
This report provides a review of available information on self-directed care (SDC) programs in mental health care settings and discusses potential policy implications of large-scale implementation of SDC programs serving persons with serious mental illness. Although SDC holds great promise to address deficiencies in mental health care, SDC also has the potential to re-invent within a new program setting some of these same problems. Building checks and balances into the design of mental health SDC programs is consequently needed to ensure that all consumers have an opportunity to participate and benefit from SDC.
"Executive Summary
Self-directed care (SDC) is an innovative program model for persons with disabilities, in which participants control an individual budget and are empowered to customize their own service plans in accordance with their preferences. The SDC approach has been used extensively to serve individuals with long-term service and support needs, including those with physical disabilities or intellectual disabilities. However, it has been used only minimally in programs that serve individuals with chronic mental health conditions. During the past decade, a few SDC programs for clients of state public mental health systems have been implemented on a trial or continuing basis in some states. Experience with these programs has led policymakers in some states to consider offering SDC to persons with a serious mental illness as a standard component of their state Medicaid plans. Although proposals to implement mental health SDC more widely within Medicaid is supported by many mental health system stakeholders, critical questions remain regarding how to successfully implement SDC programs for mental health care consumers in Medicaid.
In 2003, there was only one mental health SDC program in the United States. Since then, mental health SDC programs have been formed in at least seven other states. Although this initial phase of pilot and demonstration programs has yielded important information about mental health SDC, these programs were generally not designed for large-scale implementation within Medicaid. To make SDC a practical service model for large numbers of Medicaid beneficiaries with mental health disabilities, the mental health SDC program model will likely have to evolve and become more standardized, and new administrative infrastructure and training supports may be necessary.
The passage of the 2010 Affordable Care Act (ACA) removed key regulatory barriers to financing mental health SDC programs using Medicaid. The ACA created new state Medicaid plan options, which will allow states to offer recipients supportive services within a framework of person-centered planning and individual budgets. These provisions substantially expand states' options for implementing SDC programs in their public mental health systems. The extent to which states will utilize these new options to create streams of financing for SDC programs is still uncertain.
A key argument in favor of the SDC approach is that it has potential to offset prevalent sources of consumer dissatisfaction with mental health care, including restrictions on choice of providers and services, fragmentation of services and providers, inconsistent involvement of consumers in shared clinical decision-making, and inconsistent adoption of recovery oriented services and practices. The greater control SDC offers in relation to planning one's own care may help align service plans with consumers' preferences and could encourage more programs and providers to adopt a recovery orientation. SDC also offers consumers greater flexibility to pay providers and purchase goods and services that usually could not be purchased in a traditional Medicaid plan or other health plan. This greater flexibility allows a re-allocation of some mental health spending from traditional to non-traditional mental health care goods, services, and providers. This re-allocation could encourage greater innovation in mental health service delivery, as innovative services and programs could obtain reimbursement directly from SDC participants. Innovative programs and services would consequently not be subject to the usual approval processes of insurers and managed care companies, processes which may impede innovation.
On the other hand, greater consumer decision-making authority over spending and greater flexibility in paying for non-traditional goods and services, two core features of the SDC approach, raise potential complications for mental health SDC programs. Key issues for mental health SDC programs include how to sustain programs' fiscal solvency and the integrity of public mental health care financing; how to engage persons who have relatively more severe mental health conditions in SDC programs and how to sustain their program participation; and how to sustain or improve participants' satisfaction with public mental health care, as well as the quality of mental health care they receive. In particular, mental health SDC programs will need to:
-
Conduct outreach and establish enrollment procedures that support participation by a broad range of consumers who may want to consider SDC.
-
Provide adequate education about SDC and decision-making supports to participants, some of whom may have decisional impairments and variable service needs.
-
Provide adequate education about SDC to clinicians and other related clinical and administrative staff.
-
Provide adequate staff training and administrative support, which may require additional information systems and other administrative infrastructure.
-
Have adequate infrastructure, administrative capacities, and procedures to respond rapidly and flexibly to changes in SDC participant status resulting from mental health crises, changes in physical health, or changing life circumstances.
-
Protect participants from coercion or exploitation and protect them from harm during acute psychiatric episodes.
-
Ensure that the quality of mental health care is maintained or improved.
-
Establish reasonable standards around approvable purchases.
-
Monitor participants' spending and maintain programs' total costs (i.e., variable plus fixed costs) at acceptable levels.
Another factor that should be considered for the implementation of SDC is that prior research studies and demonstration program evaluations offer only limited information regarding the clinical benefits, budgetary consequences, and implementation issues surrounding mental health SDC programs. One conclusion that is well substantiated by prior research studies is that most clients favor SDC compared to traditional mental health care. However, empirical data regarding the impact of SDC on quality of life, long-term clinical outcomes, and cost savings are largely unavailable. Small sample sizes across pilot sites, data quality issues, and weak evaluation designs have hampered prior assessments the impacts of SDC. Moreover, large-scale implementation of SDC raises some practical issues around organization and financing of SDC programs that did not arise in earlier evaluations of small programs. For instance, large-scale implementation may require a significant culture change among traditional service providers, specialized accommodations for long-term consumers of behavioral health services, and considerable upfront investment in infrastructure development and training for both providers and consumers.
Offering persons with serious mental health conditions the opportunity to manage some of their health care dollars will move mental health care consumers, providers, and program administrators alike into new and perhaps unfamiliar territory. Consequently, successful large-scale implementation of SDC will require some re-engineering of existing partnerships among public mental health administrations, payer systems, clinicians, consumers, and case managers or financial managers. In addition, a flexible administrative infrastructure that is responsive to shifts in consumer mental health status may be critical to the long-term success of mental health SDC. Although similar issues have been navigated in prior, small-scale implementations of pilot and demonstration mental health SDC programs, larger-scale implementation of SDC within Medicaid may result in a greater degree of logistical and regulatory complexity around clinical care coordination, budgetary oversight, consumer participation, and training. As a result, further experimentation by states with the implementation of mental health SDC programs on a larger scale could yield critical lessons for the planners of future SDC programs.
1. Introduction
Self-directed care (SDC) is an innovative program model for persons with disabilities, in which participants control an individual budget and are empowered to customize their own service plans in accordance with their preferences.1, 2 The SDC model is particularly well designed to promote consumer and family driven mental health care, one of the six goals of the President's New Freedom Commission (PNFC) on Mental Health.3 In its 2003 final report, the PNFC envisioned a larger role for consumers and families in managing the funding for their services, treatments, and supports, a change that was expected to enhance their choices and increase service system accountability. The SDC approach is now being considered by some states for larger-scale implementation in Medicaid-financed public mental health programs, suggesting there is a need to examine issues that may arise when adapting the SDC approach on a large-scale for programs serving persons with serious mental illness (SMI).
Although active consumer involvement in services planning and clinical decision-making are now fairly well accepted principles, mental health systems have not consistently implemented changes needed to ensure that consumers are involved in directing their own care. By contrast, the SDC model puts consumers "in the driver's seat"2 in that they are imbued with the authority to select goods and services they decide will best meet their needs, even when those goods and services have not traditionally been reimbursed by payers. SDC program participants control how some portion of public financing is spent, choose their own providers, and have final decision-making authority over many or most aspects of service provision.4 As a result of this flexibility, SDC has the potential to overcome mental health program inertia, which might be impeding the adoption of new policies to encourage consumer involvement in decision-making and a more uniform recovery orientation among providers and programs.
During the past decade, a movement to implement SDC as a standard component of public mental health systems and offer it to persons with a SMI has attracted considerable support. The 2003 final report of the PNFC on Mental Health3 highlighted the success of the Cash and Counseling program, a SDC model for persons with physical and developmental disabilities, and endorsed it as a promising model for adaptation to mental health systems. Several federal agencies, including the Substance Abuse and Mental Health Services Administration (SAMHSA), the Centers for Medicare and Medicaid Services (CMS) and the Institute of Medicine, are now encouraging adoption of SDC in states' public mental health systems. In addition, recent changes in federal regulations, which give states new options for obtaining federal Medicaid matching funds for home and community-based services (HCBS), have made SDC programs for persons with SMI more financially viable within Medicaid.
However, the prospect of a larger-scale implementation of SDC programs for persons with SMI raises critical implementation considerations about which there is currently little information available. Greater consumer decision-making authority over spending and greater flexibility in paying for non-traditional goods and services, two core features of the SDC approach, could result in various challenges for consumers, providers, SDC programs, and public mental health agencies. Additional discussion and examination of these features of mental health SDC programs, especially in the context of programs serving large numbers of consumers within a Medicaid plan, may help clarify critical issues for large-scale implementation of mental health SDC in Medicaid.
1.1. Background
Early Self-Directed Care Programs
The concept of consumer self-direction or "consumer direction" emerged out of the independent living and disability rights movements.4, 5, 6 A tenet of these movements is that persons with disabilities can live successfully in community settings if they are given adequate supports in the form of personal assistance services, assistive technologies, home modifications, and various other enabling products and services. Advocates also maintain that persons with disabilities should be afforded as much independence and autonomy as possible in decisions about the types, amounts, and sources of the personal assistance services they receive. Independence and autonomy in decision-making are thought to be critical in order to achieve the highest quality of care and the best match between the services that are provided and consumers' service needs,4 especially given that consumers' needs are constantly changing as their health status and life circumstances change.
Similar themes have been a mainstay of mental health consumer movements at least since the 1960s and "deinstitutionalization."7 Indeed, mental health advocates have consistently endorsed greater independence and control over treatment decisions by persons receiving mental health services.8 A contemporary statement of this position can be found in the 2003 final report of the PNFC on Mental Health.3 The PNFC concluded that autonomy and person-centered care are essential for successful transformation of the mental health service delivery system. Moreover, services must be geared to give consumers "real and meaningful choices" about treatment options and providers and must "not be oriented to the requirements of bureaucracies."3
The first generation of SDC programs predominantly served persons with developmental or physical disabilities. In 1993, the Robert Wood Johnson Foundation (RWJF) provided funding for the New Hampshire Self-Determination Project, a demonstration program for persons with developmental disabilities that included individual budgets and person-centered planning.9 The program enrolled 45 individuals and their families. In an independent project evaluation, Conroy and Yuskauskas compared 27 participants' quality of life at 18 months after they entered the program to quality of life at program entry.10 At 18 months post-entry, participants reported significantly greater quality of life in all domains except family relationships.
The RWJF subsequently funded self-determination initiatives in 18 additional states. Each state designed and implemented its own unique SDC model, but all the models included core elements such as person-centered planning, individual budgets, and personal assistance to help consumers manage their service plans. An independent pre-/post-entry evaluation of consumers' outcomes in six states' programs showed mixed findings across outcome domains and states.11 The most consistent finding was a significant improvement in consumers' quality of life. In a system-level evaluation of the RWJF self-determination initiatives,12 it was found that participants in some states had better options in relation to personal assistance services than did participants in other states, a consequence partly of state-specific policies that pre-dated implementation of the self-determination initiatives. As a result, the overall success of each RWJF self-determination initiative may have been impacted by many system features specific to the geographic locations of the programs.
Cash and Counseling
The Cash and Counseling Demonstration and Evaluation Project13 provided the first rigorous comparison of a SDC model to traditional care for disabled Medicaid enrollees. Beginning in the mid-1990s with grants from the RWJF and the Office of the Assistant Secretary for Planning and Evaluation (ASPE), the Cash and Counseling Demonstration was an experimental trial of the SDC approach for adults with disabilities, elders and children with developmental disabilities. Participants at program sites in Arkansas, Florida, and New Jersey were randomly assigned either to Cash and Counseling or to traditional agency services. Participants in the Cash and Counseling group received individual budgets, access to financial counseling, and other administrative supports.
The Cash and Counseling Demonstration and Evaluation Project resulted in several key findings.14, 15, 16, 17, 18, 19 Participation in Cash and Counseling resulted in fewer unmet personal care needs, greater satisfaction with services, and greater overall life satisfaction compared to participation in traditional agency services. Participation in Cash and Counseling also resulted in similar, and in a few respects, better health outcomes on average compared to agency-based care. Largely by increasing access to paid care, Cash and Counseling also increased home care expenditures. This increase was partially offset by savings from lower Medicaid expenditures for nursing home and home health care. However, total Medicaid expenditures per participant were greater in Cash and Counseling than in traditional agency care: the median differential over the first 2 years after enrollment in Cash and Counseling was 8 percent, with a range of 4-14 percent across states and target groups.19
Cash and Counseling also benefitted family caregivers. Caregivers were more satisfied with and confident in the care they provided and reported greater life satisfaction and better health compared to the caregivers of consumers receiving agency care.17 Monies paid to family member caregivers by participants for services rendered likely accounted for some proportion of these beneficial effects, though the magnitudes of these effects could not be quantitatively determined. The Cash and Counseling Demonstration and Evaluation Project led to the replication of Cash and Counseling sites in an additional 12 states beginning in 2004.13
Mental Health Self-Directed Care Programs
The first mental health SDC program (i.e., the first SDC program designed for persons with mental health disabilities), Florida SDC, was started in 2002 in northeastern Florida.20 Mental health SDC programs for persons with SMI were later formed in at least seven other states: Iowa, Maryland, Michigan, New Hampshire, Oregon, Pennsylvania, and Texas.a This initial wave of pilot and demonstration mental health SDC programs may or may not provide exemplary models for future implementations of mental health SDC on a larger scale. All of these programs put together have had only approximately 1000 participants, some of the programs were in operation less than 5 years before being disbanded, and very few programs used Medicaid as their primary source of financial support. These programs and the results of related program evaluations and other research will be described later in this report.
In mental health SDC programs consumers direct their own treatment planning and have control over an individual budget. Individual budgets may be used to purchase both traditional and non-traditional mental health goods and services, including professional training and education, transportation, clothing, gym memberships, and potentially many other types of goods and services. This authority to plan the spending of money allocated for one's treatment and to purchase non-traditional mental health goods and services, even if these goods and services are not reimbursable under a traditional reimbursement system, separates SDC from other person-centered mental health service delivery approaches. Another core attribute of SDC is that SDC program participants are permitted to contract for services with essentially any willing provider of a service, regardless of whether that provider would ordinarily qualify for reimbursement from Medicaid or managed behavioral health care plans.
The SDC approach could help address some of the most critical sources of consumer dissatisfaction with mental health care. It may permit consumers to circumvent rigidities in mental health payment systems that have historically impeded integration of mental health with substance use treatment and physical health care services; limited consumer choice of providers, services, and medications; prevented consumers from obtaining those supports that may be needed to live independently in the community; and discouraged innovation in service delivery, including greater adoption of recovery oriented services and practices.3, 21
Public mental health payment systems in many cases are not sufficiently flexible to accommodate individuals' preferences for providers and services and may stifle innovation in service delivery. With the aim of instituting uniform standards and public accountability, states and the Federal Government traditionally stipulate regulatory (e.g., professional training and licensing) requirements that mental health care providers must satisfy in order to be eligible for reimbursement for the care they provide. In addition, public mental health systems usually specify the services that can be provided, the schedule of fees paid to providers, the frequency of service encounters, and other aspects of mental health treatment. These rules often become restrictive over time because they do not change quickly or at all in response to scientific advances in mental health intervention, evolving conventions of best clinical practice, or changes in consumers' preferences. As a result, in traditional systems, consumers and their providers may be aware of newer, better, or preferred treatment modalities but are effectively prevented from accessing them due to rigidities in payment systems.
One situation that exemplifies the challenges resulting from payment system rigidities is the slow development of medical homes and other services that integrate supports needed by persons with co-occurring chronic mental and physical health conditions. Chronic medical conditions contribute to overall disability in at least half of all persons with mental health disabilities.24 Although the need for integrated primary care models, care coordination services, in-home supports, and other services for persons with complex mental and physical health conditions is widely recognized by health care providers and experts, payments for integrated physical-mental health care services in many systems are either prohibited or severely restricted. As a result of the greater purchasing flexibility in SDC, participants in SDC programs would, in principle, have an opportunity to re-direct mental health spending from traditional outpatient programs to innovative programs that offer integrated mental health and physical health care services.
In addition, the greater degree of discretion and flexibility offered by SDC to switch from one care provider to another could help promote "shared decision-making" in mental health clinical encounters.23 "Shared decision-making" denotes an interactive process in which clients and practitioners collaborate to make health care decisions.23 Evidence from research indicates that although many persons with SMI would like to participate actively in decisions about their psychiatric care, especially in relation to selection and use of psychiatric medications, most rate their current roles in decisions about psychiatric care as "passive."25 Mentalhealth SDC programs could alter the dynamics of interactions between mental health providers and clients, because SDC in principle expands participants' opportunities to change providers. The option to "fire" one's provider theoretically should improve clients' bargaining power with providers, and consequently would be expected to result in clients having greater input into decisions, if they so desire.
Health Care Reform and Medicaid
The numbers of public sector mental health care consumers will continue to grow in the next few years, as millions of additional Americans will obtain public health care coverage under the 2010 Affordable Care Act (ACA). The Congressional Budget Office estimates that by 2016 an additional 16 million non-elderly persons will enroll in Medicaid and the Children's Health Insurance Program (CHIP), raising the total number of non-elderly participants in these two programs to 51 million in 2016 from 35 million today.26 Based on these projected enrollments and the prevalence of persons with serious mental health problems in the uninsured population, it has been estimated that he number of non-elderly adult Medicaid enrollees with one or more serious mental health problems may nearly double (an estimated increase of 1.988 million persons or +91.5 percent), from 2.174 million to 4.162 million persons.27 SDC and other person-centered service delivery models may prove to be instrumental in managing the resulting growth in public mental health services utilization and in aligning the availability of services and providers with consumers' needs and preferences.
