services, and vocational and other training services.
16.5.7 Program Interactions
States are required to determine if comparable services and benefits are available to their clients or their families under other programs. This requirement does not apply to the following services: evaluation of rehabilitation potential; counseling, guidance, and referral; vocational and other training services; placement; rehabilitation engineering services; and post-employment services.
16.5.8 Program Data
The number of clients served each year in the program has decreased from 1,095,139 in 1980 to 917,482 in 1987, although in the last five years the decline in the number of clients served has leveled off. In 1985, 28.3% of the clients were served at a cost of $100 to $1,000 per client per year, 15.9% at a cost between $1,000 and $2,000, 15.1% at a cost between $2,000 and $4,000, and 10.6% cost over $4,000 per year. In 1987, 62.1% of the severely disabled clients were rehabilitated in that they found work and maintained the job for at least 60 days under the program, with most States' severely disabled rehabilitation rate falling between 50 and 70%.
| EXHIBIT 16-7: Annual Number of Clients Served by State Vocational Rehabilitation Programs: 1980 to 1987 |
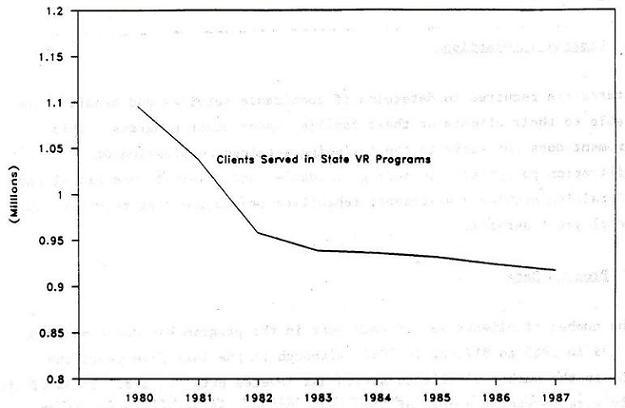 |
| EXHIBIT 16-8: Annual Federal Funding for State Vocational Rehabilitation Programs 1982 to 1990 |
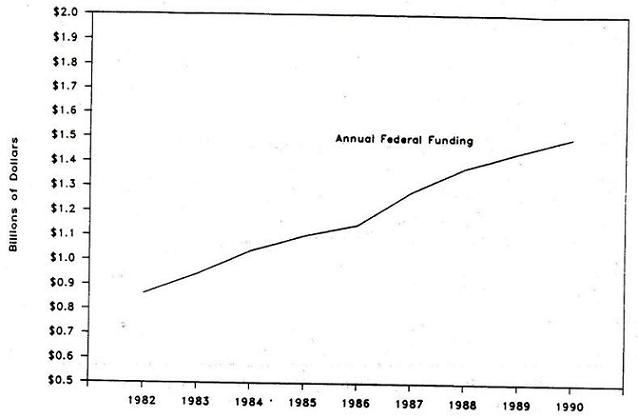 |
| 1989 and 1990 data are estimated. |
NOTES
-
At the time of this writing, new regulations effective January 1, 1990 will raise the SGA level for persons with disabilities other than blindness from $300 to $500 per month.
-
Effective January 1, 1990, a trial work period will be defined as any month in which earnings exceed $200. Earnings of less than $200 per month will not be counted as a trial work period.
-
In some cases, reversals of initial denials reflect a deterioration of the applicants functional abilities during the period of the appeal, and new medical evidence submitted to support that deterioration.
-
General Accounting Office: Social Security: Little Success Achieved in Rehabilitation Disabled Beneficiaries. HRD-88-11, Washington, D.C., December 1987.
-
Packard, M.: Income of New Disabled-Worker Beneficiaries and Their Families: Findings from the New Beneficiary Survey. Social Security Bulletin Vol. 50(3):5-23, March 1987.
-
Note that persons age 65 and over are only required to meet the financial criteria for SSI benefits, so that disabled persons age 65 and over are not required to undergo a disability determination.
-
Note, however, that the ability to earn income at the SGA level is still taken into account in the disability determination process of new SSI applicants.
-
Rymer, M. and Burwell, B.: Access to the Medicaid and Medicare Programs By the Low-Income Disabled. Prepared by SysteMetrics/McGraw-Hill for the Office of Research, Health Care Financing Administration under Contract No. HCFA-89-0333, June 1989.
-
Coe, R.D. Nonparticipation in the SSI Program by the Eligible Elderly. Southern Economic Journal Vol. 51, No. 3: 891-897, June 1985.