The 2010 ACA also creates new opportunities for financing SDC in public mental health systems. Using the 1915(i) Medicaid State Plan Option of the Social Security Act (SSA), a section first introduced as part of the 2005 Deficit Reduction Act, states can use Medicaid to reimburse providers of innovative HCBS without requiring that participants have an institutional level of need for care and without having to demonstrate that service expansions will be budget-neutral to Medicaid. However, few states have utilized the 1915(i) mechanism since it became law in 2005. The 2010 ACA removed regulatory barriers that may have prevented some states from using the 1915(i) mechanism. It also stipulated that states' 1915(i) plans must include a person-centered planning process and participating consumers should be offered the opportunity to self-direct some or all of their HCBS.28
The 1915(k) Community First Choice Option, which was added to the SSA by the ACA, is a new state plan option for the provision of community-based long-term care services in Medicaid to persons with incomes up to 150 percent of the federal poverty line who have an institutional level of need for care. Consistent with the decision of the 1999 U.S. Supreme Court in Olmstead v. L.C., this option will permit states to develop or enhance a comprehensive system of long-term care services and supports in the community rather than in institutions. States that utilize this option must offer choice through person-centered planning and self-direction.
1.2. Objectives of this Report
Although implementation of mental health SDC programs on a larger scale may now be feasible, critical questions remain regarding how to make such an implementation successful for mental health care consumers, providers, policymakers, and public budgets. This report provides a review of available information on mental health SDC programs and presents several issues that may require further examination, discussion, planning and decision-making prior to SDC program implementation. Most of these implementation issues could be addressed in more than one way, and this report does not provide an exhaustive list of policy options. Rather, relevant issues are brought forward for further examination and discussion.
One set of issues relates to the chronic and episodic nature of SMI. Persons with SMI typically have ongoing psychiatric symptoms with periodic acute exacerbations and improvements that may differ widely across individuals.32 Especially during acute exacerbations, cognitive impairments and psychiatric symptoms can impede decision-making. Also, unexpected changes in life circumstances, such as the loss of permanent housing, are common and can be associated with dramatic changes in a person's need for service supports.
Variability over time in participants' acuity of illness, ability to make decisions, and life circumstances indicates the need for specialized features in mental health SDC programs, as compared with SDC programs for persons with physical disabilities. In SDC, participants and program staff share responsibility for modifying participants' treatment plans as participants' needs change, with program staff serving primarily in an advisory capacity. By itself, this arrangement may be inadequate to ensure that participants' basic needs are met at all times. As a result, programs need standard operating procedures for maintaining regular contact with participants and for involving providers when participants are too ill to make rational decisions about their care.
Some SDC program participants or potential participants may have severe and persistent cognitive and/or functional impairments.29, 30, 31 Consequently, SDC programs should have strategies that help such persons compensate for impairments that may be preventing them from self-directing their own care and engaging in a recovery process. Some potential SDC participants, especially persons who may have a long history of involvement in public mental health systems, may not initially feel comfortable with the notion of self-directing their own care. Especially for individuals accustomed to a representative payee culture, the transition to SDC and budget management represents a significant shift not to be undertaken lightly. SDC programs must consequently be prepared to offer education and targeted outreach. SDC programs must also be prepared to work with participants who have representative payees or conservators, persons who manage their clients' finances and spending. In addition, the impact on consumers of participating in and perhaps not being able to remain in SDC has implications as well and may impact recruitment strategies for SDC and clinician care for SDC participants.
To ensure that participation in SDC in fact results in greater choice for participants with behavioral health issues, the complexities associated with training participants in budgeting and financial management as well as the development of safeguards, such as advance directives in the event of changes in mental health status changes, must be addressed in the initial planning and implementation phases. The clinician, coach, or case manager must be able to rapidly implement a real-time shift in financial management, directly with the client and within the framework that alerts the payor to this shift.
Similarly, SDC programs will need to create protections for persons with SMI from coercion and victimization by fiscal intermediaries, service providers, or family members. One issue is the possibility of coercion from existing service providers, representative payees, or family members aimed at persuading a person with SMI not to participate in SDC. Coercion not to participate could be motivated, for example, by wariness of a loss of control over a potential SDC participant's decisions regarding treatment or spending or by concern that a potential participant will not receive adequate guidance in SDC and will consequently make poor decisions. Another issue is the possibility of interference with specific decisions by a SDC program participant around spending and choice of service providers. Fiscal intermediaries, service providers, or family members could have various motivations to interfere with a participant's decision-making, including financial incentives, stigmatizing beliefs about the participant's capacity for decision-making, or concern for a participant's welfare.
Ensuring that consumers obtain effective, high quality care and that public mental health care financing is used effectively will require additional supports and safeguards. SDC programs should help protect participants from vendors of services and products that may be ineffective or harmful. Making determinations regarding appropriate expenditures of SDC money is handled in diverse ways by different programs and requires some thoughtful decisions by those implementing the programs and the consumers participating in them.
SDC programs also must be able to assure the public that limited mental health financing is being used effectively in support of the mental health care needs of persons with disabilities. Some services or products that participants would like to purchase may be insufficiently related to recovery from mental illness or may not meet community standards for appropriate uses of public disability support. Moreover, to the extent that evidence-based treatments and supports are more cost-effective than interventions having no evidence base, the public's interest in effective use of public mental health financing must be balanced against the principle of self-direction. This suggests the need for explicit purchasing policies and a process for involving consumers and other stakeholders in selecting these policies.
The consequences for programs' budgetary costs and for obtaining financing needed to support programs' infrastructure must be considered in conjunction with nearly every aspect of program design. Implementation of mental health SDC programs on a larger scale would require a transformation of standards of practice in mental health care service delivery and a substantial upfront investment in training and system re-design. There may also be costs associated with creating and operating an administrative infrastructure that provides adequate oversight of spending by SDC participants. It is not yet known how much it will cost to create these infrastructures and it has not yet been determined who will be responsible for these costs.
Finally, policymakers must decide who will bear the financial risks associated with SDC programs. In traditional public mental health service systems, financial risks are usually borne by the state mental health authority and/or by Medicaid. These risks traditionally have been managed using a variety of regulatory controls, including especially pre-authorization of service use. However, in SDC programs, participants' expenditures are generally not subjected to the same types of regulatory controls. As a result, planners of SDC programs must decide who is responsible for financial losses that may occur when SDC participants require additional mental health services but have no money left over in their individual accounts. Planners have various options for addressing this risk, options which have varying advantages or disadvantages for consumers.
The following sections of this report provide an overview of mental health SDC programs and discuss implementation and financing issues, introduced above. The remainder of the report is divided into sections for the following topics:
- report methodology;
- main features of mental health SDC programs;
- critical issues in the design of SDC programs;
- results from research and evaluation studies of the costs and benefits of SDC programs for people with SMI; and
- conclusions.
2. Methodology
This report is based on a review of published and unpublished academic articles, presentations, and policy documents and on interviews with key informants. Literature and other documents were obtained by Internet search and by requesting information from experts on SDC and other consumer-directed service models. A 2007 ASPE report on the use of the SDC model in mental health care settings33 was a key source for information on SDC programs. Interviews with key informants--state and federal policymakers, academic experts, consumer advocates and consumers, private insurance representatives in companies serving the public sector, and SDC program representatives--were conducted by the authors from December 2011 to January 2012.
Key informants were nominated by ASPE staff. Nominations were based on knowledge of SDC and other consumer-directed services. Key informant interviews focused on conceptual advantages of mental health SDC compared to traditional mental health care, risks of SDC to consumers and to the quality of care, impacts on public budgets, key features of SDC programs, infrastructure and staffing needs, potential sources of financing, and implementation barriers. Interview questions were selected by the authors in consultation with ASPE staff and sent to each key informant in advance of the interview.
Thirty persons were invited to participate in key informant interviews. Eighteen did not respond to the initial invitation and were sent a second invitation. Reponses were eventually received from 13 of the invitees, two of whom declined the interview. These key informants included representatives of mental health SDC programs in four states, as well as persons with knowledge of multiple mental health SDC programs. Three of the key informants had specific expertise in the Cash and Counseling program model and other consumer-directed services. One key informant had direct experience as a participant in SDC.
Key informants had three options for communicating their responses to interview questions: telephone interview only (n=7), telephone interview and written response (2), and written response only (4). Although the list of prepared questions generally guided the interviews, key informants were allowed to skip any given question, some of their responses addressed issues that had not been raised in the prepared questions, and some ad hoc questions were posed depending on a key informant's prior response. Telephone interviews lasted between 17 and 156 minutes. These were audio-recorded and the recordings were subsequently reviewed to identify key points and common themes. Written summaries of key informant interviews were prepared and compared to the original recordings for completeness and accuracy.
3. Features of Mental Health Self-directed CARE
3.1. Program Elements
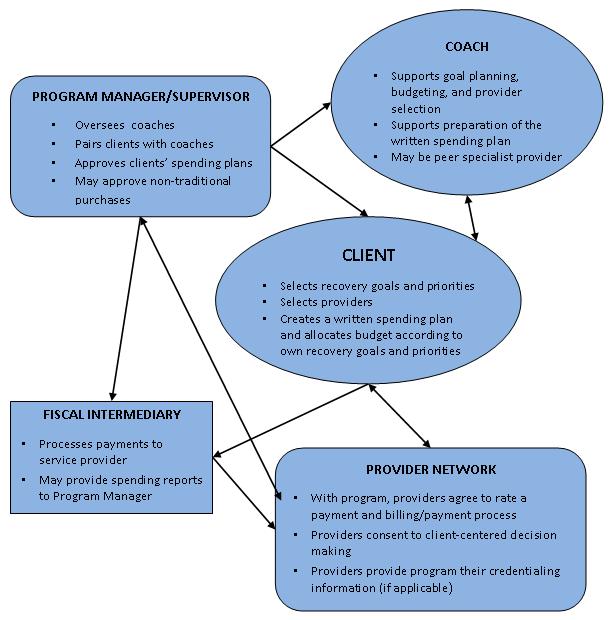
Although mental health SDC programs vary in design and staffing, most programs include the following elements (see Figure 1):1, 2
| FIGURE 1. Program Elements |
|---|
 |
Recovery Plans
Client participants with assistance from coaches (see description, below) create a "recovery plan," a detailed statement of personal recovery goals and corresponding action items. Recovery goals may be broad ranging across domains such as employment, education and training, physical and behavioral health, housing, social interaction, and hobbies.
Budgeting
Client participants with assistance from coaches (description below) create a personalized plan for spending on both traditional and non-traditional products and services, where traditional services are usually defined as those services covered by Medicaid. The total budget available to each individual is determined by the SDC program's administrators, and sometimes varies across individual participants depending on their expected needs or other factors. Budget amounts are specified in the spending plan for each of the services and products included in a consumer's "recovery plan," a detailed statement of recovery goals and corresponding action items. In most programs, program managers or supervisors (description below) are responsible for approving these spending plans.
Coaches
Coaches assist SDC participants in developing their "recovery plan," support the budgeting process, may offer advice on spending priorities, and serve as a mentor and resource. Coaches are variously termed recovery coach, life coach, support broker, support specialist, and peer-specialist. Coaches receive training in self-directed planning and recovery oriented care. Some programs hire "peers" (i.e., persons who themselves are in recovery and who embody the hope for recovery) into paid positions as SDC coaches, whereas other programs hire professional case managers who have received training in the SDC approach.
Program Manager/Supervisor
The program manager or supervisor is responsible for employing and supervising coaches, pairing SDC participants with coaches, ensuring that coaches receive appropriate training, ensuring regulatory compliance (e.g., with state mental health and Medicaid regulations), approving budgets and individual participants spending plans, and other executive functions of SDC program administration. In some programs, the program manager is responsible for approving participants' purchases of non-traditional products and services, in accordance with the SDC program's purchasing policies.
Fiscal Intermediary
A fiscal (or financial) intermediary in SDC is an agent that processes payments to service providers and helps manage accounting and other fiscal responsibilities, such as handling, managing, and accounting for funds in individual budgets, preparing payroll taxes (for personal assistance services employees) and maintaining required tax records.13 A SDC program may also contract with a fiscal intermediary to handle other tasks, such as providing standardized reports to the SDC program and its participants regarding participants' services utilization and expenditures. A fiscal intermediary could also be responsible for helping ensure that participants do not exceed their budgets, for example, by providing information. The fiscal intermediary also has an obligation to ensure that all required agreements between participants and providers are in place before making payment and may perform support functions such as checking provider qualifications and conducting reference and background checks. The fiscal intermediary does not contract directly for any services and does not serve as an employer of service providers.
In mental health SDC programs, various arrangements have been made for fiscal intermediary services. In some programs, a not-for-profit community service organization has served as fiscal intermediary under a contract to the state mental health authority. In other programs, a local core serve agency, a branch of the state mental health authority, fulfills this role. In other programs, some of the functions of the fiscal intermediary are contracted out to a managed behavioral health care organization while the program administrator fulfills others. Many non-mental healthSDC programs contract with a "fiscal management entity," an independent organization that specializes in providing fiscal intermediary services to SDC programs, though this arrangement has rarely been used in mental health SDC.
Provider Network
Most SDC programs establish a provider network and do not reimburse expenses for encounters with other (non-network) providers. However, most programs accept into the network any willing provider who agrees to the SDC program's rules and accepts the SDC approach. Often a program will also negotiate with the provider a specified level of reimbursement for encounters with SDC participants. Some SDC programs also have a vetting process that includes verification of the provider's credentials and standing in the community.
Mental health SDC participants typically have not directly hired employees, such as personal care attendants frequently hired by persons with primary physical disabilities. By contrast, the employer authority (i.e., the option offered to program participants to serve as the legal employer of a service provider) is a critical feature of Cash and Counseling and other consumer-directed programs for persons with physical disabilities. For persons with physical disabilities, in-home support services and transportation services are essential in order to be able to live independently in the community. The authority to hire and fire personal assistance services providers gives participants the flexibility to select those service providers that are most likely to meet their requirements. However, in most mental health SDC programs, providers have maintained their own employment, and have been paid on a fee-for-service basis. How the employer authority might work in mental health SDC programs should be considered, as this authority would seem to be an important component of a recovery oriented approach, at least for some SDC participants.
Information Resources
Worksheets, websites, and educational materials are offered to support planning and independence from formal services. Coaches maintain a working knowledge of these resources and help direct participants to relevant ones.
Implementing and Monitoring the Recovery Plan
The participant, with the support of the life coach as necessary, monitors the recovery plan and its implementation, the spending plan, and the budget on an ongoing basis. Participants may change services, providers and supports as needed within the constraints of their individual budgets.
Consumer Oversight
Current and former SDC participants also often have key roles in the management, oversight, and administration of SDC programs. Their participation serves, in part, to ensure that the program continues to adhere to the principles of autonomy and self-direction. Consumers also may advocate for continued program funding, nominate providers to the network, and design training materials for coaches. In some SDC programs, consumers also have input into the development of purchasing policies and procedures.
3.2. Allowable Products and Services
SDC programs offer participants much greater flexibility in choosing products, services, and providers than is available in conventional mental health services. Budgets can be used to purchase specialty mental health care as well as many other products and services that are not offered by specialty mental health care providers. Examples of non-traditional products and services that participants in existing SDC programs may purchase using SDC budgets include smoking cessation programs, tuition and other education-related expenses, general medical care, and dental care.
3.3. Spending in Individual Budgets
The total amount of money individuals can spend in SDC is typically capped at values ranging from $1500 to $4000 per participant per year, depending on the program.33 Some programs "cash out" outpatient mental health clinic services, which means that participants' individual budgets include the money that would have been allocated for these services, whereas other programs do not give participants control over this spending. Participants may use the money in their individual budgets to purchase specialty mental health care services (e.g., outpatient individual or group therapy) and may also purchase non-traditional services and products and other costs not covered by their insurance plans, for those who have insurance. Most programs do not stipulate the proportion of the individual budget that participants must spend on specialty mental health care versus other products/services, though some do, particularly for persons who are uninsured. Some SDC programs use suggested formulas such as asking participants to spend a certain proportion of their budget on traditional mental health services, usually defined as those services covered by Medicaid.
Individuals enrolled in Medicaid can utilize Medicaid-covered services with minimal out-of-pocket expense. However, Medicaid benefits in some states may not include some traditional mental health services, such as supported employment or family psycho-education, or Medicaid coverage may not fully cover the costs of care for available providers of these services. In those cases, SDC participants may decide to pay for uncovered mental health expenses using their individual SDC budgets. Uninsured persons are eligible for enrollment in some SDC programs (e.g., Florida SDC). For the uninsured, payments for mental health services are deducted from the individual's SDC budget. In some programs, uninsured participants are also required to spend at least a specified percentage of their SDC budget on clinical services.
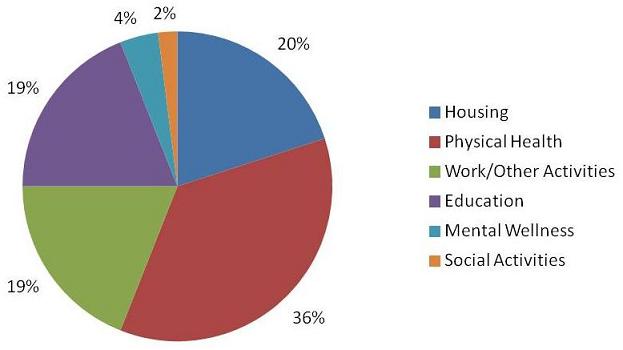
In a mental health SDC program in Delaware County, Pennsylvania individual budgets have been used to purchase a wide range of items, such as hearing and vision tests, health club memberships (for weight reduction) and nicotine patches. Figure 2 shows Freedom Funds expenditures during the first year of the program by category. The largest expenditure category was for physical health products and services (36 percent), followed by housing (20 percent), work/other activities (19 percent), education (19 percent), mental wellness (4 percent) and social activities (2 percent).
| FIGURE 2. Freedom Funds Purchases in Delaware County SDC |
|---|
 |
| SOURCE: Magellan Behavioral Health of Pennsylvania: Report to the Community, 2010. |
As pointed out by Alakeson,33 the broad categorization of spending shown in Figure 2 masks the variety of purchases made in mental health SDC programs. Physical health expenditures may be for items such as vitamins and nutritional supplements, health club memberships, vision services, hearing aids and batteries, weight loss program fees, exercise equipment, prescription drug expenses. Housing expenditures could include spending on rent, food, furniture, towels and linens, and moving expenses. Work-related expenditures could include spending on clothing, haircuts, computer software, fees for professional licensure, insurance, or car repair. Education-related expenses could include tuition, but might also include transportation, books, and computer supplies.
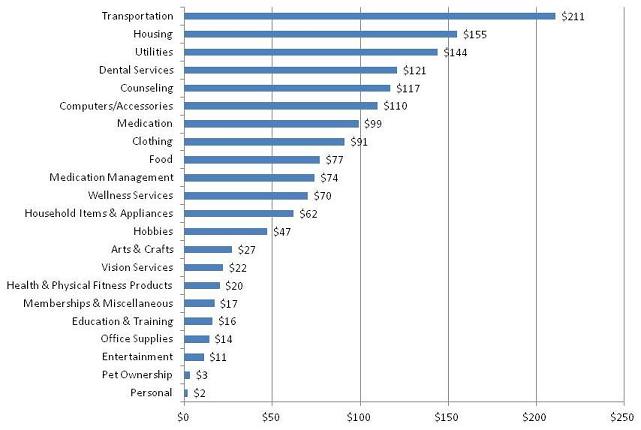
Figure 3 shows mean expenditures per person in the Florida SDC for a sample of 80 program enrollees who participated in a survey conducted by Spaulding-Givens.20 The dollar amounts are from the Florida SDC program's administrative databases and correspond to a 12-month period for each respondent sometime during fiscal years 2009 to 2010. The spending categories are those used by the SDC program. Using SDC program records, Spaulding-Givens disaggregated expenditures in a "miscellaneous" spending category into sub-categories for computers/computer accessories, household items/appliances, hobbies, arts/crafts supplies, health/physical fitness, office supplies, and memberships/miscellaneous.
| FIGURE 3. Florida SDC, Expenditures per Participant Over a 12-Month Period, by Category (Fiscal Years 2009-20010, n=80) |
|---|
 |
| SOURCE: Adapted with permission from Spaulding-Givens, J. 2001. Florida Self-Directed Care: An Exploratory Study of Participants' Characteristics, Goals, Service Utilization, and Outcomes. The Florida State University, College of Social Work: Tallahassee. |
Florida SDC participants spent $1509 per person during a 12-month period. This is only the amount paid out of participants' individual program budgets. It does not include health insurance reimbursements to mental health service providers and pharmacies for mental health care provided to participants. As shown in Figure 3, transportation had the largest mean expenditures of any category ($211 per person; 14.0 percent), followed by housing ($155 per person; 10.3 percent), utilities ($144 per person; 9.5 percent), dental services ($121 per person; 8.0 percent), and counseling ($117 per person; 7.7 percent). Medication spending ($99 per person; 6.5 percent) encompasses spending by persons who are uninsured, copayments, and any other medication expenses not covered by insurance. Wellness services ($70, 4.7 percent) include fitness club memberships and weight loss program fees as well as alternative medicine services, such as acupuncture. Although the mean values in Figure 3 may indicate a general spending pattern for the program as a whole, they do not necessarily correspond to any individual participant's spending pattern. In fact, participants' spending totals varied tremendously, from $0 to more than $3300.
3.4. Exclusions from Coverage
SDC programs generally do not include coverage for mental health visits to emergency departments or for mental health crisis, inpatient, or residential treatment services. These services also are not ones that participants self-direct or write into their recovery plans. Instead, these services are covered either by Medicaid, Medicare or private insurance, or by public mental health authorities or hospitals under uncompensated care.
There are two main reasons why "acute care" services are excluded from SDC planning. First, individuals usually do not know what expenses they will have for these services before these services are needed, and any use of these services can result in high unanticipated health care expenses. Consequently, when planning a SDC budget, most individuals would not know what amount of money to allocate for use of these services, and they might not allocate enough to cover their expenses during the course of a year. Second, public mental health systems would not want to put individuals with SMI at risk for not obtaining mental health services during periods of crisis, when they are most in need of services and most at risk of harming themselves or others. Indeed, providing or paying for services needed by individuals with SMI during periods of acute exacerbation of mental health symptoms is a primary rationale for having a public mental health system.
Psychiatric medications are not covered in most SDC programs, and psychiatric medication use is often not written into participants' SDC recovery plans. There may be no benefit to making psychiatric medications part of the SDC planning process, and there could be risks. As pointed out by one key informant, SDC participants have the option to "fire" their psychiatrist if they are unsatisfied with the medications they are being prescribed or with the medication decision-making process. Moreover, if psychiatric medications are included in SDC planning, medication expenses may affect participants' choices among medications and their use of medications over time. Such an influence could have adverse consequences for participants, including a greater risk of crises and hospitalizations. Although SDC participants are not allocated monies specifically for medications, many participants have prescription drug coverage through their health insurance plans. Also, participants usually are allowed to use part of their individual budgets to pay for medication expenses not covered by insurance.
3.5. Contrast with Traditional Services
Mental health SDC represents both a philosophical and a practical departure from the conventional approach to planning mental health care. Key informants interviewed for this report were asked to offer their perspectives on how mental health SDC differs from traditional public mental health services (i.e., those mental health services that are typically covered by Medicaid programs and states and that are administered by a state mental health authority). This section provides a summary of their comments.
As a result of having greater decision-making control, SDC program participants were thought to be more activated to establish personal goals, to select products and services that reflect their preferences and that are consistent with their goals, and to plan expenditures within a budget. One SDC expert observed that for many consumers, traditional services have not been effective in supporting them to move on in their lives and have left them disempowered and lacking in self esteem and hope. According to one member of the PNFC, SDC gives individuals a "sense of control" and "allows them to operate in the economic system, which is normalizing." The recovery oriented philosophy of SDC programs and the greater control offered by SDC over one's own care appear to be why participants generally prefer SDC to traditional services. As articulated by one SDC participant:
"[SDC provides] the freedom to have a voice and to actively participate in navigating my own personal road to recovery. [Self direction] is the ability to choose the services that will be most effective for me in reaching that destination. Self direction is the freedom to request assistance instead of receiving it based on rigid criteria for treatment. It's a method of testing my potential and responsible limits by allowing me to take ownership of the choices I make...it's about choosing professionals in those fields that will best meet [my] individual needs."
From the perspective of one public mental health system administrator interviewed for this report, SDC also tends to put participants in a position where there is a heightened sense of expectation that they are responsible for the direction of their lives. This opportunity to make one's own decisions, for better or for worse, is an integral element of self-direction. The expectation of self-responsibility is conveyed by giving participants control over an individualized budget and the authority to self-direct the service planning process. As a result, SDC participants may be more motivated to take steps towards independence and recovery than they would be otherwise, especially in comparison to institutional mental health service settings, which put consumers in a position of dependency. Compared to traditional services, SDC consequently may serve to align consumers' personal incentives with the goals of recovery oriented public mental health systems. In the words of one consumer representative:
"People who have choice and control of decisions pertaining to their lives and services are more likely to be motivated. People who are motivated are more likely to be successful."
Another key informant involved with the planning of one SDC program also emphasized the broader set of choices that SDC offers regarding providers and supports: "the whole philosophy of the [SDC] program is to take advantage of community supports not available within the traditional mental health system." These community resources may include access to additional mental health providers and programs, including private practices, and may include access to non-traditional services, such as fitness programs, transportation and education. Community resources also may include products, such as clothing for a job or household products needed to live independently. By contrast, in traditional services, the menu of reimbursable mental health programs and providers is more limited and clients are usually referred to the nearest mental health outpatient program that is accepting new clients rather than given the option to use other providers. As a result, spending in SDC can be shifted toward products, services, and providers that consumers value more highly within the constraints of a budget.
Some key informants to this report emphasized differences between the mental health SDC approach and traditional services that may impede implementation of SDC programs in Medicaid. A chief concern expressed by one key informant was how to ensure that standards for the quality of mental health care would be maintained. In public mental health systems, a minimum quality of care is ensured through provider licensing and training requirements, regulations that define the content of specific mental health services, systems' rollouts of evidence-supported practices, continuing medical education opportunities, independent performance standards, and other administrative policies. In contrast, SDC would allow consumers to select providers and services that may not be bounded by these policies. The implications of this point are discussed in Chapter 4.
Other concerns were raised regarding the much greater scope of goods and services that SDC participants may purchase in comparison to consumers in traditional outpatient mental health programs. One key informant pointed out that one reason Medicaid sets limits on the goods and services that can be purchased is to ensure the integrity of the payment system. Services that are reimbursable are all generally considered standard components of mental health treatment. By contrast, SDC programs would allow some purchases whose legitimacy could be questioned on the basis that other Medicaid recipients and other privately insured consumers may not be reimbursed by their health care plans for similar purchases. This point is further discussed in Chapter 4.
Another key informant with experience in managed behavioral health care contracting raised the concern that most SDC programs do not currently have an adequate administrative infrastructure for approving a large volume of proposed purchases. In most current mental health SDC programs, a program manager or supervisor approves participants' proposed purchases. However, the key informant indicated that if SDC programs are implemented on a much larger scale, the volume and variety of proposed purchases could overwhelm a program manager's ability to properly review each and every purchase. Consequently, in the key informant's opinion, many purchases would not be subjected to any significant review. Implications of this point for SDC program design are discussed in Chapter 4.
4. Critical Issues in the Design of Mental Health Self-directed CARE
SDC offers increased autonomy and flexibility in choosing services and providers for persons with mental health disabilities. If mental health SDC is implemented on a large-scale, mental health systems as a whole could benefit from a re-orientation of services towards a focus on recovery. However, SDC also needs checks and balances to ensure the integrity and sustainability of mental health SDC programs. Safeguards may be needed especially to ensure that SDC programs:
-
Conduct outreach and establish enrollment procedures that support participation by a broad range of consumers who may want to consider SDC.
-
Provide adequate education about SDC and decision-making supports to participants, some of whom may have decisional impairments and variable service needs.
-
Provide adequate education about SDC to clinicians and other related clinical and administrative staff.
-
Provide adequate staff training and administrative support, which may require additional information systems and other administrative infrastructure.
-
Have adequate infrastructure, administrative capacities, and procedures to respond rapidly and flexibly to changes in SDC participant status resulting from mental health crises, changes in physical health, or changing life circumstances.
-
Protect participants from coercion or exploitation and protect them from harm during acute psychiatric episodes.
-
Ensure that the quality of mental health care is maintained or improved.
-
Establish reasonable standards around approvable purchases.
-
Monitor participants' spending and maintain programs' total costs (i.e., variable plus fixed costs) at acceptable levels.
4.1. Ensuring that Participation is Equitable
SDC models automatically place consumers of mental health services "in the driver's seat"2 by making them the primary decision-makers in choosing services and providers and by giving them authority over an individual budget. Although this structure supports consumers' autonomy and self-direction, it also demands greater consumer involvement in treatment decisions and care planning. Some consumers and family members could initially perceive this new role as undesirable or risky. As a result, offering education to consumers who may be interested in participating and providing various supports to participants once they start SDC may be essential to maximize participation in SDC programs.
In key informant interviews, consumer advocates and state policy officials consistently endorsed making SDC accessible to all groups of mental health consumers, regardless of health or social factors, such as their degree of functional impairment, age, or housing status. One key informant stated that the primary criterion for entry into SDC should be that a consumer voluntarily "opts in." However, some consumers of traditional mental health services may have concerns about entering a SDC program. Some consumers may be skeptical of programs that claim to honor their autonomy.34 Others may be concerned about losing access to their current providers and services or their disability income supports. Other may simply not want to accept a greater role in decision-making about their care.23 Family members may be concerned that participation in SDC will result in less consistent or worse quality mental health care. The degree of concern about participation is likely to vary widely across consumers and family members, depending on their past experiences with providers and their level of comfort with providers' decision-making.23
Supporting SDC participation among those persons who may be ambivalent about participating as a result of perceived risks is a critical task for the next generation of mental health SDC programs. Programs need to have a capacity to provide psycho-education about SDC. A trained SDC program representative or network representative (i.e., a SDC representative serving multiple programs in a geographic area) could serve in this capacity. Such a person would presumably make regular presentations at organizations in their communities, such as consumer advocacy organizations, family member organizations, and outpatient mental health programs. Programs could also develop and/or disseminate web-based and/or printed educational toolkits for mental health SDC. In presentations and in educational toolkits, testimonials from SDC participants could provide an effective tool for communicating the risks and benefits of participation. At present, few, if any, such tools exist, and consequently they would need to be developed with public or private funding.
Separations from SDC
Supports for continued participant engagement in mental health SDC also may be needed. Participant disengagement (i.e., separation) from SDC is a concern for two reasons. First, some participants who disengage from SDC may effectively stop self-directing their own care, and as a result they may stop receiving needed mental health services. If such consumers are not self-directing their own care, some alternative arrangement for delivering services must be put into effect. Second, some ex-participants may not return to their SDC programs unless the programs actively re-engagewith them and invite them to return. For example, they may subjectively associate a sense of failure with their previous SDC effort, may not feel welcome to return, or may not know how to re-engage with the program. As a result, programs may need a capacity for re-contacting persons who become separated from SDC and a protocol for either re-engaging former participants in the program or re-directing them to another program or provider.
Hiatuses of Participation in SDC
In key informant interviews, consumer advocates pointed out that even after a consumer has started participating in a SDC program, a worsening of the consumer's health status may necessitate a hiatus of participation in SDC, although a return to SDC could occur after the consumer is sufficiently recovered. The SDC approach may not work well during an acute episode of psychiatric illness, when a participant's ability to make decisions that are consistent with his or her own interests may be impaired. Hospitalizations would also limit a participant's autonomy and ability to make decisions about their own care.
There is not yet any consensus among SDC program officials or consumer advocates regarding how hiatuses of participation in mental health SDC, due for example to a period of acute illness, would be handled. Programs would need to address various logistical questions. For example, how would SDC program staff know whether a participant's mental health status and decisional functioning had declined to such a level that a participation hiatus should be considered?
Programs could, for example, stipulate that participants must regularly check in with their coach, either by telephone or in person, and report on their mental health status. An unexpected lapse in scheduled check-ins could then serve as a prompt for program staff to investigate whether a client's status had changed. Newer reporting technologies designed for persons with SMI, such as video-based assessment, automated telephone questionnaires, interactive smart-phone reporting applications, or Internet-based reporting tools, could also be brought to bear in obtaining regular status reports from participants. However, a policy of requiring a check-in would seem to be somewhat contrary to the principle of self-direction. Also, it is unclear whether or how a reporting requirement would be enforced. Would programs be required to suspend participation for participants who do not regularly check in?
Another logistical question concerns the temporary transfer of decision-making authority from a participant to a care entity when the participant is unable to self-direct care. The care entity could be the participant's designated mental health care provider or provider organization, such as a psychiatrist or mental health clinic. It is unclear how such transfers will occur and what safeguards will be put in place to ensure they go as planned and occur in a timely manner with minimal lag between the consumer's real-time decline in ability to self-direct care, notification of or recognition by the provider, and an administrative shift from SDC status to additional oversight. A process for following up with the provider/provider organization to re-assess the participant's status and determine whether the participant is ready to re-start participation in SDC would also be needed. An administrative tracking database for tracking changes in participants' mental status and a corresponding administrative process that ensures database updating will be needed to support temporary transfers of decision-making and hiatuses of participation in SDC.
One federal official noted that SDC participants could use the SDC goals planning process to state in the form of a psychiatric advance directive their preferences for mental health service delivery and decision-making during episodes of acute illness. Results from research studies suggest that persons with psychiatric advance directives receive fewer coercive crisis interventions including inpatient hospitalization.35, 36 Studies also indicate that only a small minority (4-13 percent) of persons with psychiatric illnesses currently have an advance directive;37 consequently, their use could be increased. However, it is also known that providers are usually not legally bound by psychiatric advance directives and inconsistently adhere to instructions specified in directives.37, 38
Stefan34 suggests that SDC participants should prepare advance directives, designate health care proxies, and execute durable powers of attorney to "ensure that there is never a vacuum of decision-making and control which forces the involvement of the legal system, the mental health system, or persons who are strangers to the client's situation and values." SDC programs could encourage participants to fill out advance directives and review them periodically. In addition, recovery plans should include a crisis plan that addresses other issues besides health care, such as housing, employment, and child care. Crisis plans could also include a list of current providers, so that the primary mental health care provider can be easily identified and contacted according to the participant's preferences.