-
ICF, Incorporated: Rates of Participation of the Elderly in the Supplemental Security Income Program (SSI). A Background Paper prepared for The Commonwealth Fund Commission on Elderly People Living Alone. Background Paper Series: No. 9. Baltimore, MD, January 1988.
-
Social Security Administration, Social Security Bulletin, Annual Statistical Supplement, 1988. Tables 9.A.6 and 9.A.7.
-
Scott, C.G. A Study of Supplemental Security Income Awardees. Social Security Bulletin, Volume 52, No. 2: 2-13, February 1989.
-
The Veterans Administrations was redesignated the Department of Veterans Affairs in 1988.
-
Pneumoconiosis is a disease of the lungs caused by the habitual inhalation of irritant mineral or metallic particles.
-
This summary of the Medicare program incorporates the repeal of the Medicare Catastrophic Coverage Act of 1988 and therefore describes program eligibility and coverage benefits which were in effect in January 1990.
-
A spell of illness, also referred to as a benefit period generally begins when covered inpatient hospital services are initially furnished to an entitled individual and ends with the close of a period of 60 consecutive days during which the beneficiary was neither a patient in a hospital or a skilled nursing facility.
-
Bye, B.V. and Riley, G.F.: Eliminating the Medicare Waiting Period for Social Security Disabled-Worker Beneficiaries. Social Security Bulletin, Volume 52, Number 5: 2-15, May 1989.
-
Bye, B.V. and Riley, G.F.: Eliminating the Medicare Waiting Period for Social Security Disabled-Worker Beneficiaries. Social Security Bulletin, Vol. 52 (5):2-15, May 1989.
-
Bye, B.V. and Riley, G.F., op. cit.
-
In 1987, a total of 126,980 persons with end-stage renal disease received Medicare benefits, and of these, 47,216 (37%) were eligible on the basis of their medical diagnosis only.
-
This figure only includes persons who were both enrolled in Medicaid in 1988 and received a Medicaid-funded service. National data are not available on the number of persons who are enrolled in Medicaid but do not use any Medicaid-funded services.
-
Persons who receive Medicaid coverage but who do not receive AFDC or SSI cash assistance are generally referred to as non-cash recipients. State Medicaid agencies may contract with their own State Disability Determination Service (DDS) to determine the disability status of non-cash applicants, or they may elect to establish their own State Medical Review Teams (SMRTs) within their own Medicaid agency to conduct disability determinations of non-cash applicants.
-
States, of course, may provide Medicaid to additional groups or provide additional services than those stipulated under Federal law, but the costs of these Medicaid payments are not eligible for Federal Financial Participation (FFP).
-
In establishing eligibility for Medicaid under the medically needy spend down provision, States may use different accounting periods in determining the applicants spend-down obligation. These periods may range from 1 month up to 6 months. A six-month accounting period requires the applicant to meet a higher spend-down obligation prior to establishing eligibility for Medicaid, but once eligible, the individual remains eligible for the remainder of the six-month period.
-
Deeming of income and resources from parents to a disabled child continues as long the child lives in the same household as the parent(s) and the child is under the age of 18. Once a child turns 18 years of age, parental income is no longer deemed available in determining eligibility for SSI or Medicaid, even if the disabled child still resides with his or her parents, except if the child is a student and lives at home, in which case deeming of parental income continues until the child reaches age 21.
-
National data are not available on the number of persons who are enrolled in the Medicaid program, only on those who receive at least one Medicaid-funded service (referred to as recipients). Among the disabled, approximately 85-90 percent of Medicaid enrollees are recipients.
-
Most institutionalized recipients are non-cash recipients due to the reduced SSI benefit standard for persons in Medicaid-certified facilities (see Chapter 3).
-
Adams, E.K., Ellwood, M.R. and Pine, P.L.: Utilization and Expenditures Under Medicaid for Supplemental Security Income Disabled. Health Care Financing Review, Volume 11, No. 1:1-24, Fall 1989.
-
Rymer, M. and Burwell, B.: Access to the Medicaid and Medicare Programs by the Low-Income Disabled. Prepared by SysteMetrics/McGraw-Hill under Contract No. HCFA-89-0333 for the Office of Research and Demonstrations, Health Care Financing Administration, May 1989.
-
Braddock, D., Hemp, R., and Fujiura, G. Public Expenditures for Mental Retardation and Developmental Disability, 2nd Edition. Institute for the Study of Developmental Disabilities, University of Illinois at Chicago, 1986.
-
U.S. Congress, Office of Technology Assessment, Technology-Dependent Children: Hospital v. Home Care--A Technical Memorandum, OTA-TM-H-38 (Washington, DC: U.S. Government Printing Office, May 1987).
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services Home [http://www.hhs.gov]