Other protections besides advance directives may be needed in order to maintain self-direction during periods of acute symptom exacerbation. One option could be to require case managers at all SDC programs. The case manager would be trained in the SDC approach and would be responsible for helping participants navigate transitions into and out of SDC. Smaller SDC programs could share a case manager with other programs in their region, while larger SDC programs could have their own case manager. Payment rates for the case manager position could be built into a state's Medicaid plan.
4.2. Supporting Self-Direction in SDC
SDC programs should be prepared to help participants compensate for cognitive and functional impairments that may impede them from self-directing their own care and engaging in a recovery process. In persons with mental health disabilities, cognitive impairments and other clinical problems can impede decision-making and the ability to complete daily tasks that are required for independent living, being employed, and participating in school and other social activities.29, 30, 31, 39, 40 In addition, results from at least two clinical studies suggest that persons who have more severe mental health symptoms and functional disabilities may have greater difficulty participating in recovery oriented services.41, 42 As a result, some consumers may be able to fully engage in SDC only if they obtain decision-making supports, skills training, or other assistive services that are designed for persons with severe mental health disabilities. Obtaining these supports may be challenging for mental health SDC programs.
Supporting Activities of Daily Living
One key informant observed that some consumers transitioning from traditional services into SDC may initially not have the skills needed to fully utilize the tools offered by SDC. Persons with mental health disabilities have varying abilities to independently manage common activities of daily life, such as shopping for groceries and clothes, preparing meals, attending to personal hygiene, doing laundry, driving a car or using public transportation, managing medications, and keeping track of income and bills. Being able to complete "instrumental activities of daily living" (IADLs) is a lynchpin to recovery from mental illness,43 and clearly would facilitate participation in SDC programs. SDC programs must consequently be prepared to help participants gain access to providers of needed IADLs or to programs that provide skills training in completing IADLs.
One of the threats to the success of mental health SDC is that IADL providers who serve persons with SMI may be unavailable in many areas of the United States. A mental health workforce that provides IADLs has not been developed, probably because Medicaid and Medicare generally do not allow reimbursement for mental health IADL services. Although some mental health programs (e.g., Assertive Community Treatment programs) do provide IADLs, such programs generally have a paternalistic overtone that may conflict with SDC, are expensive, and are not available on a sufficient scale to be useful for SDC participants. Programs that provide IADL skills training are similarly rare, though there are some examples of experimental programs.44 Thus, in mental health systems, there is no parallel to the workforce of home health care workers for persons with physical disabilities. Such a mental health IADL workforce might develop if SDC programs create a viable opportunity for these types of providers to enter the marketplace and provide services.
Supporting Decision-Making
SDC participants and coaches may benefit from education and guidance in relation to the process of shared decision-making. Shared decision-making refers to a process of health care delivery in which providers and clients collaborate to access relevant information and to enable client-centered selection of health care resources.23 Shared decision-making is a method of eliciting consumer treatment preferences, providing education about treatment options and related outcomes, allowing consumers to deliberate about the possible attributes and consequences of these options, and then supporting consumers' informed treatment choices. Shared decision-making has the potential to improve uptake of effective treatment options and participant satisfaction in SDC programs, by helping ensure that treatment decisions reflect participants' preferences, are arrived at systematically, and are informed by scientific evidence.
In addition to general shared decision-making, targeted decision-making supports or training opportunities that are developed specifically for persons with SMI could be offered in SDC. For example, SDC programs could provide decision supports around identifying and addressing unmet service delivery needs. One example would be identifying the need for HIV and hepatitis prevention services. SDC programs could support risk assessment and could link participants with providers that offer convenient and free blood testing and hepatitis immunization.
Technologies that allow for self-monitoring and self-report could also be used to support decision-making by routinely querying consumers about their preferences for services, their attendance at services, and the impact of those services.45 The Patient Assessment System (PAS), tested in several trials with individuals with SMI and shown to be feasible, reliable and to improve care quality, was designed with these purposes in mind.46, 47, 48 At PAS kiosks, questions regarding service needs and utilization appear on a touch screen monitor one at a time and are also read aloud by a recorded voice. PAS responses are summarized on a report that prints for the consumer and can be used to track goals, needs, service usage, and impact. The PAS can also print text to help the consumer advocate for needed services.
4.3. Protecting Participants from Coercion and Victimization
A key purpose of the SDC approach is to increase consumers' control of decisions relating to their care, and thereby increase their independence and free them from coercion in mental health treatment. Although consumers' degree of involvement in decisions about their own treatment varies,23 many consumers experience mental health care as a coercive process, one which regularly forces them to adhere to interventions they may not believe are beneficial or do not want.22 Mental health providers, family members, police, and judges can also apply leverage to compel receipt of mental health treatment, and consumers' awareness of this leverage colors their perceptions of care.49 SDC programs give participants the authority to separate themselves from services that they do not find beneficial and to find new providers when they so choose, and this ability would be expected to result in less perceived coercion.
Even with SDC, persons with mental health disabilities may remain vulnerable to coercion. One concern is SDC participants' choices regarding services and providers may be used by persons outside the program as a basis for coercion or competency challenges.34 Another concern is that persons who are more severely ill, who have not previously been offered the opportunity to direct their own care, or who have a conservator or representative payee will be vulnerable to pressure from providers, SDC coaches, or their representatives. Such concerns create a nexus of legal, ethical, and logistical issues, which may be resolved differently in different programs. However, in designing rules and procedures for their programs, program officials may need to balance the goal of protecting participants against coercion with other important program goals, such as maintaining program integrity and sustainability and ensuring participants' safety.
In relation to maintaining program integrity and sustainability, some participants may need guidance to ensure that their spending priorities (i.e., the amounts of money being allocated to different categories of spending) purposefully reflect their health care needs. For example, persons who expect to have out-of-pocket expenses related to a frequent need for outpatient therapy should consider these expenses when planning their individual budgets. Although this guidance could come from a SDC coach, participants with more severe limitations in cognitive functioning have the assistance of a legally authorized representative, such as a conservator or representative payee. SDC programs should consequently be prepared to provide such representatives education about the SDC approach and to communicate their program's expectations around participant self-direction.
Problems with coercion could also arise if fiscal intermediaries are not made accountable to the SDC program that they serve. For example, in Washington County, Maryland, the local mental health care services agency, which is an administrative branch of the state public mental health system, serves as the fiscal intermediary of the SDC program. Although this arrangement is thought to work well in Washington County, it could raise concern because the Washington County SDC program is accountable to the core services agency. This arrangement could result in a sense of coercion, because the SDC program may fear that its funding could be jeopardized if participants make too many requests for purchases.
Protecting SDC participants from victimization by providers of services and other vendors should also be considered in the design of SDC programs. Certain behaviors, health problems, and other personal characteristics that are associated with having a SMI may increase participants' risk of being victimized. These would include illicit drug use and heavy alcohol use, impaired decision-making, low educational attainment, low self-efficacy, and poverty. SDC programs must be vigilant for and be prepared to respond to situations involving participant victimization, such as acts of financial fraud or theft, and also must monitor for unethical or unfair treatment by providers. Some SDC programs apply a vetting process to service providers, to check professional licensing and to run criminal background checks. This may help reduce outright fraud. However, SDC programs could also have procedures for administratively tracking and investigating cases of participant victimization and for designing response plans that reduce the likelihood of re-occurrences.
4.4. Ensuring Continued Receipt of Needed Care
One potential concern regarding SDC participants' greater independence in making decisions about their own care and in planning mental health spending is that some participants may choose not to receive mental health services, may dramatically reduce their spending on outpatient specialty mental health care services, or may not reserve enough money in their budget for outpatient mental health services that they later need. Although reduced spending on outpatient mental health care may reflect a consumer's preferences, it could also result from misperceptions of one's own need for care. Although very little evidence is available to evaluate these concerns, such concerns may be shared by mental health providers, state authorities, and family members.
According to one of the key informants for this report, it may be necessary to stipulate some minimum level of expenditure on outpatient mental health service use to reassure providers, state authorities, and family members. Such a stipulation exists in the Texas SDC program, wherein 60 percent of an individual's budget must be spent on traditional mental health services. Other programs (e.g., SDC in Washington County, Maryland) instead stipulate that continued participation in outpatient mental health treatment is a condition of enrollment in the SDC program, offer suggested formulas for spending a certain proportion of a participant's budget on traditional mental health services, or do not impose any rules around mental health service use.
One key informant consulted for this report stated that the issue of people entering SDC and not using mental health services is "a 'red herring,' because it seldom happens." The same key informant pointed out that current public mental health system participants have the option of using no mental health care, and was not convinced that a rationale exists for having greater limitations placed on participants in SDC.
However, one possible rationale for such limitations is that SDC may alter the social contract that underpins public mental health financing. When mental health care consumers in traditional public mental health systems do not utilize mental health care, they do not alter how public mental health financing is ultimately spent; all of the monies are spent on mental health care (for other consumers). In contrast, to the extent that SDC re-allocates public mental health care financing toward non-mental health goods and services (e.g., housing, transportation, or education), public monies spent on mental health care are reduced. This re-purposing of some public mental health financing suggests a reasonable rationale exists for establishing programmatic expectations around mental health service use by persons receiving public mental health financing for SDC.
Whether or not programs impose rules around mental health service use, ongoing participation in some form of outpatient mental health treatment would seem to be an essential protection both for SDC participants and their programs. For participants, maintaining regular contact with a provider is necessary for the purpose of monitoring psychiatric symptoms and the side-effects of medications and for updating the treatment plan as service needs change. In addition, the public integrity and sustainability of SDC programs may be threatened if SDC participants do not continue in outpatient mental health treatment; the legitimacy of the individualized budget may be challenged if SDC participants do not allocate any part of their budget to traditional mental health care.
Another potential risk to consumers in SDC programs concerns a sudden and unanticipated increase in need for outpatient mental health services, which could coincide, for example, with the onset of psychosis. Chronic mental illness is characterized by fluctuating symptoms and intermittent periods of acute crisis. A consumer's service needs could increase during the middle of a plan year and, at the time of increased service need, a consumer might not have sufficient funds left over in their individual budget to pay for needed outpatient services and medications. As a result, there is a potential risk that a consumer's access to needed outpatient mental health care would be adversely affected.
In many traditional public mental health programs and in most mental health SDC pilot programs, risks associated with fluctuating need for services are pooled among all consumers in the program. While one consumer in the program may have an unanticipated increase in service need, another consumer may have an unanticipated decrease in service need. As a result, over the entire risk pool, individual variations in service need may be balanced out and the risks to individuals are minimized. Pooling a greater number of individuals tends to provide greater protection against financial risks, providing that systematic "adverse selection" of risks into the pool is not an important factor.
The existence of relatively small and independently financed SDC programs raises the concern that any one program may not have a large enough risk pool to offset financial losses for some consumers with financial savings from others. Consequently, some form of pooling of financial risks across mental health SDC programs is desirable. One way this could be accomplished would be to roll mental health SDC programs under a single umbrella program that would be managed by a state's lead mental health agency or by a managed behavioral health care organization on behalf of a state. In that case, the state or the managed care organization would assume financial risk associated with over spending. A state could also stipulate other types of financial requirements for SDC programs. A state could, for example, require that SDC programs purchase insurance against participant over spending. The premiums collected would in essence be used to finance a large risk pool. Alternatively, a state could require that each SDC program maintain a reserve fund to cover unanticipated excess spending during the plan year.
4.5. Ensuring that the Quality of Care is Maintained or Improved
One of the rationales for the SDC approach is that giving participants the freedom to make choices, whether good or bad, encourages personal responsibility and independence. As a result, some participants in SDC may use individual budgets to select treatment interventions that psychiatrists and psychologists would consider misguided or potentially harmful. Others may spend their individual budgets in ways that they later regret. Although such outcomes are a predictable and perhaps necessary consequence of self-direction, SDC programs should seek to minimize them by offering education and decision-making supports.
Ensuring that SDC participants obtain care that is no worse in quality than the care they would have received in traditional mental health programs and instituting standards that encourage quality improvement are critical to the long-term sustainability of mental health SDC. Quality and accountability have become guiding principles of efforts to improve mental health services and the health outcomes of individuals with SMI,21, 50 just as autonomy and choice are guiding principles in the design of SDC. One concern is that many participants will purchase ineffective or unneeded products and services or will be exploited by product and service vendors. Another concern is that SDC will undermine the successful dissemination of evidence-based practices (EBPs), mental health services and clinical practices whose clinical benefits have been demonstrated in rigorously designed research studies or demonstration trials (e.g., Supported Employment). If mental health SDC programs do not establish clear standards that address these concerns, their legitimacy may be challenged and sustained financing for SDC may be put at risk.
Efforts to ensure adequate quality and accountability have often involved creating standards and payment policies that serve to reduce natural variations in service delivery and practice. In managed care health plans and Medicaid fee-for-service plans, the concern that consumers will purchase ineffective or unneeded products and services is addressed by limiting health plan reimbursement to those providers, products, and services that satisfy regulatory standards or that have been vetted for quality. Training providers to provide EBPs51, 52 and instituting payment policies, such as accountable care organizations,53 that financially reward adherence to quality indicators are leading examples of strategies states have used to achieve greater quality and accountability in health care.3
In SDC, the pursuit of autonomy and choice could conflict with the pursuit of quality and accountability. SDC participants may or may not elect to use interventions and services that are supported by evidence and may select services that raise concerns among participants' health care providers or family members. The issue of quality may be addressed through a shared decision-making process and/or by providing decision-making supports, as discussed above (Section 4.2). SDC coaches, who assist SDC participants in developing their individual service plans, can be trained to provide information and guidance about providers and services and to support shared decision-making. Such training could include education on EBPs and information about the locations where EBPs are offered within a service region. Over time, SDC coaches may also compile a more global assessment of the quality of providers in their service region based on the feedback they receive from mental health consumers, and consequently SDC coaches may be able to provide qualitative assessments of provider quality to SDC participants.
The concern that SDC programs could undermine the dissemination of EBPs raises several unresolved issues. One likely benefit of implementing SDC on a larger scale is that participants' service choices may yield new information about their preferences for various EBPs. Some EBPs may be preferred to similar non-EBP services, and in those cases SDC would likely accelerate EBP use and implementation. An evidence base is being developed for several innovative interventions that are recovery oriented, including stigma-reduction interventions,54 wellness recovery interventions,55 and peer-led illness self-management programs.56 Innovative recovery oriented interventions could be especially attractive to participants in SDC.
Some SDC participants may report a mismatch between available EBPs and the types of services they would like to have available. Such information could result in modifications of existing EBPs or the development of new EBPs. The least attractive outcome would be if policymakers and providers favored the dissemination of an EBP that SDC participants did not want to use. In such cases, implementing a shared decision-making process to enable assessment of the costs and benefits of the EBP would be critical.
One key informant to this report emphasized that it is essential for either the state or the managed care company or fiscal intermediary serving as the state's agent to ensure that information is available and that choices are made among a set of products, services, and providers that have been vetted for quality. According to this informant, allowing people to make choices from a selected menu of providers and services is a reasonable method to control quality. Whether or not programs limit choices among providers or services, programs should be able to communicate in an understandable way their policies regarding allowable services and products to participants, some of whom may have low literacy.
4.6. Managing Purchases
Procedures and policies that SDC programs adopt in relation to participants' purchases may be interpreted as manifestations of programs' commitment, or lack thereof, to the principles of client self-direction and autonomy. Purchasing policies and procedures should consequently be transparent and ideally will reflect substantial input from SDC participants and other community stakeholder groups. However, purchasing procedures and policies may also be interpreted as manifestations of SDC programs' stewardship of public financing for mental health care. Viewed from this perspective, purchasing policies and procedures should reflect input from varied constituencies.
Nearly all of the key informants interviewed for this report agreed that SDC participants should be allowed to purchase essentially any legally obtainable good or service that is consistent with one or more goals of their recovery plan. A former federal program official offered the following principle as guidance: programs should allow any purchases "related to living a full life in the community." However, at least one key informant pointed out that the legitimacy of some items could be questioned by the public even if the item is linked to a valid recovery goal, suggesting the need for some boundaries on purchases of non-traditional items.
According to key informants who have worked in or with SDC programs, proposed purchases rarely have tested the boundaries of legitimacy and denials of proposed purchases have been uncommon. One SDC program administrator said that the most frequently disallowed items are requests to receive outpatient mental health services from a provider whose hourly rate is not affordable within the constraints of the participant's available budget. Insufficient linkage between a proposed purchase and a recovery goal in a participant's recovery plan was the only other reason cited for purchase denials.
Standardization of approvable items and vendors, within a region or state, would seem to be in the interest of all SDC participants. Public controversy regarding the legitimacy of selected purchases in SDC could threaten the perceived legitimacy of the overall SDC program and continued program financing. External authorization of program policies regarding allowable purchases (e.g., as established in state regulations) and a process for auditing approved and actual purchases may encourage such standardization. SDC program coaches also will require training with respect to a program's purchasing policies.
SDC programs could also utilize modern payment technologies to minimize labor expenses associated with managing participants' budgets. For example, SDC participants in Texas SDC are given "cash cards" that have a pre-assigned spending limit and that allow purchases from a pre-specified set of vendors. Such a system would relieve the need for human review and approval of each purchase and would facilitate the monitoring of participants' budgets during a plan year.
In Cash and Counseling programs, fiscal intermediaries provide the Medicaid program with financial accountability and protection against misuse of budgets by participants and their representatives. Yet nearly all Cash and Counseling grantees report having experienced difficulties with fiscal intermediaries.57 Hence, state officials agree that it is critical to develop strong oversight capability to detect and resolve any difficulties in a timely fashion.
4.7. Protecting Public Budgets
According to key informants consulted for this report, most states and the Federal Government will only consider implementing SDC if it will not result in increased budgetary costs for mental health care. One key informant from the managed behavioral health care industry expressed a view that may be applicable to many mental health SDC programs: the costs of mental health care in SDC can normally be maintained at similar or lower levels as traditional managed behavioral health care systems, so long as appropriate administrative checks against excess spending are in place. Even so, the public budget implications of SDC should be a paramount consideration in the design of SDC programs.
Moral Hazard and its Consequences
Mental health SDC program participants are exempted from many of the usual regulatory and managed care controls over spending on mental health care. This raises concern that some SDC participants may over spend their budgets, thereby creating a financial risk to the program. If participants believe that they are not financially liable for over spending their allotted budgets, they may be even more likely to over spend in the first place. Such an incentive for health care consumers to over spend when they are not financially liable for the costs of additional spending is known as "moral hazard."
It is unclear who would be responsible for any financial losses due to over spending in SDC programs, should they occur. SDC programs may not have financial reserves or other financing available to cover such losses. Participants are unlikely themselves to bear financial risks from over spending. Medicaid is unlikely to cover such losses, either. As a result, the state government sponsoring the SDC program may turn out to be the payer of last resort for such losses. This suggests that the possibility of financial losses should be anticipated and planned for in any statewide implementation of SDC. Such contingency planning could result in additional financial oversight, a requirement for a reserve fund to cover losses, a requirement that programs purchase financial loss insurance, or other contingency plans.
Although participants may be unlikely to themselves bear financial risks from over spending, participants' autonomy may suffer as a result of over spending. If participants spend their budgets too rapidly during the plan year, their program will be forced to ensure that sufficient resources are kept in reserve to pay for expenses during the remainder of the year. Programs would have to decide whether to permit continued spending on items being purchased from individual budgets, and could deny some purchases. Not allowing continued spending could be highly disruptive to a participant's recovery and, worse still, program administrators might feel compelled to direct the participant's future spending, thereby undermining the principle of self-direction. On the other hand, letting a participant continue spending beyond the allotted budget may set an undesirable precedent that could result in financial jeopardy to the program.
Evaluations of Program Costs and Spending
Research studies comparing the costs of mental health SDC to the costs of traditional mental health care are scarce. Although there are a few reports of costs and expenditures in SDC, no studies have been conducted with sufficient methodological rigor to ensure reliable conclusions in relation to costs. Some key informants consulted for this report speculated that participation in SDC might result in lower spending on institutional care, whereas others speculated that consumers' health care expenses might increase when they begin self-directing their own care and have the freedom to choose services and providers they prefer. However, research studies to date provide little or no reliable evidence in relation to these issues.
In relation to the narrower concern that some SDC participants will out spend their allowed budgets, none of the first generation of mental health SDC programs is reported to have had problems due to systematic over spending by participants. In SDC programs in Florida and Maryland, participants have not fully spent their individual budgets, on average, at least in some years,58 though it is not clear why they have not. Other programs' experience has been that participants fully spend their budgets. However, given that participants have few individual disincentives to spending, the systemic risks of over spending are likely to increase with the overall scale of SDC participation and with greater participant experience.
Even if rigorous comparative cost evaluations of mental health SDC programs were available, the results of such analyses would not necessarily be generalizable to larger-scale implementations of SDC. How mental health SDC programs get implemented on a larger scale could dramatically affect their costs. Costs could vary especially depending on the specifications of staff training requirements and the administrative reporting requirements stipulated by states and by Medicaid. For example, programs that use peer-specialist providers may have additional supervision costs that programs using professional care managers do not have. One managed care executive also pointed out that implementation of SDC on a larger scale will require upfront investment to cover expenses for program staff, management information systems, and other overhead expenses while caseloads are accruing. Once a target caseload size is achieved, SDC programs would be expected to be self-sufficient. However, bridge funding may be needed during the start-up phase.
Managing Financial Risks
Key informants to this report generally agreed that programs can apply various administrative procedures to manage participants' expenditures, though the effectiveness of these methods has not been demonstrated. One approach to managing participants' expenditures is to complete ongoing, regular (e.g., quarterly) administrative reviews of their spending patterns. If the pace of the participant's spending suggests the budget will run out before the end of the plan year, some purchases could be denied to bring participants' spending back into alignment with their budget. Although the notion of managing participants' utilization through a process of administrative review is conceptually at odds with the principle of self-direction, economic incentives created by SDC may make utilization review or some equivalent process unavoidable if SDC programs are implemented on a larger scale.
In most existing mental health SDC programs, participants' budgets and spending patterns indeed are reviewed by an administrator at regular intervals, and any adjustments in spending are made on an individual basis. However, if SDC programs are implemented on a larger scale, such labor-intensive manual reviews of spending could become prohibitively expensive. Consequently, automation of budgetary review functions, using information systems supports and decision rules, is desirable. Programs could, for example, use an accounting system that maintains frequently updated information on claims, payments, and projected future spending to create regular reports on individual participant's spending and on spending at the program level.
SDC programs could contract with fiscal intermediaries or managed care organization to provide capacities for administrative reviews of spending, as many of these organizations have management information systems, technical expertise, and administrative infrastructure needed to manage costs, and few states have these capacities. In fact, managed behavioral care organizations have already been partners in several mental health SDC programs. However, partnering with managed care organizations may require considerable advance and ongoing planning by SDC programs and their managed care partners, especially in relation to communicating to managedcare staff the purposes and principles of the SDC approach. SDC program administrators also may require training in accessing managed care organizations' information systems, to enter information and obtain reports. It seems likely that the costs of this training would be the responsibility of the state government, although perhaps other funding sources, such as Data Infrastructure Grants (from SAMHSA) could be used to cover these expenses.
Another method that has been used to prevent cost increases following consumers' entry into SDC is indexing new participants' budgets to their level of spending on outpatient mental health care prior to entering SDC. Consumers with higher mental health expenditures prior to starting SDC receive higher budgetary allocations than consumers with lower expenditures prior to starting SDC. Indexing an individual's budget to prior spending may help ensure that the individual's spending in SDC will not exceed their spending in prior years. It is unclear whether this type of "risk adjustment" would generally work well in mental health SDC programs. Indexing implies, for example, that consumers who were inconsistently engaged in outpatient treatment prior to SDC get relatively smaller SDC budgets and consequently have less money available to them compared to consumers who were consistently engaged in outpatient treatment. Such an allocation formula may result in a gap between an individual's budget and the costs of their care for an individual whose needs increase substantially from one plan year to the next. Programs using indexing would consequently need some fiscal flexibility, perhaps a reserve fund, to be able to adjust during a plan year to unexpected changes in individuals' service needs.
4.3. Protecting Participants from Coercion and Victimization
A key purpose of the SDC approach is to increase consumers' control of decisions relating to their care, and thereby increase their independence and free them from coercion in mental health treatment. Although consumers' degree of involvement in decisions about their own treatment varies,23 many consumers experience mental health care as a coercive process, one which regularly forces them to adhere to interventions they may not believe are beneficial or do not want.22 Mental health providers, family members, police, and judges can also apply leverage to compel receipt of mental health treatment, and consumers' awareness of this leverage colors their perceptions of care.49 SDC programs give participants the authority to separate themselves from services that they do not find beneficial and to find new providers when they so choose, and this ability would be expected to result in less perceived coercion.
Even with SDC, persons with mental health disabilities may remain vulnerable to coercion. One concern is SDC participants' choices regarding services and providers may be used by persons outside the program as a basis for coercion or competency challenges.34 Another concern is that persons who are more severely ill, who have not previously been offered the opportunity to direct their own care, or who have a conservator or representative payee will be vulnerable to pressure from providers, SDC coaches, or their representatives. Such concerns create a nexus of legal, ethical, and logistical issues, which may be resolved differently in different programs. However, in designing rules and procedures for their programs, program officials may need to balance the goal of protecting participants against coercion with other important program goals, such as maintaining program integrity and sustainability and ensuring participants' safety.
In relation to maintaining program integrity and sustainability, some participants may need guidance to ensure that their spending priorities (i.e., the amounts of money being allocated to different categories of spending) purposefully reflect their health care needs. For example, persons who expect to have out-of-pocket expenses related to a frequent need for outpatient therapy should consider these expenses when planning their individual budgets. Although this guidance could come from a SDC coach, participants with more severe limitations in cognitive functioning have the assistance of a legally authorized representative, such as a conservator or representative payee. SDC programs should consequently be prepared to provide such representatives education about the SDC approach and to communicate their program's expectations around participant self-direction.
Problems with coercion could also arise if fiscal intermediaries are not made accountable to the SDC program that they serve. For example, in Washington County, Maryland, the local mental health care services agency, which is an administrative branch of the state public mental health system, serves as the fiscal intermediary of the SDC program. Although this arrangement is thought to work well in Washington County, it could raise concern because the Washington County SDC program is accountable to the core services agency. This arrangement could result in a sense of coercion, because the SDC program may fear that its funding could be jeopardized if participants make too many requests for purchases.
Protecting SDC participants from victimization by providers of services and other vendors should also be considered in the design of SDC programs. Certain behaviors, health problems, and other personal characteristics that are associated with having a SMI may increase participants' risk of being victimized. These would include illicit drug use and heavy alcohol use, impaired decision-making, low educational attainment, low self-efficacy, and poverty. SDC programs must be vigilant for and be prepared to respond to situations involving participant victimization, such as acts of financial fraud or theft, and also must monitor for unethical or unfair treatment by providers. Some SDC programs apply a vetting process to service providers, to check professional licensing and to run criminal background checks. This may help reduce outright fraud. However, SDC programs could also have procedures for administratively tracking and investigating cases of participant victimization and for designing response plans that reduce the likelihood of re-occurrences.
4.4. Ensuring Continued Receipt of Needed Care
One potential concern regarding SDC participants' greater independence in making decisions about their own care and in planning mental health spending is that some participants may choose not to receive mental health services, may dramatically reduce their spending on outpatient specialty mental health care services, or may not reserve enough money in their budget for outpatient mental health services that they later need. Although reduced spending on outpatient mental health care may reflect a consumer's preferences, it could also result from misperceptions of one's own need for care. Although very little evidence is available to evaluate these concerns, such concerns may be shared by mental health providers, state authorities, and family members.
According to one of the key informants for this report, it may be necessary to stipulate some minimum level of expenditure on outpatient mental health service use to reassure providers, state authorities, and family members. Such a stipulation exists in the Texas SDC program, wherein 60 percent of an individual's budget must be spent on traditional mental health services. Other programs (e.g., SDC in Washington County, Maryland) instead stipulate that continued participation in outpatient mental health treatment is a condition of enrollment in the SDC program, offer suggested formulas for spending a certain proportion of a participant's budget on traditional mental health services, or do not impose any rules around mental health service use.
One key informant consulted for this report stated that the issue of people entering SDC and not using mental health services is "a 'red herring,' because it seldom happens." The same key informant pointed out that current public mental health system participants have the option of using no mental health care, and was not convinced that a rationale exists for having greater limitations placed on participants in SDC.
However, one possible rationale for such limitations is that SDC may alter the social contract that underpins public mental health financing. When mental health care consumers in traditional public mental health systems do not utilize mental health care, they do not alter how public mental health financing is ultimately spent; all of the monies are spent on mental health care (for other consumers). In contrast, to the extent that SDC re-allocates public mental health care financing toward non-mental health goods and services (e.g., housing, transportation, or education), public monies spent on mental health care are reduced. This re-purposing of some public mental health financing suggests a reasonable rationale exists for establishing programmatic expectations around mental health service use by persons receiving public mental health financing for SDC.
Whether or not programs impose rules around mental health service use, ongoing participation in some form of outpatient mental health treatment would seem to be an essential protection both for SDC participants and their programs. For participants, maintaining regular contact with a provider is necessary for the purpose of monitoring psychiatric symptoms and the side-effects of medications and for updating the treatment plan as service needs change. In addition, the public integrity and sustainability of SDC programs may be threatened if SDC participants do not continue in outpatient mental health treatment; the legitimacy of the individualized budget may be challenged if SDC participants do not allocate any part of their budget to traditional mental health care.
Another potential risk to consumers in SDC programs concerns a sudden and unanticipated increase in need for outpatient mental health services, which could coincide, for example, with the onset of psychosis. Chronic mental illness is characterized by fluctuating symptoms and intermittent periods of acute crisis. A consumer's service needs could increase during the middle of a plan year and, at the time of increased service need, a consumer might not have sufficient funds left over in their individual budget to pay for needed outpatient services and medications. As a result, there is a potential risk that a consumer's access to needed outpatient mental health care would be adversely affected.
In many traditional public mental health programs and in most mental health SDC pilot programs, risks associated with fluctuating need for services are pooled among all consumers in the program. While one consumer in the program may have an unanticipated increase in service need, another consumer may have an unanticipated decrease in service need. As a result, over the entire risk pool, individual variations in service need may be balanced out and the risks to individuals are minimized. Pooling a greater number of individuals tends to provide greater protection against financial risks, providing that systematic "adverse selection" of risks into the pool is not an important factor.
The existence of relatively small and independently financed SDC programs raises the concern that any one program may not have a large enough risk pool to offset financial losses for some consumers with financial savings from others. Consequently, some form of pooling of financial risks across mental health SDC programs is desirable. One way this could be accomplished would be to roll mental health SDC programs under a single umbrella program that would be managed by a state's lead mental health agency or by a managed behavioral health care organization on behalf of a state. In that case, the state or the managed care organization would assume financial risk associated with over spending. A state could also stipulate other types of financial requirements for SDC programs. A state could, for example, require that SDC programs purchase insurance against participant over spending. The premiums collected would in essence be used to finance a large risk pool. Alternatively, a state could require that each SDC program maintain a reserve fund to cover unanticipated excess spending during the plan year.
4.5. Ensuring that the Quality of Care is Maintained or Improved
One of the rationales for the SDC approach is that giving participants the freedom to make choices, whether good or bad, encourages personal responsibility and independence. As a result, some participants in SDC may use individual budgets to select treatment interventions that psychiatrists and psychologists would consider misguided or potentially harmful. Others may spend their individual budgets in ways that they later regret. Although such outcomes are a predictable and perhaps necessary consequence of self-direction, SDC programs should seek to minimize them by offering education and decision-making supports.
Ensuring that SDC participants obtain care that is no worse in quality than the care they would have received in traditional mental health programs and instituting standards that encourage quality improvement are critical to the long-term sustainability of mental health SDC. Quality and accountability have become guiding principles of efforts to improve mental health services and the health outcomes of individuals with SMI,21, 50 just as autonomy and choice are guiding principles in the design of SDC. One concern is that many participants will purchase ineffective or unneeded products and services or will be exploited by product and service vendors. Another concern is that SDC will undermine the successful dissemination of evidence-based practices (EBPs), mental health services and clinical practices whose clinical benefits have been demonstrated in rigorously designed research studies or demonstration trials (e.g., Supported Employment). If mental health SDC programs do not establish clear standards that address these concerns, their legitimacy may be challenged and sustained financing for SDC may be put at risk.
Efforts to ensure adequate quality and accountability have often involved creating standards and payment policies that serve to reduce natural variations in service delivery and practice. In managed care health plans and Medicaid fee-for-service plans, the concern that consumers will purchase ineffective or unneeded products and services is addressed by limiting health plan reimbursement to those providers, products, and services that satisfy regulatory standards or that have been vetted for quality. Training providers to provide EBPs51, 52 and instituting payment policies, such as accountable care organizations,53 that financially reward adherence to quality indicators are leading examples of strategies states have used to achieve greater quality and accountability in health care.3
In SDC, the pursuit of autonomy and choice could conflict with the pursuit of quality and accountability. SDC participants may or may not elect to use interventions and services that are supported by evidence and may select services that raise concerns among participants' health care providers or family members. The issue of quality may be addressed through a shared decision-making process and/or by providing decision-making supports, as discussed above (Section 4.2). SDC coaches, who assist SDC participants in developing their individual service plans, can be trained to provide information and guidance about providers and services and to support shared decision-making. Such training could include education on EBPs and information about the locations where EBPs are offered within a service region. Over time, SDC coaches may also compile a more global assessment of the quality of providers in their service region based on the feedback they receive from mental health consumers, and consequently SDC coaches may be able to provide qualitative assessments of provider quality to SDC participants.
The concern that SDC programs could undermine the dissemination of EBPs raises several unresolved issues. One likely benefit of implementing SDC on a larger scale is that participants' service choices may yield new information about their preferences for various EBPs. Some EBPs may be preferred to similar non-EBP services, and in those cases SDC would likely accelerate EBP use and implementation. An evidence base is being developed for several innovative interventions that are recovery oriented, including stigma-reduction interventions,54 wellness recovery interventions,55 and peer-led illness self-management programs.56 Innovative recovery oriented interventions could be especially attractive to participants in SDC.
Some SDC participants may report a mismatch between available EBPs and the types of services they would like to have available. Such information could result in modifications of existing EBPs or the development of new EBPs. The least attractive outcome would be if policymakers and providers favored the dissemination of an EBP that SDC participants did not want to use. In such cases, implementing a shared decision-making process to enable assessment of the costs and benefits of the EBP would be critical.
One key informant to this report emphasized that it is essential for either the state or the managed care company or fiscal intermediary serving as the state's agent to ensure that information is available and that choices are made among a set of products, services, and providers that have been vetted for quality. According to this informant, allowing people to make choices from a selected menu of providers and services is a reasonable method to control quality. Whether or not programs limit choices among providers or services, programs should be able to communicate in an understandable way their policies regarding allowable services and products to participants, some of whom may have low literacy.
4.6. Managing Purchases
Procedures and policies that SDC programs adopt in relation to participants' purchases may be interpreted as manifestations of programs' commitment, or lack thereof, to the principles of client self-direction and autonomy. Purchasing policies and procedures should consequently be transparent and ideally will reflect substantial input from SDC participants and other community stakeholder groups. However, purchasing procedures and policies may also be interpreted as manifestations of SDC programs' stewardship of public financing for mental health care. Viewed from this perspective, purchasing policies and procedures should reflect input from varied constituencies.
Nearly all of the key informants interviewed for this report agreed that SDC participants should be allowed to purchase essentially any legally obtainable good or service that is consistent with one or more goals of their recovery plan. A former federal program official offered the following principle as guidance: programs should allow any purchases "related to living a full life in the community." However, at least one key informant pointed out that the legitimacy of some items could be questioned by the public even if the item is linked to a valid recovery goal, suggesting the need for some boundaries on purchases of non-traditional items.
According to key informants who have worked in or with SDC programs, proposed purchases rarely have tested the boundaries of legitimacy and denials of proposed purchases have been uncommon. One SDC program administrator said that the most frequently disallowed items are requests to receive outpatient mental health services from a provider whose hourly rate is not affordable within the constraints of the participant's available budget. Insufficient linkage between a proposed purchase and a recovery goal in a participant's recovery plan was the only other reason cited for purchase denials.
Standardization of approvable items and vendors, within a region or state, would seem to be in the interest of all SDC participants. Public controversy regarding the legitimacy of selected purchases in SDC could threaten the perceived legitimacy of the overall SDC program and continued program financing. External authorization of program policies regarding allowable purchases (e.g., as established in state regulations) and a process for auditing approved and actual purchases may encourage such standardization. SDC program coaches also will require training with respect to a program's purchasing policies.
SDC programs could also utilize modern payment technologies to minimize labor expenses associated with managing participants' budgets. For example, SDC participants in Texas SDC are given "cash cards" that have a pre-assigned spending limit and that allow purchases from a pre-specified set of vendors. Such a system would relieve the need for human review and approval of each purchase and would facilitate the monitoring of participants' budgets during a plan year.
In Cash and Counseling programs, fiscal intermediaries provide the Medicaid program with financial accountability and protection against misuse of budgets by participants and their representatives. Yet nearly all Cash and Counseling grantees report having experienced difficulties with fiscal intermediaries.57 Hence, state officials agree that it is critical to develop strong oversight capability to detect and resolve any difficulties in a timely fashion.
4.7. Protecting Public Budgets
According to key informants consulted for this report, most states and the Federal Government will only consider implementing SDC if it will not result in increased budgetary costs for mental health care. One key informant from the managed behavioral health care industry expressed a view that may be applicable to many mental health SDC programs: the costs of mental health care in SDC can normally be maintained at similar or lower levels as traditional managed behavioral health care systems, so long as appropriate administrative checks against excess spending are in place. Even so, the public budget implications of SDC should be a paramount consideration in the design of SDC programs.
Moral Hazard and its Consequences
Mental health SDC program participants are exempted from many of the usual regulatory and managed care controls over spending on mental health care. This raises concern that some SDC participants may over spend their budgets, thereby creating a financial risk to the program. If participants believe that they are not financially liable for over spending their allotted budgets, they may be even more likely to over spend in the first place. Such an incentive for health care consumers to over spend when they are not financially liable for the costs of additional spending is known as "moral hazard."
It is unclear who would be responsible for any financial losses due to over spending in SDC programs, should they occur. SDC programs may not have financial reserves or other financing available to cover such losses. Participants are unlikely themselves to bear financial risks from over spending. Medicaid is unlikely to cover such losses, either. As a result, the state government sponsoring the SDC program may turn out to be the payer of last resort for such losses. This suggests that the possibility of financial losses should be anticipated and planned for in any statewide implementation of SDC. Such contingency planning could result in additional financial oversight, a requirement for a reserve fund to cover losses, a requirement that programs purchase financial loss insurance, or other contingency plans.
Although participants may be unlikely to themselves bear financial risks from over spending, participants' autonomy may suffer as a result of over spending. If participants spend their budgets too rapidly during the plan year, their program will be forced to ensure that sufficient resources are kept in reserve to pay for expenses during the remainder of the year. Programs would have to decide whether to permit continued spending on items being purchased from individual budgets, and could deny some purchases. Not allowing continued spending could be highly disruptive to a participant's recovery and, worse still, program administrators might feel compelled to direct the participant's future spending, thereby undermining the principle of self-direction. On the other hand, letting a participant continue spending beyond the allotted budget may set an undesirable precedent that could result in financial jeopardy to the program.
Evaluations of Program Costs and Spending
Research studies comparing the costs of mental health SDC to the costs of traditional mental health care are scarce. Although there are a few reports of costs and expenditures in SDC, no studies have been conducted with sufficient methodological rigor to ensure reliable conclusions in relation to costs. Some key informants consulted for this report speculated that participation in SDC might result in lower spending on institutional care, whereas others speculated that consumers' health care expenses might increase when they begin self-directing their own care and have the freedom to choose services and providers they prefer. However, research studies to date provide little or no reliable evidence in relation to these issues.
In relation to the narrower concern that some SDC participants will out spend their allowed budgets, none of the first generation of mental health SDC programs is reported to have had problems due to systematic over spending by participants. In SDC programs in Florida and Maryland, participants have not fully spent their individual budgets, on average, at least in some years,58 though it is not clear why they have not. Other programs' experience has been that participants fully spend their budgets. However, given that participants have few individual disincentives to spending, the systemic risks of over spending are likely to increase with the overall scale of SDC participation and with greater participant experience.
Even if rigorous comparative cost evaluations of mental health SDC programs were available, the results of such analyses would not necessarily be generalizable to larger-scale implementations of SDC. How mental health SDC programs get implemented on a larger scale could dramatically affect their costs. Costs could vary especially depending on the specifications of staff training requirements and the administrative reporting requirements stipulated by states and by Medicaid. For example, programs that use peer-specialist providers may have additional supervision costs that programs using professional care managers do not have. One managed care executive also pointed out that implementation of SDC on a larger scale will require upfront investment to cover expenses for program staff, management information systems, and other overhead expenses while caseloads are accruing. Once a target caseload size is achieved, SDC programs would be expected to be self-sufficient. However, bridge funding may be needed during the start-up phase.
Managing Financial Risks
Key informants to this report generally agreed that programs can apply various administrative procedures to manage participants' expenditures, though the effectiveness of these methods has not been demonstrated. One approach to managing participants' expenditures is to complete ongoing, regular (e.g., quarterly) administrative reviews of their spending patterns. If the pace of the participant's spending suggests the budget will run out before the end of the plan year, some purchases could be denied to bring participants' spending back into alignment with their budget. Although the notion of managing participants' utilization through a process of administrative review is conceptually at odds with the principle of self-direction, economic incentives created by SDC may make utilization review or some equivalent process unavoidable if SDC programs are implemented on a larger scale.
In most existing mental health SDC programs, participants' budgets and spending patterns indeed are reviewed by an administrator at regular intervals, and any adjustments in spending are made on an individual basis. However, if SDC programs are implemented on a larger scale, such labor-intensive manual reviews of spending could become prohibitively expensive. Consequently, automation of budgetary review functions, using information systems supports and decision rules, is desirable. Programs could, for example, use an accounting system that maintains frequently updated information on claims, payments, and projected future spending to create regular reports on individual participant's spending and on spending at the program level.
SDC programs could contract with fiscal intermediaries or managed care organization to provide capacities for administrative reviews of spending, as many of these organizations have management information systems, technical expertise, and administrative infrastructure needed to manage costs, and few states have these capacities. In fact, managed behavioral care organizations have already been partners in several mental health SDC programs. However, partnering with managed care organizations may require considerable advance and ongoing planning by SDC programs and their managed care partners, especially in relation to communicating to managedcare staff the purposes and principles of the SDC approach. SDC program administrators also may require training in accessing managed care organizations' information systems, to enter information and obtain reports. It seems likely that the costs of this training would be the responsibility of the state government, although perhaps other funding sources, such as Data Infrastructure Grants (from SAMHSA) could be used to cover these expenses.
Another method that has been used to prevent cost increases following consumers' entry into SDC is indexing new participants' budgets to their level of spending on outpatient mental health care prior to entering SDC. Consumers with higher mental health expenditures prior to starting SDC receive higher budgetary allocations than consumers with lower expenditures prior to starting SDC. Indexing an individual's budget to prior spending may help ensure that the individual's spending in SDC will not exceed their spending in prior years. It is unclear whether this type of "risk adjustment" would generally work well in mental health SDC programs. Indexing implies, for example, that consumers who were inconsistently engaged in outpatient treatment prior to SDC get relatively smaller SDC budgets and consequently have less money available to them compared to consumers who were consistently engaged in outpatient treatment. Such an allocation formula may result in a gap between an individual's budget and the costs of their care for an individual whose needs increase substantially from one plan year to the next. Programs using indexing would consequently need some fiscal flexibility, perhaps a reserve fund, to be able to adjust during a plan year to unexpected changes in individuals' service needs.
5. Research on the Benefits and Costs of Mental Health Self-directed CARE
At the present time, few firm conclusions can be drawn about either the benefits or the costs of mental health SDC approaches. Research on SDC programs for persons with SMI is at an early stage of development. Only a few research and evaluation studies have been completed to date. All of these studies have substantial methodological limitations. However, the strongest evidence available relates to the effects of SDC on program process outcomes (e.g., whether or not service planning is person-centered) and in relation to participants' level of satisfaction with SDC programs. In independently conducted evaluations of SDC programs in Florida and Oregon, SDC participants reported a generally high level of satisfaction with SDC programs, generally agreed that SDC programs have a strong recovery orientation, and endorsed various process indicators of person-centered planning.67, 68 In contrast, currently available research lacks any reliable information regarding the effects of SDC on participants' outcomes in several domains considered critical by state and federal policymakers, such as functional and residential independence, participation in competitive employment, use of inpatient mental health care, and physical health and health-related quality of life. Information on these outcomes is either completely unavailable or has limited reliability. Reliable information regarding the effects of SDC participation on participants' mental health care utilization and the overall public costs of care is similarly scarce.
5.1. Participant Satisfaction and Program Person-Centeredness
Evidence on SDC participant satisfaction with their SDC programs and on participants' perceptions of whether their program offers self-direction and person-centered planning is generally encouraging. In a report from 2006, Sullivan68 reported the findings of an evaluation of the Oregon Empowerment Initiatives Brokerage (EIB), a peer-run program that helps participants transition to independent community housing. Experiences in the program for the first 27 participants were collected using a questionnaire at 3-month intervals following participants' initial entry into the program. Their responses at follow-up were compared to their responses at entry into the program. The questionnaire presented respondents with a series of subjective statements about the program (e.g., "staff treat me as an equal") and asked them to rate their level of agreement, using a categorical scale from 1 "Strongly Disagree" to 4 "Strongly Agree." Participants reported improvement from program entry to follow-up on nearly all indicators of person-centeredness, sense of empowerment and self-efficacy, and sense of positive support from staff.
In a 2008 report on Florida SDC,58 Cook and colleagues reported findings from an evaluation based on interviews with 13 participants and eight non-participants. The non-participantswere interested in enrolling in SDC but did not enroll in the program. Participants indicated "high levels of satisfaction" with the program and gave "more positive responses" than non-participants in relation to attaining their personal recovery goals. Independent of the study by Cook and colleagues, the Florida Office of Program Policy Analysis and Government Accountability (OPPAGA) conducted interviews in 2010 with 64 Florida SDC participants.67 The OPPAGA reported that the 64 participants "generally expressed satisfaction with the program and believed that it was helping them maintain their ability to live independently or move toward recovery."
5.2. Independence, Employment, Education, and Health
SDC participants would be expected to have greater functional and residential independence and greater participation in competitive employment and education compared to participants in traditional mental health services. SDC programs are designed to advance these recovery goals through the person-centered planning process. SDC would, for example, be expected to result in greater independent living skills, such as cooking meals and using public transportation, greater numbers of starts in new jobs, and greater numbers of courses taken in community colleges and other educational programs. In relation to health outcomes, participation in SDC would be expected to result in increases in the amount of time spent in physical exercise and in greater participation in weight loss programs, since these are common recovery goals chosen by participants. However, evaluations of such changes have been rare.
Cook and colleagues58 reported results from an analysis of (n=106) Florida SDC participants' days spent in the community (i.e., days not spent in institutions) in the 1-year period after they entered the Florida SDC program compared to 1-year period immediately prior entering the program. Participants spent 17 more days in the in the community during the first year of participation in the program compared to the year prior to participation (354 days in the first year of participation versus 337 days in the prior year).
In a report on the Iowa SDC program,69 Ellison and colleagues examined participants' residential status, employment status and earnings in the 12 months after entering the SDC program, using information self-reported by program participants. Compared to the period prior to entering the program, participants reported greater residential independence and slight improvements in employment participation and earnings.
Results from the pre-/post-studies by Cook and colleagues58 and Ellison and colleagues,69 summarized in the preceding paragraphs, are intriguing because they suggest that the SDC approach could have substantial benefits in relation to improved independence, quality of life, employment and housing stability and could result in lower health care costs. However, the relationships between SDC program participation and outcomes that were reported in these studies may not be causal. Comparisons of participants' outcomes after the start of program participation to measures taken prior to participation are vulnerable to biases resulting from association between program participation and unmeasured factors that are related to participants' outcomes after program entry. For example, Cook and colleagues could not rule out the possibility that Florida SDC participants' days spent in institutions would have decreased even if participants had not started the Florida SDC program. As a result, it is difficult to know whether SDC program participation has any direct effect on participants' days spent in institutions, housing stability, or employment participation.
SDC programs could also result in better physical health outcomes and greater health-related quality of life if goals for personal wellness, such as increased physical exercise, weight loss, or reduced smoking, are achieved. SDC might also result in better control of psychiatric symptoms and reduced use of inpatient mental health care, as SDC participants may adhere more consistently to treatment plans that they select and that reflect their individualized goals for recovery compared to traditional treatment services.
Greater standardization of data on SDC participants' outcomes in SDC would seem to greatly facilitate opportunities for SDC program evaluation and quality improvement. In an evaluation report on the Florida SDC program,67 the authors concluded that measures of functional independence, participation in employment/education, and health were not systematically collected by Florida SDC. Consequently, they could not assess program impacts on participants' outcomes in key domains of interest to policymakers. In a letter of response to the OPPAGA report,67 the Florida Department of Children and Families, the state agency that initially funded the Florida SDC program, indicated that no funding was available to create a data system for the collection of participant outcome data, although the agency was taking steps to improve data collection in the future. Systematic collection of data on SDC participants' outcomes is not standard practice in other states' programs, either.
5.3. Current/Ongoing Research
Two ongoing randomized trials of SDC programs in Texas and Pennsylvania may soon provide much more information about the effects of mental health SDC than is currently available. Both studies have a rigorous design and are expected to provide estimates of SDC participation effects in relation to mental health symptoms, health-related quality of life, general health status, overall mental health services utilization, mental health treatment adherence, budgetary costs, and other key outcomes. The first of these projects involves participants in Delaware County Self-Directed Care for Community Integration of Individuals with Psychiatric Disabilities. Researchers at Temple University are collaborating with Magellan Health Services, which serves as the program's fiscal intermediary, on a randomized controlled demonstration and evaluation. The evaluation will consist of 75 SDC participants and a 75-person comparison group.
A second randomized controlled trial is being conducted at Texas NorthSTAR, a mental health SDC program in Dallas County, Texas. The University of Illinois at Chicago's (UIC's) National Research and Training Center on Psychiatric Disability is the trial's lead evaluator. The primary issue addressed by the evaluation is whether the program improves participants' mental health and enhances their quality of life, while being cost-effective. Seventy-five persons with SMI who are receiving mental health care services in Dallas and surrounding counties and who consent to join the study are randomly assigned to either SDC (44 persons) or a "services-as-usual" condition (31 persons). Those in the services as usual condition continue to receive services through the area's NorthSTAR managed care network. Study outcomes include participant satisfaction, service use and costs, clinical indicators, and recovery outcomes such as employment, education, social integration, and quality of life.
5.4. Issues for Future Research
Research on SDC programs that serve persons with SMI is at an early stage. This report raises a number of program design and financing issues that have not been addressed in prior research studies and that may be critical when implementing SDC on a larger scale. Some of the issues requiring further exploration are the following:
-
How does entry into SDC affect new participants' spending on mental health care and other medical care and how does entry into SDC affect the quality of the mental health and medical care services they receive?
-
What can SDC participation and spending patterns tell us about SMI consumers' preferred interventions and services and providers?
-
How does participation in SDC affect participation in competitive employment and education, and how does it affect participants' ability to live independently?
-
How do consumers' mental and physical health outcomes in SDC compare to their outcomes in traditional mental health care?
-
How should the mental health SDC approach be adapted to facilitate integration of somatic and mental health services for persons with chronic mental and physical health conditions?
-
What functional and cognitive limitations of consumers with SMI are associated with the likelihood of participating in SDC and with engagement in a recovery planning process, and how can SDC programs help ensure equitable participation in SDC in relation to illness and disability severity?
-
What are the most effective and cost-effective approaches to training and supervising new SDC coaches and what specialized training is needed by peer-specialist providers?
-
Do SDC programs facilitate or impede participants' use of evidence-supported practices, and what decision-making supports or other program approaches may guide participants toward use of evidence-based care?
-
Does participation in SDC result in more active consumer participation in clinical decision-making, and how can SDC programs encourage shared decision-making processes?
-
What are the implications for public budgets and Medicaid costs of large-scale participation in SDC by persons with SMI, and how should budgetary risks be addressed in the design of programs?
-
What technologies can be brought to bear in helping SDC programs manage participants' needs for physical health care services and crisis services, and how should these technologies be implemented in SDC programs?
Current research evidence on SDC programs offers very little insight into the longer term benefits and risks of SDC programs, and provides essentially no guidance on the design of SDC programs. New data pertaining to some of the research questions listed above may be available within the next 2 years following the completion of two ongoing trials of SDC programs in Texas and Pennsylvania. These two research studies are likely to provide new information especially in relation to effects of SDC on mental health symptoms, quality of life, and utilization of mental health services.
Additional large-scale demonstrations will be needed to establish the feasibility of implementing SDC within multiple sites and making it available to any mental health care consumer, irrespective of their level of impairment. Such a large-scale evaluation would likely identify many implementation issues, including challenges associated with making SDC continuously accessible to people who have frequent episodes of acute need for psychiatric care. A larger scale demonstration could also be used to try out different program design features and assess their strengths.
Another issue that has received scant attention in research on SDC is the potential of SDC to help young adults navigate the path to independence in adulthood and reduce the need for long-term disability supports. Young persons with SMI who are entering adulthood and adapting to adult roles and responsibilities often do not have access to those supports that are needed to live independently. Rigidities in mental health payment systems would normally impede young adults from using their public mental health funding to, for example, purchase clothing for work, a means of transportation, and a place to live. Without these supports, many young adults who have a SMI may be left with few options for obtaining needed income and mental health care in adulthood except to enroll the Supplemental Security Income (SSI) program as an adult. Unfortunately, enrollment in SSI as an adult financially discourages participation in competitive employment and education. SDC programs consequently have the potential to offer young adults a wider range of supports and to couple these supports with coaching on how to successfully make the transition to adulthood.
A special population for whom the mental health SDC approach could be customized and tested is adults with SMI and chronic physical health conditions. The SDC approach could be particularly helpful in paying for programs that integrate mental health care with physical health care services. In many states' Medicaid programs, mental health care is "carved out" from general medical care for physical health conditions. This usually implies that financing for general medical care cannot be combined with financing for mental health care in order to provide integrated medical and mental health services. This separation often results in poor quality care and health outcomes, because emotional and behavioral problems can impede medical treatment and vice versa. SDC is more flexible in terms of payment, and it consequently offers the potential to pay for providers from both the general medical and mental health sectors of the health care system.
Future research on mental health SDC programs should also seek to examine whether SDC is a transformational approach in mental health care. In principle, SDC allows public financing for mental health care to flow to those providers and services that offer participants' the best opportunities for recovery from a mental illness and for improving the quality of their lives. If implemented on a large-scale, SDC would consequently be expected to shift public financing towards innovative services and providers. SDC would also encourage other providers within the same system to adopt similarly recovery oriented practices, or face the consequences of losing their customers. Finally, SDC would be expected to increase the bargaining power of participants in interactions with mental health care providers, and consequently should result in more shared decision-making. These hopeful, albeit entirely theoretical, propositions should be entertained in future examinations of the SDC approach.
6. Conclusions
Compared to traditional mental health care, the SDC approach has the potential to offer persons with SMI greater control over the selection of services and providers and greater freedom to choose those recovery supports that they believe will make the greatest difference in their lives. Although information relating to the effects of SDC is incomplete, participation in SDC could be expected to result in greater consumer satisfaction with services and providers, higher quality of life for consumers, and more consistent engagement in recovery planning by consumers. SDC programs, if implemented on a large-scale, might also be expected to shift payments towards those service providers who offer recovery oriented, person-centered services and might shift spending towards innovative services that integrate (i.e., bundle together) the various services needed by persons with SMI.
Implementation of SDC in programs serving persons with SMI will require further customization of the conventional SDC model to ensure equity in program access as well as program integrity and sustainability. In relation to equity, a key concern is that persons with SMI who have previously been discouraged from active participation in decisions about their own care will either not be viewed as a candidate for SDC or will view SDC as a risky proposition, and consequently will not take advantage of the opportunity offered by SDC. To counter these possibilities, SDC programs must offer outreach and education to potential participants and decision-making supports to participants. However, it must also be recognized that participation in SDC programs should be entirely voluntary, and that many consumers who are offered SDC may prefer to remain in a traditional mental health program rather than enter a SDC program.
In designing SDC programs, mental health system leaders must successfully balance participant autonomy with the need for public accountability. Public accountability will require programs to ensure that participants receive equal or better quality of mental health care in SDC compared to traditional mental health programs, participants' individual purchases meet a public standard of reasonableness for persons receiving public disability supports, participants are not victimized by venders of products and services, and participants remain safe during periods of acute psychiatric crisis. This balance could be achieved in a variety of ways, all of which will involve some form of administrative review of providers and purchases. Achieving this balance may also require use of personnel and technologies for regular monitoring of participants' health status and administrative procedures for obtaining needed supports during periods of crisis.
In relation to ensuring public accountability, one approach that should be explored is for a state agency or the managed care company or fiscal intermediary serving as the state's agent to design the boundaries of the marketplace accessed by SDC participants. The marketplace design would include an approval process for vetting service providers, a list of products and services that are approvable for purchase, and rules and procedures for administratively reviewing proposed purchases and for appealing administrative decisions. SDC participants would then have the authority to exercise choices within this virtual marketplace, and the marketplace could be amended as participants' needs or other circumstances change. If such an approach is pursued, mental health consumers or their advocates clearly should be partners in designing the marketplace and in reviewing its adherence to the SDC principles.
Any conclusions regarding the impacts of SDC on mental health care costs or other public costs for persons with SMI are pre-mature given that almost no reliable information on cost impacts is available. A large-scale, rigorously designed demonstration trial of SDC compared to traditional care would be expected to yield important new information about the impacts of mental health SDC on mental health care costs and other policy-relevant outcomes. However, even a large-scale demonstration would not be expected to yield firm conclusions about the impacts of SDC on public budgets, as these effects could vary dramatically depending on how SDC programs are implemented and managed.
The 2010 ACA removed key barriers to financing mental health SDC programs using Medicaid and created new mechanisms for state Medicaid plan options that must include person-centered planning and individual budgets. Under new rules created by the ACA, states can offer an expanded array of HCBS to persons with SMI (under a 1915(i) state plan amendment) irrespective of whether these persons meet "an institutional level of need." States also do not have to demonstrate budget-neutrality in order to obtain approval for the 1915(i) state plan amendment. Both of these changes substantially improve the chances that states will re-assess the feasibility of implementing SDC programs designed for persons with SMI. Whether or not states will utilize these options is uncertain. Two ongoing randomized trials of the SDC approach may soon provide critical new information about the risks and benefits of SDC, which may prove helpful in designing the next generation of mental health SDC programs.
Future Medicaid-based mental health SDC models could look quite dissimilar to prior pilot and demonstration mental health SDC programs. To make SDC a usual component of mental health care available to many thousands of Medicaid beneficiaries with mental health disabilities, previous mental health SDC models will likely have to be adapted to account for at least four constraints in Medicaid. First, future programs will have to be made consistent with Medicaid regulations covering allowable goods and services and participating providers, regulations which may limit the types of goods and services that can be financed. Second, rules around eligibility for SDC will have to be established, as Medicaid plans generally limit eligibility for specialized mental health programs to those persons who meet pre-specified administrative criteria for need. Third, SDC programs will have to be replicable and scalable (i.e., they will have to be designed for dissemination and enrollment growth) without jeopardizing the integrity of public mental health services. Fourth, SDC programs will have to be sustainable within prevailing Medicaid cost constraints. Adaptation to these constraints could result in a substantial evolution of previous mental health SDC program models.
Appendix
Mental health SDC programs for persons with SMI have been formed in at least eight states: Florida, Iowa, Maryland, Michigan, New Hampshire, Oregon, Pennsylvania, and Texas. Most of these programs were designed as innovative pilot programs or as experimental programs in randomized evaluations of the SDC approach. However, some programs have continued to operate beyond their initial demonstration phase. This Appendix provides a summary of these SDC programs.
Florida
Florida SDC is the earliest SDC program implemented specifically for mental health care consumers with SMI.b The Florida SDC program was established in January 2000 and is administered through the Florida Department of Children and Families.58 Florida SDC has two administratively separate program sites; one serves the Jacksonville area and another serves the Fort Myers area. The Jacksonville program (http://www.floridasdc4.com) began enrolling participants in 2002 and at any given time has 150-250 participants. The Fort Myers program (http://flsdc.org) began enrolling participants in 2005 and has approximately 90 participants. Both Florida SDC sites receive state general revenues and both utilize Medicaid, Medicare, Veterans Health Administration (VHA), and private insurance plans for coverage of mental health care services.33
Alakeson reported that in 2007 insured participants in the Jacksonville program received an annual budget of $1,672, with insurance picking up the remaining costs of care; uninsured participants received an annual budget of $3,192 and were required to spend 48 percent of this amount on clinical services.33 The program has five professional recovery coaches who are employed as independent contractors. Providers of clinical, dental and optical services must be registered in the SDC program's provider network in order to receive payment for services provided to participants. Although this arrangement implies that participants cannot see other (unapproved) providers of these services, approved providers can bill the fiscal intermediary directly for services provided.
In 2007, participants in the Fort Myers program received $1,924 if they were Medicaid or VHA eligible and $2,811 if they were Medicare eligible. Uninsured participants received $3,700 but and were required to spend 48 percent of this amount on clinical services.33 The Fort Myers program is run by a local chapter of the National Alliance on Mental Illness (NAMI). Recovery (or "life") coaches are trained peer-providersand are employed directly by NAMI. In contrast to the Jacksonville program, Fort Myers SDC participants may choose any qualified clinical, optical or dental care provider.
Iowa
Iowa implemented the SDC approach on a pilot basis within an Intensive Psychiatric Rehabilitation program.2 The SDC program operated between 2006 and 2008 and was developed in partnership with Magellan Health Services, the managed care organization that manages Iowa's Medicaid plan for behavioral health.69 Under its contract with the State of Iowa, Magellan is required to set aside 2.5 percent of its capitation fee as community reinvestment funds. These funds were used to support the program administration and to pay for individualized budgets for program participants. The Iowa SDC program served 36 participants who were receiving intensive psychiatric rehabilitation services. Each participant chose one rehabilitation goal relating to housing, education, employment or relationships and could use a budget of up to $2,000 in support of achieving this goal. Magellan operated as the fiscal intermediary for the program.
Maryland
The SDC program in Washington County, Maryland was started in 2007 and continues to operate with funding from the Maryland Mental Hygiene Administration. The program is modeled after the Florida SDC program, and is managed by a consumer-run organization, the Office of Consumer Advocates. The Washington County Mental Health Authority, a local "core service agency" that receives funding from the Mental Hygiene Administration, serves as the fiscal intermediary. By the end of 2009, approximately 165 consumers had enrolled in the program.
The program administration and individual budgets are supported with state general funds. Additional costs for training, program evaluation and other related technical assistance were funded by a Mental Health Transformation State Incentive Grant. Each participant could, on average, receive a budget of approximately $3,000 per year. However, there is no cap on the amount allotted to each individual and many consumers use less than the full $3,000. Instead, budgets vary from consumer to consumer based on the services that the consumer identifies as necessary to support his or her ongoing progress in recovery.
The program employs one full-time and two part-time peer-advocates (two full-time equivalents). Peers help consumers finding community resources within natural support networks wherever possible. Once the services that need to be purchased to support a consumer's recovery have been identified, participants submit purchase requests to the core services agency. Approved items are paid by check or by direct reimbursement to the participant.
Michigan
In Michigan, statewide implementation of the SDC approach began in 2003 and is formally supported by the Mental Health and Substance Abuse Administration (MHSAA), the state mental health authority. The MHSAA has created a policy framework--the Choice Voucher System--for implementing SDC arrangements in programs serving adult participants in the state's public mental health system.70 The Choice Voucher System provides prototype contractual agreements, payment mechanisms and other technical assistance information for supporting the SDC approach in programs for adults who are receiving mental health and/or developmental disability services. SDC programs can operate with flexible funding from Medicaid, using the state's 1915b/c waiver authority.c SDC programs are managed by county mental health service providers and peers are employed to support SDC participants. The development of SDC programs was also promoted by state grants awarded to Kalamazoo and Oakland Counties in 2005.
New Hampshire
The State of New Hampshire developed the Dollars and Sense Individual Career Account (ICA) demonstration research project to test the impact of greater beneficiary choice and control over vocational service planning, budgeting and service/item procurement on vocational outcomes and consumer satisfaction.71, 72 Although the ICA service model did not include all SDC components, it did include person-centered planning and individualized budgeting. The project also offered a subset of individuals a "cash account" developed with project dollars and matching funds from the New Hampshire Division of Behavioral Health. A total of 181 individuals enrolled in the project over a 3-year period. All participants were Social Security Disability Insurance beneficiaries or SSI recipients at the time of enrollment, and two-thirds had a mental health disability.
Oregon
Oregon has an innovative SDC program called the Empowerment Initiatives Brokerage (EIB). The EIB is a consumer-operated organization started in 2004 using funding from a Real Choice Systems Grant.68, d Unlike SDC programs in other states, EIB offers participants only a 1-year period of participation. Participants have access to an individual budget of $3,000 and are supported through a person-centered planning process. Peer service providers are employed as coaches or "resource brokers." Alakeson reports that the program's total cost is approximately $10,000 per consumer served.33
Although the Real Choice Systems Change grant ended in September 2005, EIB continues to operate under contracts with Multnomah and Clackamas Counties, where the program has operated since 2001. EIB services in Multnomah County are similar to SDC services in other states, and are funded by a mixture of Medicaid dollars and state general revenue. In Clackamas County, EIB has a specific focus of supporting transitions to independent living arrangements for individuals currently living in group homes. The housing brokerage is state funded but overseen by Clackamas County.
Pennsylvania
The Delaware County Self-Directed Care for Community Integration of Individuals with Psychiatric Disabilities is a 2-year pilot SDC program for non-elderly disabled adults with SMI who have a history of ongoing engagement in public mental health care services. The program, which began operating in 2010, is part of an ongoing collaboration between the Delaware County Office of Behavioral Health, Magellan Behavioral Health of Pennsylvania, the Mental Health Association of Southeastern Pennsylvania, and the University of Pennsylvania Collaborative for Community Integration.
The program was implemented for the purpose of conducting a randomized trial to compare mental health SDC to traditional care. Beginning in January 2010, approximately 150-160 persons, all of whom were receiving Medicaid, were randomized either to the Delaware County SDC program (75-85 persons) or to traditional managed behavioral health care (75 persons). The SDC program features individualized budgets and person-centered planning. Peer support specialists serve as recovery coaches, and they are managed by a program supervisor. Magellan serves as the program's fiscal intermediary.
The amount of money assigned to participants' individualized budgets is calibrated based on each participant's 2-year history of Medicaid expenditures for outpatient mental health care services. As a result, each participant may have been allocated a unique budget for spending on traditional and non-traditional products and services. Using this method, SDC participants with more intensive service needs in the past could be expected to spend more money during their first 2 years of SDC participation than participants with less intensive service needs.
All mental health care services that are available through the Pennsylvania's 1915(b) HealthChoices Medicaid waiver program are paid for using Medicaid funding from the 1915(b) waiver. All products and services not covered under the 1915(b) waiver (e.g., classes at a community college) are paid for using "Freedom Funds." Freedom Funds are residual savings from the prior fiscal year of the state's 1915(b) HealthChoices waiver. Expenditures are deducted on an ongoing basis from the balance of participants' individual budgets. The financial intermediary monitors budget balances to ensure that participants are not likely to over spend their budgets before the end of the plan year.
Certified peer support specialists--individuals who are in recovery themselves and who embody the message that recovery is possible--are reimbursed using 1915(b) HealthChoices waiver funding, as peer support services are Medicaid-reimbursable. By using certified peer support specialists in the role of recovery coaches, the program does not require additional funding from another (non-Medicaid) source to pay for coaching services. The rate paid for peer support specialist services also includes an administrative reimbursement to cover the costs of a program supervisor. These reimbursements cover the costs of the Delaware County SDC program supervisor, who approves participants' purchases and is responsible for various administrative tasks. During the Delaware County program's first year, some additional funding was provided by the mental health authority to cover training and operational expenses.
Texas
The SDC program in Dallas County, Texas (Texas SDC) was established in 2009 through a public-academic partnership between the Texas Department of State Health Services (DSHS) and the UIC).73 In 2005, the two organizations began planning a pilot SDC program for persons with SMI. In that year, Texas was awarded a SAMHSA Transformation State Incentive Grant, which provided funding for pilot program planning, implementation, and evaluation. The Texas SDC program is being rigorously evaluated in a randomized trial comparing Texas SDC (150 persons) to services as usual (150 persons). Those assigned to SDC are provided with tools for person-centered planning and creation of an individual budget tied to specific recovery goals.
The program planning process was designed to ensure that the resulting program would be responsive to the needs of the local community and also based on the available evidence.73 Multi-stakeholder subcommittees were formed, made up of consumers, providers, researchers, DSHS staff, family members and other mental health advocates. Subcommittees met weekly via teleconference and in-person over a 3-month period to decide on the program's policies and procedures, determine staffing and organization, create a purchasing policy, design the provider network, and discuss use of information technology to enhance program operation. Subcommittees sought research evidence as well as information from participants and state administrators at SDC programs in Florida and Oregon.
Texas has a Medicaid 1915(b) managed care waiver for Dallas County, which permits Medicaid financing to be combined with state general revenues, mental health block grant funding, and other local program funding. Participants in Texas SDC are allocated an individual budget of $4,000 per year, with up to $7,000 per year available for individuals who need high levels of service.73 This latter group includes individuals whose outpatient service expenditures in the year prior to program entry exceeded the average of $4,000 due to mental health or related life crises. Medications, crisis services, and inpatient care are not covered in the SDC budget but remain available through the current service system. The program is managed by a managed behavioral health care organization, Value Options, which also serves as the fiscal intermediary.
In relation to program organization, participants can select services and providers from the program's provider network, and participants complete a person-centered planning and budgeting process with assistance from coaches, who are called "SDC Advisors." Although participants must use care providers in the Texas SDC program network, any provider who agrees to abide by the SDC program's philosophy and policies can enroll. This implies that participants can continue seeing the same providers they were seeing before entering SDC as long as these providers are willing to enroll in the Texas SDC provider network. Persons in mental health recovery are involved in all aspects of the program, including recruiting and hiring the program's director and SDC Advisors, and serving on the community advisory board.73
Information technology is integrated into the design of the Texas SDC program. Participants' purchases are made with pre-paid debit cards (the Allow Card of America™ pre-paid MasterCard). SDC Advisors travel in the community to provide brokerage services with laptops and portable printers, using wireless technology to help participants create recovery plans and budgets. A Texas SDC program website (http://www.texassdc.org) establishes a public presence for the program and serves as a portal for communications among participants, coaches, and program administrators. Participants communicate with each other via a chat room that is closed to outsiders, which they access through a secure link from the website.
References
-
Cook JA, Terrell S, JonikasJA. 2004. Promoting Self-Determination for Individuals with Psychiatric Disabilities through Self-Directed Services: A Look at Federal, State and Public Systems as Sources of Cash-Outs and Other Fiscal Expansion Opportunities. Rockville, MD: Substance Abuse and Mental Health Services Administration.
-
Koyanagi C, Alfano E, Carty L. 2008. In The Driver's Seat: A Guide to Self-Directed Mental Health Care. Washington, DC: Bazelon Center for Mental Health Law and UPENN Collaborative on Community Integration.
-
President's New Freedom Commission on Mental Health. 2003. Achieving the Promise: Transforming Mental Health Care in America. Final Report. Rockville, MD: Substance Abuse and Mental Health Services Administration, DHHS Pub. No. SMA-03-3832.
-
Doty P, Kasper J, LitvakS. 1996. Consumer-directed models of personal care: Lessons from Medicaid. Milbank Quarterly, 74(3):377-409. [http://aspe.hhs.gov/daltcp/reports/lessons.htm]
-
Simon-Rusinowitz L, Hofland BF. 1993. Adopting a disability approach to home care services for older adults. Gerontologist, 33(2):159-167.
-
Batavia AI. 2002. Consumer direction, consumer choice, and the future of long-term care. Journal of Disability Policy Studies, 13(2):67-74.
-
Grob GN. 1995. The paradox of deinstitutionalization. Society, 32(5):51-59.
-
Tomes N. 2006. The patient as a policy factor: A historical case study of the consumer/survivor movement in mental health. Health Affairs, 25(3):720-729.
-
Cook JA. 2005. "Patient-Centered" and "Consumer-Directed" Mental Health Services. Washington, DC: Institute of Medicine, Committee on Crossing the Quality Chasm--Adaptation to Mental Health and Addictive Disorders.
-
Conroy JW, YuskauskasA. 1996. Independent Evaluation of the Monadnock Self Determination Project. Narberth, PA: The Center for Outcome Analysis.
-
Conroy JW, Fullerton AY, Brown M, Garrow J. 2002. Outcomes of the Robert Wood Johnson Foundation's National Initiative on Self-Determination for Persons with Developmental Disabilities: Final Report on 3 Years of Research and Analysis. Narberth, PA: Center for Outcome Analysis.
-
Bradley V, Agosta J, Smith G, Taub S, AshbaughJ, Silver J, Heaviland M. 2001. The Robert Wood Johnson Foundation Self-Determination Initiative: Final Impact Assessment Report. Cambridge, MA: The Human Services Research Institute.
-
Doty P, Mahoney KJ, Simon RusinowitzL. 2007 Designing the Cash and Counseling demonstration and evaluation. Health Services Research, 42(1p2):378-396.
-
Carlson BL, Foster L, Dale SB, Brown R. 2007. Effects of Cash and Counseling on personal care and well-being. Health Services Research, 42(1p2):467-487.
-
Dale S, Brown R, Phillips B, Schore J, Carlson BL. 2003. The effects of Cash and Counseling on personal care services and Medicaid costs in Arkansas. Health Affairs, W3-566-W3-575.
-
Dale SB, Brown RS. 2007. How does cash and counseling affect costs? Health Services Research, 42(1p2):488-509.
-
Foster L, Dale SB, Brown R. 2007. How caregivers and workers fared in cash and counseling. Health Services Research, 42(1):510-532.
-
Brown RS, Dale SB. 2007. The research design and methodological issues for the cash and counseling evaluation. Health Services Research, 42(1p2):414-445.
-
Kemper P. 2007. Commentary: Social experimentation at its best: The cash and counseling demonstration and its implications. Health Services Research, 42(1 Pt 2):577-586.
-
Spaulding-Givens J. 2011. Florida Self-Directed Care: An Exploratory Study of Participants' Characteristics, Goals, Service Utilization, and Outcomes. Florida State University, College of Social Work.
-
Institute of Medicine. 2006. Improving the Quality of Health Care for Mental and Substance-Use Conditions: Quality Chasm Series. Washington, DC: The National Academies Press.
-
Corrigan PW. 2002. Empowerment and serious mental illness: Treatment partnerships and community opportunities. Psychiatric Quarterly, 73(3):217-228.
-
Adams JR, Drake RE. 2006. Shared decision-making and evidence-based practice. Community Mental Health Journal, 42:87-105.
-
Druss BG, Marcus SC, Rosenheck RA, Olfson M, Tanielian T, Pincus HA. 2000. Understanding disability in mental and general medical conditions. American Journal of Psychiatry, 157(9):1485-1491.
-
Adams J, Drake R, Wolford G. 2007. Shared decision-making preferences of people with severe mental illness. Psychiatric Services, 58:1219-1221.
-
Elmendorf DW. 2011. Analysis of the Major Health Care Legislation Enacted in March 2010. Washington, DC: Congressional Budget Office.
-
Garfield RL, ZuvekasSH, Lave JR, Donohue JM. 2011. The impact of national health care reform on adults with severe mental disorders. American Journal of Psychiatry, 168:486-494.
-
Mann C. 2010. CMS Letter to State Medicaid Directors: Improving Access to Home and Community-Based Services. Baltimore, MD: Centers for Medicare and Medicaid Services, Center for Medicaid, CHIP, and Survey and Certification.
-
U.S. Department of Health and Human Services. 1999. Mental Health: A Report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration and the National Institute of Mental Health.
-
Sharma T, Antonova L. 2003. Cognitive function in schizophrenia. Deficits, functional consequences, and future treatment. Psychiatric Clinics of North America, 26(1):25-40.
-
Velligan DI, Mahurin RK, Diamond PL, Hazleton BC, Eckert SL, Miller AL. 1997. The functional significance of symptomatologyand cognitive function in schizophrenia. Schizophrenia Research, 25(1):21-31.
-
Dickerson FB. 1997. Assessing clinical outcomes: The community functioning of persons with serious mental illness. Psychiatric Services, 48(7):897-902.
-
Alakeson V. 2007. The Contribution of Self-Direction to Improving the Quality of Mental Health Services. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services. [http://aspe.hhs.gov/daltcp/reports/2007/MHslfdir.htm]
-
Stefan S. 2004. Competence Issues in Self-Directed Care. Newton, MA: Center for Public Representation.
-
Swanson JW, Swartz MS, ElbogenEB, Van Dorn RA, Wagner HR, Moser LA, Wilder C, Gilbert AR. 2008. Psychiatric advance directives and reduction of coercive crisis interventions. Journal of Mental Health, 17(3):255-267.
-
Henderson C, Swanson J, SzmuklerG, Thornicroft G, ZinklerM. 2008. A typology of advance statements in mental health care. Psychiatric Services, 59(1):63-71.
-
Swanson J, Swartz M, FerronJ, Elbogen E, Van Dorn R. 2006. Psychiatric advance directives among public mental health consumers in five US cities: Prevalence, demand, and correlates. Journal of the American Academy of Psychiatry and the Law Online, 34(1):43-57.
-
Swanson JW, Van McCrary S, Swartz MS, Elbogen EB, Van Dorn RA. 2006. Superseding psychiatric advance directives: Ethical and legal considerations. Journal of the American Academy of Psychiatry and the Law Online, 34(3):385-394.
-
Green MF. 1996. What are the functional consequences of neurocognitive deficits in schizophrenia? American Journal of Psychiatry, 153(3):321-330.
-
Rosenheck R, Leslie D, Keefe R, McEvoy J, Swartz M, Perkins D, Stroup S, Hsiao JK, Lieberman J. 2006. Barriers to employment for people with schizophrenia.American Journal of Psychiatry, 163(3):411-417.
-
Rosenheck R, Stroup S, Keefe RSE, McEvoy J, Swartz M, Perkins D, Hsiao J, Shumway M, Lieberman J. 2005. Measuring outcome priorities and preferences in people with schizophrenia. British Journal of Psychiatry, 187(6):529-536.
-
Resnick SG, Rosenheck RA, Lehman AF. 2004. An exploratory analysis of correlates of recovery. Psychiatric Services, 55(5):540-547.
-
Swartz M, Perkins D, Stroup T, Davis S, Capuano G, Rosenheck R, Reimherr F, McGee M, Keefe R, McEvoy J. 2007. Effects of antipsychotic medications on psychosocial functioning in patients with chronic schizophrenia: Findings from the NIMH CATIE study. American Journal of Psychiatry, 164(3):428-436.
-
Granholm E, McQuaid JR, McClure FS, AuslanderLA, Perivoliotis D, PedrelliP, Patterson T, Jeste DV. 2005. A randomized, controlled trial of cognitive behavioral social skills training for middle-aged and older outpatients with chronic schizophrenia. American Journal of Psychiatry, 162(3):520-529.
-
Brown AH, Cohen AN, ChinmanMJ, Kessler C, Young AS. 2008. EQUIP: Implementing chronic care principles and applying formative evaluation methods to improve care for schizophrenia: QUERI series. Implementation Science, 3(9), doi:10.1186/1748-5908-3-9.
-
Young AS, Mintz J, Cohen AN. 2004. Clinical computing: Using information systems to improve care for persons with schizophrenia. Psychiatric Services, 55(3):253-255, doi: 10.1176/appi.ps.55.3.253.
-
Chinman M, Young AS, Schell T, Hassell J, MintzJ. 2004. Computer-assisted self-assessment in persons with severe mental illness. Journal of Clinical Psychiatry, 65(10):1343-1351.
-
Chinman M, Hassell J, Magnabosco J, Nowlin-Finch N, Marusak S, Young AS. 2007. The feasibility of computerized patient self-assessment at mental health clinics. Administration and Policy in Mental Health and Mental Health Services Research, 34(4):401-409.
-
Elbogen EB, Swanson JW, Swartz MS. 2003. Effects of legal mechanisms on perceived coercion and treatment adherence among persons with severe mental illness. Journal of Nervous and Mental Disease, 191(10):629-637.
-
Goldman HH, Azrin ST. 2003. Public policy and evidence-based practice. Psychiatric Clinics of North America, 26(4):899-917.
-
Ganju V. 2003. Implementation of evidence-based practices in state mental health systems. Schizophrenia Bulletin, 29(1):125-131.
-
Rapp CA, Bond GR, Becker DR, CarpinelloSE, Nikkel RE, Gintoli G. 2005. The role of state mental health authorities in promoting improved client outcomes through evidence-based practice. Community Mental Health Journal, 41(3):347-363.
-
Berwick DM. 2011. Launching accountablecare organizations--the proposed rule for the Medicare shared savings program. New England Journal of Medicine, 364(e32).
-
Watson AC, Corrigan P, Larson JE, Sells M. 2007. Self-stigma in people with mental illness. Schizophrenia Bulletin, 33(6):1312-1318.
-
Cook J, Copeland ME, Hamilton M, Jonikas J, Razzano L, Floyd C, Hudson W, Macfarlane R, Grey D. 2009. Initial outcomes of a mental illness self-management program based on wellness recovery action planning. Psychiatric Services, 60(2):246-249.
-
Druss BG, Zhao L, von Esenwein SA, Bona JR, Fricks L, Jenkins-Tucker S, Sterling E, DiClemente R, Lorig K. 2010. The health and recovery peer(HARP) program: A peer-led intervention to improve medical self-management for persons with serious mental illness. Schizophrenia Research, 118(1-3):264-270.
-
Doty P, Mahoney KJ, SciegajM. 2010. New state strategies to meet long-term care needs. Health Affairs, 29(1):49-56.
-
Cook JA, Russell C, Grey DD, JonikasJA. 2009. Economic grand rounds: A self-directed care model for mental health recovery. Psychiatric Services, 59(6):600-602.
-
Smith G, O'Keefe J, Carpenter L, Doty P, et al. 2000. Understanding Medicaid Home and Community-Based Services: A Primer. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. [http://aspe.hhs.gov/daltcp/reports/primer.htm]
-
Rosenbaum S, TeitelbaumJ. 2004. Olmstead at Five: Assessing the Impact. Washington, DC: Kaiser Commission on Medicaid and the Uninsured, Henry J. Kaiser Family Foundation, 1-27.
-
Crawley JS. 2003. An Overview of the Independence PlusInitiative to Promote Consumer-Direction of Services in Medicaid. Washington, DC: The Henry J. Kaiser Family Foundation.
-
Smith DG. 2007. CMS Letter to State Medicaid Directors, SMDL #07-013. Baltimore, MD: Centers for Medicare and Medicaid Services, Center for Medicaid and State Operations.
-
Centers for Medicare and Medicaid Services. 2008. Medicaid program: Self-directed personal assistance services program state plan option (cash and counseling). Federal Register, 73(13): 3546-3566.
-
Centers for Medicare and Medicaid Services. 2011. Medicaid program: Community First Choice Option. Federal Register, 76(38):10736-10753.
-
Wishon-Siegwarth AA, Koyanagi C. 2011. The new Health Care Reform Act and Medicaid: New opportunities for psychiatric rehabilitation. Psychiatric Rehabilitation Journal, 34(4):277-284.
-
NASMHPD. 2011. FY2009 State Mental Health Revenue and Expenditure Study Results. Falls Church, VA: NRI.
-
Office of Program Policy Analysis and Government Accountability. 2010. Insufficient Information Available to Fully Assess the Success of the Self-Directed Care Program. Tallahassee, FL: OPPAGA,10-40.
-
Sullivan A. 2006. Empowerment Initiatives Brokerage Service: Quality and Outcome Evaluation. Salem, OR: Oregon Technical Assistance Corporation.
-
Ellison ML, Rogers ES, LyassA, Massaro J, Wewiorski NJ, Hsu ST, Anthony WA. 2011. Statewide initiative of intensive psychiatric rehabilitation: Outcomes and relationship to other mental health service use. Psychiatric Rehabilitation Journal, 35(1):9-19.
-
Michigan Department of Community Health. 2008. Choice Voucher System: Self-Determination Technical Advisory, Version 2.0. Lansing, MI: Mental Health and Substance Abuse Administration.
-
O'Brien D, Ford L, Malloy J. 2005. Person centered funding: Using vouchers and personal budgets to support recovery and employment for people with psychiatric disabilities. Journal of Vocational Rehabilitation, 23(2):71-79.
-
Cloutier H, Mallory J,Hagner D, Cotton P. 2006. Choice and control over resources: New Hampshire's individual career account demonstration projects. Journal of Rehabilitation, 72(2):4-11.
-
Cook JA, Shore SE, Burke-Miller JK, Jonikas JA, Ferrara M, ColegroveS, Norris WT, Ruckdeschel B, BatteigerAP, Ohrtman M. 2010. Participatory action research to establish self-directed care for mental health recovery in Texas. Psychiatric Rehabilitation Journal, 34(2):137-144.
Notes
-
Although other mental health SDC programs might pre-date Florida SDC, documentation of these programs is scarce.
-
The 1915b/c waiver combines a Medicaid 1915(b) Managed Care waiver with a Medicaid 1915(c) HCBS waiver.
-
Real Choice Systems Change from the CMS support states' development of regulatory, administrative, program, and funding infrastructure for reducing individuals' reliance on institutional services and increasing their assess to HCBS.
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human Services
Office of Disability, Aging and Long-Term Care Policy
Room 424E, H.H. Humphrey Building
200 Independence Avenue, S.W.
Washington, D.C. 20201
FAX: 202-401-7733
Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/office_specific/daltcp.cfm]
Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]
U.S. Department of Health and Human Services (HHS) Home [http://www.hhs.gov]